
Port Placement Variations for Robotic Lung Resection: Focusing on Their History, Conventional Look-Up-View and Horizontal Open-Thoracotomy-View Techniques, and More

Abstract
:
1. Introduction
2. Material and Methods
2.1. Report Selection
2.2. Categorization
2.3. Visualization
3. Results and Discussion
3.1. Initial Phase: Three-Arm Procedure with a Utility Incision Derived from a Three-Port VATS Lobectomy Technique
3.2. Second Phase: Total Port (Four-Arm) Robotic Surgery without Using Robotic Staplers
3.3. Third Phase: Total Port (Four-Arm) Robotic Surgery Using Robotic Staplers
3.4. Fourth Phase: Maximizing the Functional Features of the Xi System
3.4.1. Fourth Phase A: Horizontal Open-Thoracotomy-View Approaches

3.4.2. Fourth Phase B: Reducing the Number of Ports
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Melfi, F.M.; Menconi, G.F.; Mariani, A.M.; Angeletti, C.A. Early experience with robotic technology for thoracoscopic surgery. Eur. J. Cardio-Thorac. Surg. 2002, 21, 864–868. [Google Scholar] [CrossRef] [Green Version]
- Ashton, R.C., Jr.; Connery, C.P.; Swistel, D.G.; DeRose, J.J., Jr. Robot-assisted lobectomy. J. Thorac. Cardiovasc. Surg. 2003, 126, 292–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, B.J.; Flores, R.M.; Rusch, V. Robotic assistance for video-assisted thoracic surgical lobectomy: Technique and initial results. J. Thorac. Cardiovasc. Surg. 2006, 131, 54–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gharagozloo, F.; Margolis, M.; Tempesta, B. Robot-assisted thoracoscopic lobectomy for early-stage lung cancer. Ann. Thorac. Surg. 2008, 85, 1880–1885. [Google Scholar] [CrossRef]
