
The Need for Individualized Risk Assessment in Cardiovascular Disease

 , ,
, ,
Abstract
:1. Introduction
2. Traditional Risk Factors for Cardiovascular Disease
3. Current Available Risk Assessment Tools
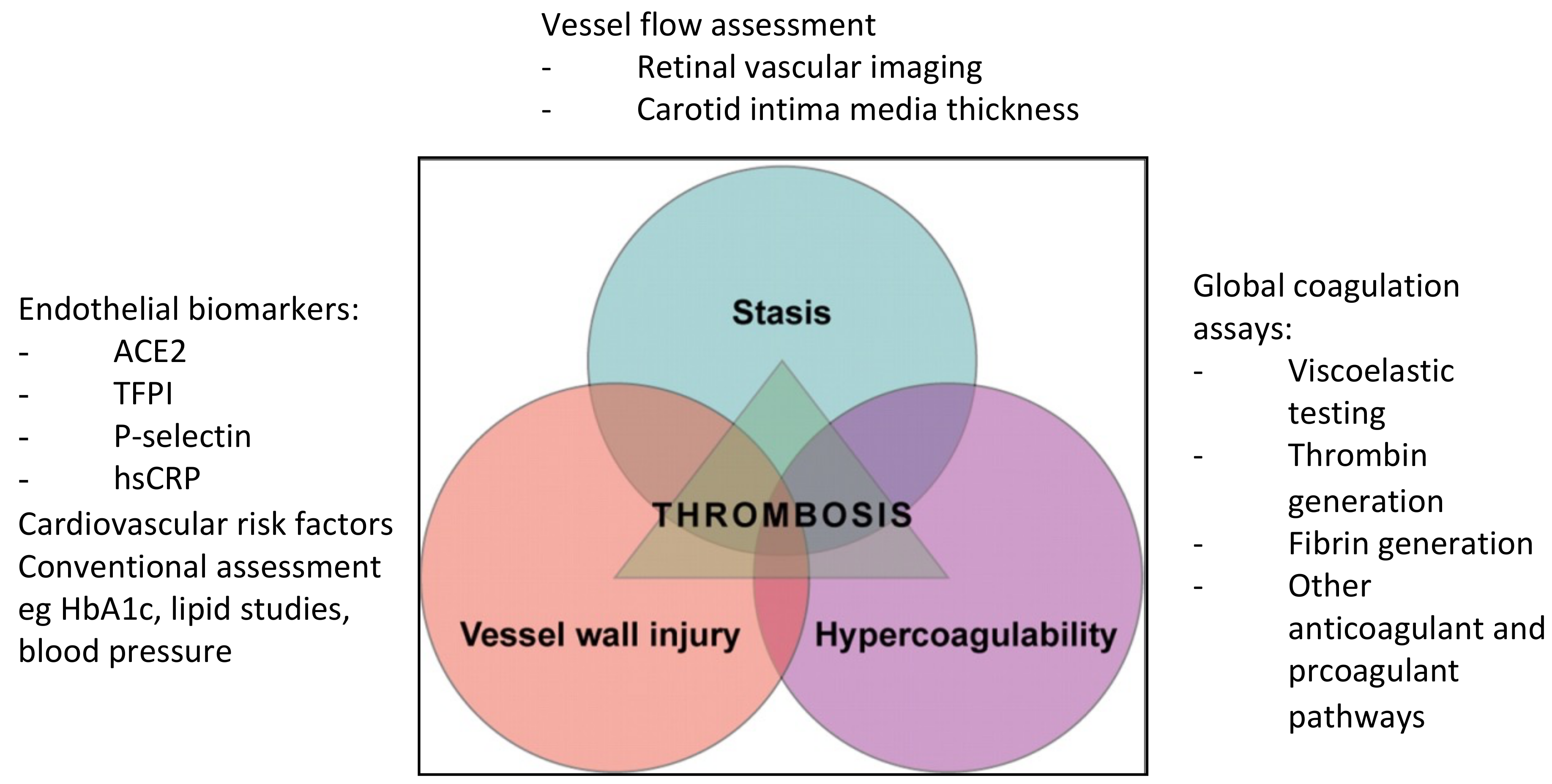
4. Virchow’s Triad and Its Association with Thrombosis and Cardiovascular Disease
4.1. Assessment of Hypercoagulability with Global Coagulation Assays
4.2. Endothelial Dysfunction
4.3. Vessel Flow
5. Genetic Insights into Cardiovascular Risk and Disease
6. Clinical Implications and Future Prospects
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Cardiovascular Diseases. Available online: https://www.who.int/health-topics/cardiovascular-diseases#tab=tab_1 (accessed on 1 June 2022).
