
Discontinuing Hepatitis Activity Reduced Hepatocellular Carcinoma Recurrence after Primary Curative Therapy


Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinicopathological Characteristics of the Studied Patients
2.2. Diagnosis of HCC
2.3. Follow-Up Studies
2.4. Statistical Analysis
3. Results
3.1. Clinical Characteristics of the Patients
3.2. Risk Factor Selection
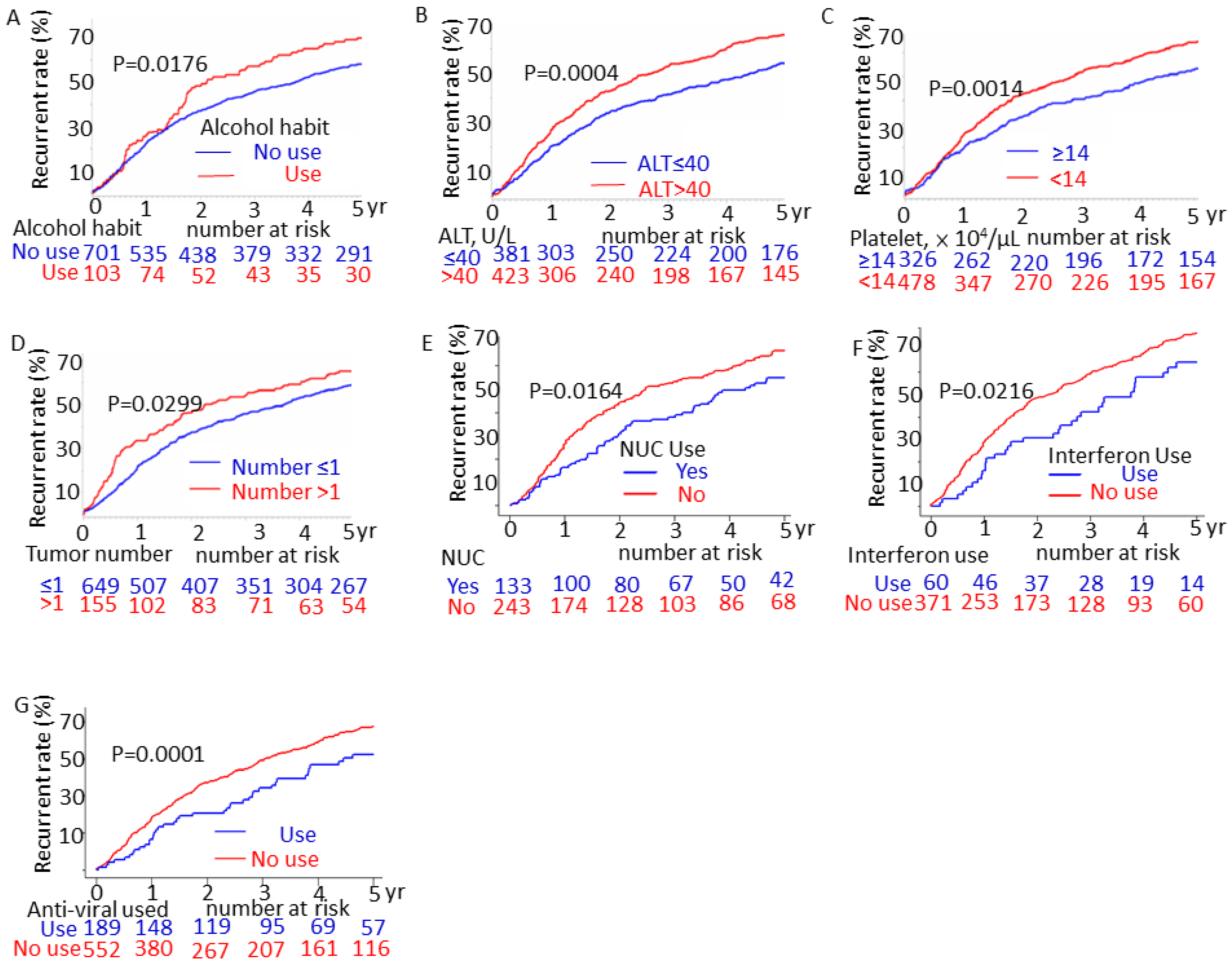
3.3. Comparison of HCC Recurrence Rates through the Log-Rank Test
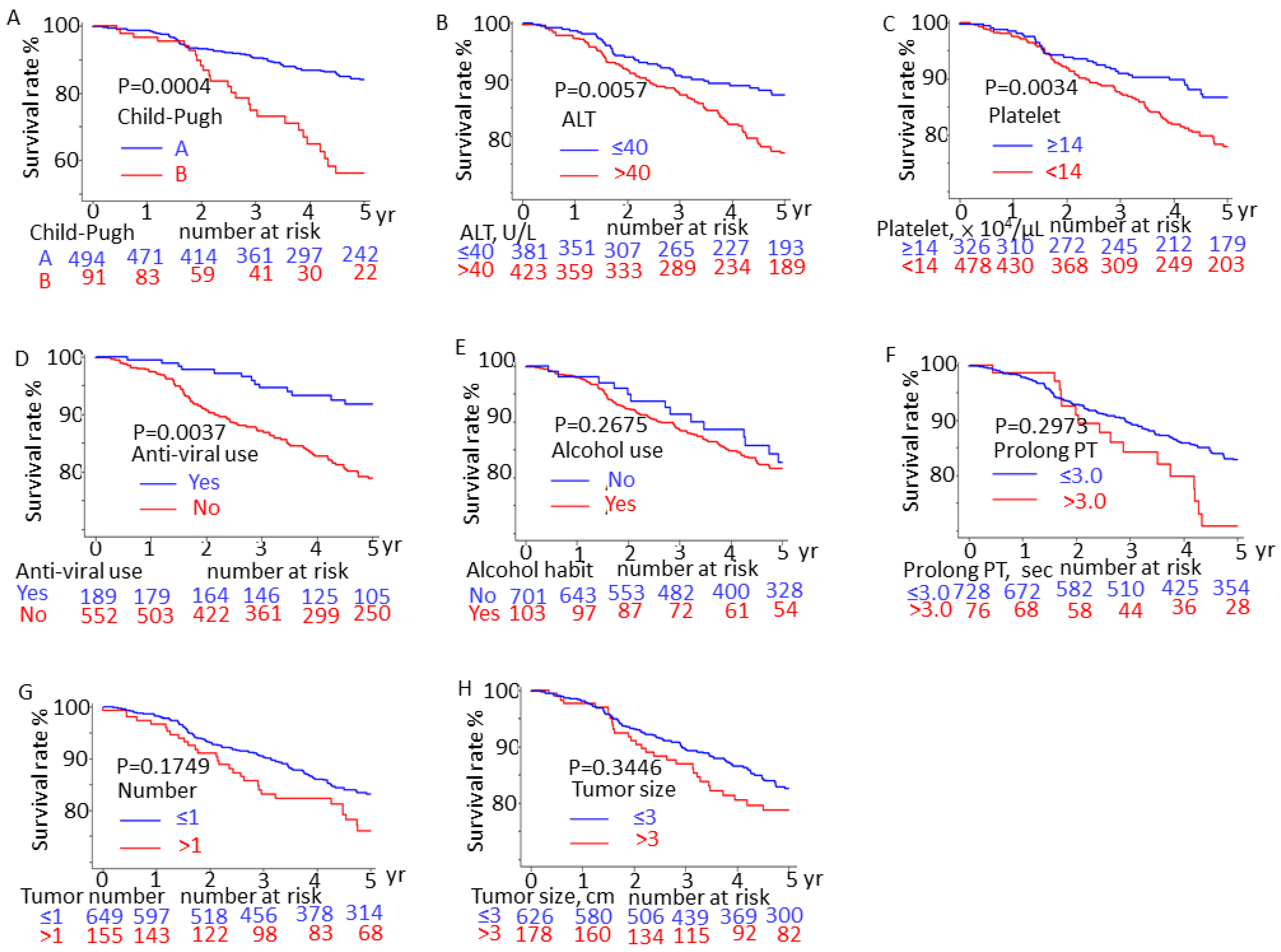
3.4. Survival Rates of Patients with HCC with and without Confounding Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fitzmaurice, C.; Abate, D.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdel-Rahman, O.; Abdelalim, A.; Abdoli, A.; Abdollahpour, I.; Abdulle, A.S.M.; et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 1990 to 2017: A systematic analysis for the global burden of disease study. JAMA Oncol. 2019, 5, 1749–1768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsieh, C.-H.; Wei, C.-K.; Yin, W.-Y.; Chang, C.-M.; Tsai, S.-J.; Wang, L.-Y.; Chiou, W.-Y.; Lee, M.-S.; Lin, H.-Y.; Hung, S.-K. Vascular invasion affects survival in early hepatocellular carcinoma. Mol. Clin. Oncol. 2015, 3, 252–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, B.; Yang, X.-R.; Xu, Y.; Sun, Y.-F.; Sun, C.; Guo, W.; Zhang, X.; Wang, W.-M.; Qiu, S.-J.; Zhou, J.; et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin. Cancer Res. 2014, 20, 6212–6222. [Google Scholar] [CrossRef] [Green Version]
- Sugawara, Y.; Hibi, T. Surgical treatment of hepatocellular carcinoma. Biosci. Trends 2021, 15, 138–141. [Google Scholar] [CrossRef]
- Nagasue, N.; Uchida, M.; Makino, Y.; Takemoto, Y.; Yamanoi, A.; Hayashi, T.; Chang, Y.-C.; Kohno, H.; Nakamura, T.; Yukaya, H. Incidence and factors associated with intrahepatic recurrence following resection of hepatocellular carcinoma. Gastroenterology 1993, 105, 488–494. [Google Scholar] [CrossRef]
- Valenzuela, A.; Ha, N.B.; Gallo, A.; Bonham, C.; Ahmed, A.; Melcher, M.; Kim, L.H.; Esquivel, C.; Concepcion, W.; Ayoub, W.S.; et al. Recurrent hepatocellular carcinoma and poorer overall survival in patients undergoing left-sided compared with right-sided partial hepatectomy. J. Clin. Gastroenterol. 2015, 49, 158–164. [Google Scholar] [CrossRef]