- Veronesi, G.; Galetta, D.; Maisonneuve, P.; Melfi, F.; Schmid, R.A.; Borri, A.; Vannucci, F.; Spaggiari, L. Four-arm robotic lobectomy for the treatment of early-stage lung cancer. J. Thorac. Cardiovasc. Surg. 2010, 140, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Ninan, M.; Dylewski, M.R. Total port-access robot-assisted pulmonary lobectomy without utility thoracotomy. Eur. J. Cardio-Thorac. Surg. 2010, 38, 231–232. [Google Scholar] [CrossRef] [Green Version]
- Dylewski, M.R.; Ohaeto, A.C.; Pereira, J.F. Pulmonary Resection Using a Total Endoscopic Robotic Video-Assisted Approach. Semin. Thorac. Cardiovasc. Surg. 2011, 23, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Cerfolio, R.J.; Bryant, A.S.; Skylizard, L.; Minnich, D.J. Initial consecutive experience of completely portal robotic pulmonary resection with 4 arms. J. Thorac. Cardiovasc. Surg. 2011, 142, 740–746. [Google Scholar] [CrossRef] [Green Version]
- Pearlstein, D.P. Robotic Lobectomy Utilizing the Robotic Stapler. Ann. Thorac. Surg. 2016, 102, e591–e593. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.P.; Chan, E.Y. “Five on a dice” port placement for robot-assisted thoracoscopic right upper lobectomy using robotic stapler. J. Thorac. Dis. 2017, 9, 5355–5362. [Google Scholar] [CrossRef] [Green Version]
- Khan, N.; Fikfak, V.; Chan, E.Y.; Kim, M.P. “Five on a Dice” Port Placement Allows for Successful Robot-Assisted Left Pneumonectomy. Thorac. Cardiovasc. Surg. Rep. 2017, 6, e42–e44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamazaki, K.; Toyokawa, G.; Shoji, F.; Takeo, S. A novel technique for robotic-assisted lobectomy for lung cancer: The anterior approach. Interact. Cardiovasc. Thorac. Surg. 2020, 30, 328. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, K.; Toyokawa, G.; Kozuma, Y.; Shoji, F.; Shimokawa, M.; Takeo, S. Cumulative experience of the anterior approach in robot-assisted thoracic surgery for lung cancer patients. J. Thorac. Dis. 2021, 13, 5487–5495. [Google Scholar] [CrossRef]
