

Results of Treating Mild to Moderate Knee Osteoarthritis with Autologous Conditioned Adipose Tissue and Leukocyte-Poor Platelet-Rich Plasma

 , ,
, ,  , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Clinical Questionnaires
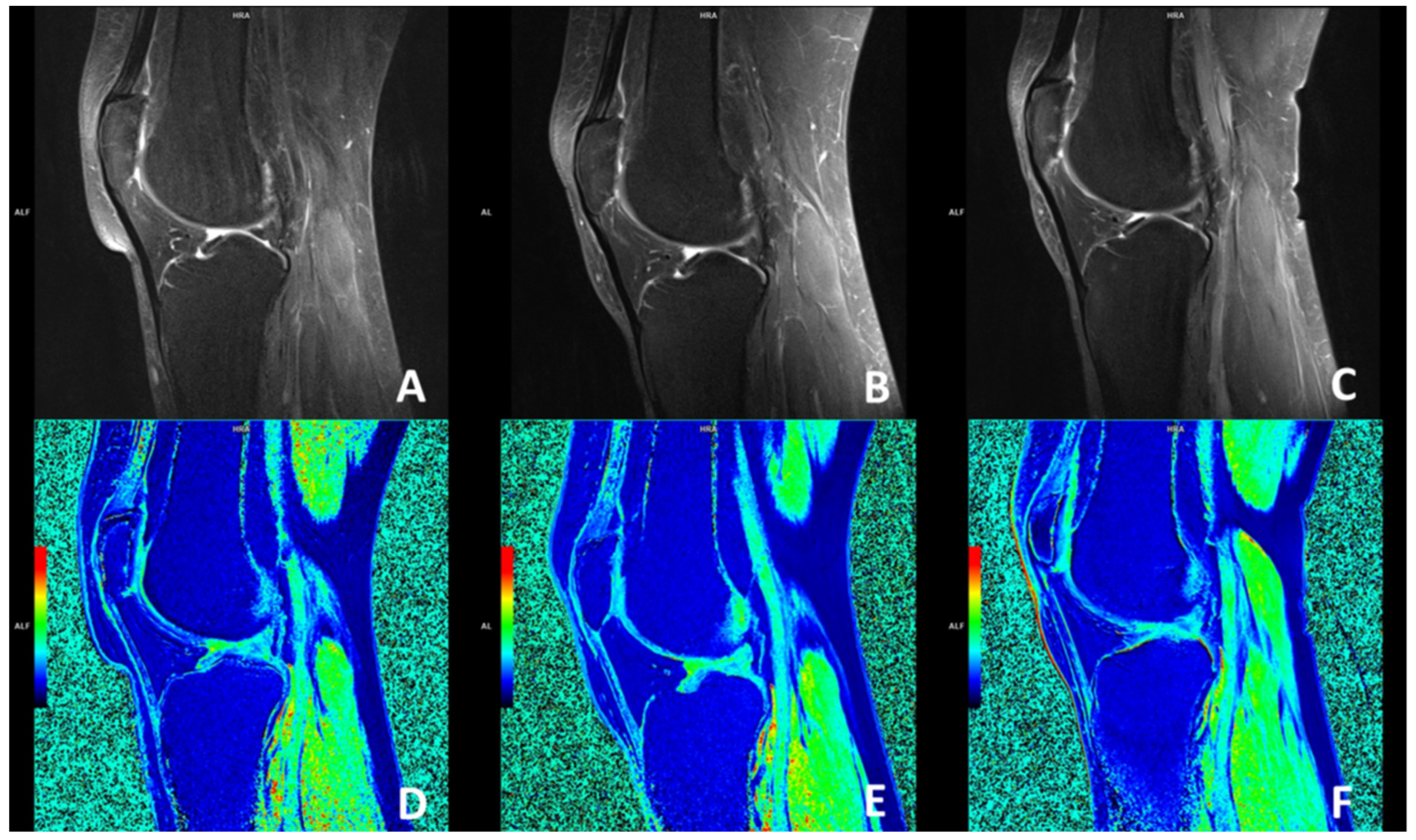
2.4. Delayed Gadolinium-Enhanced Magnetic Resonance Imaging of Cartilage (dGEMRIC) Protocol
2.5. Lipoaspiration and ACA Production
2.6. LP-PRP Protocol
2.7. Application of ACA + LP-PRP
2.8. Follow-Up Appointments
2.9. Statistical Analysis
3. Results
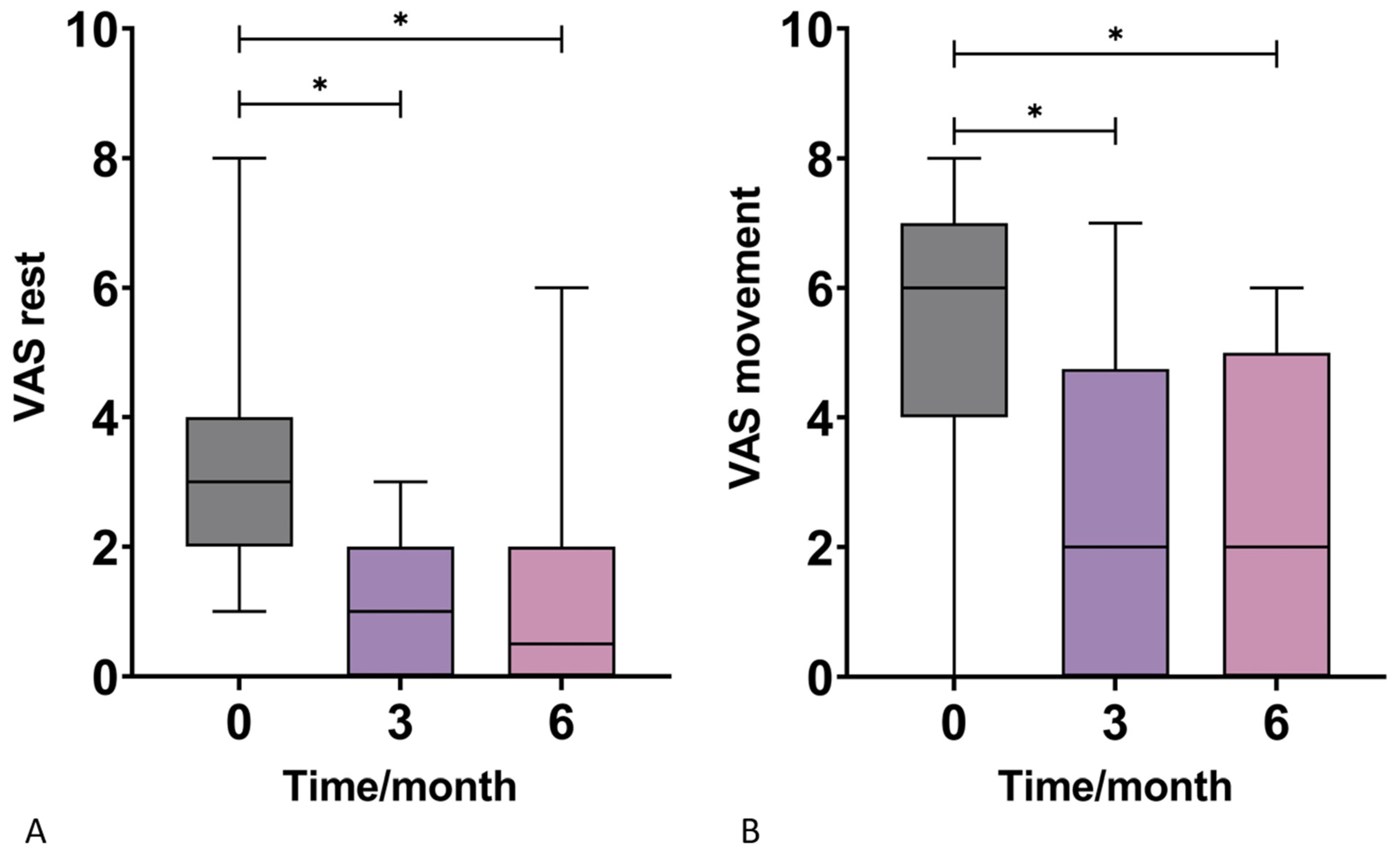
3.1. Visual Analog Scale (VAS)
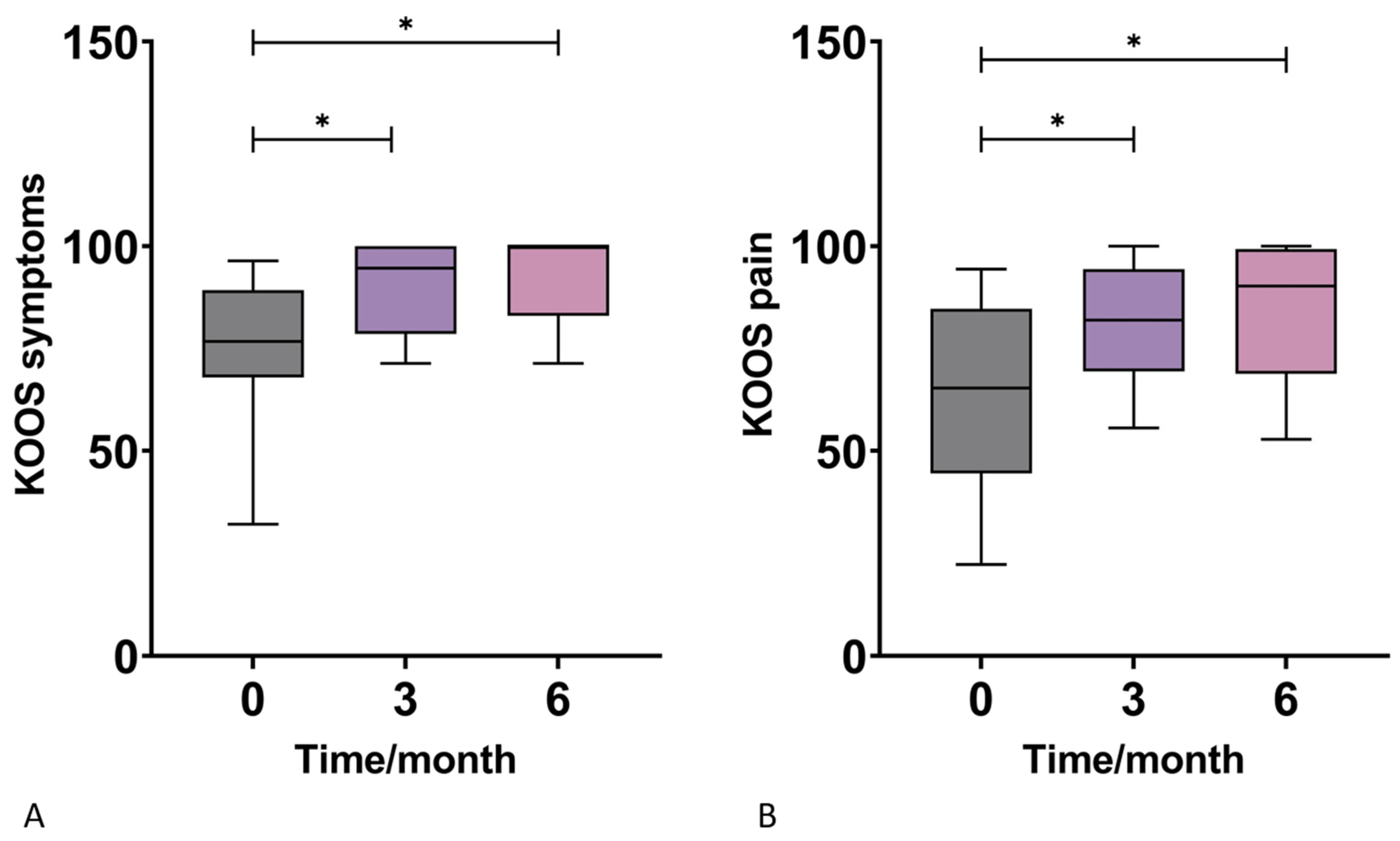
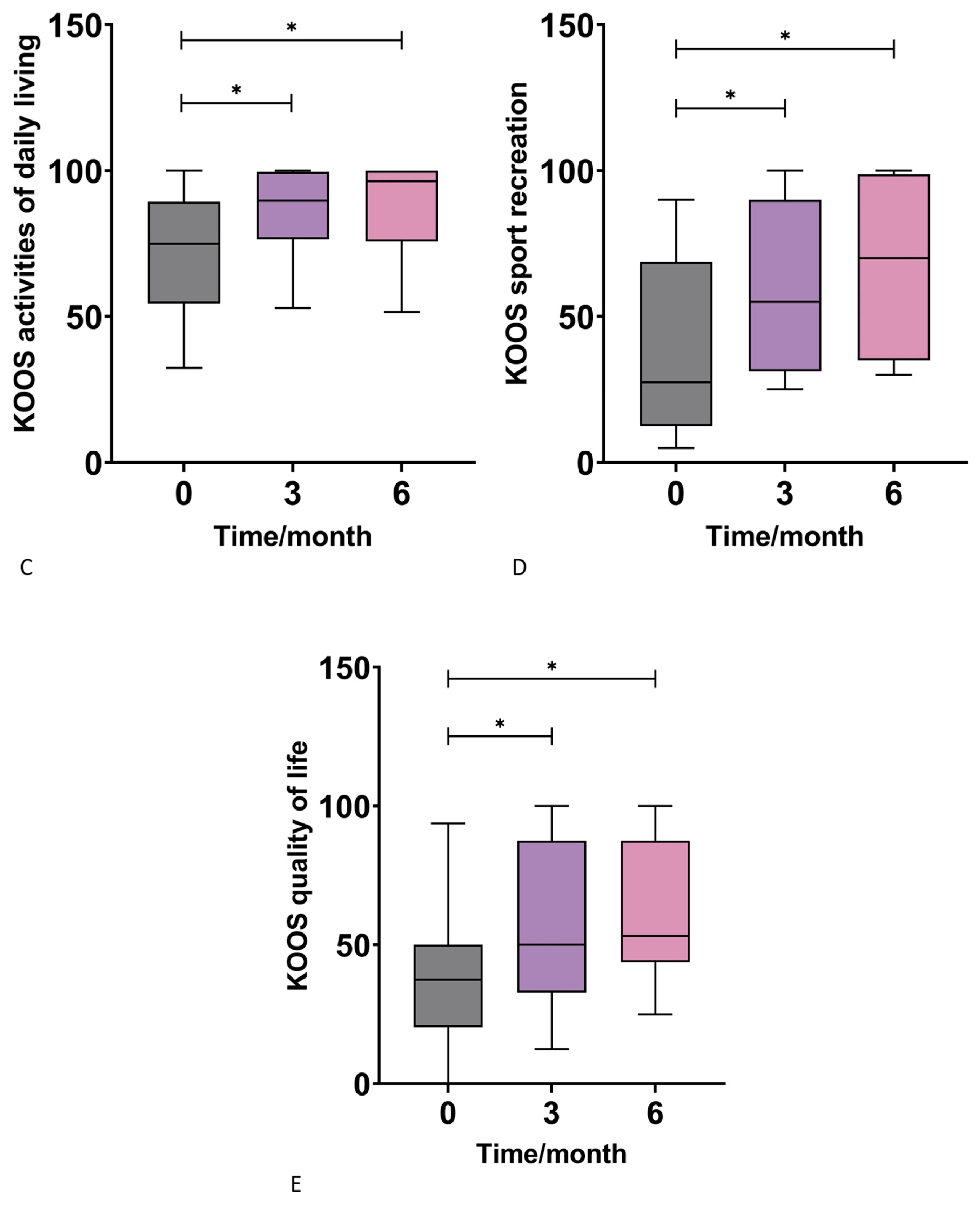
3.2. Knee Injury and Osteoarthritis Outcome Score (KOOS)
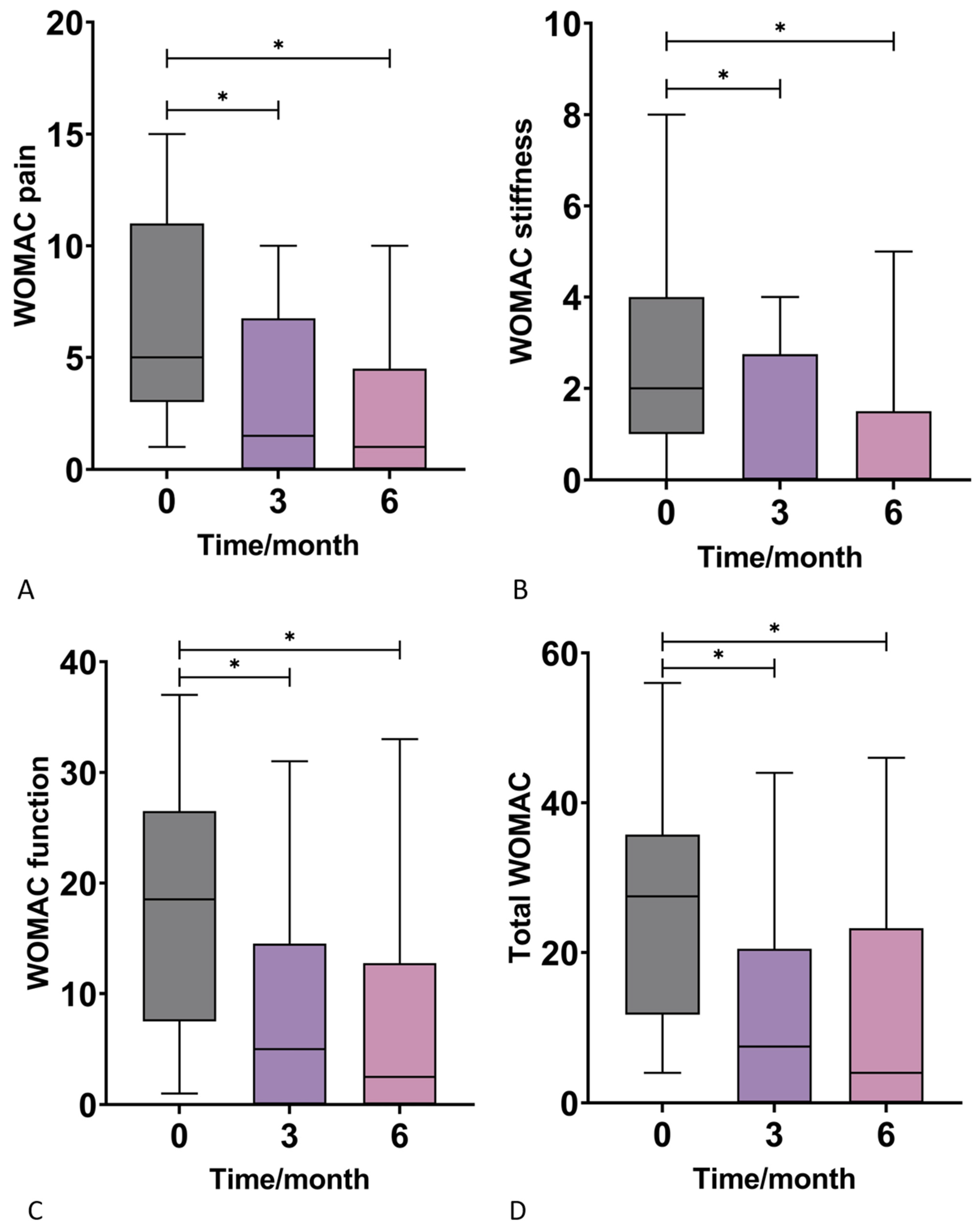
3.3. Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)
3.4. dGEMRIC
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cui, A.; Li, H.; Wang, D.; Zhong, J.; Chen, Y.; Lu, H. EClinicalMedicine Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. EClinicalMedicine 2020, 29, 100587. [Google Scholar] [CrossRef] [PubMed]
- Hunter, D.J.; Bierma-Zeinstra, S. Osteoarthritis. Lancet 2019, 393, 1745–1759. [Google Scholar] [CrossRef] [PubMed]
- Uhlig, T.; Slatkowsky-Christensen, B.; Moe, R.H.; Kvien, T.K. The burden of osteoarthritis: The societal and the patient perspective. Therapy 2010, 7, 605–619. [Google Scholar] [CrossRef]
- Losina, E.; Paltiel, A.D.; Weinstein, A.M.; Yelin, E.; Hunter, D.J.; Chen, S.P.; Klara, K.; Suter, L.G.; Solomon, D.H.; Burbine, S.A.; et al. Lifetime medical costs of knee osteoarthritis management in the United States: Impact of extending indications for total knee arthroplasty. Arthritis Care Res. 2015, 67, 203–215. [Google Scholar] [CrossRef] [Green Version]
- Lanes, S.F.; Lanza, L.L.; Radensky, P.W.; Yood, R.A.; Meenan, R.F.; Walker, A.M.; Dreyer, N.A. Resource utilization and cost of care for rheumatoid arthritis and osteoarthritis in a managed care setting: The importance of drug and surgery costs. Arthritis Rheum. 1997, 40, 1475–1481. [Google Scholar] [CrossRef]