- Chen, Q.; Shu, C.; Laurence, A.D.; Chen, Y.; Peng, B.-G.; Zhen, Z.-J.; Cai, J.-Q.; Ding, Y.-T.; Li, L.-Q.; Zhang, Y.-B.; et al. Effect of huaier granule on recurrence after curative resection of hcc: A multicentre, randomised clinical trial. Gut 2018, 67, 2006–2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, L.; Wang, S.-B.; Chen, S.-G.; Qu, Q.; Rui, J.-A. Prognostic value of alt, ast, and aar in hepatocellular carcinoma with b-type hepatitis-associated cirrhosis after radical hepatectomy. Clin. Lab. 2018, 64, 1739–1747. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Wang, D.; Liu, H.; Li, H. Tenofovir decrease hepatocellular carcinoma recurrence in chronic hepatitis b patients after liver resection. Infect. Agent Cancer 2018, 13, 19. [Google Scholar] [CrossRef] [Green Version]
- Yu, D.; Holmes, S.; Uhanova, J.; Lipschitz, J.; McKay, A.; Gerald, M.Y. Predicting hepatocellular carcinoma recurrence and survival. Hepato-Gastroenterol. 2014, 61, 776–783. [Google Scholar]
- Fuke, H.; Sugimoto, K.; Shiraki, K.; Tanaka, J.; Beppu, T.; Yoneda, K.; Yamamoto, N.; Ito, K.; Takaki, H.; Nakatsuka, A.; et al. Predictive factors for distant recurrence of hcv-related hepatocellular carcinoma after radiofrequency ablation combined with chemoembolization. Aliment. Pharmacol. Ther. 2008, 27, 1253–1260. [Google Scholar] [CrossRef] [PubMed]
- Idilman, R.; Demir, M.; Aladag, M.; Erol, C.; Cavus, B.; Iliaz, R.; Koklu, H.; Cakaloglu, Y.; Sahin, M.; Ersoz, G.; et al. Low recurrence rate of hepatocellular carcinoma following ledipasvir and sofosbuvir treatment in a real-world chronic hepatitis c patients cohort. J. Viral Hepat. 2019, 26, 666–674. [Google Scholar] [CrossRef] [PubMed]
- Hoyos, S.; Escobar, J.; Cardona, D.; Guzmán, C.; Mena, Á.; Osorio, G.; Pérez, C.; Restrepo, J.C.; Correa, G. Factors associated with recurrence and survival in liver transplant patients with hcc—A single center retrospective study. Ann. Hepatol. 2015, 14, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.C.; Ho, C.M.; Hu, R.H.; Ho, M.C.; Wu, Y.M.; Lee, P.H. Prophylactic liver transplantation for high-risk recurrent hepatocellular carcinoma. World J. Hepatol. 2016, 8, 1309–1317. [Google Scholar] [CrossRef] [PubMed]
