

Preoperative Perforator Mapping in DIEP Flaps for Breast Reconstruction. The Impact of New Contrast-Enhanced Ultrasound Techniques
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ultrasound Examinations
- A 2–8 MHz transducer was utilized with settings aligned to the depiction of peripheral arteries. First, large vessels, including the external and internal iliac arteries, were identified, followed by the identification of the origin of the deep inferior epigastric arteries (DIEA).
- Settings were then adjusted in order to visualize lower-flow arterial vessels. Complete PM then included the following:
- (a)
- (b)
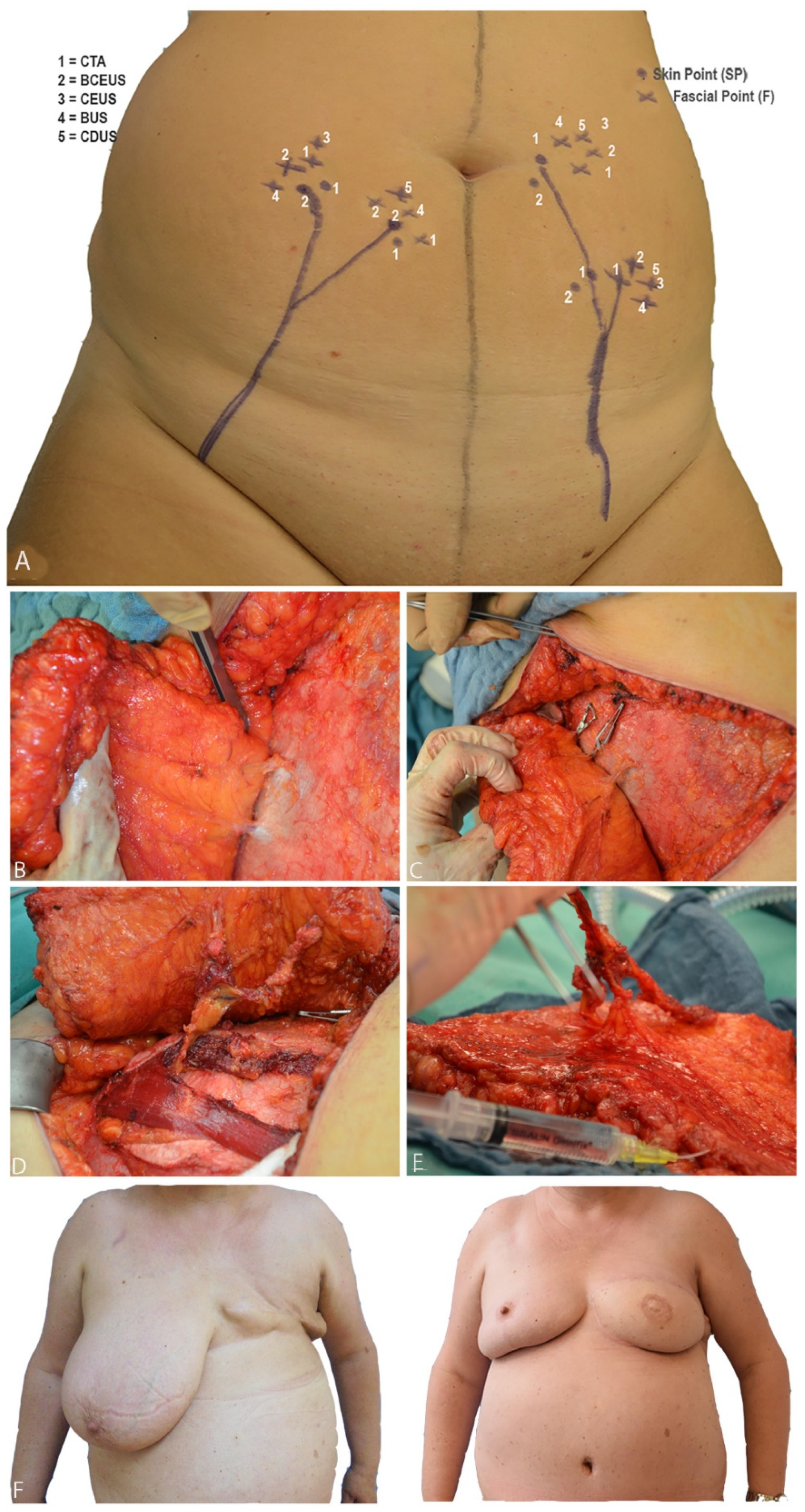
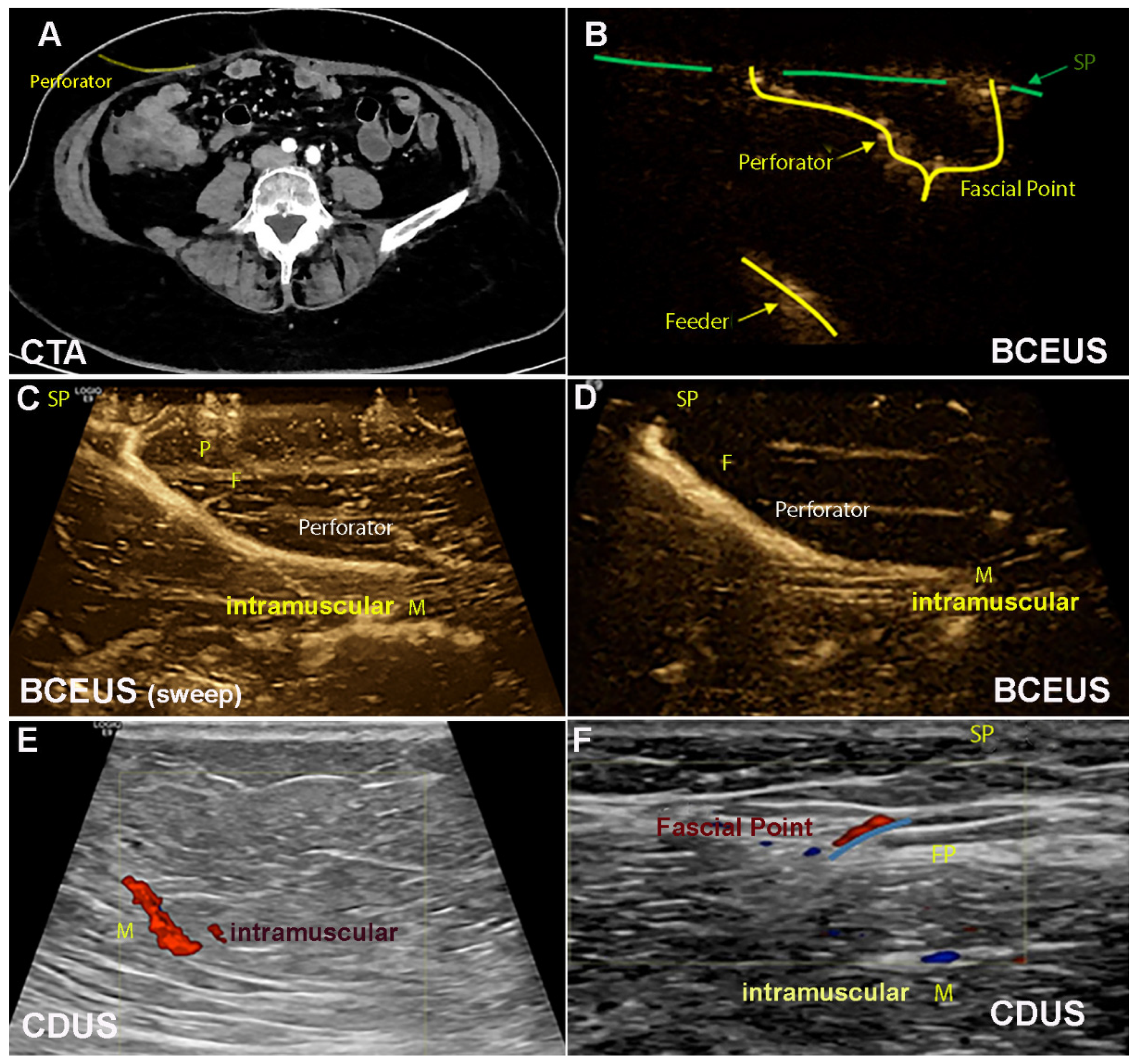
- F was then analyzed, including P and SP (Supplementary Videos S1 and S2, Figure 2). PM was performed with each technique, namely CDUS, CEUS, BUS and BCEUS and was subsequently documented and recorded by cine loops and freeze frames and traced to the skin (Table 1, Table 2, Table 3, Table 4, Table 5 and Table 6, Figure 2, Figure 3 and Figure 4). For CEUS and BCEUS, the contrast agent SonoVue (Bracco®) was prepared according to the guidelines provided [21,22]. The contrast agent was fully dissolved in 15 mL of saline. An amount of 2 mL was injected intravenously, followed by a bolus of 10 mL saline. The blood flow signal was enhanced without excessive overflow [22]. It was then evaluated whether the course of F, P and SP could be visualized with clear delineation (Figure 2 and Figure 4).