- Primorac, D.; Molnar, V.; Rod, E.; Jeleč, Ž.; Čukelj, F.; Matišić, V.; Vrdoljak, T.; Hudetz, D.; Hajsok, H.; Borić, I. Knee Osteoarthritis: A Review of Pathogenesis and State-Of-The-Art Non-Operative Therapeutic Considerations. Genes 2020, 11, 854. [Google Scholar] [CrossRef]
- Hudetz, D.; Borić, I.; Rod, E.; Jeleč, Ž.; Kunovac, B.; Polašek, O.; Vrdoljak, T.; Plečko, M.; Skelin, A.; Polančec, D.; et al. Early results of intra-articular micro-fragmented lipoaspirate treatment in patients with late stages knee osteoarthritis: A prospective study. Croat. Med. J. 2019, 60, 227–236. [Google Scholar] [CrossRef]
- Hudetz, D.; Jeleč, Ž.; Rod, E.; Borić, I.; Plečko, M.; Primorac, D. The Future of Cartilage Repair. Pers. Med. Healthc. Syst. 2019, 5, 375–411. [Google Scholar] [CrossRef]
- Hudetz, D.; Borić, I.; Rod, E.; Jeleč, Ž.; Radić, A.; Vrdoljak, T.; Skelin, A.; Lauc, G.; Trbojević-Akmačić, I.; Plečko, M.; et al. The effect of intra-articular injection of autologous microfragmented fat tissue on proteoglycan synthesis in patients with knee osteoarthritis. Genes 2017, 8, 270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borić, I.; Hudetz, D.; Rod, E.; Jeleč, Ž.; Vrdoljak, T.; Skelin, A.; Polašek, O.; Plečko, M.; Trbojević-Akmačić, I.; Lauc, G.; et al. A 24-month follow-up study of the effect of intra-articular injection of autologous microfragmented fat tissue on proteoglycan synthesis in patients with knee osteoarthritis. Genes 2019, 10, 1051. [Google Scholar] [CrossRef]
- Chaput, B.; Bertheuil, N.; Escubes, M.; Grolleau, J.L.; Garrido, I.; Laloze, J.; Espagnolle, N.; Casteilla, L.; Sensebé, L.; Varin, A. Mechanically Isolated Stromal Vascular Fraction Provides a Valid and Useful Collagenase-Free Alternative Technique: A Comparative Study. Plast. Reconstr. Surg. 2016, 138, 807–819. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.S.; Choi, Y.J.; Suh, D.S.; Heo, D.B.; Kim, Y.I.; Ryu, J.S.; Koh, Y.G. Mesenchymal stem cell implantation in osteoarthritic knees: Is fibrin glue effective as a scaffold? Am. J. Sport. Med. 2015, 43, 176–185. [Google Scholar] [CrossRef] [PubMed]
- Tsubosaka, M.; Matsumoto, T.; Sobajima, S.; Matsushita, T.; Iwaguro, H.; Kuroda, R. The influence of adipose-derived stromal vascular fraction cells on the treatment of knee osteoarthritis. BMC Musculoskelet. Disord. 2020, 21, 207. [Google Scholar] [CrossRef] [PubMed]