- Funai, K.; Kawase, A.; Mizuno, K.; Koyama, S.; Takanashi, Y.; Shiiya, N. Uniquely modified robotic-assisted thoracic surgery with good intrathoracic visual field. Ann. Thorac. Surg. 2020, 110, e435–e436. [Google Scholar] [CrossRef] [PubMed]
- Sakakura, N.; Nakada, T.; Shirai, S.; Takahara, H.; Nakanishi, K.; Matsui, T.; Ueno, H.; Takahashi, Y.; Kuroda, H. Robotic open-thoracotomy-view approach using vertical port placement and confronting monitor setting. Interact. Cardiovasc. Thorac. Surg. 2021, 33, 60–67. [Google Scholar] [CrossRef]
- Sakakura, N.; Nakada, T.; Takahashi, Y.; Suzuki, A.; Shinohara, S.; Kuroda, H. Three-Arm Robotic Lung Resection via the Open-Thoracotomy-View Approach Using Vertical Port Placement and Confronting Monitor Setting: Focusing on Segmentectomy. J. Pers. Med. 2022, 12, 1771. [Google Scholar] [CrossRef]
- Kang, C.H. The Anterolateral Approach in Robotic Lung Cancer Surgery. Ann. Thorac. Surg. 2019, 108, e401–e403. [Google Scholar] [CrossRef] [PubMed]
- Ueda, K.; Umehara, T.; Maeda, K.; Suzuki, S.; Yokomakura, N.; Kariatsumari, K.; Sato, M. Three-incision robotic major lung resection for cancer. Transl. Cancer Res. 2021, 10, 4617–4623. [Google Scholar] [CrossRef]
- Han, K.N.; Lee, J.H.; Hong, J.I.; Kim, H.K. Comparison of two-port and three-port approaches in robotic lobectomy for non-small cell lung cancer. World, J. Surg. 2022, 46, 2517–2525. [Google Scholar] [CrossRef]
- Yang, Y.; Song, L.; Huang, J.; Cheng, X.; Luo, Q. A uniportal right upper lobectomy by three-arm robotic-assisted thoracoscopic surgery using the da Vinci (Xi) Surgical System in the treatment of early-stage lung cancer. Transl. Lung Cancer Res. 2021, 10, 1571–1575. [Google Scholar] [CrossRef]