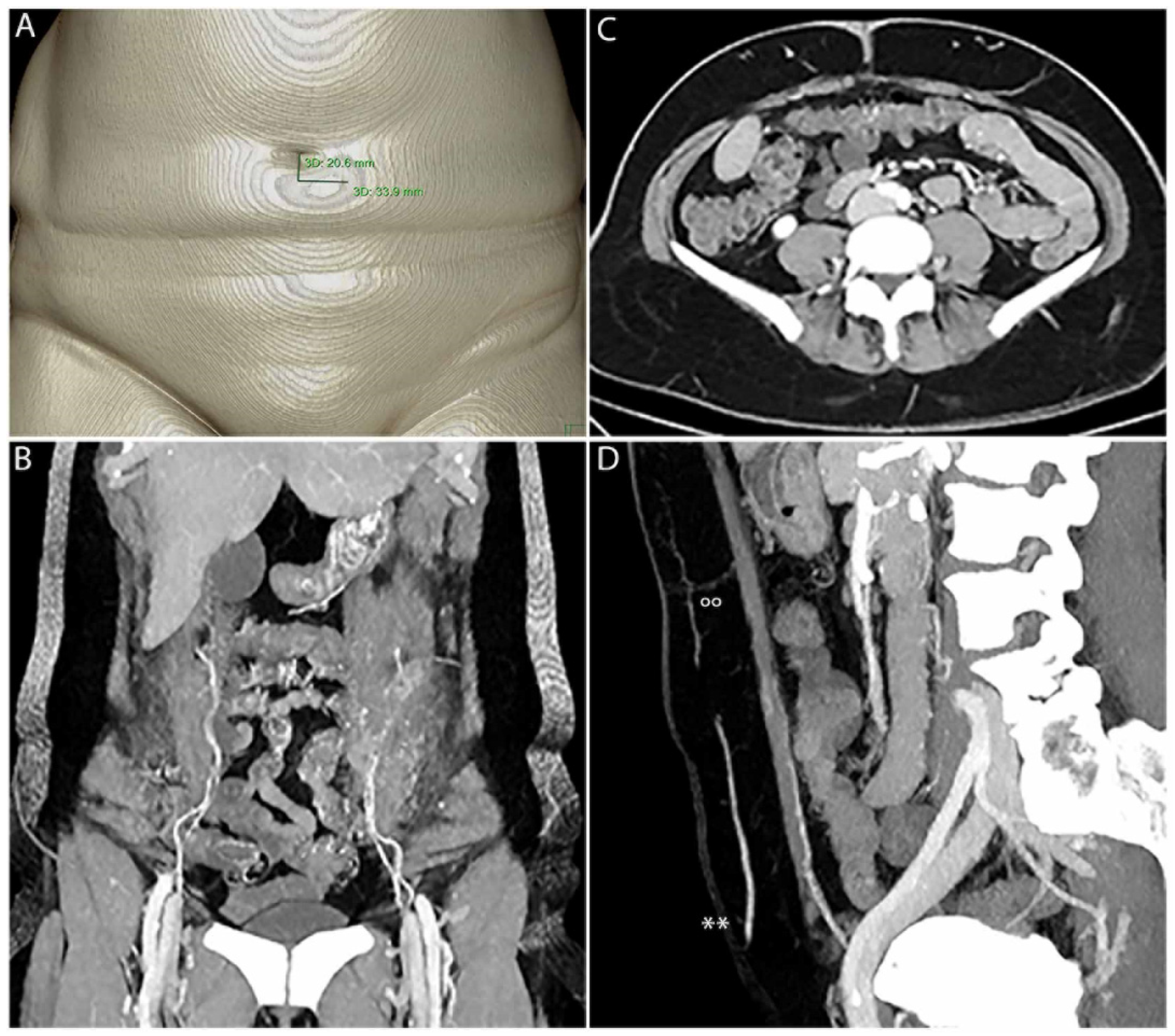
2.2. Computed Tomographic Angiography
2.3. Comparison Ultrasound Techniques versus CT-Angiography
- Precision of perforator mapping.
- Number of perforators detected at the fascial level (F).
- Delineation and diagnostic efficiency of the ultrasound modes compared to CTA.