- Hong, Z.; Chen, J.; Zhang, S.; Zhao, C.; Bi, M.; Chen, X.; Bi, Q. Intra-articular injection of autologous adipose-derived stromal vascular fractions for knee osteoarthritis: A double-blind randomized self-controlled trial. Int. Orthop. 2019, 43, 1123–1134. [Google Scholar] [CrossRef] [PubMed]
- Fodor, P.B.; Paulseth, S.G. Adipose Derived Stromal Cell (ADSC) Injections for Pain Management of Osteoarthritis in the Human Knee Joint. Aesthetic Surg. J. 2016, 36, 229–236. [Google Scholar] [CrossRef] [Green Version]
- Marx, R.E. Platelet-Rich Plasma (PRP): What Is PRP and What Is Not PRP? Implant Dent. 2001, 10, 225–228. [Google Scholar] [CrossRef] [Green Version]
- Everts, P.; Onishi, K.; Jayaram, P.; Lana, J.F.; Mautner, K. Platelet-rich plasma: New performance understandings and therapeutic considerations in 2020. Int. J. Mol. Sci. 2020, 21, 7794. [Google Scholar] [CrossRef]
- Mazzucco, L.; Balbo, V.; Cattana, E.; Guaschino, R.; Borzini, P. Not every PRP-gel is born equal Evaluation of growth factor availability for tissues through four PRP-gel preparations: Fibrinet®, RegenPRP-Kit®, Plateltex® and one manual procedure. Vox Sang. 2009, 97, 110–118. [Google Scholar] [CrossRef]
- Degen, R.M.; Bernard, J.A.; Oliver, K.S.; Dines, J.S. Commercial Separation Systems Designed for Preparation of Platelet-Rich Plasma Yield Differences in Cellular Composition. HSS J. 2017, 13, 75–80. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.Z.; Rui, Y.F.; Tan, Q.; Wang, C. Enhancing intervertebral disc repair and regeneration through biology: Platelet-rich plasma as an alternative strategy. Arthritis Res. Ther. 2013, 15, 220. [Google Scholar] [CrossRef] [PubMed]
- Knezevic, N.N.; Candido, K.D.; Desai, R.; Kaye, A.D. Is Platelet-Rich Plasma a Future Therapy in Pain Management? Med. Clin. N. Am. 2016, 100, 199–217. [Google Scholar] [CrossRef] [PubMed]
- Migliorini, F.; Driessen, A.; Quack, V.; Sippel, N.; Cooper, B.; El Mansy, Y.; Tingart, M.; Eschweiler, J. Comparison between intra-articular infiltrations of placebo, steroids, hyaluronic and PRP for knee osteoarthritis: A Bayesian network meta-analysis. Arch. Orthop. Trauma Surg. 2021, 141, 1473–1490. [Google Scholar] [CrossRef]
