


Pandemic Stressors and Adaptive Responses: A Longitudinal Analysis of the Quality of Life and Psychosocial Dynamics among Urothelial Cancer Patients

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Research Design and Ethical Considerations
2.2. Inclusion Criteria
2.3. Variables
2.4. Employed Surveys
2.5. Statistical Analysis
3. Results
4. Discussion
4.1. Important Findings and Literature Review
4.2. Study Limitations and Future Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kesner, L.; Horáček, J. Three challenges that the COVID-19 pandemic represents for psychiatry. Br. J. Psychiatry 2020, 217, 475–476. [Google Scholar] [CrossRef] [PubMed]
- WHO Coronavirus (COVID-19) Dashboard|WHO Coronavirus (COVID-19) Dashboard with Vaccination Data. Available online: https://covid19.who.int/ (accessed on 20 October 2023).
- Feier, C.V.I.; Faur, A.M.; Muntean, C.; Blidari, A.; Contes, O.E.; Streinu, D.R.; Olariu, S. The Challenges of Gastric Cancer Surgery during the COVID-19 Pandemic. Healthcare 2023, 11, 1903. [Google Scholar] [CrossRef] [PubMed]
- Anderson, D.; Razzak, A.N.; McDonald, M.; Cao, D.; Hasoon, J.; Viswanath, O.; Kaye, A.D.; Urits, I. Mental Health in Urologic Oncology. Health Psychol. Res. 2022, 10, 37518. [Google Scholar] [CrossRef] [PubMed]
- Barbos, V.; Feciche, B.; Bratosin, F.; Bogdan, I.; Negrean, R.A.; Latcu, S.; Croitor, A.; Dema, V.; Bardan, R.; Cumpanas, A.A. A Retrospective Analysis of the Challenges of Urothelial Cancer Management during the COVID-19 Pandemic at a Single Academic Center in Romania. Healthcare 2023, 11, 812. [Google Scholar] [CrossRef]
- Papava, I.; Dehelean, L.; Romosan, R.S.; Bondrescu, M.; Dimeny, C.Z.; Domuta, E.M.; Bratosin, F.; Bogdan, I.; Grigoras, M.L.; Tigmeanu, C.V.; et al. The Impact of Hyper-Acute Inflammatory Response on Stress Adaptation and Psychological Symptoms of COVID-19 Patients. Int. J. Environ. Res. Public Health 2022, 19, 6501. [Google Scholar] [CrossRef] [PubMed]
- Saginala, K.; Barsouk, A.; Aluru, J.S.; Rawla, P.; Padala, S.A.; Barsouk, A. Epidemiology of Bladder Cancer. Med. Sci. 2020, 8, 15. [Google Scholar] [CrossRef]
- Caballero, J.M.; Gili, J.M.; Pereira, J.C.; Gomáriz, A.; Castillo, C.; Martín-Baranera, M. Risk Factors Involved in the High Incidence of Bladder Cancer in an Industrialized Area in North-Eastern Spain: A Case-Control Study. J. Clin. Med. 2023, 12, 728. [Google Scholar] [CrossRef]
- Halaseh, S.A.; Halaseh, S.; Alali, Y.; Ashour, M.E.; Alharayzah, M.J. A Review of the Etiology and Epidemiology of Bladder Cancer: All You Need To Know. Cureus 2022, 14, e27330. [Google Scholar] [CrossRef]