- Gonzalez-Rivas, D.; Bosinceanu, M.; Motas, N.; Manolache, V. Uniportal robotic-assisted thoracic surgery for lung resections. Eur. J. Cardiothorac. Surg. 2022, 62, ezac410. [Google Scholar] [CrossRef]
- Bodner, J.; Wykypiel, H.; Wetscher, G.; Schmid, T. First experiences with the da vinci™ operating robot in thoracic surgery. Eur. J. Cardio-Thorac. Surg. 2004, 25, 844–851. [Google Scholar] [CrossRef] [Green Version]
- Cerfolio, R.J.; Bryant, A.S. Robotic-assisted pulmonary resection - Right upper lobectomy. Ann. Cardiothorac. Surg. 2012, 1, 77–85. [Google Scholar]
- Cerfolio, R.J. Total port approach for robotic lobectomy. Thorac. Surg. Clin. 2014, 24, 151–156. [Google Scholar] [CrossRef]
- Cerfolio, R.J.; Watson, C.; Minnich, D.J.; Calloway, S.; Wei, B. One hundred planned robotic segmentectomies: Early results, technical details, and preferred port placement. Ann. Thorac. Surg. 2016, 101, 1089–1095. [Google Scholar] [CrossRef] [Green Version]
- Veronesi, G.; Novellis, P.; Voulaz, E.; Alloisio, M. Robot-assisted surgery for lung cancer: State of the art and perspectives. Lung Cancer 2016, 101, 28–34. [Google Scholar] [CrossRef]
- Veronesi, G.; Novellis, P.; Difrancesco, O.; Dylewski, M. Robotic assisted lobectomy for locally advanced lung cancer. J. Vis. Surg. 2017, 3, 78. [Google Scholar] [CrossRef] [Green Version]
- Sakakura, N.; Nakada, T.; Shirai, S.; Takahara, H.; Suzuki, A.; Takahashi, Y.; Kuroda, H. Emergency rollout and conversion procedures during the three-arm robotic open-thoracotomy-view approach. Interact. Cardiovasc. Thorac. Surg. 2022, 34, 1045–1051. [Google Scholar] [CrossRef]
- Eguchi, T.; Miura, K.; Hamanaka, K.; Shimizu, K. Robotic segmentectomy using a lung base-flip approach. JTCVS Tech. 2022, 15, 174–176. [Google Scholar] [CrossRef]