- Koh, Y.G.; Choi, Y.J. Infrapatellar fat pad-derived mesenchymal stem cell therapy for knee osteoarthritis. Knee 2012, 19, 902–907. [Google Scholar] [CrossRef] [PubMed]
- Koh, Y.G.; Choi, Y.J.; Kwon, S.K.; Kim, Y.S.; Yeo, J.E. Clinical results and second-look arthroscopic findings after treatment with adipose-derived stem cells for knee osteoarthritis. Knee Surg. Sport. Traumatol. Arthrosc. 2015, 23, 1308–1316. [Google Scholar] [CrossRef] [PubMed]
- Pak, J.; Chang, J.J.; Lee, J.H.; Lee, S.H. Safety reporting on implantation of autologous adipose tissue-derived stem cells with platelet-rich plasma into human articular joints. BMC Musculoskelet. Disord. 2013, 14, 337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Pham, P.; Bui, K.H.-T.; Duong, T.D.; Nguyen, N.T.; Nguyen, T.D.; Le, V.T.; Mai, V.T.; Phan, N.L.-C.; Le, D.M.; Ngoc, N.K. Symptomatic knee osteoarthritis treatment using autologous adipose derived stem cells and platelet-rich plasma: A clinical study. Biomed. Res. Ther. 2014, 1, 2–8. [Google Scholar] [CrossRef]
- Bansal, H.; Comella, K.; Leon, J.; Verma, P.; Agrawal, D.; Koka, P.; Ichim, T. Intra-articular injection in the knee of adipose derived stromal cells (stromal vascular fraction) and platelet rich plasma for osteoarthritis. J. Transl. Med. 2017, 15, 141. [Google Scholar] [CrossRef] [Green Version]
- Schouten, W.R.; Arkenbosch, J.H.C.; van der Woude, C.J.; de Vries, A.C.; Stevens, H.P.; Fuhler, G.M.; Dwarkasing, R.S.; van Ruler, O.; de Graaf, E.J.R. Efficacy and safety of autologous adipose-derived stromal vascular fraction enriched with platelet-rich plasma in flap repair of transsphincteric cryptoglandular fistulas. Tech. Coloproctol. 2021, 25, 1301–1309. [Google Scholar] [CrossRef]
- DiMarino, A.M.; Caplan, A.I.; Bonfield, T.L. Mesenchymal Stem Cells in Tissue Repair. Front. Immunol. 2013, 4, 201. [Google Scholar] [CrossRef] [Green Version]