- Lloyd-Jones, D.M.; Larson, M.G.; Beiser, A.; Levy, D. Lifetime risk of developing coronary heart disease. Lancet 1999, 353, 89–92. [Google Scholar] [CrossRef]
- Patel, S.A.; Winkel, M.; Ali, M.K.; Narayan, K.M.; Mehta, N.K. Cardiovascular mortality associated with 5 leading risk factors: National and state preventable fractions estimated from survey data. Ann. Intern. Med. 2015, 163, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Chung, I.; Lip, G.Y.H. Virchow’s triad revisited: Blood constituents. Pathophysiol. Haemost. Thromb. 2004, 33, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Seidman, M.A.; Mitchell, R.N.; Stone, J.R. Pathophysiology of atherosclerosis. In Cellular and Molecular Pathobiology of Cardiovascular Disease; Willis, M., Homeister, J., Stone, J., Eds.; Elsevier: San Diego, CA, USA, 2014; pp. 221–237. ISBN 978-0-12-405206-2. [Google Scholar]
- Singh, R.B.; Mengi, S.A.; Xu, Y.; Arneja, A.S.; Dhalla, N.S. Pathogenesis of atherosclerosis: A multifactorial process. Exp. Clin. Cardiol. 2002, 7, 40–53. [Google Scholar]
- Bergheany, S.C.; Bodde, M.C.; Jukema, J.W. Pathophysiology and treatment of atherosclerosis: Current view and future perspective on lipoprotein modification treatment. Neth. Heart J. 2017, 25, 231–242. [Google Scholar] [CrossRef] [Green Version]
- Lakatta, E.; Levy, D. Arterial and cardiac aging: Major shareholders in cardiovascular disease enterprises. Circulation 2003, 107, 139–146. [Google Scholar] [CrossRef] [Green Version]
- Lakatta, E. So! What’s aging? Is cardiovascular aging a disease? J. Mol. Cell. Cardiol. 2015, 83, 1–13. [Google Scholar] [CrossRef] [Green Version]
- AlGhatrif, M.; Wang, M.; Fedorova, O.V.; Bagrov, A.Y.; Lakatta, E.G. The pressure of aging. Med. Clin. N. Am. 2017, 101, 81–101. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Weber, N.C.; Cohn, D.M.; Hollmann, M.W.; Hans DeVries, J.; Hermanides, J.; Preckel, B. Effects of hyperglycemia and diabetes mellitus on coagulation and hemostasis. J. Clin. Med. 2021, 10, 2419. [Google Scholar] [CrossRef]
- Carr, M.E. Diabetes mellitus: A hypercoagulable state. J. Diabetes Complicat. 2001, 15, 44–54. [Google Scholar] [CrossRef]
- Alzahrani, S.H.; Ajjan, R.A. Coagulation and fibrinolysis in diabetes. Diabetes Vasc. Dis. Res. 2010, 7, 260–273. [Google Scholar] [CrossRef] [PubMed]
- Dokken, B.B. The pathophysiology of cardiovascular disease and diabetes: Beyond blood pressure and lipids. Diabetes Spectr. 2008, 21, 160–165. [Google Scholar] [CrossRef] [Green Version]
- Tabas, I. Consequences of cellular cholesterol accumulation: Basic concepts and physiological implications. J. Clin. Investig. 2002, 110, 905–911. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 8 May 2022).
- Wilson, P.; Bozeman, S.R.; Burton, T.M.; Hoaglin, D.C.; Ben-Joseph, R.; Pashos, C.L. Prediction of first events of coronary heart disease and stroke with consideration of adiposity. Circulation 2008, 118, 124–130. [Google Scholar] [CrossRef] [Green Version]
- Powell-Wiley, T.M.; Poirier, P.; Burke, L.E.; Després, J.P.; Gordon-Larsen, P.; Lavie, C.J.; Lear, S.A.; Ndumele, C.E.; Neeland, I.J.; Sanders, P.; et al. Obesity and cardiovascular disease: A scientific statement from the American Heart Association. Circulation 2021, 143, e984–e1010. [Google Scholar] [CrossRef]
- Scuteri, A.; Franco, O.H.; Majiid, A.; Jolita, B.; Sergey, B.; Cheng, H.M.; Chen, C.H.; Choi, S.W.; Francesco, C.; De Buyzere, M.L.; et al. The relationship between the metabolic syndrome and arterial wall thickness: A mosaic still to be interpreted. Atherosclerosis 2016, 255, 11–16. [Google Scholar] [CrossRef]
- Khambhati, J.; Allard-Ratick, M.; Dhindsa, D.; Lee, S.; Chen, J.; Sandesara, P.B.; O’Neal, W.; Quyyumi, A.A.; Wong, N.D.; Blumenthal, R.S.; et al. The art of cardiovascular risk assessment. Clin. Cardiol. 2018, 41, 677–684. [Google Scholar] [CrossRef] [Green Version]
- National Vascular Disease Prevention Alliance. Guidelines for the Management of Absolute Cardiovascular Disease Risk. Available online: http://www.cvdcheck.org.au/index.php?option=com_content&view=article&id=47&Itemid=27 (accessed on 30 December 2020).