- Tanimine, N.; Tanaka, Y.; Kobayashi, T.; Tashiro, H.; Miki, D.; Imamura, M.; Aikata, H.; Tanaka, J.; Chayama, K.; Ohdan, H. Quantitative effect of natural killer-cell licensing on hepatocellular carcinoma recurrence after curative hepatectomy. Cancer Immunol. Res. 2014, 2, 1142–1147. [Google Scholar] [CrossRef] [Green Version]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. Bclc strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef]
- Wu, C.Y.; Chen, Y.J.; Ho, H.J.; Hsu, Y.C.; Kuo, K.N.; Wu, M.S.; Lin, J.T. Association between nucleoside analogues and risk of hepatitis b virus–related hepatocellular carcinoma recurrence following liver resection. JAMA 2012, 308, 1906–1914. [Google Scholar] [CrossRef] [Green Version]
- Omata, M.; Cheng, A.-L.; Kokudo, N.; Kudo, M.; Lee, J.M.; Jia, J.; Tateishi, R.; Han, K.-H.; Chawla, Y.K.; Shiina, S.; et al. Asia-pacific clinical practice guidelines on the management of hepatocellular carcinoma: A 2017 update. Hepatol. Int. 2017, 11, 317–370. [Google Scholar] [CrossRef] [Green Version]
- Taniai, M. Alcohol and hepatocarcinogenesis. Clin. Mol. Hepatol. 2020, 26, 736–741. [Google Scholar] [CrossRef]
- Chao, X.; Ding, W.X. Role and mechanisms of autophagy in alcohol-induced liver injury. Adv. Pharmacol. 2019, 85, 109–131. [Google Scholar] [CrossRef]
- Ceni, E.; Mello, T.; Galli, A. Pathogenesis of alcoholic liver disease: Role of oxidative metabolism. World J. Gastroenterol. 2014, 20, 17756–17772. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.; Kumar, R.; Hissar, S.S.; Saraswat, M.K.; Sharma, B.C.; Sakhuja, P.; Sarin, S.K. Risk factors analysis for hepatocellular carcinoma in patients with and without cirrhosis: A case-control study of 213 hepatocellular carcinoma patients from india. J. Gastroenterol. Hepatol. 2007, 22, 1104–1111. [Google Scholar] [CrossRef] [PubMed]
