
Quality of Life Assessment of Chronic Otitis Media Patients Following Surgery
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Backous, D.; Center, S.S.M.; Choi, B.Y.; Jaramillo, R.; Kong, K.; Lenarz, T.; Ray, J.; Thakar, A.; Hol, M.K.; Ses, M.C.H.; et al. Hearing Rehabilitation of Patients with Chronic Otitis Media: A Discussion of Current State of Knowledge and Research Priorities. J. Int. Adv. Otol. 2022, 18, 365–370. [Google Scholar] [CrossRef]
- Jotic, A.D.; Opankovic, A.M.; Radin, Z.Z.; Cvorovic, L.; Vujovic, K.R.S.; Krejovic-Trivic, S.B.; Bukurov, B.M.; Milicic, B.R.; Stojanovic, J.D. Symptoms of depression, anxiety and stress in patients with chronic otitis media. PLoS ONE 2022, 17, e0270793. [Google Scholar] [CrossRef] [PubMed]
- Lailach, S.; Langanke, T.; Zahnert, T.; Garthus-Niegel, S.; Neudert, M. Impact of depressive disorders on quality of life after middle ear surgery in patients with chronic otitis media. Eur. Arch. Oto-Rhino-Laryngol. 2020, 278, 3217–3225. [Google Scholar] [CrossRef]
- World Health Organization. Chronic Suppurative Otitis Media: Burden of Illness and Management Options; World Health Organization: Geneva, Switzerland, 2004.
- Phillips, J.S.; Tailor, B.V.; Nunney, I.; Yung, M.W.; Doruk, C.; Kara, H.; Kong, T.; Quaranta, N.; Peñaranda, A.; Bernardeschi, D.; et al. Impact of Hearing Disability and Ear Discharge on Quality-of-Life in Patients with Chronic Otitis Media: Data from the Multinational Collaborative COMQ-12 Study. Otol. Neurotol. 2021, 42, e1507–e1512. [Google Scholar] [CrossRef] [PubMed]
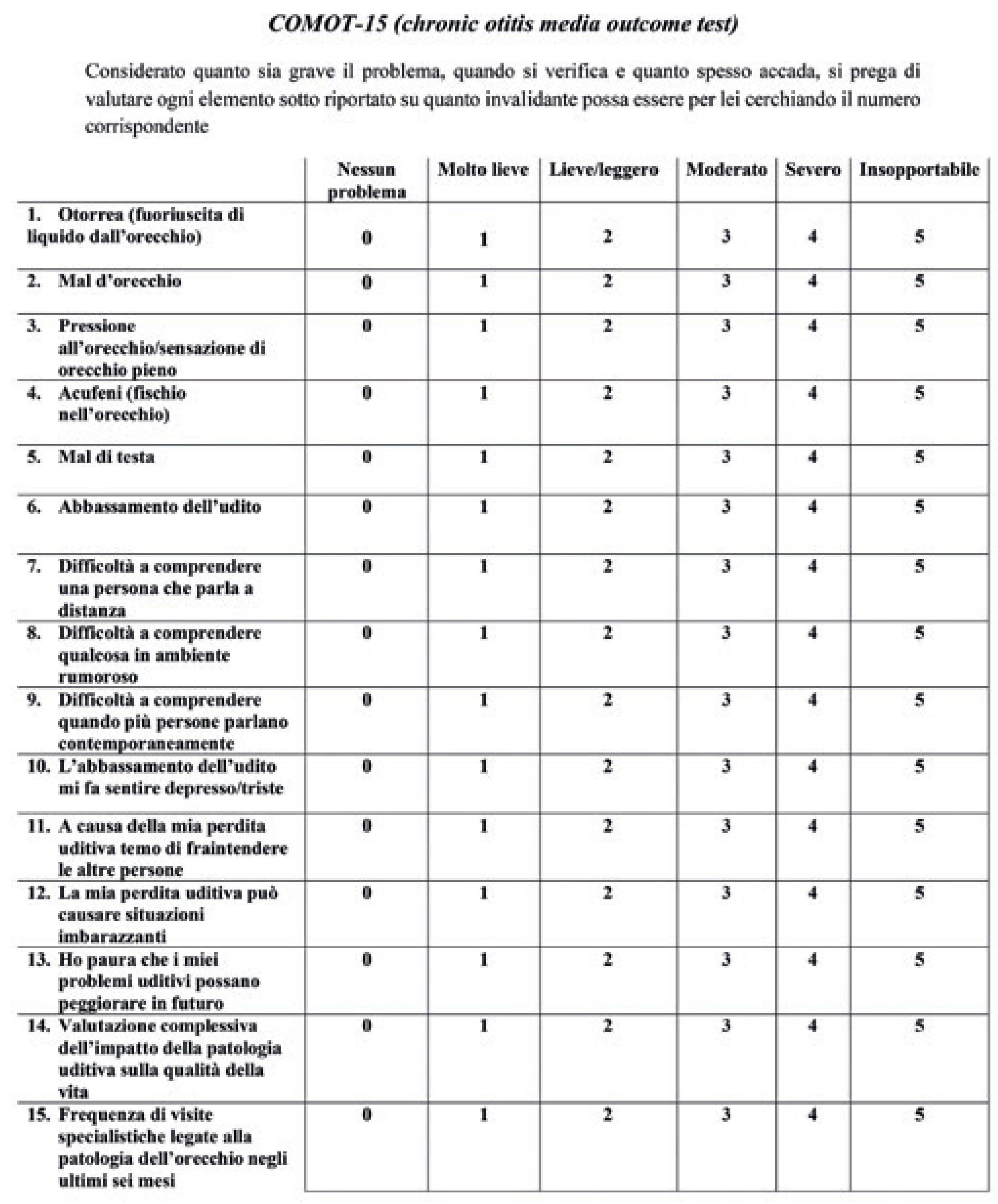
- Baumann, I.; Kurpiers, B.; Plinkert, P.; Praetorius, M. Entwicklung und Validierung des Chronic Otitis Media Outcome Test 15 (COMOT-15). HNO 2009, 57, 889–895. [Google Scholar] [CrossRef]
- Nadol, J.B.; Staecker, H.; Gliklich, R.E. Outcomes Assessment for Chronic Otitis Media: The Chronic Ear Survey. Laryngoscope 2000, 110, 32–35. [Google Scholar] [CrossRef] [PubMed]
- Pontillo, V.; Damiani, M.; Harib, A.; Sammali, M.; Graziano, G.; Quaranta, N. Quality of life after cholesteatoma surgery: Comparison between surgical techniques. Acta Otorhinolaryngol. Ital. 2022, 42, 293–299. [Google Scholar] [CrossRef]
- Bächinger, D.; Röösli, C.; Ditzen, B.; Huber, A. Development and validation of the Zurich chronic middle ear inventory (ZCMEI-21): An electronic questionnaire for assessing quality of life in patients with chronic otitis media. Eur. Arch. Oto-Rhino-Laryngol. 2016, 273, 3073–3081. [Google Scholar] [CrossRef]