- Eguchi, T.; Miura, K.; Hamanaka, K.; Shimizu, K. Adoption of Robotic Core Technology in Minimally Invasive Lung Segmentectomy: Review. J. Pers. Med. 2022, 12, 1417. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author/Year [Reference] | da Vinci System | View Type | Number of Skin Incisions a | Number of Robot Arms b | Scope Type | Location of Scope (ICS) | Location of Utility Port for Assistant (ICS) | CO2 Insufflation | Number of Patients [Reference] | Features |
|---|---|---|---|---|---|---|---|---|---|---|
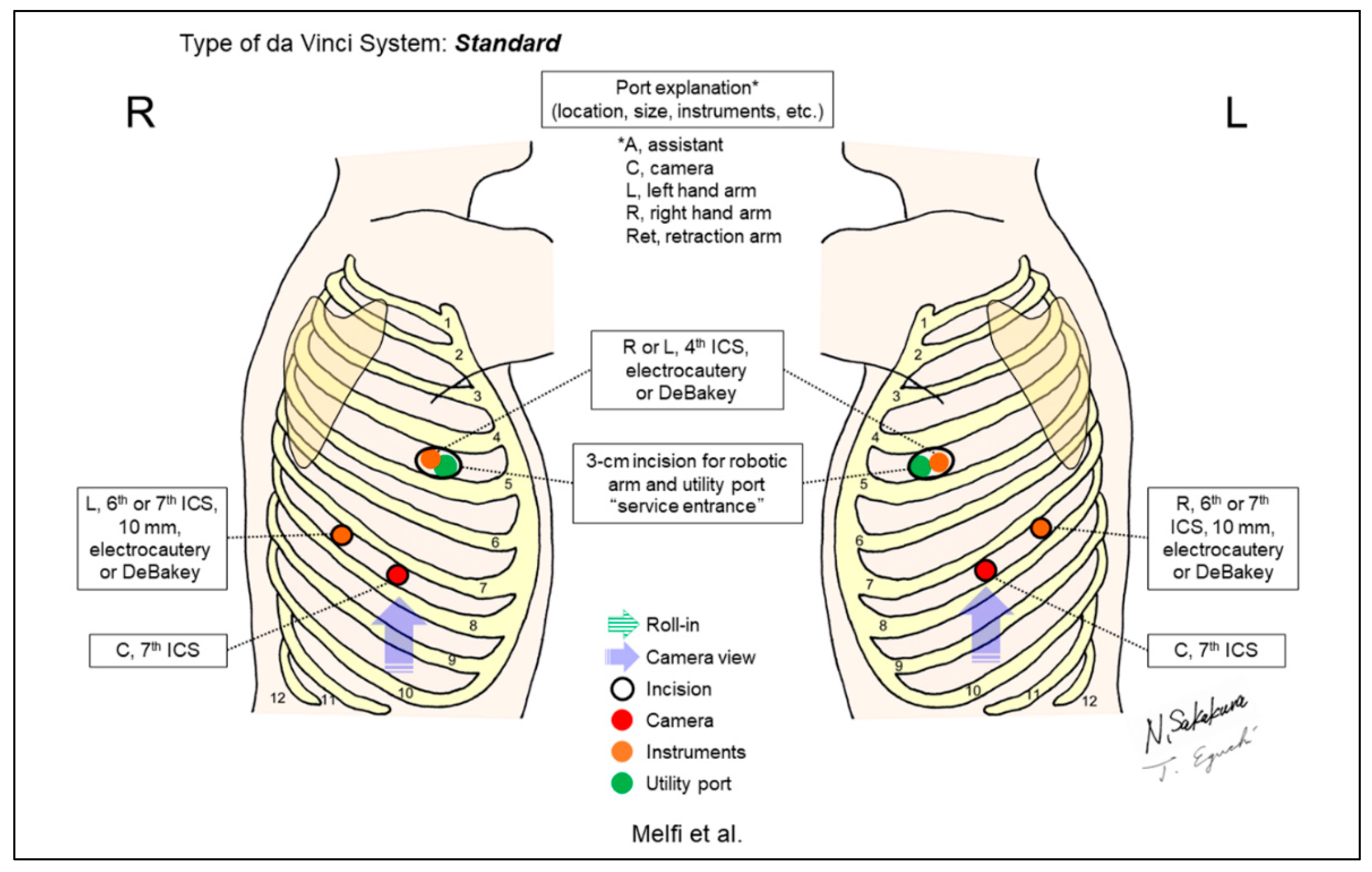
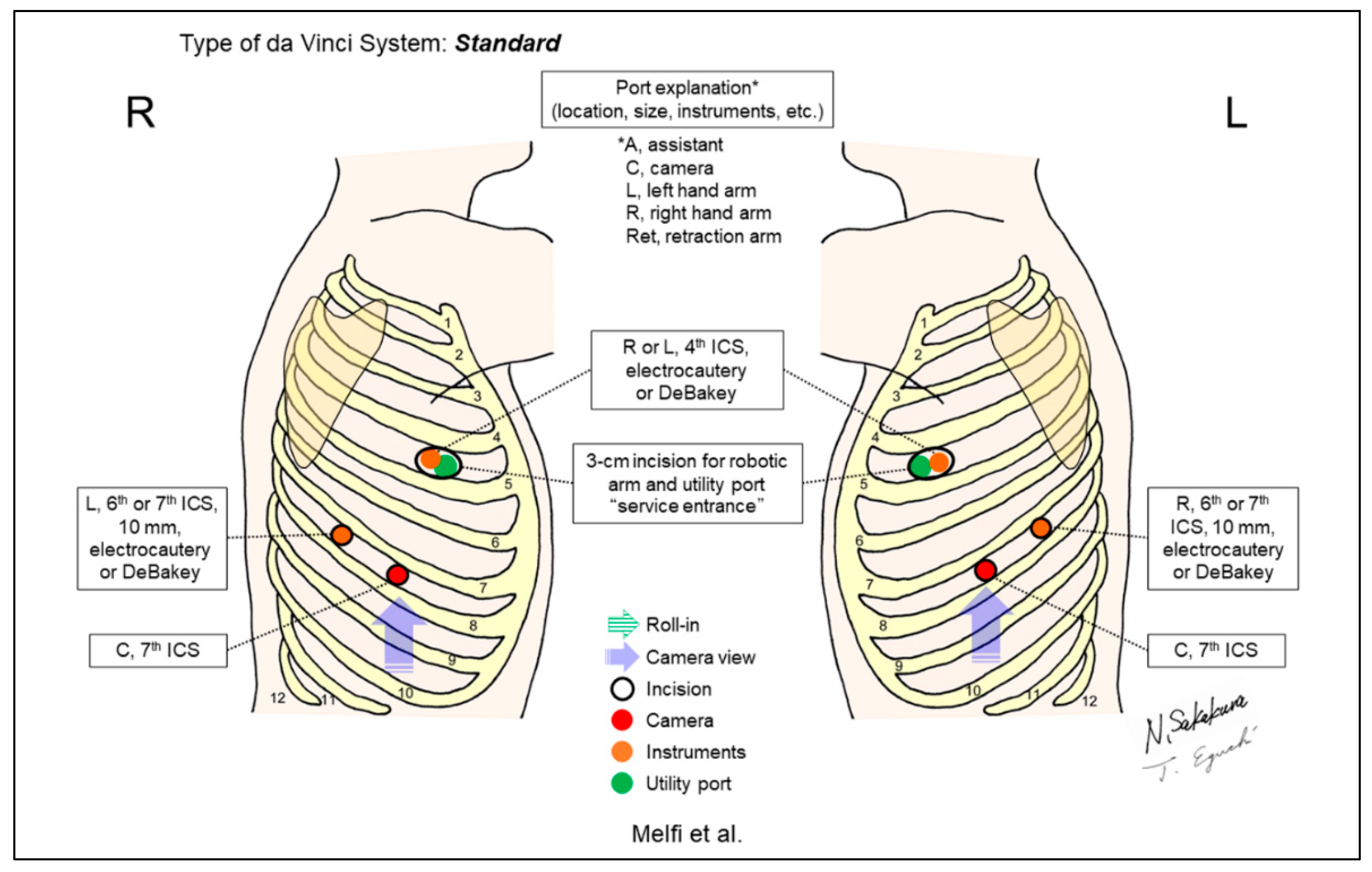
| Melfi 2002 [1] | Standard c | Look-up | 3 | 3 | 0-degree | 7th | 4th | No | 12 (5 lower lobectomies) | The first report on robotic surgery for thoracic diseases. A utility incision “service entrance” is placed at the 4th ICS, which is shared for an assistant and a robotic arm. |
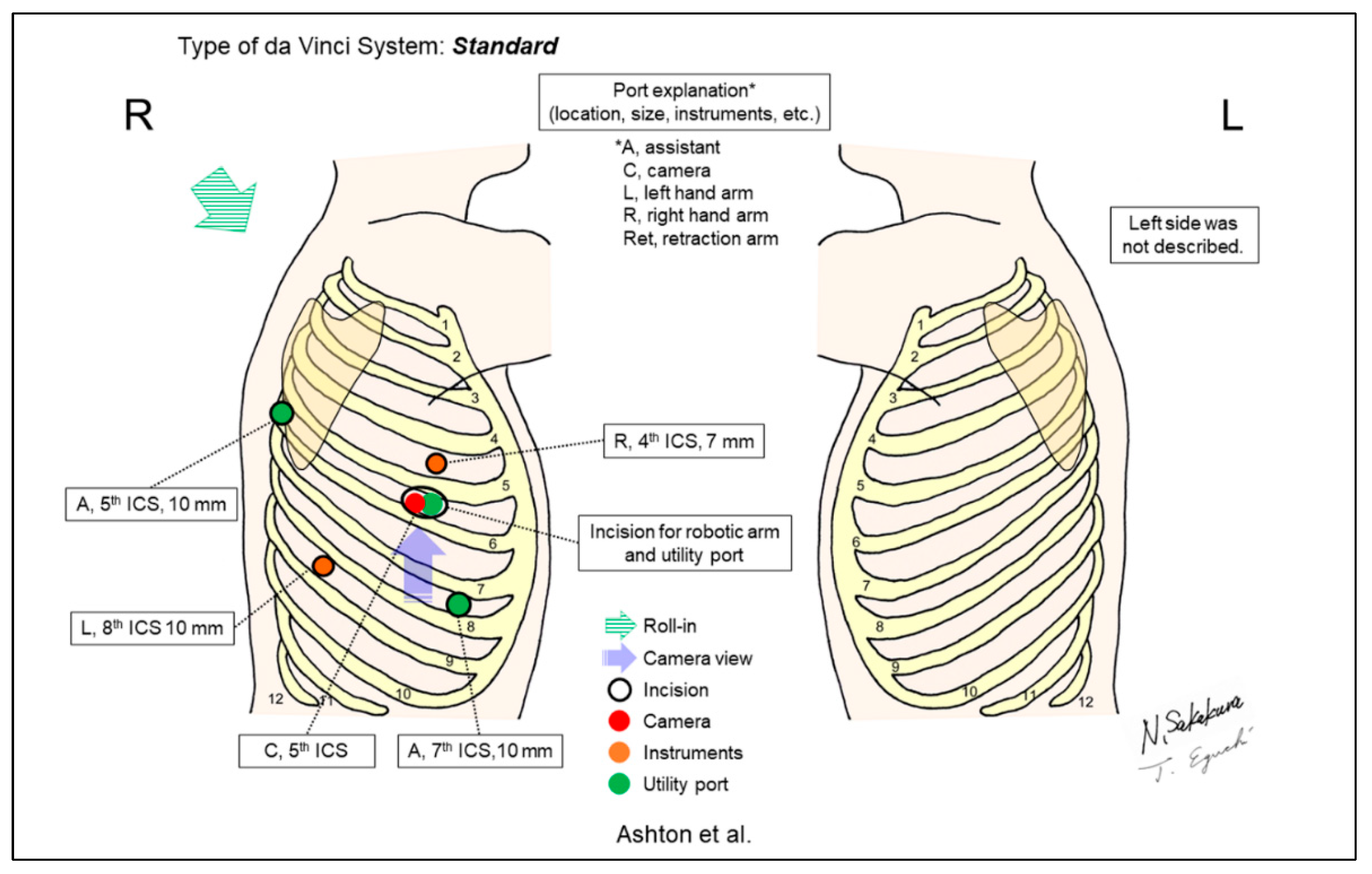
| Ashton/2003 [2] | Standard c | Look-up | 5 | 3 | 0-degree | 5th | 3 utility ports, anterior 5th, 7th, and posterior 5th | No | 1 (lower lobectomy) | Three utility incisions were placed at the anterior 5th, 7th, and posterior 5th ICSs. The anterior 5th ICS was shared with a robotic scope. |
| Park/2006 [3] | Standard c | Look-up | 3 | 3 | 30-degree, down/up | 7–8th | Superior pulmonary vein level or one ICS lower | No | 34 | The incisions used for authors’ thoracoscopic lobectomy were applied. A utility incision is placed at the level of the superior pulmonary vein or one ICS lower, which is shared for an assistant and a robotic arm. |
| Gharagozloo/2008 [4] | ND d | Look-up | 4 | 3 | ND | 8th | ND | ND | 61 | A hybrid robotic-VATS technique. In addition to 3 robotic ports, a 1cm assistant port for an endoretractor was placed. Authors used a robot to dissect the pulmonary artery and the hilum. Once dissection was completed, the robot was withdrawn, and lobectomy was completed by VATS. |