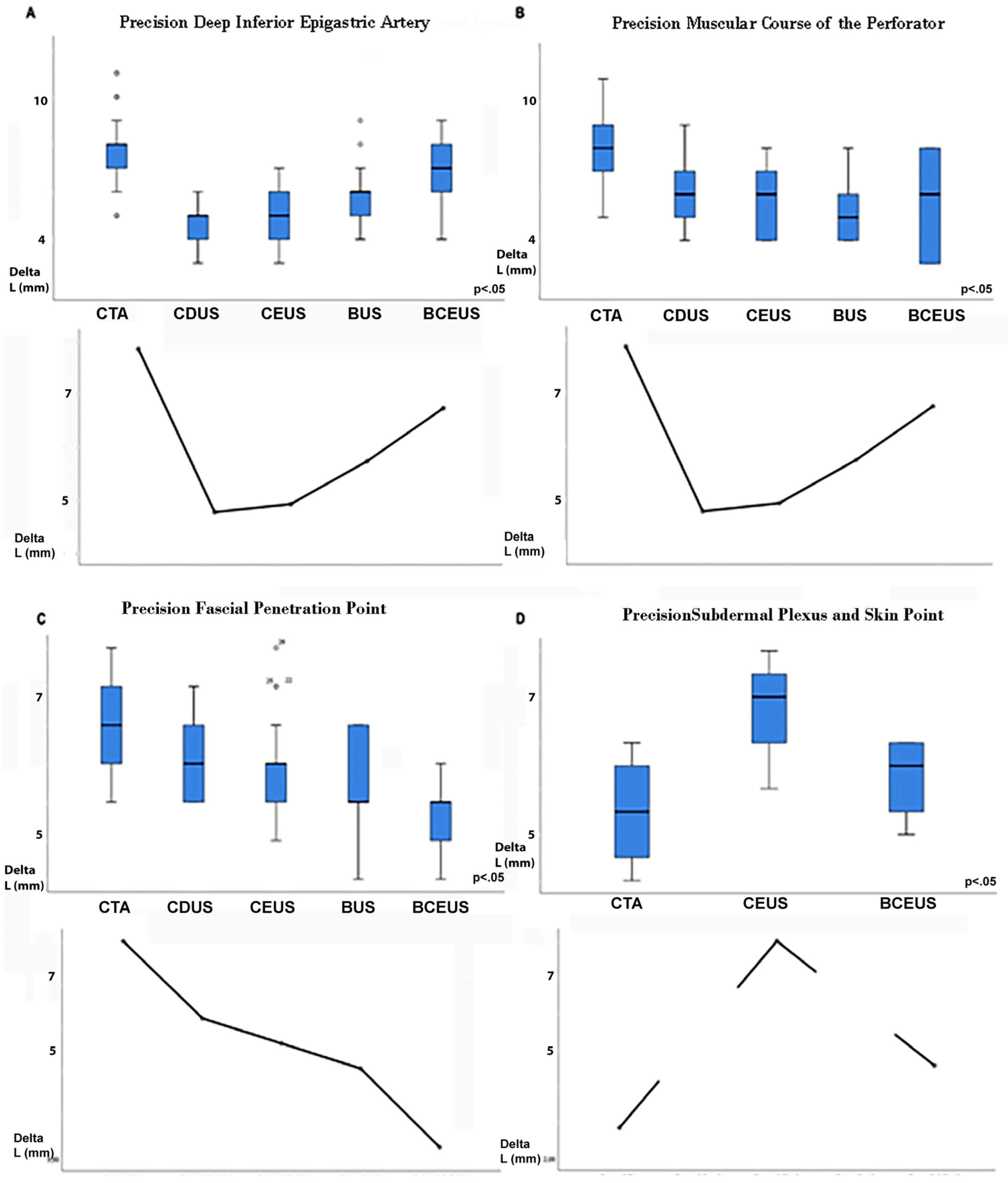
2.3.1. Precision of Perforator Mapping
2.3.2. Number of Perforators Detected at the Fascial Level (F)
2.3.3. Delineation and Diagnostic Efficiency Compared to CTA
2.4. Statistical Analysis
3. Results
3.1. Precision of PM
3.1.1. Number of Perforators Detected with Each Technique at the Fascial Level (F)
3.1.2. Delineation and Diagnostic Strength of the Ultrasound Modes
- PM should be started at the DIEA (origin). Then, M should be displayed. Therefore, we recommend CDUS, since contrast-enhanced techniques (BCEUS and CEUS) were not necessary for better diagnostic efficiency (Table 5).
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Holmstroem, H. The free abdominoplasty flap and its use in breast reconstruction. An experimental study and clinical case report. Scand. J. Plast. Reconstr. Surg. 1979, 13, 423–427. [Google Scholar] [CrossRef] [PubMed]
- Robbins, T.H. Post-mastectomy breast reconstruction using a rectus abdominis musculocutaneous island flap. Br. J. Plast. Surg. 1981, 34, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Hartrampf, C.R.; Scheflan, M.; Black, P.W.; Hartrampf, C.R. Breast reconstruction with a transverse abdominal island flap. Plast. Reconstr. Surg. 1982, 69, 216–225. [Google Scholar] [CrossRef] [PubMed]
- Seth, A.K.; Koolen, P.G.L.; Sultan, S.M.; Lee, B.T.; Erhard, H.A.; Greenspun, D.T. Unilateral Autologous Breast Reconstruction with Bi-pedicled, Conjoined Deep Inferior Epigastric Perforator Flaps. J. Reconstr. Microsurg. 2019, 35, 145–155. [Google Scholar] [CrossRef]
- Kaplan, J.L.; Allen, R.J. Cost based comparison between perforator flaps and TRAM flaps for breast reconstruction. Plast. Reconstr. Surg. 2000, 105, 943–948. [Google Scholar] [CrossRef]
- Ireton, J.E.; Lakhiani, C.; Saint-Cyr, M. Vascular anatomy of the deep inferior epigastric artery perforator flap: A systematic review. Plast. Reconstr. Surg. 2014, 134, 810–821. [Google Scholar] [CrossRef]
- Kiely, J.; Kumar, M.; Wade, R.G. The accuracy of different modalities of perforator mapping for unilateral DIEP breast reconstruction: A systematic review and meta-analysis. J. Plast. Reconstr. Aesthet. Surg. 2021, 74, 945–956. [Google Scholar] [CrossRef]
- Mijuskovic, B.; Tremp, M.; Heimer, M.M.; Boll, D.; Aschwanden, M.; Zeindler, J.; Kurzeder, C.; Schaefer, D.J.; Haug, M.D.; Kappos, E.A. Color Doppler ultrasound and computed tomographic angiography for perforator mapping in DIEP flap breast reconstruction revisited: A cohort study. J. Plast. Reconstr. Aesthet. Surg. 2019, 72, 1632–1639. [Google Scholar] [CrossRef]
- Blondeel, P.N.; Beyens, G.; Verhaeghe, R.; Van Landuyt, K.; Tonnard, P.; Monstrey, S.J.; Matton, G. Doppler flowmetry in the planning of perforator flaps. Br. J. Plast. Surg. 1998, 51, 202–209. [Google Scholar] [CrossRef]
- Masia, J.; Larrañaga, J.; Clavero, J.A.; Vives, L.; Pons, G.; Pons, J.M. The value of the multidetector row computed tomography for the preoperative planning of deep inferior epigastric artery perforator flap: Our experience in 162 cases. Ann. Plast. Surg. 2008, 60, 29–36. [Google Scholar] [CrossRef]