- Vlastos, I.; Kandiloros, D.; Manolopoulos, L.; Ferekidis, E.; Yiotakis, I. Quality of life in children with chronic suppurative otitis media with or without cholesteatoma. Int. J. Pediatr. Otorhinolaryngol. 2009, 73, 363–369. [Google Scholar] [CrossRef]
- Quaranta, N.; De Robertis, V.; Milella, C.; Pontrelli, M.; Greco, A.; Fiorella, M.L.; Pontillo, V.; de Vincentiis, M.; Phillips, J.S.; Ralli, M. Cross-cultural adaption and validation of the Chronic Otitis Media Questionnaire 12 (COMQ-12) in the Italian language. Eur. Arch. Oto-Rhino-Laryngol. 2019, 276, 3027–3033. [Google Scholar] [CrossRef]
- Lailach, S.; Baumann, I.; Zahnert, T.; Neudert, M. Aktueller Stand der Lebensqualitätsmessung bei Patienten mit chronischer Otitis media und Schallleitungsschwerhörigkeit. HNO 2018, 66, 578–589. [Google Scholar] [CrossRef] [PubMed]
- Cavaliere, M.; Ricciardiello, F.; Mesolella, M.; Iengo, M. Stapedotomy: Functional Results with Different Diameter Prostheses. ORL 2012, 74, 93–96. [Google Scholar] [CrossRef] [PubMed]
- Mlynski, R.; Bächinger, D.; Langanke, T.; Lailach, S.; Neudert, M.; Weiss, N.M. Comparison of two disease-specific instruments assessing health-related quality of life in patients with chronic otitis media. Eur. Arch. Oto-Rhino-Laryngol. 2021, 279, 703–711. [Google Scholar] [CrossRef] [PubMed]
- Cavaliere, M.; Capriglione, P.; Cavaliere, F.; De Corso, E.; Zanoletti, E.; Motta, G.; Iengo, M.; Cantone, E. Cross-cultural adaptation and Italian validation of chronic otitis media outcome test 15 (COMOT-15). Acta Otorhinolaryngol. Ital. 2021, 41, 277–281. [Google Scholar] [CrossRef]
- Hellmann, F.; Verdi, M.; Schlemper, B.R., Jr.; Caponi, S. 50th anniversary of the Declaration of Helsinki: The double standard was introduced. Arch. Med. Res. 2014, 45, 600–601. [Google Scholar] [CrossRef]
- Prunty, S.; Ha, J.; Vijayasekaran, S. Management of chronic suppurative otitis media. In Otitis Media: State of the Art Concepts and Treatment; Preciado, D., Ed.; Springer: Berlin/Heidelberg, Germany, 2015. [Google Scholar]
- Russo, C.; Elefante, A.; Cavaliere, M.; Di Lullo, A.M.; Motta, G.; Iengo, M.; Brunetti, A. Apparent diffusion coefficients for predicting primary cholesteatoma risk of recurrence after surgical clearance. Eur. J. Radiol. 2020, 125, 108915. [Google Scholar] [CrossRef]