- Vrdoljak, E.; Wojtukiewicz, M.Z.; Pienkowski, T.; Bodoky, G.; Berzinec, P.; Finek, J.; Todorović, V.; Borojević, N.; Croitoru, A. South Eastern European Research Oncology Group. Cancer epidemiology in Central, South and Eastern European countries. Croat. Med. J. 2011, 52, 478–487. [Google Scholar] [CrossRef]
- Richters, A.; Aben, K.K.H.; Kiemeney, L.A.L.M. The global burden of urinary bladder cancer: An update. World J. Urol. 2020, 38, 1895–1904. [Google Scholar] [CrossRef]
- Dybowski, B.; Ossoliński, K.; Ossolińska, A.; Peller, M.; Bres-Niewada, E.; Radziszewski, P. Impact of stage and comorbidities on five-year survival after radical cystectomy in Poland: Single centre experience. Cent. Eur. J. Urol. 2015, 68, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Jeong, C.W.; Kwak, C.; Kim, H.H.; Ku, J.H. Disease-Free Survival at 2 and 3 Years is a Significant Early Surrogate Marker Predicting the 5-Year Overall Survival in Patients Treated with Radical Cystectomy for Urothelial Carcinoma of the Bladder: External Evaluation and Validation in a Cohort of Korean Patients. Front. Oncol. 2015, 5, 246. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Octavian Neagoe, C.; Mazilu, O. Pelvic intraoperative iatrogenic oncosurgical injuries: Single-center experience. JBUON Off. J. Balk. Union Oncol. 2016, 21, 498–504. [Google Scholar]
- Toma, A.O.; Boeriu, E.; Decean, L.; Bloanca, V.; Bratosin, F.; Levai, M.C.; Vasamsetti, N.G.; Alambaram, S.; Oprisoni, A.L.; Miutescu, B.; et al. The Effects of Lack of Awareness in Age-Related Quality of Life, Coping with Stress, and Depression among Patients with Malignant Melanoma. Curr. Oncol. 2023, 30, 1516–1528. [Google Scholar] [CrossRef]
- Feier, C.V.I.; Muntean, C.; Faur, A.M.; Blidari, A.; Contes, O.E.; Streinu, D.R.; Olariu, S. The Changing Landscape of Thyroid Surgery during the COVID-19 Pandemic: A Four-Year Analysis in a University Hospital in Romania. Cancers 2023, 15, 3032. [Google Scholar] [CrossRef]
- Shariat, S.F.; Sfakianos, J.P.; Droller, M.J.; Karakiewicz, P.I.; Meryn, S.; Bochner, B.H. The effect of age and gender on bladder cancer: A critical review of the literature. BJU Int. 2010, 105, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Khaki, A.R.; Li, A.; Diamantopoulos, L.N.; Bilen, M.A.; Santos, V.; Esther, J.; Morales-Barrera, R.; Devitt, M.; Nelson, A.; Hoimes, C.J.; et al. Impact of performance status on treatment outcomes: A real-world study of advanced urothelial cancer treated with immune checkpoint inhibitors. Cancer 2020, 126, 1208–1216. [Google Scholar] [CrossRef] [PubMed]