- Cina, A.; Salgarello, M.; Barone-Adesi, L.; Rinaldi, P.; Bonomoet, L. Planning breast reconstruction with deep inferior epigastric artery perforating vessels: Multidetector CT angiography versus color Doppler US. Radiology 2010, 255, 979–987. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, M.D.; Thimmappa, N.D.; Vasile, J.V.; Levine, J.L.; Allen, R.J.; Greenspun, D.T.; Ahn, C.Y.; Chen, C.M.; Hedgire, S.S.; Prince, M.R. Autologous breast reconstruction: Preoperative magnetic resonance angiography for perforator flap vessel mapping. J. Reconstr. Microsurg. 2015, 31, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blondeel, P.N.; Van Landuyt, K.H.; Monstrey, S.J.; Hamdi, M.; Matton, G.E.; Allen, R.J.; Dupin, C.; Feller, A.M.; Koshima, I.; Kostakoglu, N.; et al. The “Gent” consensus on perforator flap terminology: Preliminary definitions. Plast. Reconstr. Surg. 2003, 112, 1378–1383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, W.; Lu, L.; Lazzeri, D.; Zhang, Y.X.; Wang, D.; Innocenti, M.; Qian, Y.; Agostini, T.; Levin, L.S.; Messmer, C. Contrast-enhanced Ultrasound Combined with Three-Dimensional Reconstruction in Preoperative Perforator Flap Planning. Plast. Reconstr. Surg. 2013, 131, 80–93. [Google Scholar] [CrossRef]
- Rozen, W.M.; Phillips, T.J.; Ashton, M.W.; Stella, D.L.; Gibson, R.N.; Taylor, G.I. Preoperative Imaging for DIEA Perforator Flaps: A Comparative Study of Computed Tomographic Angiography and Doppler Ultrasound. Plast. Reconstr. Surg. 2008, 121, 9–16. [Google Scholar] [CrossRef]
- Klasson, S.; Svensson, H.; Malm, K.; Wassélius, J.; Velander, P. Preoperative CT angiography versus Doppler ultrasound mapping of abdominal perforator in DIEP breast reconstructions: A randomized prospective study. J. Plast. Reconstr. Aesthet. Surg. 2015, 68, 782–786. [Google Scholar] [CrossRef]
- Heneweer, C.; Zirk, M.; Safi, A.; Smeets, R.; Malter, W.; Kröger, N.; Zöller, J.E.; Maintz, D.; Zinser, M. An innovative approach for preoperative perforator flap planning using contrast-enhanced B-Flow imaging. Plast. Reconstr. Surg. Glob. Open 2021, 9, 3547. [Google Scholar] [CrossRef]
- Cosgrove, D.; Lassau, N. Imaging of perfusion using ultrasound. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 65–85. [Google Scholar] [CrossRef]
- Scott, J.R.; Liu, D.; Said, H.; Neligan, P.C.; Mathes, D.W. Computed tomographic angiography in planning abdomen-based microsurgical breast reconstruction: A comparison with color duplex ultrasound. Plast. Reconstr. Surg. 2010, 125, 446–453. [Google Scholar] [CrossRef]
- Moon, H.K.; Taylor, G.I. The Vascular Anatomy of Rectus Abdominis Musculocutaneous Flaps Based on the Deep Superior Epigastric System. Plast. Reconstr. Surg. 1988, 82, 815–832. [Google Scholar] [CrossRef]
- Healthcare, G.E. Flow Imaging, LOGIQ E10 Series. General Electric Company. 2020. Available online: http://www.gehealth-care.com.au/Ijssmedia/fe8dObe639e544139fea346561401715.pdf?la=en-au (accessed on 15 February 2021).