- Cavaliere, M.; Di Lullo, A.M.; Russo, C.; Mesolella, M.; Cantone, E.; Di Lorenzo, G.; Motta, G.; Elefante, A. Computed-Tomography-Structured Reporting in Middle Ear Opacification: Surgical Results and Clinical Considerations From a Large Retrospective Analysis. Front. Neurol. 2021, 12, 615356. [Google Scholar] [CrossRef]
- Russo, C.; Di Lullo, A.M.; Cantone, E.; Klain, M.; Motta, G.; Elefante, A.; Cavaliere, M. Combining Thin-Section Coronal and Axial Diffusion Weighted Imaging: Good Practice in Middle Ear Cholesteatoma Neuroimaging. Front. Neurol. 2021, 12, 606692. [Google Scholar] [CrossRef]
- Bächinger, D.; Mlynski, R.; Weiss, N.M. Establishing the minimal clinically important difference (MCID) of the Zurich Chronic Middle Ear Inventory (ZCMEI-21) in patients treated for chronic middle ear disease. Eur. Arch. Oto-Rhino-Laryngol. 2020, 277, 1039–1044. [Google Scholar] [CrossRef] [Green Version]
- Choi, S.Y.; Cho, Y.-S.; Lee, N.J.; Lee, J.; Chung, W.-H.; Hong, S.H. Factors Associated With Quality of Life After Ear Surgery in Patients With Chronic Otitis Media. Arch. Otolaryngol. Neck Surg. 2012, 138, 840–845. [Google Scholar] [CrossRef]
- Maile, E.J.; Tharu, P.B.; Blanchford, H.L.K.; Edmiston, R.; Youngs, R. Quality of life of Nepali patients with ear disease before and after corrective surgery. Trop. Med. Int. Health 2015, 20, 1041–1047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiss, N.M.; Bächinger, D.; Rrahmani, A.; Bernd, H.E.; Huber, A.; Mlynski, R.; Röösli, C. Mapping the ChOLE classification to hearing outcomes and disease-specific health-related quality of life. Eur. Arch. Oto-Rhino-Laryngol. 2020, 277, 2729–2738. [Google Scholar] [CrossRef] [PubMed]
- Weiss, N.M.; Bächinger, D.; Botzen, J.; Großmann, W.; Mlynski, R. Mastoid cavity obliteration leads to a clinically significant improvement in health-related quality of life. Eur. Arch. Oto-Rhino-Laryngol. 2020, 277, 1637–1643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucidi, D.; De Corso, E.; Paludetti, G.; Sergi, B. Quality of life and functional results in canal wall down vs canal wall up mastoidectomy. Acta Otorhinolaryngol. Ital. 2019, 39, 53–60. [Google Scholar] [CrossRef] [Green Version]