- Hogea, P.; Tudorache, E.; Fira-Mladinescu, O.; Pescaru, C.; Manolescu, D.; Bratosin, F.; Rosca, O.; Kakarla, M.; Horhat, F.G.; Oancea, C. Bronchial Microbiota and the Stress Associated with Invasive Diagnostic Tests in Lung Cancer vs. Benign Pulmonary Diseases: A Cross-Sectional Study. Diagnostics 2023, 13, 2419. [Google Scholar] [CrossRef]
- Dehelean, L.; Papava, I.; Musat, M.I.; Bondrescu, M.; Bratosin, F.; Bucatos, B.O.; Bortun, A.-M.C.; Mager, D.V.; Romosan, R.S.; Romosan, A.-M.; et al. Coping Strategies and Stress Related Disorders in Patients with COVID-19. Brain Sci. 2021, 11, 1287. [Google Scholar] [CrossRef]
- Nicola, A.; Oancea, C.; Barata, P.I.; Adelina, M.; Mateescu, T.; Manolescu, D.; Bratosin, F.; Fericean, R.M.; Pingilati, R.A.; Paleru, C. Health-Related Quality of Life and Stress-Related Disorders in Patients with Bronchiectasis after Pulmonary Resection. J. Pers. Med. 2023, 13, 1310. [Google Scholar] [CrossRef]
- Niedzwiedz, C.L.; Knifton, L.; Robb, K.A.; Katikireddi, S.V.; Smith, D.J. Depression and anxiety among people living with and beyond cancer: A growing clinical and research priority. BMC Cancer 2019, 19, 943. [Google Scholar] [CrossRef]
- Aparicio Betancourt, M.; Duarte-Díaz, A.; Vall-Roqué, H.; Seils, L.; Orrego, C.; Perestelo-Pérez, L.; Barrio-Cortes, J.; Beca-Martínez, M.T.; Molina Serrano, A.; Bermejo-Caja, C.J.; et al. Global Healthcare Needs Related to COVID-19: An Evidence Map of the First Year of the Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 10332. [Google Scholar] [CrossRef]
- Nicolescu, L.-C.; Popescu, C.-L.; Popescu, C.-V.; Nicolescu, C.-M.; Nesiu, A.; Stanciu, A.N.; Mihu, A.G. The evaluation of vitamin D deficiency as a risk factor in the case of patients with moderate COVID-19. Farmacia 2022, 70, 507–513. [Google Scholar] [CrossRef]
- Yıldırım, M. Loneliness and Psychological Distress: A Mediating Role of Meaning in Life during COVID-19 Pandemic. Anxiety, Uncertainty, and Resilience during the Pandemic Period—Anthropological and Psychological Perspectives; IntechOpen: London, UK, 2021. [Google Scholar] [CrossRef]
- Yıldırım, M.; Şanli, M. Psychometric properties of the Turkish version of the COVID-19 Impact Scale in university students. J. Sch. Educ. Psychol. 2023, 3, 22–33. [Google Scholar] [CrossRef]
- Annunziata, M.A.; Muzzatti, B.; Bidoli, E.; Flaiban, C.; Bomben, F.; Piccinin, M.; Gipponi, K.M.; Mariutti, G.; Busato, S.; Mella, S. Hospital Anxiety and Depression Scale (HADS) accuracy in cancer patients. Support. Care Cancer 2020, 28, 3921–3926. [Google Scholar] [CrossRef]