- Molnar, V.; Pavelić, E.; Vrdoljak, K.; Čemerin, M.; Klarić, E.; Matišić, V.; Bjelica, R.; Brlek, P.; Kovačić, I.; Tremolada, C.; et al. Mesenchymal Stem Cell Mechanisms of Action and Clinical Effects in Osteoarthritis: A Narrative Review. Genes 2022, 13, 949. [Google Scholar] [CrossRef]
- Baria, M.R.; Miller, M.M.; Borchers, J.; Desmond, S.; Onate, J.; Magnussen, R.; Vasileff, W.K.; Flanigan, D.; Kaeding, C.; Durgam, S. High Intensity Interval Exercise Increases Platelet and Transforming Growth Factor-β Yield in Platelet-Rich Plasma. PM&R 2020, 12, 1244–1250. [Google Scholar] [CrossRef]
- Zenic, L.; Polancec, D.; Hudetz, D.; Jelec, Z.; Rod, E.; Vidovic, D.; Staresinic, M.; Sabalic, S.; Vrdoljak, T.; Petrovic, T.; et al. Polychromatic Flow Cytometric Analysis of Stromal Vascular Fraction from Lipoaspirate and Microfragmented Counterparts Reveals Sex-Related Immunophenotype Differences. Genes 2021, 12, 1999. [Google Scholar] [CrossRef] [PubMed]
- Primorac, D.; Molnar, V.; Matišić, V.; Hudetz, D.; Jeleč, Ž.; Rod, E.; Čukelj, F.; Vidović, D.; Vrdoljak, T.; Dobričić, B.; et al. Comprehensive review of knee osteoarthritis pharmacological treatment and the latest professional societies’ guidelines. Pharmaceuticals 2021, 14, 205. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Kadamb, A.G.; Kadamb, K.G. Mesenchymal or maintenance stem cell & understanding their role in osteoarthritis of the knee joint: A review article. Arch. Bone Jt. Surg. 2020, 8, 560–569. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.K.; Chullikana, A.; Rengasamy, M.; Shetty, N.; Pandey, V.; Agarwal, V.; Wagh, S.Y.; Vellotare, P.K.; Damodaran, D.; Viswanathan, P.; et al. Efficacy and safety of adult human bone marrow-derived, cultured, pooled, allogeneic mesenchymal stromal cells (Stempeucel®): Preclinical and clinical trial in osteoarthritis of the knee joint. Arthritis Res. Ther. 2016, 18, 301. [Google Scholar] [CrossRef] [Green Version]
- Buzaboon, N.; Alshammary, S. Clinical Applicability of Adult Human Mesenchymal Stem Cell Therapy in the Treatment of Knee Osteoarthritis. Stem Cells Cloning Adv. Appl. 2020, 13, 117–136. [Google Scholar] [CrossRef]