- Marié, C.; Fouquet, G.; Courtois, A.; Amrathlal, R.S.; Jankovsky, N.; Ouled-Haddou, H.; Tebbakha, R.; Bouhlal, H.; Nguyen-Khac, È.; Naassila, M.; et al. Mechanisms of chronic alcohol exposure-induced aggressiveness in cellular model of hcc and recovery after alcohol withdrawal. Cell Mol. Life Sci. 2022, 79, 366. [Google Scholar] [CrossRef] [PubMed]
- Bishayee, A. The role of inflammation and liver cancer. Adv. Exp. Med. Biol. 2014, 816, 401–435. [Google Scholar] [CrossRef]
- Kwon, O.S.; Choi, S.H.; Kim, J.H. Inflammation and hepatic fibrosis, then hepatocellular carcinoma. Korean J. Gastroenterol. 2015, 66, 320–324. [Google Scholar] [CrossRef]
- D’Souza, S.; Lau, K.C.; Coffin, C.S.; Patel, T.R. Molecular mechanisms of viral hepatitis induced hepatocellular carcinoma. World J. Gastroenterol. 2020, 26, 5759–5783. [Google Scholar] [CrossRef]
- Ishikawa, T. Anti-viral therapy to reduce recurrence and improve survival in hepatitis b virus-related hepatocellular carcinoma. World J. Gastroenterol. 2013, 19, 8861–8866. [Google Scholar] [CrossRef]
- Chen, V.L.; Yeh, M.-L.; Le, A.K.; Jun, M.; Saeed, W.K.; Yang, J.D.; Huang, C.-F.; Lee, H.Y.; Tsai, P.-C.; Lee, M.-H.; et al. Anti-viral therapy is associated with improved survival but is underutilised in patients with hepatitis b virus-related hepatocellular carcinoma: Real-world east and west experience. Aliment. Pharmacol. Ther. 2018, 48, 44–54. [Google Scholar] [CrossRef] [Green Version]
- Liaw, Y.-F.; Sung, J.J.Y.; Chow, W.C.; Farrell, G.; Lee, C.-Z.; Yuen, H.; Tanwandee, T.; Tao, Q.-M.; Shue, K.; Keene, O.N.; et al. Lamivudine for patients with chronic hepatitis b and advanced liver disease. N. Engl. J. Med. 2004, 351, 1521–1531. [Google Scholar] [CrossRef]
- Syed, T.; Fazili, J.D.; Ali, I.A.; Zhao, D.; Hughes, D.; Mahmood, S.M. Hepatocellular carcinoma occurrence and recurrence in hepatitis c-infected patients treated with direct-acting antivirals. Cureus 2018, 10, e2843. [Google Scholar] [CrossRef] [Green Version]
- Zanetto, A.; Senzolo, M.; Campello, E.; Bulato, C.; Gavasso, S.; Shalaby, S.; Gambato, M.; Vitale, A.; Cillo, U.; Farinati, F.; et al. Influence of hepatocellular carcinoma on platelet aggregation in cirrhosis. Cancers 2021, 13, 1150. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Lin, Y.J.; Lin, C.C.; Yen, C.L.; Shen, C.H.; Chang, C.J.; Hsieh, S.Y. Pretreatment platelet count early predicts extrahepatic metastasis of human hepatoma. Liver Int. 2015, 35, 2327–2336. [Google Scholar] [CrossRef] [PubMed]