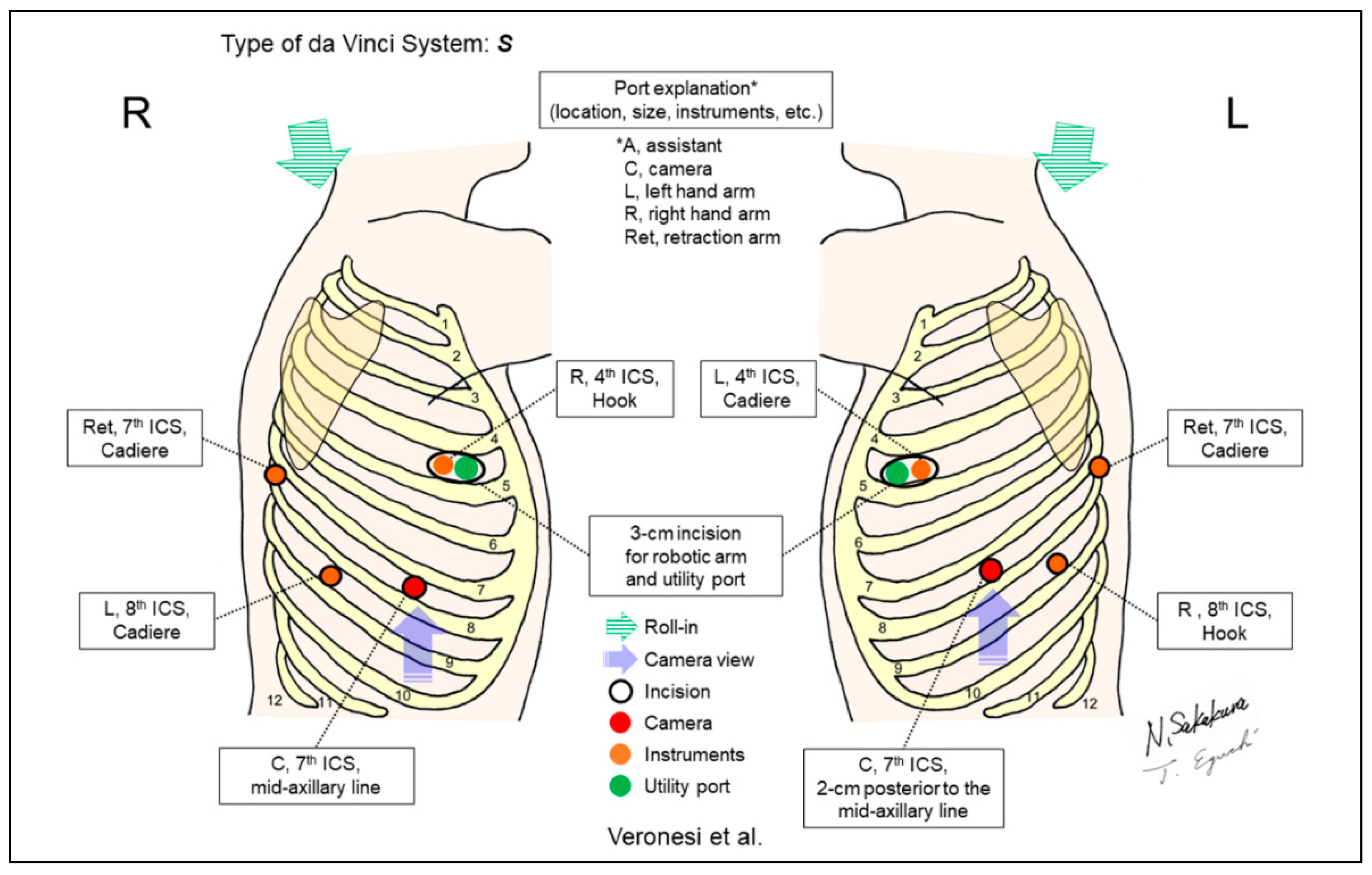
| Veronesi/2010 [5] | S e | Look-up | 4 | 4 | ND | 7th | 4th | No | 54 | A posterior port for the 4th retraction arm was placed. The additional retraction by the 4th arm could reduce the requirement to change instruments and avoid possible interferences between robotic and assistant’s instruments. |
| Ninan/2010 [6] Dylewski/2011 [7] | ND d | Look-up | 4 or 5 | 3 or 4 | 0-degree | 5–7th | Subcostal | Yes | 74 [6], 200 [7] | The “total endoscopic robotic video-assisted approach.” The subcostal trans-diaphragmatic incision was placed for a utility port by a bedside assistant. |
| Cerfolio/2011 [8] | ND d | Look-up | 5 | 4 | ND | 7th | 9–10th | Yes | 106 (robotic lobectomies) | The “completely portal robotic pulmonary lobectomy with 4 arms (CPRL-4).” |
| Pearlstein/2016 [9] | Xi | Look-up | 5 | 4 | 0-degree | 7th | 9th | ND | ND | Specific techniques to use robotic staplers were described. Locating the stapling ports as low caudal as possible (close to the diaphragm) allows the greatest degree of maneuverability of the stapler in the chest. |
| Kim/2017 [10] Khan/2017 [11] | Xi | Look-up | 5 | 4 | 30-degree c | 7th | 4th | Yes | ND | “Five on a dice” method. Improved control of vascular stapler via inferior ports in the both sides and good retraction of the lung using tip-up grasper with sponge. A challenging robotic left pneumonectomy was performed [11]. |
| Yamazaki/2020 [12], 2021 [13] | Si | Horizontal | 5 | 4 | 30-degree, down | 4th | 7–9th | Yes | 87 (anterior approach) [13] | “Anterior approach” technique. Intrathorax is always viewed from the ventral side of the patient regardless of the side to be operated on. |
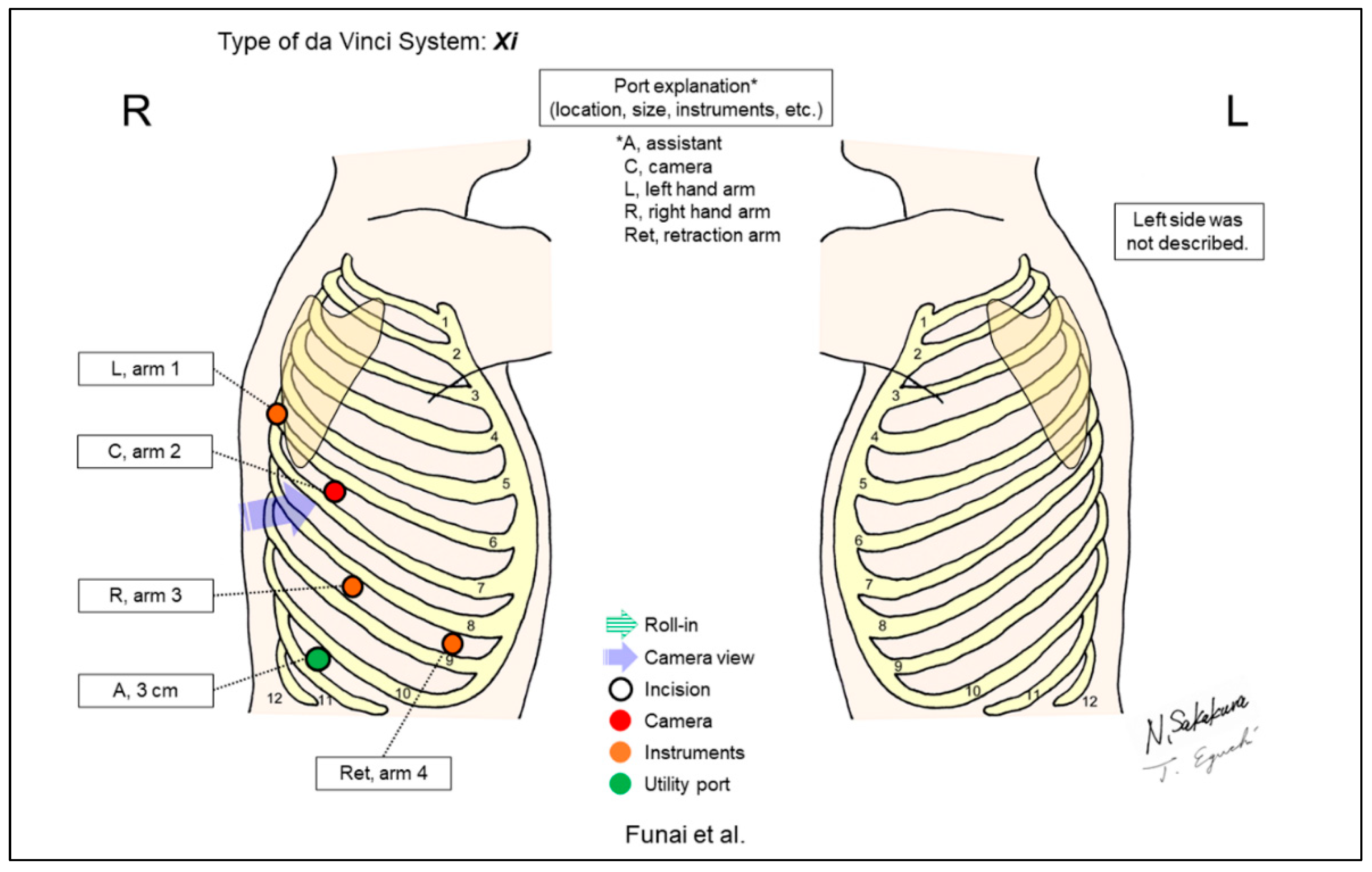