- Chahal, J.; Gómez-Aristizábal, A.; Shestopaloff, K.; Bhatt, S.; Chaboureau, A.; Fazio, A.; Chisholm, J.; Weston, A.; Chiovitti, J.; Keating, A.; et al. Bone Marrow Mesenchymal Stromal Cell Treatment in Patients with Osteoarthritis Results in Overall Improvement in Pain and Symptoms and Reduces Synovial Inflammation. Stem Cells Transl. Med. 2019, 8, 746–757. [Google Scholar] [CrossRef] [Green Version]
- Crisan, M.; Yap, S.; Casteilla, L.; Chen, C.-W.; Corselli, M.; Park, T.S.; Andriolo, G.; Sun, B.; Zheng, B.; Zhang, L.; et al. A Perivascular Origin for Mesenchymal Stem Cells in Multiple Human Organs. Cell Stem Cell 2008, 3, 301–313. [Google Scholar] [CrossRef] [Green Version]
- Su, X.; Wu, Z.; Chen, J.; Wu, N.; Ma, P.; Xia, Z.; Jiang, C.; Ye, Z.; Liu, S.; Liu, J.; et al. CD146 as a new marker for an increased chondroprogenitor cell sub-population in the later stages of osteoarthritis. J. Orthop. Res. 2015, 33, 84–91. [Google Scholar] [CrossRef]
- Tremolada, C. Mesenchymal Stromal Cells and Micro Fragmented Adipose Tissue: New Horizons of Effectiveness of Lipogems. J. Stem Cells Res. Dev. Ther. 2019, 5, 017. [Google Scholar] [CrossRef]
- Filardo, G.; Tschon, M.; Perdisa, F.; Brogini, S.; Cavallo, C.; Desando, G.; Giavaresi, G.; Grigolo, B.; Martini, L.; Nicoli Aldini, N.; et al. Micro-fragmentation is a valid alternative to cell expansion and enzymatic digestion of adipose tissue for the treatment of knee osteoarthritis: A comparative preclinical study. Knee Surg. Sport. Traumatol. Arthrosc. 2022, 30, 773–781. [Google Scholar] [CrossRef] [PubMed]
- Michalek, J.; Moster, R.; Lukac, L.; Proefrock, K.; Petrasovic, M.; Rybar, J.; Chaloupka, A.; Darinskas, A.; Michalek, J.; Kristek, J.; et al. Stromal Vascular Fraction Cells of Adipose and Connective Tissue in People with Osteoarthritis: A Case Control Prospective Multi-Centric Non-Randomized Study. Glob. Surg. 2017, 3, 163. [Google Scholar] [CrossRef]
- Belk, J.W.; Kraeutler, M.J.; Houck, D.A.; Goodrich, J.A.; Dragoo, J.L.; McCarty, E.C. Platelet-Rich Plasma Versus Hyaluronic Acid for Knee Osteoarthritis: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Am. J. Sport. Med. 2021, 49, 249–260. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient inclusion criteria |
|
| Patient exclusion criteria |
|