- Peck-Radosavljevic, M. Thrombocytopenia in chronic liver disease. Liver Int. 2017, 37, 778–793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, Y.; Muheremu, A.; Wu, X.; Liu, J. Relationship between platelet parameters and hepatic pathology in patients with chronic hepatitis b infection—A retrospective cohort study of 677 patients. J. Int. Med. Res. 2016, 44, 779–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, W.; Li, C.; Zhang, X.; Wen, T.; Chen, Z. The impact of thrombocytopenia on prognosis of hbv-related small hepatocellular carcinoma: A propensity score matching analysis. World J. Surg. Oncol. 2021, 19, 46. [Google Scholar] [CrossRef]
- Aryal, B.; Yamakuchi, M.; Shimizu, T.; Kadono, J.; Furoi, A.; Gejima, K.; Komokata, T.; Hashiguchi, T.; Imoto, Y. Deciphering platelet kinetics in diagnostic and prognostic evaluation of hepatocellular carcinoma. Can. J. Gastroenterol. Hepatol. 2018, 2018, 9142672. [Google Scholar] [CrossRef]
- Fattovich, G.; Stroffolini, T.; Zagni, I.; Donato, F. Hepatocellular carcinoma in cirrhosis: Incidence and risk factors. Gastroenterology 2004, 127, S35–S50. [Google Scholar] [CrossRef]
- Jung, K.S.; Kim, J.H.; Kim, S.U.; Song, K.; Kim, B.K.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Moon, D.C.; Song, I.J.; et al. Liver stiffness value-based risk estimation of late recurrence after curative resection of hepatocellular carcinoma: Development and validation of a predictive model. PLoS ONE 2014, 9, e99167. [Google Scholar] [CrossRef]
- Fields, T.D.; Philips, P.; Scoggins, C.R.; Tatum, C.; Kelly, L.; McMasters, K.M.; Martin, R.C.G. Multi-disciplinary concurrent management of recurrent hepatocellular therapy is superior to sequential therapy. World J. Surg. 2017, 41, 1331–1339. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| without Recurrence | with Recurrence | p-Value | |||
|---|---|---|---|---|---|
| n = 311 | % | n = 493 | % | ||
| Age (year) | |||||
| <65 | 165 | 20.52% | 261 | 32.46% | 0.975 |