- Baumann, I.; Gerendas, B.S.; Plinkert, P.K.; Praetorius, M. General and disease-specific quality of life in patients with chronic suppurative otitis media—A prospective study. Health Qual. Life Outcomes 2011, 9, 48. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (Years) | ≤50 | >50 | Total | |
|---|---|---|---|---|
| Closed Techniques | CWUT | 6 | 1 | 7 |
| U-MPL | 7 | 5 | 12 | |
| O-MPL | 1 | 1 | 2 | |
| Open Techniques | CWDT | 10 | 21 | 31 |
| Total | 24 | 28 | 52 |
| Open Techniques | Closed Techniques | |||
|---|---|---|---|---|
| Type of intervention | CWDT | CWUT | U-MPL | O-MPL |
| Patients (nr). | 31 | 7 | 12 | 2 |
| QoL OS T0 | 36.76 ± 13.1 | |||
| QoL OS T1 | 26.88 ± 12 | |||
| ∆-COMOT OS | +9.88 (p: 0.00011) * | |||
| QoL ES T0 | 11.05 ± 4.45 | |||
| QoL ES T1 | 4.15 ± 3.61 | |||
| ∆-COMOT ES | +6.9 (p: 0.000007) * | |||
| QoL HF T0 | 13.48 ± 5.83 | |||
| QoL HF T1 | 12.17 ± 5.71 | |||
| ∆-COMOT HF | +1.31 (p: 0.02511) * | |||
| QoL MH T0 | 9.69 ± 4.65 | |||
| QoL MH T1 | 7.903 ± 5.409 | |||
| ∆-COMOT MH | +1.79 (p: 0.073) | |||
| QoL OS T0 | 39.6 ± 13.4 | 33.23 ± 12.05 | ||
| QoL OS T1 | 30.29 ± 10.85 | 21.85 ± 11.92 | ||
| ∆-COMOT OS | +9.31(p: 0.000072) * | +11.38 (p: 0.000051) * | ||
| QoL ES T0 | 12.03 ± 4,16 | 9.61 ± 4.57 | ||
| QoL ES T1 | 4.54 ± 4.20 | 3.57 ± 2.42 | ||
| ∆-COMOT ES | +7.49 (p: 0.0000837) * | +6.04 (p: 0.0000031) * | ||
| QoL HF T0 | 13.9 ± 6.26 | 12.85 ± 5.21 | ||
| QoL HF T1 | 13.78 ± 4.95 | 10.14 ± 6.26 | ||
| ∆-COMOT HF | +0.12 (p: 0.68) | +2.71 (p: 0.038) * | ||
| QoL MH T0 | 10.41 ± 4.85 | 8.61 ± 4.23 | ||
| QoL MH T1 | 9.38 ± 5.48 | 5.71 ± 4.58 | ||
| ∆-COMOT MH | +1.03 (p: 0.20) | +2.90 (p: 0.00015) * | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cavaliere, M.; Di Lullo, A.M.; Capriglione, P.; Motta, G.; Cantone, E. Quality of Life Assessment of Chronic Otitis Media Patients Following Surgery. J. Pers. Med. 2023, 13, 74. https://doi.org/10.3390/jpm13010074
Cavaliere M, Di Lullo AM, Capriglione P, Motta G, Cantone E. Quality of Life Assessment of Chronic Otitis Media Patients Following Surgery. Journal of Personalized Medicine. 2023; 13(1):74. https://doi.org/10.3390/jpm13010074
Chicago/Turabian StyleCavaliere, Michele, Antonella Miriam Di Lullo, Pasquale Capriglione, Gaetano Motta, and Elena Cantone. 2023. "Quality of Life Assessment of Chronic Otitis Media Patients Following Surgery" Journal of Personalized Medicine 13, no. 1: 74. https://doi.org/10.3390/jpm13010074