- International Contrast Ultrasound Society (ICUS). Video Ceus Watch CEUS Demonstrations. Available online: http://icus-society.org/?s=video+ceuswatchCEUSdemonstrations (accessed on 15 February 2021).
- Beugels, J.; Hoekstra, L.T.; Tuinder, S.M.H.; Heuts, E.M.; van der Hulst, R.R.W.J.; Piatkowski, A.A. Complications in unilateral versus bilateral deep inferior epigastric artery perforator flap breast reconstructions: A multicentre study. J. Plast. Reconstr. Aesthet. Surg. 2016, 69, 1299–1300. [Google Scholar] [CrossRef] [PubMed]
- Wade, R.G.; Razzano, S.; Sassoon, E.M.; Haywood, R.M.; Ali, R.S.; Figus, A. Complications in DIEP Flap Breast Reconstruction After Mastectomy for Breast Cancer: A Prospective Cohort Study Comparing Unilateral versus Bilateral Reconstructions. Ann. Surg. Oncol. 2017, 24, 1465–1474. [Google Scholar] [CrossRef] [PubMed]
- Marre, D.; Hontanilla BMarre, D. Increments in ischaemia time induces microvascular complications in the DIEP flap for breast reconstruction. J. Plast. Reconstr. Aesthet. Surg. 2013, 66, 80–86. [Google Scholar] [CrossRef]
- Giunta, R.; Geisweid, A.; Feller, A. The value of preoperative Doppler sonography for planning free perforator flaps. Plast. Reconstr. Surg. 2000, 105, 2381–2386. [Google Scholar] [CrossRef] [PubMed]
- Rozen, W.; Ashton, M.; Stella, D.L.; Phillips, T.J.; Taylor, G.I. The accuracy of computed tomographic angiography for mapping the perforators of the DIEA: A cadaveric study. Plast. Reconstr. Surg. 2008, 122, 363–369. [Google Scholar] [CrossRef]
- Mah, E.; Temple, F.; Morrison, W.A. Value of preoperative Doppler ultrasound assessment of deep inferior epigastric perforators in free flap breast reconstruction. Aust. N. Z. J. Surg. 2005, 75, 89–97. [Google Scholar] [CrossRef] [Green Version]
- Hancerliougullari Koksalmis, G. Drivers to adopting B-flow ultrasonography: Contextualizing the integrated technology acceptance model. BMC Med. Imaging 2019, 19, 56–62. [Google Scholar] [CrossRef]
- Kappos, E.A.; Jaskolka, J.; Butler, K.; O’Neill, A.C.; Hofer, S.O.P.; Zhong, T. Preoperative Computed Tomographic Angiogram Measurement of Abdominal Muscles Is a Valuable Risk Assessment for Bulge Formation after Microsurgical Abdominal Free Flap Breast Reconstruction. Plast. Reconstr. Surg. 2017, 140, 170–177. [Google Scholar] [CrossRef]
- Levi, B.; Rinkinen, J.; Kidwell, K.M.; Benedict, M.; Stein, I.C.; Lisiecki, J.; Enchakalody, B.; Wang, S.C.; Kozlow, J.H.; Momoh, A.O. Morphomic analysis for preoperative donor site risk assessment in patients undergoing abdominal perforator flap breast reconstruction: A proof of concept study. J. Reconstr. Microsurg. 2014, 30, 635–640. [Google Scholar] [CrossRef]
- Wagner, R.D.; Doval, A.F.; Mehra, N.V.; Le, H.B.; Niziol, P.A.; Ellsworth, W.A.; Spiegel, A.J. Incidental Findings in CT and MR Angiography for Preoperative Planning in DIEP Flap Breast Reconstruction. Plast. Reconstr. Surg. Glob. Open 2020, 23, e3159-64. [Google Scholar] [CrossRef]
- Long, J.; Evans, T.G.; Bailey, D.; Lewis, M.H.; Gower-Thomas, K.; Murray, A. Uptake of Risk-Reducing Surgery in BRCA Gene Carriers in Wales, UK. Breast. J. 2018, 24, 580–585. [Google Scholar] [CrossRef] [PubMed]