- Shrestha, A.; Martin, C.; Burton, M.; Walters, S.; Collins, K.; Wyld, L. Quality of life versus length of life considerations in cancer patients: A systematic literature review. Psychooncology 2019, 28, 1367–1380. [Google Scholar] [CrossRef]
- Horhat, F.; Rogobete, A.; Papurica, M.; Sandesc, D.; Tanasescu, S.; Dumitrascu, V.; Licker, M.; Nitu, R.; Cradigati, C.; Sarandan, M.; et al. The Use of Lipid Peroxidation Expression as a Biomarker for the Molecular Damage in the Critically Ill Polytrauma Patient. Clin. Lab. 2016, 62, 1601–1607. [Google Scholar] [CrossRef] [PubMed]
- Randall, P.S.; Koppel, P.D.; Docherty, S.L.; De Gagne, J.C. The Psychological Impact of the COVID-19 Pandemic on Postsecondary Students: An Analysis of Self-Determination. Int. J. Environ. Res. Public Health 2022, 19, 8545. [Google Scholar] [CrossRef]
- Azam, F.; Latif, M.F.; Farooq, A.; Tirmazy, S.H.; AlShahrani, S.; Bashir, S.; Bukhari, N. Performance Status Assessment by Using ECOG (Eastern Cooperative Oncology Group) Score for Cancer Patients by Oncology Healthcare Professionals. Case Rep. Oncol. 2019, 12, 728–736. [Google Scholar] [CrossRef]
- Nicolescu, C.; Pop, A.; Mihu, A.; Pilat, L.; Bedreag, O.; Nicolescu, L. The Evaluation of the Role of the Cytokines TNF- alfa and IL 6 in the Production of Hypoalbuminemia in Patients Undergoing Major Surgical Interventions. Rev. Chim. 2018, 69, 1830–1837. [Google Scholar] [CrossRef]
- Toma, A.O.; Prodan, M.; Reddyreddy, A.R.; Seclaman, E.; Crainiceanu, Z.; Bloanca, V.; Bratosin, F.; Dumitru, C.; Pilut, C.N.; Alambaram, S.; et al. The Epidemiology of Malignant Melanoma during the First Two Years of the COVID-19 Pandemic: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 20, 305. [Google Scholar] [CrossRef] [PubMed]
- Petrovici, I.; Ionica, M.; Neagoe, O.C. Economic Crisis: A Factor for the Delayed Diagnosis of Breast Cancer. Int. J. Environ. Res. Public Health 2021, 18, 3998. [Google Scholar] [CrossRef] [PubMed]
- Burholt, V.; Nash, P. Short Form 36 (SF-36) Health Survey Questionnaire: Normative data for Wales. J. Public Health 2011, 33, 587–603. [Google Scholar] [CrossRef] [PubMed]
- Rishi, P.; Rishi, E.; Maitray, A.; Agarwal, A.; Nair, S.; Gopalakrishnan, S. Hospital anxiety and depression scale assessment of 100 patients before and after using low vision care: A prospective study in a tertiary eye-care setting. Indian J. Ophthalmol. 2017, 65, 1203–1208. [Google Scholar] [CrossRef]