| ≥65 | 146 | 18.16% | 232 | 28.86% | |
| Sex (n, %) | |||||
| Male | 107 | 13.31% | 160 | 19.90% | 0.591 |
| Female | 204 | 25.37% | 333 | 41.42% | |
| Alcohol (yes) | 29 | 3.61% | 74 | 9.20% | 0.023 |
| HBV (yes) | 161 | 20.02% | 215 | 26.74% | 0.025 |
| HCV (yes) | 147 | 18.28% | 284 | 35.32% | 0.005 |
| Diabetes mellitus (yes) | 81 | 10.07% | 132 | 16.42% | 0.870 |
| Hypertension (yes) | 108 | 13.43% | 182 | 22.64% | 0.547 |
| Cirrhosis (yes) | 243 | 30.22% | 407 | 50.62% | 0.141 |
| Child–Pugh | 0.070 | ||||
| A | 189 | 23.51% | 305 | 37.94% | |
| B | 25 | 3.11% | 67 | 8.33% | |
| Sugar >100 mg/dL | 71 | 8.83% | 123 | 15.30% | 0.060 |
| Albumin < 3.0 g/dl | 130 | 16.17% | 183 | 22.76% | 0.312 |
| Total bilirubin > 3.0 mg/dL | 97 | 12.06% | 123 | 15.30% | 0.150 |
| AST > 40 U/L | 108 | 13.43% | 216 | 26.87% | 0.029 |
| ALT > 40 U/L | 140 | 17.41% | 283 | 35.20% | 0.003 |
| ALP > 142 U/L | 214 | 26.62% | 305 | 37.94% | 0.099 |
| Creatinine > 2.0 mg/dL | 16 | 1.99% | 28 | 3.48% | 0.946 |
| WBC ≤4000/μL | 77 | 9.58% | 140 | 17.41% | 0.025 |
| Platelet < 14 × 104/μL | 156 | 19.40% | 314 | 39.05% | <0.001 |
| Prolonged PT 3.0–5.0 sec | 23 | 2.86% | 53 | 6.59% | 0.262 |
| NLR < 2.49 | 148 | 18.41% | 237 | 29.48% | 0.333 |
| PLR < 150 | 195 | 24.25% | 301 | 37.44% | 0.438 |
| SII > 610 × 1000/μL | 38 | 4.73% | 58 | 7.21% | 0.963 |
| AFP > 10 ng/mL | 272 | 33.83% | 430 | 53.48% | 0.612 |
| Tumor size >3 cm | 75 | 9.33% | 108 | 13.43% | 0.490 |
| Tumor number >1 | 52 | 6.47% | 103 | 12.81% | 0.168 |
| BCLC 0 | 102 | 12.68% | 137 | 17.03% | |
| A | 209 | 25.99% | 349 | 43.41% | 0.307 |
| Nucleoside analogue (yes) | 65 | 8.08% | 68 | 8.46% | 0.011 |
| Interferon (yes) | 27 | 3.36% | 33 | 4.10% | 0.335 |
| Nucleoside analogue or interferon (yes) | 90 | 11.19% | 99 | 12.31% | 0.005 |
| First treatment | |||||
| RFA | 135 | 16.79% | 225 | 27.99% | 0.561 |
| Surgery | 176 | 21.89% | 268 | 33.33% | |
| Univariate Cox Model | Multivariate Cox Model | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | HR | 95%CI | p-Value | HR | 95%CI | p-Value | |||
| Age (year) | ≤65 | 1.000 | - | - | - | ||||
| >65 | 1.048 | 0.878 | 1.251 | 0.605 | |||||