- Goff, D.C.; Lloyd-Jones, D.M.; Bennett, G.; Coady, S.; D’agostino, R.B.; Gibbons, R.; Greenland, P.; Lackland, D.T.; Levy, D.; O’Donnell, C.J.; et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014, 129, S49–S73. [Google Scholar] [CrossRef] [Green Version]
- D’Agostino Sr, R.B.; Vasan, R.S.; Pencina, M.J.; Wolf, P.A.; Cobain, M.; Massaro, J.M.; Kannel, W.B. General cardiovascular risk profile for use in primary care: The Framingham Heart Study. Circulation 2008, 117, 743–753. [Google Scholar] [CrossRef] [Green Version]
- SCORE2 Working Group; ESC Cardiovascular Risk Collaboration. SCORE2 risk prediction algorithms: New models to estimate 10-year risk of cardiovascular disease in Europe. Eur. Heart J. 2021, 42, 2439–2454. [Google Scholar] [CrossRef]
- Hippisley-Cox, J.; Coupland, C.; Brindle, P. Development and validation of QRISK3 risk prediction algorithms to estimate future risk of cardiovascular disease: Prospective cohort study. BMJ 2017, 357, j2099. [Google Scholar] [CrossRef] [Green Version]
- DeFilippis, A.P.; Young, R.; Carrubba, C.J.; McEvoy, J.W.; Budoff, M.J.; Blumenthal, R.S.; Kronmal, R.A.; McClelland, R.L.; Nasir, K.; Blaha, M.J. An analysis of calibration and discrimination among multiple cardiovascular risk scores in a modern multiethnic cohort. Ann. Intern. Med. 2015, 162, 266–275. [Google Scholar] [CrossRef] [Green Version]
- Lim, H.Y.; Donnan, G.; Nandurkar, H.; Ho, P. Global coagulation assays in hypercoagulable states. J. Thromb. Thrombolysis 2022, 54, 132–144. [Google Scholar] [CrossRef]
- Kleinegris, M.C.; Ten Cate-Hoek, A.J.; Ten Cate, H. Coagulation and the vessel wall in thrombosis and atherosclerosis. Pol. Arch. Med. Wewn. 2012, 122, 557–566. [Google Scholar] [CrossRef] [Green Version]
- Ageno, W.; Becattini, C.; Brighton, T.; Selby, R.; Kamphuisen, P.W. Cardiovascular risk factors and venous thromboembolism: A meta-analysis. Circulation 2008, 117, 93–102. [Google Scholar] [CrossRef] [Green Version]
- Prandoni, P.; Bilora, F.; Marchiori, A.; Bernardi, E.; Petrobelli, F.; Lensing, A.W.A.; Prins, M.H.; Girolami, A. An association between atherosclerosis and venous thrombosis. N. Engl. J. Med. 2003, 348, 1435–1441. [Google Scholar] [CrossRef] [Green Version]
- Lebas, H.; Yahiaoui, K.; Martos, R.; Boulaftali, Y. Platelets are at the nexus of vascular diseases. Front. Cardiovasc. Med. 2019, 6, 132. [Google Scholar] [CrossRef]
- Adams, R.L.C.; Bird, R.J. Review article: Coagulation cascade and therapeutics update: Relevance to nephrology. Part 1: Overview of coagulation, thrombophilias and history of anticoagulants. Nephrology 2009, 14, 462–470. [Google Scholar] [CrossRef]
- Loeffen, R.; Spronk, H.M.H.; ten Cate, H. The impact of blood coagulability on atherosclerosis and cardiovascular disease. J. Thromb. Haemost. 2012, 10, 1207–1216. [Google Scholar] [CrossRef]
- Lancé, M.D. A general review of major global coagulation assays: Thrombelastography, thrombin generation test and clot waveform analysis. Thromb. J. 2015, 13, 1. [Google Scholar] [CrossRef] [Green Version]
- Lim, H.Y.; O’Malley, C.; Donnan, G.; Nandurkar, H.; Ho, P. A review of global coagulation assays—Is there a role in thrombosis risk prediction? Thromb. Res. 2019, 179, 45–55. [Google Scholar] [CrossRef]
- Bowbrick, V.A.; Mikhailidis, D.P.; Stansby, G. The use of citrated whole blood in thromboelastography. Anesth. Analg. 2000, 90, 1086–1088. [Google Scholar] [CrossRef]