- Johnson, S.U.; Ulvenes, P.G.; Øktedalen, T.; Hoffart, A. Psychometric Properties of the General Anxiety Disorder 7-Item (GAD-7) Scale in a Heterogeneous Psychiatric Sample. Front. Psychol. 2019, 10, 1713. [Google Scholar] [CrossRef] [PubMed]
- Levis, B.; Benedetti, A.; Thombs, B.D. DEPRESsion Screening Data (DEPRESSD) Collaboration. Accuracy of Patient Health Questionnaire-9 (PHQ-9) for screening to detect major depression: Individual participant data meta-analysis. BMJ 2019, 365, l1476. [Google Scholar] [CrossRef]
- Ravindran, O.S.; Shankar, A.; Murthy, T. A Comparative Study on Perceived Stress, Coping, Quality of Life, and Hopelessness between Cancer Patients and Survivors. Indian J. Palliat. Care 2019, 25, 414–420. [Google Scholar] [CrossRef]
- Antoni, M.H.; Moreno, P.I.; Penedo, F.J. Stress Management Interventions to Facilitate Psychological and Physiological Adaptation and Optimal Health Outcomes in Cancer Patients and Survivors. Annu. Rev. Psychol. 2023, 74, 423–455. [Google Scholar] [CrossRef]
- Barre, P.V.; Padmaja, G.; Rana, S. Tiamongla Stress and Quality of Life in Cancer Patients: Medical and Psychological Intervention. Indian J. Psychol. Med. 2018, 40, 232–238. [Google Scholar] [CrossRef]
- Ruiz-Rodríguez, I.; Hombrados-Mendieta, I.; Melguizo-Garín, A.; Martos-Méndez, M.J. The Association of Sources of Support, Types of Support and Satisfaction with Support Received on Perceived Stress and Quality of Life of Cancer Patients. Integr. Cancer Ther. 2021, 20, 1534735421994905. [Google Scholar] [CrossRef]
- Katsaros, D.; Hawthorne, J.; Patel, J.; Pothier, K.; Aungst, T.; Franzese, C. Optimizing Social Support in Oncology with Digital Platforms. JMIR Cancer 2022, 8, e36258. [Google Scholar] [CrossRef]
- Wang, Y.; Duan, Z.; Ma, Z.; Mao, Y.; Li, X.; Wilson, A.; Qin, H.; Ou, J.; Peng, K.; Zhou, F.; et al. Epidemiology of mental health problems among patients with cancer during COVID-19 pandemic. Transl. Psychiatry 2020, 10, 263. [Google Scholar] [CrossRef]
- Romito, F.; Dellino, M.; Loseto, G.; Opinto, G.; Silvestris, E.; Cormio, C.; Guarini, A.; Minoia, C. Psychological distress in outpatients with lymphoma during the COVID-19 pandemic. Front. Oncol. 2020, 10, 1270. [Google Scholar] [CrossRef]
- Koca, S.; Koca, E.; Okten, I.N.; Orengül, F.F.; Oztürk, A.; Ozçelik, M.; Oyman, A.; Çil, I.; Gümüş, M. Psychological impacts of COVID-19 pandemic in cancer patients on active treatment. Heliyon 2022, 8, e10142. [Google Scholar] [CrossRef] [PubMed]
- Massie, M.J. Prevalence of depression in patients with cancer. J. Natl. Cancer Inst. Monogr. 2004, 32, 57–71. [Google Scholar] [CrossRef] [PubMed]