| Funai/2020 [14] | Xi | Horizontal | 5 | 4 | ND | 5th | 10th | Yes | ND | A four-arm, horizontal-view approach, the “Hamamatsu method.” A change of port distribution from the conventional Cerfolio’s CPRL-4 technique was shown on the right-side surgery. |
| Sakakura/2021 [15], 2022 [16] | Xi | Horizontal | 4 | 3 | 30-degree, down/up | Right 5–6th, Left 4–6th | Right 5–7th, Left 7–9th | Yes | 58 [15], 114 [16] | “Three-arm, open-thoracotomy-view approach” using vertical port placement and confronting up-side down monitor setting. All surgeons obtain “bird-eye” views as though they perform thoracotomy surgery. Ventral/dorsal hilum becomes visible by switching the 30-degree camera down/up. |
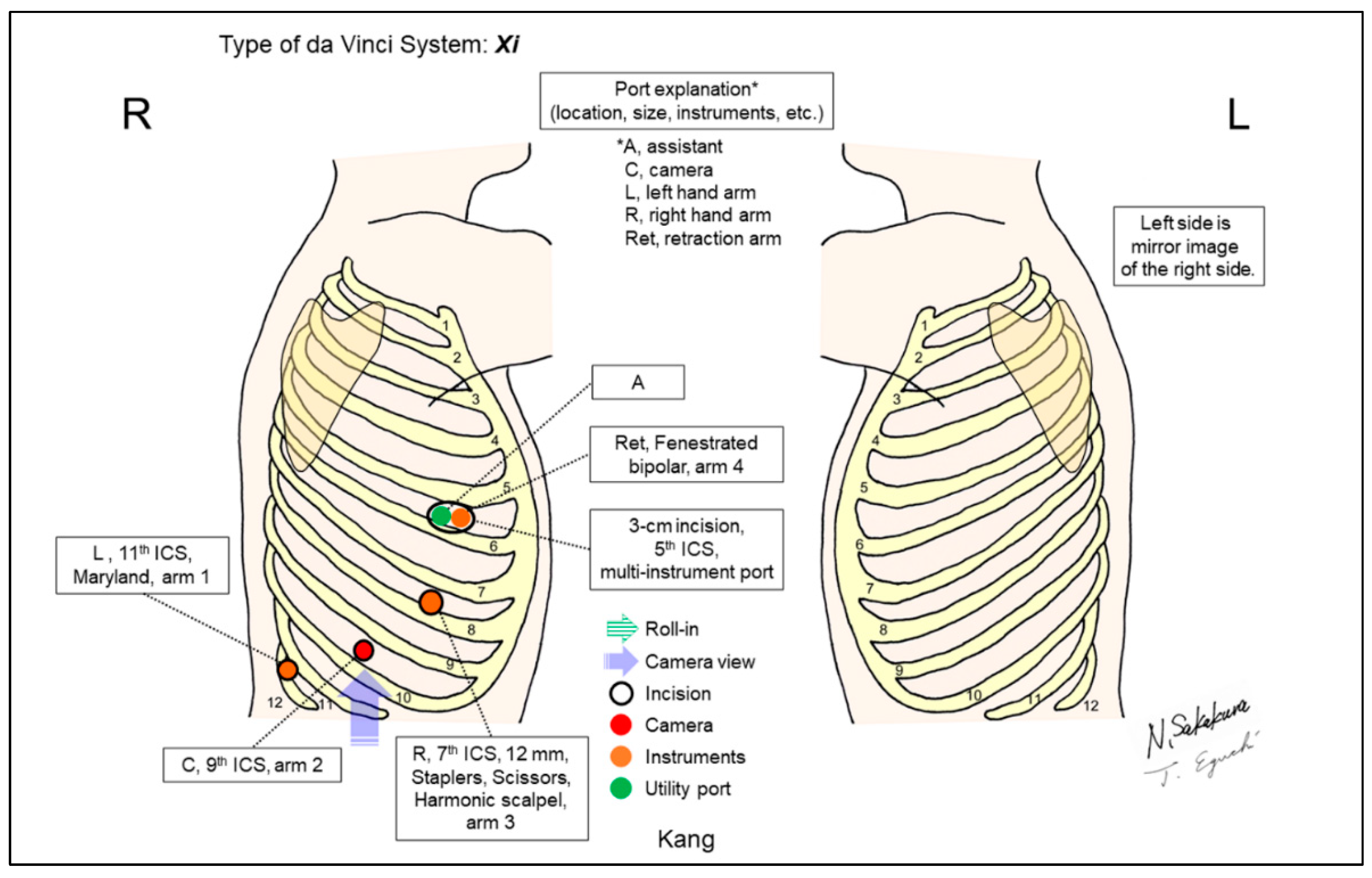
| Kang/2019 [17] | Xi | Look-up | 4 | 4 | ND | 9th | 5th | Yes | 36 | “Anterolateral approach.” A utility port in the 5th ICS shares with a robotic arm. Fully use the 4-arm technique, minimize the assistant’s role and establish a solo surgical method, and avoid painful posterior ports. |
| Ueda/2021 [18] | Xi | Look-up | 3 | 3 | 30-degree, down | 8th | 5th | No | 39 | A “three-incision robotic surgery.” A 4cm incision was shared for two robotic arms (scope and instrument). Interference between the two arms were prevented by “para-axial method.” |
| Han/2022 [19] | Xi | Look-up | 2 or 3 | 3 | ND | 7–8th | 7–8th | Yes | 142 | A matched analysis for “two-port” and “three-port” approaches. In the two-port setting, a 3–4cm working port was shared for two robotic arms (scope and instrument) and an additional assistant instrument using multi-instrument laparoscopic port. |
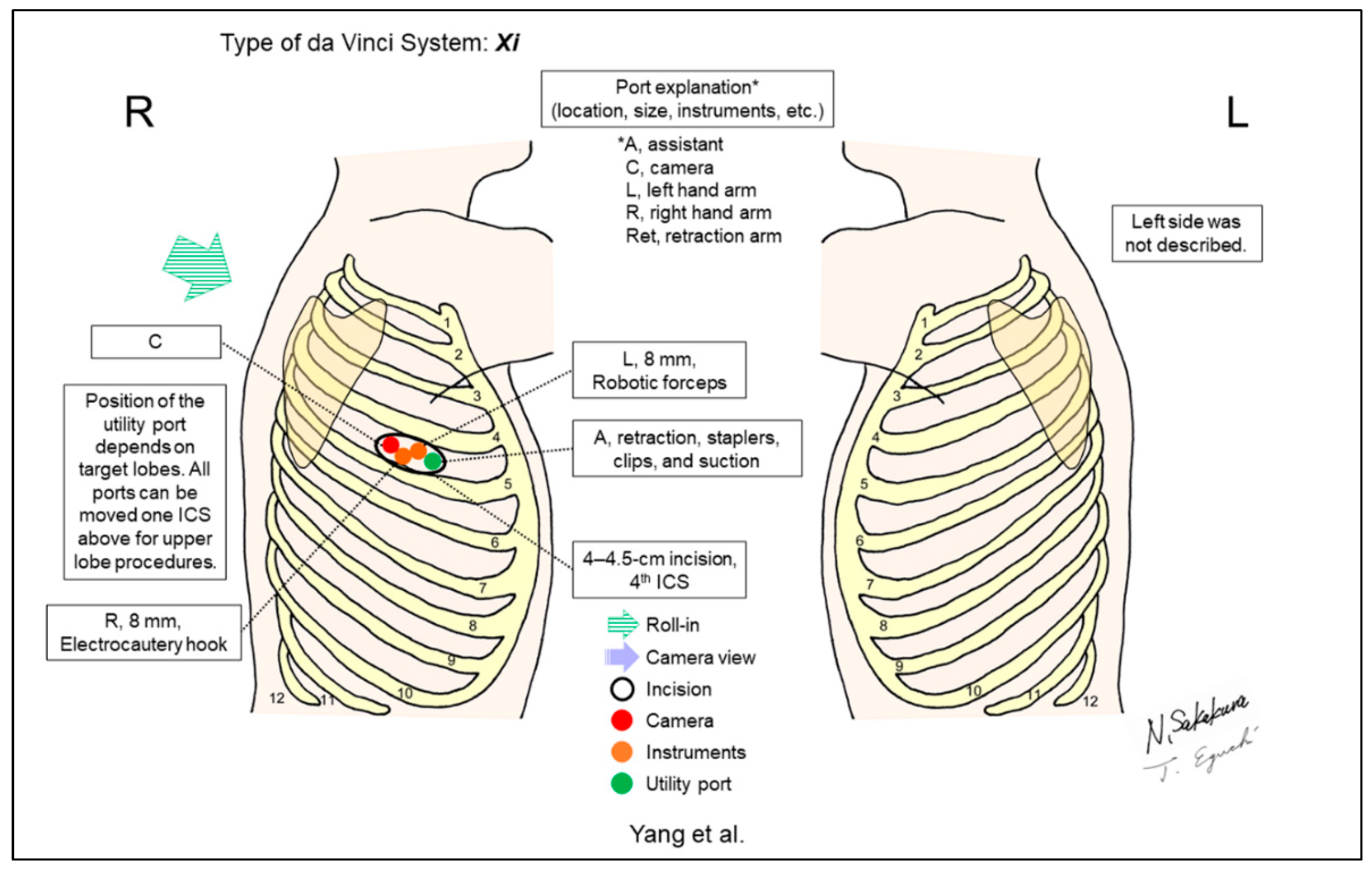
| Yang/2021 [20] | Xi | Undefined f | 1 | 3 | 30-degree | 4th | 4th | No | 1 (right upper lobectomy) | Uniportal RATS. A single 4–4.5cm incision was created to be shared by three robotic arms and the assistant. Robotic arms were intercrossed inside the chest and the control of the arms needed to be reset on the console accordingly. |