- Wade, R.G.; Watford, J.; Wormald, J.C.R.; Bramhall, R.J.; Figus, A. Perforator mapping reduces the operative time of DIEP flap breast reconstruction: A systematic review and meta-analysis of preoperative ultrasound, computed tomography and magnetic resonance angiography. J. Plast. Reconstr. Aesthet. Surg. 2018, 71, 468–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thimmappa, N.; Bhat, A.P.; Bishop, K.; Nagpal, P.; Prince, M.R.; Saboo, S.S. Preoperative cross-sectional mapping for deep inferior epigastric and profunda artery perforator flaps. Cardiovasc. Diagn. Ther. 2019, 9, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.K.; Chang, E.I. Preoperative Perforator Mapping in SGAP Flap: Does Magnetic Resonance Imaging Make the Difference? Plast. Reconstr. Surg. 2019, 144, 820–881. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. of Flaps No. of Patients | 39 30 |
| Mean BMI (kg/m2) | 24.7 SD ± 3.9 |
| Mean age (years) | 52 SD ± 46 |
| Hemi-abdomen analyzed | 60 |
| Autologous breast reconstructions | |
| Single sided | 21 |
| Double sided | 9 |
| DIEA branching pattern (Type I-III, Moon, Taylor [20]) Type I 22% Type II 49% Type III 29% | |
| CT Scan Parameters | |
|---|---|
| Scanner | IQon (Philips Healthcare, Best, The Netherlands) |
| Slice thickness | 2 mm |
| Detector pitch | 0.671 |
| Gantry rotation time | 0.5 s |
| Tube potential | 120 kV |
| Tube current | Tube current modulation activated by default (DoseRight 3D-DOM; Philips Healthcare, Best, The Netherlands). |
| IV contrast | Accupaque 350 mg/mL (GE Healthcare; Little Chalfort, UK); IVI 4 mL/s |
| Range | Xiphisternum to the pubic symphysis |
| Bolus tracking | 150 HU within the abdominal aorta (activated bolus tracking) Cranio-caudal direction, supine position and inspirational breath hold |
| Ultrasound parameters | |
| Scanner | LOGIQ E9 (GE Healthcare, Chicago, IL, USA) |
| Linear probe | 9L-D; 2–8 MHz (GE Healthcare, Chicago, IL, USA) |
| Matrix probe | ML6-15; 4–15 MHz (GE Healthcare, Chicago, IL, USA) |
| Modes | Color Doppler ultrasound (CDUS) Contrast-enhanced ultrasound (CEUS) B-flow imaging (BUS) Contrast-enhanced B-flow imaging (BCEUS) |
| IV contrast | SonoVue 2 mL (Bracco®, Milan, Italy) |
| Perforator Mapping | Diagnostic Mode | ||||
|---|---|---|---|---|---|
| CTA | CDUS | CEUS | BUS | BCEUS | |
| Deep inferior epigastric art. | |||||
| Mean ∆L (mm) | 7.85 | 4.77 | 4.92 | 5.73 | 6.73 |
| Deviation ± (mm) | ±1.57 | ±0.863 | ±1.02 | ±1.31 | ±1.43 |
| Confidence interval (95%) | 7.21–8.48 | 4.42–5.12 | 4.51–5.33 | 5.20–6.26 | 6.15–7.31 |
| Kruskall–Wallis | p < 0.05 significance between the groups | ||||
| Levene test | p > 0.05 equality of variances | ||||
| Post hoc-test (Bonferroni) | Reference | p < 0.05 | p < 0.05 | p < 0.05 | p = 0.19 |
| Correlation Spearman | Reference | R = 0.372 (p < 0.05) | R = −0.10 (p = 0.31) | R = 0.19 (p = 0.17) | R = 0.09 (p = 0.33) |
| Muscular course (M) | |||||
| Mean ∆L (mm) | 8.04 | 5.92 | 5.88 | 5.50 | 5.42 |
| Deviation ± (mm) | ±1.59 | ±1.32 | ±1.56 | ±1.34 | ±2.18 |
| Confidence interval (95%) | 7.39–8.67 | 5.39–6.46 | 5.26–6.51 | 4.96–6.04 | 4.54–6.30 |
| Kruskall–Wallis | p < 0.05 significance between the groups | ||||
| Levene test | p > 0.05 equality of variances | ||||
| Post hoc-test (Bonferroni) | Reference | p < 0.05 | p < 0.05 | p < 0.05 | p = 0.19 |
| Correlation Spearman | Reference | R = −0.233 (p = 0.126) | R = 0.131 (p = 0.261) | R = −0.172 (p = 0.201) | R = −0.216 (p = 0.144) |
| Fascial penetration point (F) | |||||
| Mean ∆L (mm) | 6.00 | 5.12 | 4.83 | 4.54 | 3.63 |
| Deviation ± (mm) | ±1.17 | ±1.03 | ±1.19 | ±1.21 | ±0.84 |
| Confidence interval (95%) | 5.53–6.47 | 4.70–5.54 | 4.35–5.31 | 4.05–5.03 | 3.29–3.98 |
| Kruskall–Wallis | p < 0.05 significance between the groups | ||||
| Levene test | p > 0.05 equality of variances | ||||
| Post hoc-test (Bonferroni) | Reference | p < 0.05 | p < 0.05 | p < 0.05 | p < 0.05 |
| Correlation Spearman | Reference | R = −0.361 (p < 0.05) | R = 0.116 (p = 0.126) | R = −0.059 (p = 0.387) | R = 0.799 (p < 0.05) |