- Karataş, T.; Ayaz-Alkaya, S.; Özdemir, N. Fear, Anxiety, and Coping Self-Efficacy of Individuals with Cancer during COVID-19 and Predictive Risk Factors: A Descriptive and Correlational Study. Semin. Oncol. Nurs. 2023, 39, 151420. [Google Scholar] [CrossRef] [PubMed]
- Kangas, M.; Henry, J.L.; Bryant, R.A. Posttraumatic stress disorder following cancer. A conceptual and empirical review. Clin. Psychol. Rev. 2002, 22, 499–524. [Google Scholar] [CrossRef]
- Forte, G.; Favieri, F.; Tambelli, R.; Casagrande, M. COVID-19 pandemic in the Italian population: Validation of a post-traumatic stress disorder questionnaire prevalence of PTSD symptomatology. Int. J. Environ. Res. Public Health 2020, 17, 4151. [Google Scholar] [CrossRef] [PubMed]
- O’Meara, S.; Bhatt, N.R.; Flynn, R.J.; Manecksha, R.P.; Thomas, A.Z. Bladder cancer in Ireland: A 21-year review. Ir. J. Med. Sci. 2021, 190, 531–538. [Google Scholar] [CrossRef]
- Leow, J.J.; Tan, W.S.; Tan, T.W.; Chan, V.W.-S.; Tikkinen, K.A.O.; Kamat, A.; Sengupta, S.; Meng, M.V.; Shariat, S.; Roupret, M.; et al. A systematic review and meta-analysis on delaying surgery for urothelial carcinoma of bladder and upper tract urothelial carcinoma: Implications for the COVID-19 pandemic and beyond. Front. Surg. 2022, 9, 879774. [Google Scholar] [CrossRef]
- Guan, M.; Han, J.Y.; Shah, D.V.; Gustafson, D.H. Exploring the Role of Social Support in Promoting Patient Participation in Health Care among Women with Breast Cancer. Health Commun. 2021, 36, 1581–1589. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| 2020 (n = 56) | 2021 (n = 52) | 2022 (n = 55) | p-Value * | |
|---|---|---|---|---|
| Age, years (mean ± SD) ** | 61.8 ± 9.9 | 62.3 ± 9.5 | 60.5 ± 10.2 | 0.618 |
| Sex (male) | 31 (55.4%) | 28 (53.8%) | 33 (60.0%) | 0.797 |
| BMI, kg/m2 (mean ± SD) ** | 26.4 ± 3.9 | 26.9 ± 4.1 | 25.8 ± 4.3 | 0.379 |
| Substance use behavior | ||||
| Chronic smoking | 18 (32.1%) | 18 (34.6%) | 15 (27.3%) | 0.705 |
| Chronic alcohol use | 5 (8.9%) | 3 (5.8%) | 6 (10.9%) | 0.634 |
| Place of origin (urban) | 35 (62.5%) | 30 (57.7%) | 39 (70.9%) | 0.352 |
| Referral Source | 0.678 | |||
| Primary care | 17 (30.4%) | 19 (36.5%) | 16 (29.1%) | |
| Secondary care | 39 (69.6%) | 33 (63.5%) | 39 (70.9%) | |
| COVID-19-vaccinated | - | 12 (23.1%) | 28 (50.9%) | 0.003 |
| Number of comorbidities | ||||
| 0–1 | 14 (25.0%) | 10 (19.2%) | 16 (29.1%) | |
| 2 | 30 (53.6%) | 29 (55.8%) | 25 (45.5%) | |
| ≥3 | 12 (21.4%) | 13 (25.0%) | 14 (25.5%) | |