| T0 | T3 | T6 | p Value (Kruskal-Wallis Test) | ||
|---|---|---|---|---|---|
| VAS-Rest | M | 3.00 | 1.00 | 0.50 | <0.001 |
| IQR | 2.00 | 2.00 | 2.00 | ||
| SD | ±1.797 | ±1.063 | ±1.628 | ||
| VAS-Active | M | 6.00 | 2.00 | 2.00 | 0.002 |
| IQR | 3.00 | 4.75 | 5.00 | ||
| SD | ±2.066 | ±2.613 | ±2.277 | ||
| KOOS Symptoms | M | 76.79 | 94.64 | 100.00 | 0.001 |
| IQR | 21.43 | 21.43 | 16.96 | ||
| SD | ±16.24 | ±10.93 | ±9.873 | ||
| KOOS Pain | M | 65.28 | 81.94 | 90.28 | 0.017 |
| IQR | 40.28 | 25.00 | 30.56 | ||
| SD | ±21.42 | ±15.00 | ±17.22 | ||
| KOOS Activities of Daily Living | M | 75.00 | 89.71 | 96.32 | 0.014 |
| IQR | 34.93 | 23.16 | 24.26 | ||
| SD | ±20.00 | ±14.91 | ±15.37 | ||
| KOOS Sport and Recreation Function | M | 27.50 | 55.00 | 70.00 | 0.006 |
| IQR | 56.25 | 58.75 | 63.75 | ||
| SD | ±28.72 | ±29.71 | ±29.42 | ||
| KOOS Quality of Life | M | 37.50 | 50.00 | 53.13 | 0.064 |
| IQR | 29.69 | 54.69 | 43.75 | ||
| SD | ±26.81 | ±29.75 | ±27.28 | ||
| WOMAC Pain | M | 5.00 | 1.50 | 1.00 | 0.009 |
| IQR | 8.00 | 6.75 | 4.50 | ||
| SD | ±4.423 | ±3.637 | ±3.856 | ||
| WOMAC Stiffness | M | 2.00 | 0.00 | 0.00 | 0.014 |
| IQR | 3.00 | 2.75 | 1.50 | ||
| SD | ±2.160 | ±1.455 | ±1.559 | ||
| WOMAC Function | M | 18.50 | 5.00 | 2.50 | 0.006 |
| IQR | 19.00 | 14.50 | 12.75 | ||
| SD | ±10.92 | ±9.793 | ±9.858 | ||
| Total WOMAC | M | 27.50 | 7.50 | 4.00 | 0.005 |
| IQR | 24.00 | 20.50 | 23.25 | ||
| SD | ±15.75 | ±13.87 | ±14.08 | ||
| T0 | T3 | T6 | p value (Friedman test) | ||
| VAS-Rest | M | 3 | 1 | 0.5 | <0.0001 |
| IQR | 2 | 2 | 2 | ||
| SD | ±1.797 | ±1.063 | ±1.628 | ||
| VAS-Active | M | 6 | 2 | 2 | <0.0001 |
| IQR | 3 | 4.75 | 5 | ||
| SD | ±2.066 | ±2.613 | ±2.277 | ||
| KOOS Symptoms | M | 76.79 | 94.64 | 100 | <0.0001 |
| IQR | 21.43 | 21.43 | 16.96 | ||
| SD | ±16.24 | ±10.93 | ±9.873 | ||
| KOOS Pain | M | 65.28 | 81.94 | 90.28 | <0.0001 |
| IQR | 40.28 | 25 | 30.56 | ||
| SD | ±21.42 | ±15.00 | ±17.22 | ||
| KOOS Activities of Daily Living | M | 75 | 89.71 | 96.32 | 0.0001 |
| IQR | 34.93 | 23.16 | 24.26 | ||
| SD | ±20.00 | ±14.91 | ±15.37 | ||
| KOOS Sport and Recreation Function | M | 27.5 | 55 | 70 | <0.0001 |