| Sex | Male | 1.000 | - | - | - | ||||
| Female | 1.050 | 0.869 | 1.268 | 0.609 | |||||
| Alcohol | No | 1.000 | - | - | - | 1.000 | - | - | - |
| Yes | 1.361 | 1.063 | 1.743 | 0.015 | 1.711 | 1.232 | 2.375 | 0.001 | |
| HBV | No | 1.000 | - | - | - | 1.000 | - | - | - |
| Yes | 0.788 | 0.658 | 0.941 | 0.009 | 1.070 | 0.718 | 1.595 | 0.739 | |
| HCV | No | 1.000 | - | - | - | 1.000 | - | - | - |
| Yes | 1.349 | 1.128 | 1.613 | 0.001 | 0.966 | 0.643 | 1.45 | 0.869 | |
| Diabetes mellitus | No | 1.000 | - | - | - | ||||
| Yes | 1.064 | 0.872 | 1.299 | 0.539 | |||||
| Hypertension | No | 1.000 | - | - | - | ||||
| Yes | 1.034 | 0.861 | 1.241 | 0.723 | |||||
| Cirrhosis | No | 1.000 | - | - | - | ||||
| Yes | 1.165 | 0.923 | 1.470 | 0.2 | |||||
| Child–Pugh score | A | 1.000 | 1.000 | ||||||
| B | 1.703 | 1.303 | 2.225 | <0.0001 | 1.450 | 0.998 | 2.109 | 0.051 | |
| Sugar | ≤100 | 1.000 | - | - | - | ||||
| (mg/dL) | >100 | 0.658 | 0.418 | 1.038 | 0.0717 | ||||
| Albumin | <3.0 | 1.000 | - | - | - | ||||
| (g/dl) | ≥3.0 | 1.147 | 0.948 | 1.387 | 0.159 | ||||
| Total bilirubin | ≤3.0 | 1.000 | - | - | - | 1.000 | - | - | - |
| (mg/dl) | >3.0 | 0.787 | 0.640 | 0.968 | 0.0234 | 0.878 | 0.664 | 1.160 | 0.358 |
| AST | ≤40 | 1.000 | - | - | - | 1.000 | - | - | - |
| (U/L) | >40 | 1.313 | 1.092 | 1.579 | 0.0038 | 1.034 | 0.782 | 1.365 | 0.817 |
| ALT | ≤40 | 1.000 | - | - | - | 1.000 | - | - | - |
| (U/L) | >40 | 1.46 | 1.21 | 1.761 | <0.0001 | 1.379 | 1.035 | 1.838 | 0.028 |
| ALP | ≤142 | 1.000 | - | - | - | 1.000 | - | - | - |
| (U/L) | >142 | 0.736 | 0.573 | 0.945 | 0.0164 | 0.895 | 0.655 | 1.223 | 0.486 |
| Creatinine | ≤2.0 | 1.000 | - | - | - | ||||
| (mg/dL) | >2.0 | 1.264 | 0.863 | 1.853 | 0.229 | ||||
| WBC | >4.0 | 1.000 | - | - | - | ||||
| (×1000/μL) | ≤4.0 | 1.185 | 0.976 | 1.439 | 0.087 | ||||
| Platelet (× 104/μL) | ≥14 | 1.000 | - | - | - | 1.000 | - | - | - |
| <14 | 1.628 | 1.352 | 1.960 | <0.0001 | 1.533 | 1.155 | 2.035 | 0.003 | |
| Prolonged PT | ≤3.0 | 1.000 | - | - | - | 1.000 | - | - | - |
| (sec) | >3.0 | 1.412 | 1.059 | 1.881 | 0.0186 | 1.171 | 0.778 | 1.763 | 0.448 |
| NLR | <2.49 | 1.000 | - | - | - | ||||