| Relationship status | 0.679 | |||
| Single/divorced/widowed | 7 (12.5%) | 10 (19.2%) | 9 (16.4%) | |
| In a relationship/married | 40 (71.4%) | 34 (65.4%) | 41 (74.5%) | |
| Unknown | 9 (16.1%) | 8 (15.4%) | 5 (9.1%) | |
| Surveying period | 0.312 | |||
| 1st quarter | 7 (12.5%) | 9 (17.3%) | 11 (20.0%) | |
| 2nd quarter | 20 (35.7%) | 15 (28.8%) | 12 (21.8%) | |
| 3rd quarter | 17 (30.4%) | 21 (40.4%) | 16 (29.1%) | |
| 4th quarter | 12 (21.4%) | 7 (13.5%) | 16 (29.1%) |
| 2020 (n = 56) | 2021 (n = 52) | 2022 (n = 55) | p-Value * | |
|---|---|---|---|---|
| Tumoral infiltration (NMIBC) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | - |
| TNM stage 1 | 56 (100%) | 52 (100%) | 55 (100%) | - |
| ECOG 1 | 56 (100%) | 52 (100%) | 55 (100%) | - |
| TURBT | 56 (100%) | 52 (100%) | 55 (100%) | - |
| Grading | 0.818 | |||
| Low grade | 21 (37.5%) | 18 (34.9%) | 23 (41.8%) | |
| High grade | 19 (33.9%) | 20 (38.5%) | 15 (27.3%) | |
| Unknown | 16 (28.6%) | 14 (26.9%) | 17 (30.9%) | |
| Days of hospitalization (mean ± SD) ** | 3.6 ± 2.1 | 3.8 ± 2.5 | 4.0 ± 2.4 | 0.663 |
| Question | 2020 (n = 56) | 2021 (n = 52) | 2022 (n = 55) | p-Value * |
|---|---|---|---|---|
| Since the onset of the pandemic, have you experienced any changes in the frequency or severity of your urinary symptoms? (Yes, %) | 16 (28.6%) | 19 (36.5%) | 21 (38.2%) | 0.523 |
| Do you believe your current symptoms might be associated with the COVID-19 pandemic? (Yes, %) | 21 (37.5%) | 33 (63.5%) | 28 (50.9%) | 0.026 |
| During the pandemic, have there been any changes in your access to medical care or the quality of the medical care you received? (Yes, %) | 41 (73.2%) | 38 (73.1%) | 29 (52.7%) | 0.033 |
| Did you feel challenged in adhering to any treatment regimens during the pandemic? (Yes, %) | 19 (33.9%) | 24 (46.2%) | 15 (27.3%) | 0.118 |
| Have you noticed any changes in your emotional well-being? (Yes, %) | 37 (66.1%) | 30 (57.7%) | 41 (74.5%) | 0.183 |
| Has the pandemic affected your ability to engage in physical activities or maintain a healthy lifestyle? (rate on a 1 to 10 scale) ** | 7.3 ± 2.6 | 6.5 ± 2.9 | 6.0 ± 2.4 | 0.034 |
| How often did you experience stress and anxiety symptoms during the pandemic? (rate on a 1 to 10 scale) ** | 6.9 ± 3.1 | 6.2 ± 3.0 | 6.6 ± 2.7 | 0.466 |
| How would you rate your overall quality of life since the onset of the pandemic compared to before? ** | 5.1 ± 2.2 | 5.8 ± 2.4 | 6.4 ± 3.5 | 0.049 |
| Do you believe the pandemic will influence your cancer prognosis and treatment outcomes? (Yes, %) | 24 (42.9%) | 20 (38.5%) | 15 (27.3%) | 0.213 |