- Lim, H.Y.; Lui, B.; Tacey, M.; Kwok, A.; Varadarajan, S.; Donnan, G.; Nandurkar, H.; Ho, P. Global coagulation assays in patients with diabetes mellitus. Res. Pract. Thromb. Haemost. 2021, 5, e12611. [Google Scholar] [CrossRef]
- Walsh, M.; Moore, E.E.; Moore, H.; Thomas, S.; Lune, S.V.; Zimmer, D.; Dynako, J.; Hake, D.; Crowell, Z.; McCauley, R.; et al. Use of viscoelastography in malignancy-associated coagulopathy and thrombosis: A review. Semin. Thromb. Hemost. 2019, 45, 354–372. [Google Scholar] [CrossRef] [PubMed]
- Yao, X.; Dong, Q.; Song, Y.; Wang, Y.; Deng, Y.; Li, Y. Thrombelastography maximal clot strength could predict one-year functional outcome in patients with ischemic stroke. Cerebrovasc. Dis. 2014, 38, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Rafiq, S.; Johansson, P.I.; Ostrowski, S.R.; Stissing, T.; Steinbrüchel, D.A. Hypercoagulability in patients undergoing coronary artery bypass grafting: Prevalence, patient characteristics and postoperative outcome. Eur. J. Cardiothorac. Surg. 2012, 41, 550–555. [Google Scholar] [CrossRef] [PubMed]
- Carcaillon, L.; Alhenc-Gelas, M.; Bejoy, Y.; Spaft, C.; Ducimetiere, P.; Ritchie, K.; Dartigues, J.; Scarabin, P. Increased thrombin generation is associated with acute ischemic stroke but not with coronary heart disease in the elderly: The Three-City cohort study. Arterioscler. Thromb. Vasc. Biol. 2011, 31, 1445–1451. [Google Scholar] [CrossRef] [Green Version]
- Schneider, J.G.; Isermann, B.; Kleber, M.E.; Wang, H.; Boehm, B.O.; Grammer, T.B.; Prueller, F.; Nawroth, P.P.; Maerz, W. Inverse association of the endogenous thrombin potential (ETP) with cardiovascular death: The Ludwigshafen Risk and Cardiovascular Health (LURIC) study. Int. J. Cardiol. 2014, 176, 139–144. [Google Scholar] [CrossRef] [Green Version]
- Lim, H.Y.; Lui, B.; Tacey, M.; Selan, C.; Donnan, G.; Burrell, L.M.; Nandurkar, H.; Ho, P. Global coagulation assays in healthy controls: Are there compensatory mechanisms within the coagulation system? J. Thromb. Thrombolysis 2021, 52, 610–619. [Google Scholar] [CrossRef]
- Seljeflot, I.; Larsen, J.R.; Dahl-Jorgensen, K.; Hanssen, K.F.; Arnesen, H. Fibrinolytic activity is highly influenced by long-term glycemic control in Type 1 diabetic patients. J. Thromb. Haemost. 2006, 4, 686–688. [Google Scholar] [CrossRef]
- McEwen, B.J.; Morel-Kopp, M.C.; Tofler, G.H.; Ward, C.M. The effect of omega-3 polyunsaturated fatty acids on fibrin and thrombin generation in healthy subjects and subjects with cardiovascular disease. Semin. Thromb. Hemost. 2015, 41, 315–322. [Google Scholar] [CrossRef]
- Reddel, C.J.; Curnow, J.L.; Voitl, J.; Rosenov, A.; Pennings, G.J.; Morel-Kopp, M.C.; Brieger, D.B. Detection of hypofibrinolysis in stable coronary artery disease using the overall haemostatic potential assay. Thromb. Res. 2013, 131, 457–462. [Google Scholar] [CrossRef]
- Miszta, A.; Huskens, D.; Donkervoot, D.; Roberts, M.K.M.; Wolberg, A.S.; de Laat, B. Assessing plasmin generation in health and disease. Int. J. Mol. Sci. 2021, 22, 2758. [Google Scholar] [CrossRef]
- Miszta, A.; Kopec, A.; Pant, A.; Holle, L.A.; Byrnes, J.R.; Lawrence, D.A.; Hansen, K.C.; Flick, M.J.; Luyendyk, J.P.; de Laat, B.; et al. A high-fat diet delays plasmin generation in a thrombomodulin-dependent manner in mice. Blood 2020, 135, 1704–1717. [Google Scholar] [CrossRef]
- Sun, H.; Wu, Z.; Nie, X.; Bian, J. Role of endothelial dysfunction in cardiovascular diseases: The link between inflammation and hydrogen sulfide. Front. Pharm. 2020, 10, 1568. [Google Scholar] [CrossRef] [Green Version]