| IQR | 56.25 | 58.75 | 63.75 | ||
| SD | ±28.72 | ±29.71 | ±29.42 | ||
| KOOS Quality of Life | M | 37.5 | 50 | 53.13 | 0.0004 |
| IQR | 29.69 | 54.69 | 43.75 | ||
| SD | ±26.81 | ±29.75 | ±27.28 | ||
| WOMAC Pain | M | 5 | 1.5 | 1 | <0.0001 |
| IQR | 8 | 6.75 | 4.5 | ||
| SD | ±4.423 | ±3.637 | ±3.856 | ||
| WOMAC Stiffness | M | 2 | 0 | 0 | <0.0001 |
| IQR | 3 | 2.75 | 1.5 | ||
| SD | ±2.160 | ±1.455 | ±1.559 | ||
| WOMAC Function | M | 18.5 | 5 | 2.5 | 0.0003 |
| IQR | 19 | 14.5 | 12.75 | ||
| SD | ±10.92 | ±9.793 | ±9.858 | ||
| Total WOMAC | M | 27.5 | 7.5 | 4 | 0.0002 |
| IQR | 24 | 20.5 | 23.25 | ||
| SD | ±15.75 | ±13.87 | ±14.08 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molnar, V.; Pavelić, E.; Jeleč, Ž.; Brlek, P.; Matišić, V.; Borić, I.; Hudetz, D.; Rod, E.; Vidović, D.; Starčević, N.; et al. Results of Treating Mild to Moderate Knee Osteoarthritis with Autologous Conditioned Adipose Tissue and Leukocyte-Poor Platelet-Rich Plasma. J. Pers. Med. 2023, 13, 47. https://doi.org/10.3390/jpm13010047
Molnar V, Pavelić E, Jeleč Ž, Brlek P, Matišić V, Borić I, Hudetz D, Rod E, Vidović D, Starčević N, et al. Results of Treating Mild to Moderate Knee Osteoarthritis with Autologous Conditioned Adipose Tissue and Leukocyte-Poor Platelet-Rich Plasma. Journal of Personalized Medicine. 2023; 13(1):47. https://doi.org/10.3390/jpm13010047
Chicago/Turabian StyleMolnar, Vilim, Eduard Pavelić, Željko Jeleč, Petar Brlek, Vid Matišić, Igor Borić, Damir Hudetz, Eduard Rod, Dinko Vidović, Neven Starčević, and et al. 2023. "Results of Treating Mild to Moderate Knee Osteoarthritis with Autologous Conditioned Adipose Tissue and Leukocyte-Poor Platelet-Rich Plasma" Journal of Personalized Medicine 13, no. 1: 47. https://doi.org/10.3390/jpm13010047
APA StyleMolnar, V., Pavelić, E., Jeleč, Ž., Brlek, P., Matišić, V., Borić, I., Hudetz, D., Rod, E., Vidović, D., Starčević, N., Čemerin, M., Karli, D. C., & Primorac, D. (2023). Results of Treating Mild to Moderate Knee Osteoarthritis with Autologous Conditioned Adipose Tissue and Leukocyte-Poor Platelet-Rich Plasma. Journal of Personalized Medicine, 13(1), 47. https://doi.org/10.3390/jpm13010047