| Subcutaneous course of the plexus (P) and skin point (SP) | |||||
| Mean ∆L (mm) | 2.85 | no signal | 8.00 | no signal | 4.57 |
| Deviation ± (mm) | ±1.26 | -- | ±0.82 | -- | ±1.34 |
| Confidence interval (95%) | 2.34–3.35 | -- | 6.70–9.30 | -- | 3.98–5.15 |
| Kruskall–Wallis | p < 0.05 significance between the groups | ||||
| Levene test | p > 0.05 equality of variances | ||||
| Post hoc-test (Bonferroni) | Reference | -- | p < 0.05 | -- | p = 0.32 |
| Correlation Spearman | -- | R = −0.316 (p=0.342) | -- | R = 0.778 (p < 0.05) | |
| Number of Perforators (F) | Intraoperative Situation | Diagnostic Modes | ||||
|---|---|---|---|---|---|---|
| Real | CTA | CDUS | CEUS | BUS | BCEUS | |
| Mean | 2.59 | 2.48 | 1.10 | 1.40 | 1.81 | 2.27 |
| Deviation ± | ±0.129 | ±0.122 | ±0.069 | ±0.072 | ±0.076 | ±0.103 |
| Sum | 101 | 97 | 43 | 55 | 70 | 88.5 |
| Deviation ± | ±1.487 | ±1.411 | ±0.803 | ±0.827 | ±0.874 | ±1.185 |
| Correlation Spearman | Reference (1.00) | 0.981 | 0.091 | 0.225 | 0.584 | 0.947 |
| Significance | p = 0.346 | (p < 0.05) | (p < 0.05) | (p < 0.05) | p = 0.173 | |
| Delineation of Perforator Mapping | Diagnostic Modes | ||||
|---|---|---|---|---|---|
| CTA | CDUS | CEUS | BUS | BCEUS | |
| Deep inferior epigastric artery (DIEA) | Reference | ||||
| Sensitivity (%) | -- | 100 | 100 | 100 | 100 |
| Specificity (%) | -- | 100 | 100 | 100 | 100 |
| Youden index (%) | -- | 100 | 100 | 100 | 100 |
| Muscular course (M) | Reference | ||||
| Sensitivity (%) | 91.3 | 95.7 | 96.3 | 92 | |
| Specificity (%) | -- | 95.4 | 66.7 | 66.7 | 69.4 |
| Youden index (%) | -- | 86.7 | 62.4 | 63 | 61.4 |
| Fascial penetration point (F) | Reference | ||||
| Sensitivity (%) | 68.2 | 81.8 | 72.7 | 90.9 | |
| Specificity (%) | -- | 93 | 92 | 94 | 92 |
| Youden index (%) | -- | 61.2 | 73.8 | 66.7 | 82.9 |
| Subcutaneous course (P) | Reference | ||||
| Sensitivity (%) | 38.1 | 71.4 | 52.4 | 90.1 | |
| Specificity (%) | -- | 68.6 | 75.3 | 70.4 | 93.2 |
| Youden index (%) | -- | 6.7 | 46.7 | 22.8 | 83.3 |
| Skin point (SP) | Reference | ||||
| Sensitivity (%) | -- | 15.8 | 52.6 | 42.1 | 91.2 |
| Specificity (%) | -- | 72.4 | 57.1 | 68.3 | 88.9 |
| Youden index (%) | -- | −11.8 | 9.7 | 10.4 | 80.1 |
| Ultrasound Mode | Perforator Mapping |
|---|---|
| Color Doppler ultrasound (CDUS) | Inferior epigastric artery (IEA) Muscular course (M) |
| Contrast-enhanced B-flow imaging (BCEUS) | Fascial point (F) Subcutaneous plexus (P) Skin point (SP) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zinser, M.J.; Kröger, N.; Malter, W.; Schulz, T.; Puesken, M.; Mallmann, P.; Zirk, M.; Schröder, K.; Andree, C.; Seidenstuecker, K.; et al. Preoperative Perforator Mapping in DIEP Flaps for Breast Reconstruction. The Impact of New Contrast-Enhanced Ultrasound Techniques. J. Pers. Med. 2023, 13, 64. https://doi.org/10.3390/jpm13010064
Zinser MJ, Kröger N, Malter W, Schulz T, Puesken M, Mallmann P, Zirk M, Schröder K, Andree C, Seidenstuecker K, et al. Preoperative Perforator Mapping in DIEP Flaps for Breast Reconstruction. The Impact of New Contrast-Enhanced Ultrasound Techniques. Journal of Personalized Medicine. 2023; 13(1):64. https://doi.org/10.3390/jpm13010064
Chicago/Turabian StyleZinser, Max J, Nadja Kröger, Wolfram Malter, Tino Schulz, Michael Puesken, Peter Mallmann, Matthias Zirk, Kai Schröder, Christoph Andree, Kathrin Seidenstuecker, and et al. 2023. "Preoperative Perforator Mapping in DIEP Flaps for Breast Reconstruction. The Impact of New Contrast-Enhanced Ultrasound Techniques" Journal of Personalized Medicine 13, no. 1: 64. https://doi.org/10.3390/jpm13010064