| Have you experienced any changes in social support during the pandemic? (Yes, %) | 29 (51.8%) | 33 (63.5%) | 20 (36.4%) | 0.019 |
| SF-36 (Mean ± SD) | 2020 (n = 56) | 2021 (n = 52) | 2022 (n = 55) | p-Value |
|---|---|---|---|---|
| Physical | 53.0 ± 7.7 | 56.6 ± 7.5 | 55.7 ± 8.0 | 0.043 |
| Mental | 51.0 ± 8.1 | 53.2 ± 8.4 | 54.9 ± 8.6 | 0.049 |
| Total score | 55.9 ± 8.9 | 58.9 ± 8.0 | 59.3 ± 8.8 | 0.077 |
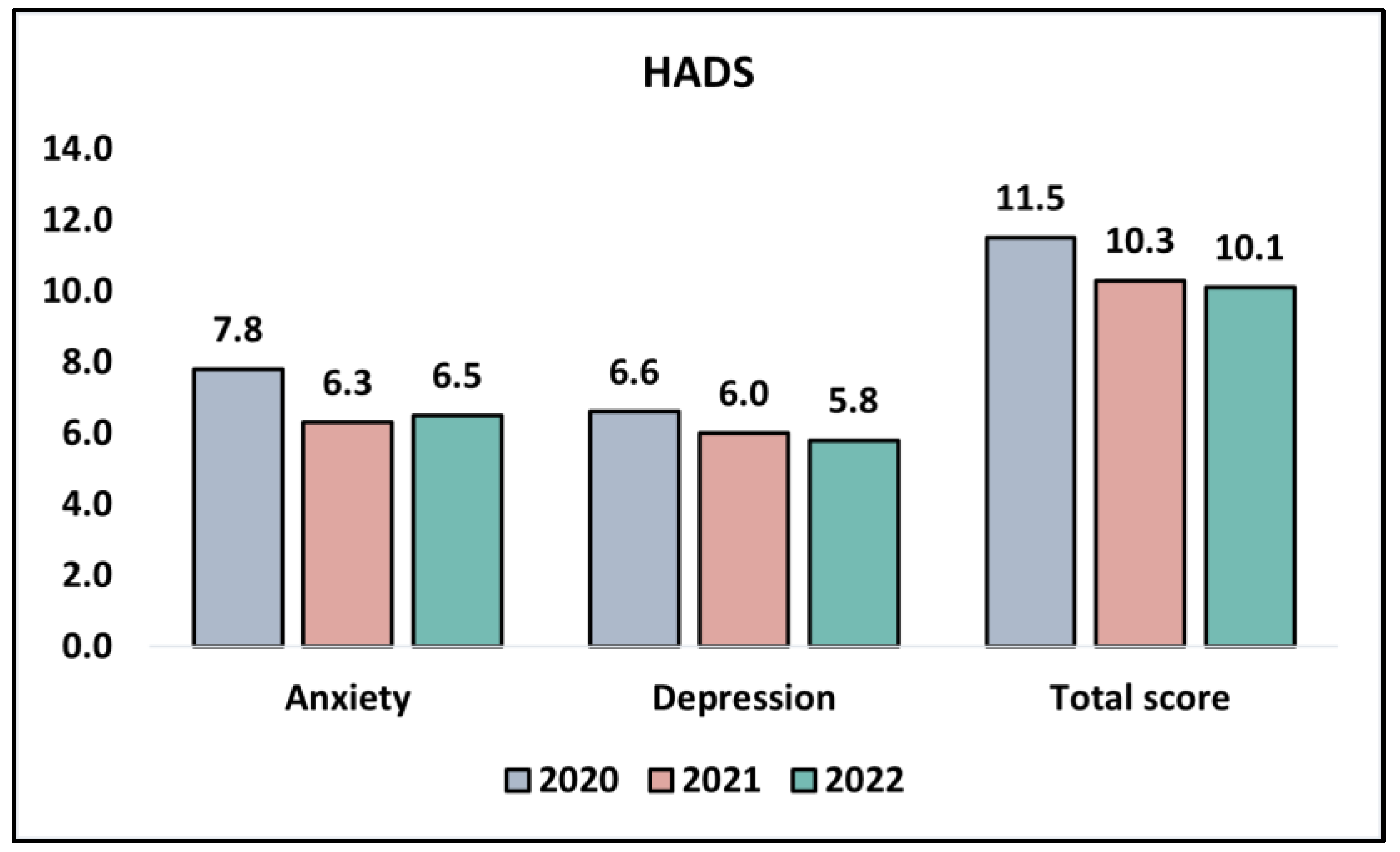
| HADS (Mean ± SD) | 2020 (n = 56) | 2021 (n = 52) | 2022 (n = 55) | p-Value |
|---|---|---|---|---|
| Anxiety | 7.8 ± 2.9 | 6.3 ± 3.0 | 6.5 ± 2.2 | 0.008 |
| Depression | 6.6 ± 2.1 | 6.0 ± 2.8 | 5.8 ± 2.4 | 0.201 |
| Total score | 11.5 ± 5.3 | 10.3 ± 5.0 | 10.1 ± 5.8 | 0.541 |
| Variables (Mean ± SD) | 2020 (n = 56) | 2021 (n = 52) | 2022 (n = 55) | p-Value |
|---|---|---|---|---|
| GAD-7 | 7.8 ± 2.5 | 6.9 ± 2.2 | 6.6 ± 2.8 | 0.034 |
| PHQ-9 | 4.7 ± 2.2 | 4.2 ± 2.6 | 4.0 ± 2.3 | 0.276 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barbos, V.; Feciche, B.; Bratosin, F.; Tummala, D.; Shetty, U.S.A.; Latcu, S.; Croitor, A.; Dema, V.; Bardan, R.; Cumpanas, A.A. Pandemic Stressors and Adaptive Responses: A Longitudinal Analysis of the Quality of Life and Psychosocial Dynamics among Urothelial Cancer Patients. J. Pers. Med. 2023, 13, 1547. https://doi.org/10.3390/jpm13111547
Barbos V, Feciche B, Bratosin F, Tummala D, Shetty USA, Latcu S, Croitor A, Dema V, Bardan R, Cumpanas AA. Pandemic Stressors and Adaptive Responses: A Longitudinal Analysis of the Quality of Life and Psychosocial Dynamics among Urothelial Cancer Patients. Journal of Personalized Medicine. 2023; 13(11):1547. https://doi.org/10.3390/jpm13111547
Chicago/Turabian StyleBarbos, Vlad, Bogdan Feciche, Felix Bratosin, Durganjali Tummala, Uday Shree Akkala Shetty, Silviu Latcu, Alexei Croitor, Vlad Dema, Razvan Bardan, and Alin Adrian Cumpanas. 2023. "Pandemic Stressors and Adaptive Responses: A Longitudinal Analysis of the Quality of Life and Psychosocial Dynamics among Urothelial Cancer Patients" Journal of Personalized Medicine 13, no. 11: 1547. https://doi.org/10.3390/jpm13111547
APA StyleBarbos, V., Feciche, B., Bratosin, F., Tummala, D., Shetty, U. S. A., Latcu, S., Croitor, A., Dema, V., Bardan, R., & Cumpanas, A. A. (2023). Pandemic Stressors and Adaptive Responses: A Longitudinal Analysis of the Quality of Life and Psychosocial Dynamics among Urothelial Cancer Patients. Journal of Personalized Medicine, 13(11), 1547. https://doi.org/10.3390/jpm13111547