- Alexander, Y.; Osto, E.; Schmidt-Trucksass, A.; Shechter, M.; Trifunovic, D.; Duncker, D.J.; Aboyans, V.; Back, M.; Badimon, L.; Cosentino, F.; et al. Endothelial function in cardiovascular medicine: A consensus paper of the European Society of Cardiology Working Groups on Atherosclerosis and Vascular Biology, Aorta and Peripheral Vascular Diseases, Coronary Pathophysiology and Microcirculation, and Thrombosis. Cardiovasc. Res. 2021, 117, 29–42. [Google Scholar] [CrossRef] [Green Version]
- Kitta, Y.; Obata, J.; Nakamura, T.; Hirano, M.; Kodama, Y.; Fujioka, D.; Saito, Y.; Kawabata, K.; Sano, K.; Kobayashi, T.; et al. Persistent impairment of endothelial vasomotor function has a negative impact on outcome in patients with coronary artery disease. J. Am. Coll. Cardiol. 2009, 53, 323–330. [Google Scholar] [CrossRef] [Green Version]
- Leander, K.; Malarstig, A.; Van’t Hooft, F.M.; Hyde, C.; Hellénius, M.L.; Troutt, J.S.; Konrad, R.J.; Öhrvik, J.; Hamsten, A.; de Faire, U. Circulating proprotein convertase subtilisin/kexin type 9 (PCSK9) predicts future risk of cardiovascular events independently of established risk factors. Circulation 2016, 133, 1230–1239. [Google Scholar] [CrossRef]
- Ingelsson, E.; Schaefer, E.J.; Contois, J.H.; McNamara, J.R.; Sullivan, L.; Keyes, M.J.; Pencina, M.J.; Schoonmaker, C.; Wilson, P.W.; D’Agostino, R.B.; et al. Clinical utility of different lipid measures for prediction of coronary heart disease in men and women. JAMA 2007, 298, 776–785. [Google Scholar] [CrossRef] [Green Version]
- Garza, C.A.; Montori, V.M.; McConnell, J.P.; Somers, V.K.; Kullo, I.J.; Lopez-Jimenez, F. Association between lipoprotein-associated phospholipase A2 and cardiovascular disease: A systematic review. Mayo Clin. Proc. 2007, 82, 159–165. [Google Scholar] [CrossRef]
- Meuwese, M.C.; Stroes, E.S.G.; Hazen, S.L.; van Miert, J.N.; Kuivenhoven, J.A.; Schaub, R.G.; Wareham, N.J.; Luben, R.; Kastelein, J.J.; Khaw, K.; et al. Serum myeloperoxidase levels are associated with the future risk of coronary artery disease in apparently healthy individuals: The EPIC-Norfolk Prospective Population Study. J. Am. Coll. Cardiol. 2007, 50, 159–165. [Google Scholar] [CrossRef] [Green Version]
- Ridker, P.M. C-reactive protein and the prediction of cardiovascular events among those at intermediate risk. J. Am. Coll. Cardiol. 2007, 49, 2129–2138. [Google Scholar] [CrossRef] [Green Version]
- Cook, N.R.; Buring, J.; Ridker, P.M. The effect of including C-reactive protein in cardiovascular risk prediction models for women. Ann. Intern. Med. 2006, 145, 21–29. [Google Scholar] [CrossRef] [Green Version]
- Hagstrom, E.; James, S.K.; Bertilsson, M.; Becker, R.C.; Himmelmann, A.; Husted, S.; Katus, H.A.; Steg, P.G.; Storey, R.F.; Siegbahn, A.; et al. Growth differentiation factor-15 level predicts major bleeding and cardiovascular events in patients with acute coronary syndromes: Results from the PLATO study. Eur. Heart J. 2016, 37, 1325–1333. [Google Scholar] [CrossRef] [Green Version]
- Donoghue, M.; Hsieh, F.; Baronas, E.; Godbout, K.; Gosselin, M.; Stagliano, N.; Donovan, M.; Woolf, B.; Robison, K.; Jeyaseelan, R.; et al. A novel angiotensin-converting enzyme-related carboxypeptidase (ACE2) converts angiotensin I to angiotensin 1–9. Circ. Res. 2000, 87, E1–E9. [Google Scholar] [CrossRef]