| ≥2.49 | 1.082 | 0.870 | 1.345 | 0.478 | |||||
| PLR | <150 | 1.000 | - | - | - | ||||
| ≥150 | 0.964 | 0.730 | 1.271 | 0.793 | |||||
| SII | ≤610 | 1.000 | |||||||
| >610 | 1.096 | 0.830 | 1.449 | 0.517 | |||||
| AFP | ≤10 | 1.000 | - | - | - | ||||
| (ng/mL) | >10 | 1.079 | 0.727 | 1.604 | 0.705 | ||||
| Tumor size | ≤3 | 1.000 | - | - | - | ||||
| (cm) | >3 | 0.933 | 0.754 | 1.155 | 0.526 | ||||
| Tumor number | ≤1 | 1.000 | - | - | - | 1.000 | - | - | - |
| >1 | 1.332 | 1.072 | 1.656 | 0.0097 | 1.321 | 0.988 | 1.768 | 0.060 | |
| BCLC stage | 0 | 1.000 | |||||||
| A | 1.138 | 0.934 | 1.387 | 0.199 | |||||
| Nucleoside analogue | No | 1.000 | 1.000 | ||||||
| Yes | 0.646 | 0.5 | 0.835 | 0.0008 | 1.015 | 0.552 | 1.867 | 0.961 | |
| Interferon | No | 1.000 | |||||||
| Yes | 0.785 | 0.551 | 1.117 | 0.178 | |||||
| Nucleoside analogue or interferon | No | 1.000 | - | - | - | 1.000 | - | - | - |
| Yes | 0.666 | 0.535 | 0.831 | 0.0003 | 0.593 | 0.360 | 0.977 | 0.040 | |
| Initial treatment | RFA | 1.000 | |||||||
| Surgery | 0.935 | 0.783 | 1.117 | 0.461 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, C.-H.; Shen, C.-H.; Yen, C.-L.; Yen, T.-H.; Hsieh, S.-Y. Discontinuing Hepatitis Activity Reduced Hepatocellular Carcinoma Recurrence after Primary Curative Therapy. J. Pers. Med. 2023, 13, 397. https://doi.org/10.3390/jpm13030397
Lee C-H, Shen C-H, Yen C-L, Yen T-H, Hsieh S-Y. Discontinuing Hepatitis Activity Reduced Hepatocellular Carcinoma Recurrence after Primary Curative Therapy. Journal of Personalized Medicine. 2023; 13(3):397. https://doi.org/10.3390/jpm13030397
Chicago/Turabian StyleLee, Chern-Horng, Chien-Heng Shen, Cho-Li Yen, Tzung-Hai Yen, and Sen-Yung Hsieh. 2023. "Discontinuing Hepatitis Activity Reduced Hepatocellular Carcinoma Recurrence after Primary Curative Therapy" Journal of Personalized Medicine 13, no. 3: 397. https://doi.org/10.3390/jpm13030397
APA StyleLee, C.-H., Shen, C.-H., Yen, C.-L., Yen, T.-H., & Hsieh, S.-Y. (2023). Discontinuing Hepatitis Activity Reduced Hepatocellular Carcinoma Recurrence after Primary Curative Therapy. Journal of Personalized Medicine, 13(3), 397. https://doi.org/10.3390/jpm13030397