| Gonzalez-Rivas/2022 [21] | Xi | Undefined f | 1 | 3 | ND | ND | ND | No | ND | Pure uniportal RATS. To avoid collision, cancel arm 1 on the right side (arm 2 for camera) and arm 4 on the left side (arm 3 for camera). The camera is placed in the posterior part of the incision to allow the other two robotic instruments to work. All types of lung resections, including segmentectomies, sleeves and carinal resections were performed. |
| Eguchi (Shinshu University, unpublished data) | Si | Look-up | 5 | 4 | 0-degree | 6–7th | 7–10th | Yes | 180 (50 lobectomies, 130 segmentectomies, unpublished data) | A modification of Cerfolio’s setting. Moving the three ventral ports from the Cerfolio setting to the one or two ICS cranial side to avoid port collisions, considering the smaller body sizes of Asians compared to Westerners. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sakakura, N.; Eguchi, T. Port Placement Variations for Robotic Lung Resection: Focusing on Their History, Conventional Look-Up-View and Horizontal Open-Thoracotomy-View Techniques, and More. J. Pers. Med. 2023, 13, 230. https://doi.org/10.3390/jpm13020230
Sakakura N, Eguchi T. Port Placement Variations for Robotic Lung Resection: Focusing on Their History, Conventional Look-Up-View and Horizontal Open-Thoracotomy-View Techniques, and More. Journal of Personalized Medicine. 2023; 13(2):230. https://doi.org/10.3390/jpm13020230
Chicago/Turabian StyleSakakura, Noriaki, and Takashi Eguchi. 2023. "Port Placement Variations for Robotic Lung Resection: Focusing on Their History, Conventional Look-Up-View and Horizontal Open-Thoracotomy-View Techniques, and More" Journal of Personalized Medicine 13, no. 2: 230. https://doi.org/10.3390/jpm13020230