- Oudit, G.Y.; Crackower, M.A.; Backx, P.H.; Penninger, J.M. The role of ACE2 in cardiovascular physiology. Trends Cardiovasc. Med. 2003, 13, 93–101. [Google Scholar] [CrossRef]
- Lew, R.A.; Warner, F.J.; Hanchapola, I.; Yarski, M.A.; Ramchand, J.; Burrell, L.M.; Smith, A.I. Angiotensin-converting enzyme 2 catalytic activity in human plasma is masked by an endogenous inhibitor. Exp. Physiol. 2008, 93, 685–693. [Google Scholar] [CrossRef]
- Hamming, I.; Cooper, M.E.; Haagmans, B.L.; Hooper, N.M.; Korstanje, R.; Osterhaus, A.D.M.E.; Timens, W.; Turner, A.J.; Navis, G.; van Goor, H. The emerging role of ACE2 in physiology and disease. J. Pathol. 2007, 212, 1–11. [Google Scholar] [CrossRef]
- Úri, K.; Fagyas, M.; Kertész, A.; Borbély, A.; Jenei, C.; Bene, O.; Csanádi, Z.; Paulus, W.J.; Édes, I.; Papp, Z.; et al. Circulating ACE2 activity correlates with cardiovascular disease development. J. Renin Angiotensin Aldosterone Syst. 2016, 17, 1470320316668435. [Google Scholar] [CrossRef] [Green Version]
- Úri, K.; Fagyas, M.; Mányiné Siket, I.; Kertész, A.; Csanádi, Z.; Sándorfi, G.; Clemens, M.; Fedor, R.; Papp, Z.; Édes, I.; et al. New perspectives in the renin-angiotensin-aldosterone system (RAAS) IV: Circulating ACE2 as a biomarker of systolic dysfunction in human hypertension and heart failure. PLoS ONE 2014, 9, e87845. [Google Scholar] [CrossRef]
- Soro-Paavonen, A.; Gordin, D.; Forsblom, C.; Rosengard-Barlund, M.; Waden, J.; Thorn, L.; Sandholm, N.; Thomas, M.C.; Groop, P.H.; FinnDiane Study Group. Circulating ACE2 activity is increased in patients with type 1 diabetes and vascular complications. J. Hypertens. 2012, 30, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Anguiano, L.; Riera, M.; Pascual, J.; Valdivielso, J.M.; Barrios, C.; Betriu, A.; Clotet, S.; Mojal, S.; Fernández, E.; Soler, M.J.; et al. Circulating angiotensin converting enzyme 2 activity as a biomarker of silent atherosclerosis in patients with chronic kidney disease. Athrerosclerosis 2016, 253, 135–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, M.A.; Velkoska, E.; Ierino, F.L.; Burrell, L.M. Angiotensin-converting enzyme 2 activity in patients with chronic kidney disease. Nephrol. Dial. Transpl. 2013, 28, 2287–2294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anguiano, L.; Riera, M.; Pascual, J.; Valdivielso, J.M.; Barrios, C.; Betriu, A.; Mojal, S.; Fernández, E.; Soler, M.J.; NEFRONA study. Circulating angiotensin-converting enzyme 2 activity in patients with chronic kidney disease without previous history of cardiovascular disease. Nephrol. Dial. Transpl. 2015, 30, 1176–1185. [Google Scholar] [CrossRef] [Green Version]
- Epelman, S.; Shreshta, K.; Troughton, R.W.; Francis, G.S.; Sen, S.; Klein, A.L.; Wilson Tang, W.H. Soluble angiotensin-converting enzyme 2 in human heart failure: Relation with myocardial function and clinical outcomes. J. Card. Fail. 2009, 15, 565–571. [Google Scholar] [CrossRef] [Green Version]
- Ramchand, J.; Patel, S.; Srivastava, P.M.; Farouque, O.; Burrell, L.M. Elevated plasma angiotensin converting enzyme 2 activity is an independent predictor of major adverse cardiac events in patients with obstructive coronary artery disease. PLoS ONE 2018, 13, e0198144. [Google Scholar] [CrossRef]
- Ramchand, J.; Patel, S.; Kearney, L.G.; Matalanis, G.; Farouque, O.; Srivastava, P.M.; Burrell, L.M. Plasma ACE2 activity predicts mortality in aortic stenosis and is associated with severe myocardial fibrosis. JACC Cardiovasc. Imaging 2020, 13, 655–664. [Google Scholar] [CrossRef]
