

Emergence from General Anaesthesia: Can We Discriminate between Emergence Delirium and Postoperative Pain?

{kind=link}
Abstract
:1. Introduction
2. Evaluation Tools and Scoring Systems
3. Emergence Delirium
3.1. Common Features in Emergence Delirium
- Does the child communicate needs and wants?
- Is the child underactive—very little movement while awake?
- Does it take the child a long time to respond to interactions?
3.2. The Difficulty of Differentiating between ED and Postoperative Pain
3.3. Prevention of Unsettled Behavior after General Anaesthesia
- Happy—Calm and controlled. Compliant with induction.
- Sad—Tearful and/or withdrawn but compliant with induction.
- Mad—Loud vocal resistance (screaming or shouting) and/or physical resistance to induction requiring physical restraint by staff and/or parents.
3.4. Management of Unsettled Behavior after General Anaesthesia
4. Conclusions and Key Points
- Evaluate the presence of preoperative anxiety and unsettled behaviors during induction of anaesthesia.
- Tailor the anaesthesia plan to prevent unsettled behaviors after general anaesthesia.
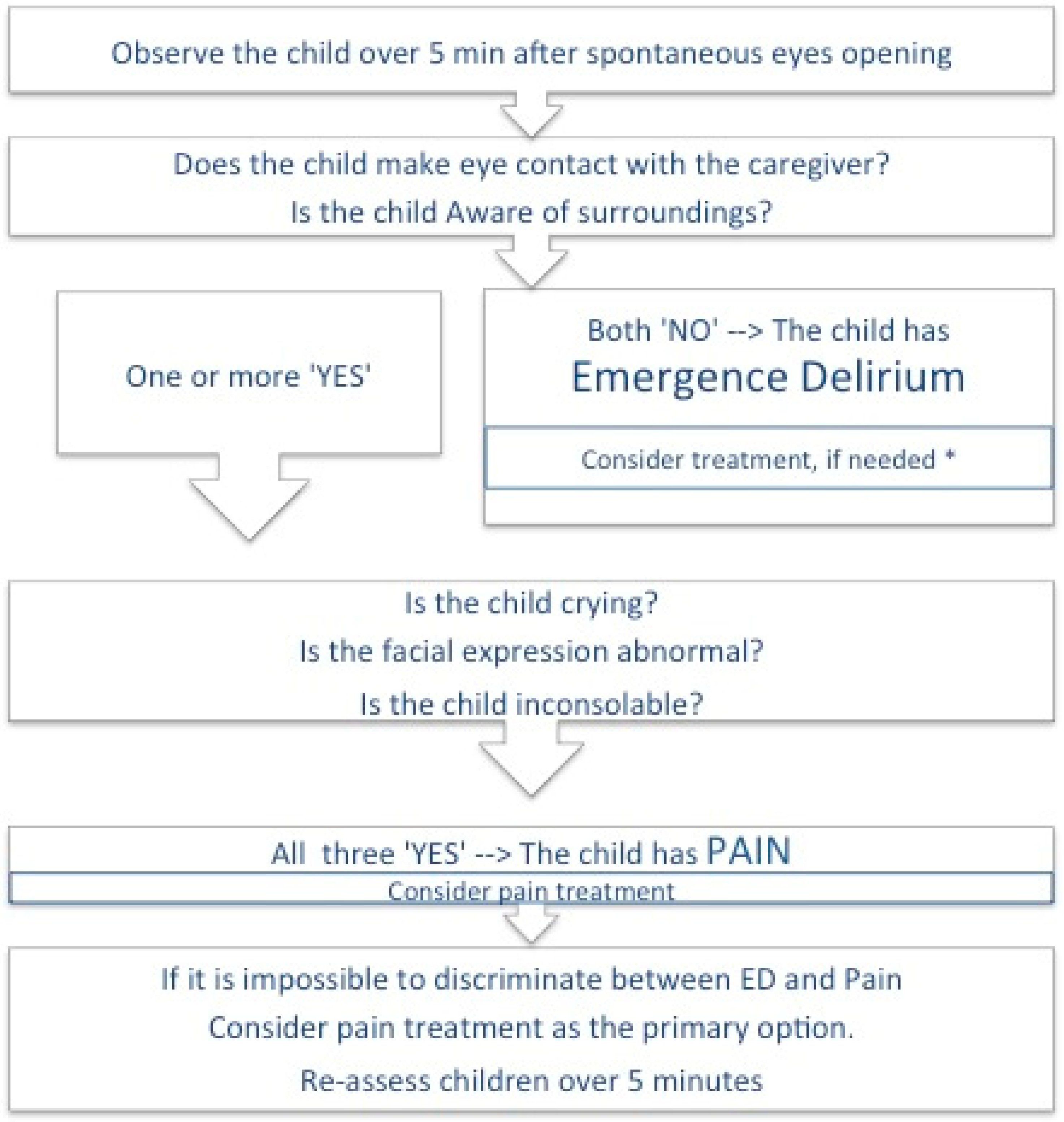
- If the child has ‘No eye contact’ and is ‘Not aware of surroundings’, we should suspect and treat ED.
- If the child has an ‘Abnormal facial expression’, is ‘Crying’ and is ‘Inconsolable’, the child is likely to be in pain.
- If the cause of the unpleasant behavior is unclear, providing general comfort, offering something to drink and reassessing the patient within 5 min is required until the underlying problem is identified.