- Bentzon, J.F.; Otsuka, F.; Virmani, R.; Falk, E. Mechanisms of plaque formation and rupture. Circ. Res. 2014, 114, 1852–1866. [Google Scholar] [CrossRef]
- Saraste, A.; Knuuti, J. ESC 2019 guidelines for the diagnosis and management of chronic coronary syndromes: Recommendations for cardiovascular imaging. Herz 2020, 45, 409–420. [Google Scholar] [CrossRef]
- Divakaran, S.; Cheezum, M.; Hulten, E.A.; Bittencourt, M.S.; Silverman, M.G.; Nasir, K.; Blankstein, R. Use of cardiac CT and calcium scoring for detecting coronary plaque: Implications on prognosis and patient management. Br. J. Radiol. 2015, 88, 20140594. [Google Scholar] [CrossRef] [Green Version]
- Douglas, P.S.; Hoffmann, U.; Patel, M.R.; Mark, D.B.; Al-Khalidi, H.R.; Cavanaugh, B.; Cole, J.; Dolor, R.J.; Fordyce, C.B.; Huang, M.; et al. Outcomes of anatomical versus functional testing for coronary artery disease. N. Engl. J. Med. 2015, 372, 1291–1300. [Google Scholar] [CrossRef] [Green Version]
- Min, J.K.; Dunning, A.; Lin, F.Y.; Achenbach, S.; Al-Mallah, M.; Budoff, M.J.; Cademartiri, F.; Callister, T.Q.; Chang, H.; Cheng, V.; et al. Age- and sex-related differences in all-cause mortality risk based on coronary computed tomography angiography findings results from the International Multicenter CONFIRM (Coronary CT Angiography Evaluation for Clinical Outcomes: An International Multicenter Registry) of 23,854 patients without known coronary artery disease. J. Am. Coll. Cardiol. 2011, 58, 849–860. [Google Scholar] [CrossRef] [Green Version]
- Cheung, C.Y.; Xu, D.; Cheng, C.Y.; Sabanayagam, C.; Tham, Y.C.; Yu, M.; Rim, T.H.; Chai, C.Y.; Gopinath, B.; Mitchell, P.; et al. A deep-learning system for the assessment of cardiovascular disease risk via the measurement of retinal-vessel calibre. Nat. Biomed. Eng. 2021, 5, 498–508. [Google Scholar] [CrossRef]
- Li, L.; Ikram, M.K.; Wong, T.Y. Retinal vascular imaging in early life: Insights into processes and risk of cardiovascular disease. J. Physiol. 2016, 594, 2175–2203. [Google Scholar] [CrossRef] [Green Version]
- Darabian, S.; Hormuz, M.; Latif, M.A.; Pahlevan, S.; Budoff, M.J. The role of carotid intimal thickness testing and risk prediction in the development of coronary atherosclerosis. Curr. Atheroscler. Rep. 2013, 15, 306. [Google Scholar] [CrossRef] [Green Version]
- O’Donnell, C.J.; Nabel, E.G. Genomics of cardiovascular disease. N. Engl. J. Med. 2011, 365, 2098–2109. [Google Scholar] [CrossRef]
- Vrablik, M.; Dlouha, D.; Todorovova, V.; Stefler, D.; Hubacek, J.A. Genetics of cardiovascular disease: How far are we from personalized CVD risk prediction and management? Int. J. Mol. Sci. 2021, 22, 4182. [Google Scholar] [CrossRef]
- Preuss, M.; Konig, I.R.; Thompson, J.R.; Erdmann, J.; Absher, D.; Assimes, T.L.; Blankenberg, S.; Boerwinkle, E.; Chen, L.; Cupples, L.A.; et al. Design of the Coronary ARtery DIsease Genome-Wide Replication And Meta-Analysis (CARDIoGRAM) Study: A Genome-wide association meta-analysis involving more than 22 000 cases and 60 000 controls. Circ. Cardiovasc. Genet. 2010, 3, 475–483. [Google Scholar] [CrossRef]
- Jaiswal, S.; Fontanillas, P.; Flannick, J.; Manning, A.; Grauman, P.V.; Mar, B.G.; Lindsley, R.C.; Mermel, C.H.; Burtt, N.; Chavez, A.; et al. Age-related clonal hematopoiesis associated with adverse outcomes. N. Engl. J. Med. 2014, 371, 2488–2498. [Google Scholar] [CrossRef] [Green Version]
- Jaiswal, S.; Natarajan, P.; Silver, A.J.; Gibson, C.J.; Bick, A.G.; Shvartz, E.; McConkey, M.; Gupta, N.; Gabriel, S.; Ardissino, D.; et al. Clonal hematopoiesis and risk of atherosclerotic cardiovascular disease. N. Engl. J. Med. 2017, 377, 111–121. [Google Scholar] [CrossRef]
- Senguttuvan, N.B.; Subramanian, V.; Venkatesan, V.; Muralidharan, T.R.; Sankaranarayanan, K. Clonal hematopoiesis of indeterminate potential (CHIP) and cardiovascular diseases—an updated systematic review. J. Genet. Eng. Biotechnol. 2021, 19, 105. [Google Scholar] [CrossRef]
- Papa, V.; Marracino, L.; Fortini, F.; Rizzo, P.; Campo, G.; Vaccarezza, M.; Vieceli Dalla Sega, F. Translating evidence from Clonal hematopoiesis to cardiovascular disease: A systematic review. J. Clin. Med. 2020, 9, 2480. [Google Scholar] [CrossRef]
- Vasan, R.S. Biomarkers of cardiovascular disease: Molecular basis and practical considerations. Circulation 2006, 113, 2335–2362. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Australian Absolute CVD Risk Calculator [21] | ASCVD Risk Estimator Plus [22] | Framingham General CVD Risk Score [23] | SCORE2 [24] | QRISK3 [25] | |
|---|---|---|---|---|---|
| Year | 2012 | 2013 | 2008 | 2021 | 2018 |
| Components | |||||
| Race | √ | √ | |||
| Gender | √ | √ | √ | √ | √ |
| Age | √ | √ | √ | √ | √ |
| Total cholesterol | √ | √ | √ | √ | √ |
| HDL | √ | √ | √ | √ | √ |
| LDL | √ | √ | |||
| Systolic blood pressure | √ | √ | √ | √ | √ |
| Diastolic blood pressure | √ | ||||
| Anti-hypertensives | √ | √ | √ | ||
| Diabetes | √ | √ | √ | √ | |
| Smoking | √ | √ | √ | √ | √ |
| Location | √ | √ | |||
| Others | ECG LVH | Statin Aspirin | Family history, body mass index, chronic kidney disease, SLE, migraine, atypical antipsychotics, corticosteroids, mental illness, erectile dysfunction | ||
| Age range (years) | 35–74 | 40–79 | >30 | 40–69 | 25–84 |
| Risk projection | 5-year risk | 10-year risk | 10-year risk | 10-year risk | 10-year risk |
| Endpoints assessed | MI Stroke | Nonfatal MI CHD death Fatal/nonfatal stroke | CHD death Nonfatal MI Angina Fatal/nonfatal stroke Intermittent claudication Heart failure | CHD death Nonfatal MI AnginaFatal/nonfatal stroke Intermittent claudication Coronary revascularization | CHD death Nonfatal MI AnginaFatal/nonfatal stroke Intermittent claudication Coronary revascularization |
| Webpage | https://www.cvdcheck.org.au/calculator (accessed on 1 June 2022) | https://tools.acc.org/ASCVD-Risk-Estimator-Plus/ (accessed on 1 June 2022) | https://www.ahajournals.org/doi/10.1161/circulationaha.107.699579 (accessed on 1 June 2022) | https://www.heartscore.org/en_GB (accessed on 1 June 2022) | https://qrisk.org/three/ (accessed on 1 June 2022) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, H.Y.; Burrell, L.M.; Brook, R.; Nandurkar, H.H.; Donnan, G.; Ho, P. The Need for Individualized Risk Assessment in Cardiovascular Disease. J. Pers. Med. 2022, 12, 1140. https://doi.org/10.3390/jpm12071140
Lim HY, Burrell LM, Brook R, Nandurkar HH, Donnan G, Ho P. The Need for Individualized Risk Assessment in Cardiovascular Disease. Journal of Personalized Medicine. 2022; 12(7):1140. https://doi.org/10.3390/jpm12071140
Chicago/Turabian StyleLim, Hui Yin, Louise M. Burrell, Rowena Brook, Harshal H. Nandurkar, Geoffrey Donnan, and Prahlad Ho. 2022. "The Need for Individualized Risk Assessment in Cardiovascular Disease" Journal of Personalized Medicine 12, no. 7: 1140. https://doi.org/10.3390/jpm12071140