- Support the parents of children displaying unsettled behaviors after anaesthesia. The problem may continue after discharge.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Malarbi, S.; Stargatt, R.; Howard, K.; Davidson, A. Characterizing the behavior of children emerging with delirium from general anesthesia. Paediatr. Anaesth. 2011, 21, 942–950. [Google Scholar] [CrossRef]
- Bajwa, S.A.; Costi, D.; Cyna, A.M. A comparison of emergence delirium scales following general anaesthesia in children. Paediatr. Anaesth. 2010, 20, 704–711. [Google Scholar] [CrossRef] [PubMed]
- Somaini, M.; Ingelmo, P.M. Negative Behaviour After Surgery. In Perioperative Medicine in Pediatric Anesthesia. Anesthesia, Intensive Care and Pain in Neonates and Children; Astuto, M., Ingelmo, P., Eds.; Springer: Berlin/Heidelberg, Germany, 2016. [Google Scholar]
- Lee-Archer, P.F.; von Ungern-Sternberg, B.S.; Reade, M.C.; Law, K.C.; Long, D. An observational study of hypoactive delirium in the post-anesthesia recovery unit of a pediatric hospital. Paediatr. Anaesth. 2021, 31, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Ingelmo, P.M.; Somaini, M.; Engelhardt, T. Emergence delirium may not just be a recovery room problem. Paediatr. Anaesth. 2021, 31, 1022–1024. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Byun, S.H.; Kim, J.W.; Kim, J.Y.; Choi, N.; Lee, B.S.; Yu, S.; Kim, E. Behavioral changes after hospital discharge in preschool children experiencing emergence delirium after general anesthesia: A prospective observational study. Paediatr. Anaesth. 2021, 31, 1056–1064. [Google Scholar] [CrossRef] [PubMed]
- Mason, K.B. Paediatric emergence delirium: A comprehensive review and interpretation of the literature. BJA 2017, 118, 335–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sikich, N.; Lerman, J. Development and psychometric evaluation of the pediatric anesthesia emergence delirium scale. Anesthesiology 2004, 100, 1138–1145. [Google Scholar] [CrossRef]
- Bortone, L.; Bertolizio, G.; Engelhardt, T.; Frawley, G.; Somaini, M.; Ingelmo, P.M. The effect of fentanyl and clonidine on early postoperative negative behavior in children: A double-blind placebo controlled trial. Paediatr. Anaesth. 2014, 24, 614–619. [Google Scholar] [CrossRef]
- Banchs, R.J.; Lerman, J. Preoperative anxiety management, emergence delirium, and postoperative behavior. Anesthesiol. Clin. 2014, 32, 1–23. [Google Scholar] [CrossRef]
- Doerrfuss, J.; Kramer, S.; Tafelski, S.; Spies, C.D.; Wernecke, K.-D.; Nachtigall, I. Frequency, predictive factors and therapy of Emergence Delirium: Data from a large observational clinical trial in a broad spectrum of postoperative pediatric patients. Minerva Anestesiol. 2019, 85, 617–624. [Google Scholar] [CrossRef]
- Reynolds, R.; Dennis, S.; Hasan, I.; Slewa, J.; Chen, W.; Tian, D.; Bobba, S.; Zwar, N. A systematic review of chronic disease management interventions in primary care. BMC Fam. Pract. 2018, 19, 11. [Google Scholar] [CrossRef]
- Somaini, M.; Sahillioğlu, E.; Marzorati, C.; Lovisari, F.; Engelhardt, T.; Ingelmo, P.M. Emergence delirium, pain or both? A challenge for clinicians. Paediatr. Anaesth. 2015, 25, 524–529. [Google Scholar] [CrossRef] [PubMed]
- Somaini, M.; Engelhardt, T.; Fumagalli, R.; Ingelmo, P. Emergence delirium or pain after anaesthesia--how to distinguish between the two in young children: A retrospective analysis of observational studies. BJA 2016, 116, 377–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Locatelli, B.G.; Ingelmo, P.M.; Emre, S.; Meroni, V.; Minardi, C.; Frawley, G.; Benigni, A.; Marco, S.; Spotti, A.; Busi, I.; et al. Emergence delirium in children: A comparison of sevoflurane and desflurane anesthesia using the Paediatric Anesthesia Emergence Delirium scale. Paediatr. Anaesth. 2013, 23, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Somaini, M.; Astuto, M.; Lonnqvist, P.A. Early negative behavior in the pediatric postoperative anesthesia care unit. Interference between frequently used observational tools. Int. J. Dev. Res. 2016, 6, 8473–8477. [Google Scholar]
- Merkel, S.I.; Voepel-Lewis, T.; Shayevitz, J.R.; Malviya, S. The FLACC: A behavioral scale for scoring postoperative pain in young children. Pediatr. Nurs. 1997, 23, 293–297. [Google Scholar]
- Aldecoa, C.; Bettelli, G.; Bilotta, F.; Sanders, R.; Audisio, R.; Borozdina, A.; Cherubini, A.; Jones, C.; Kehlet, H.; MacLullich, A.; et al. European Society of Anaesthesiology evidence-based and consensus-based guideline on postoperative delirium. Eur. J. Anaesthesiol. 2017, 34, 192–214. [Google Scholar] [CrossRef]
- Beringer, R.M.; Greenwood, R.; Kilpatrick, N. Development and validation of the Pediatric Anesthesia Behavior score--an objective measure of behavior during induction of anesthesia. Paediatr. Anaesth. 2014, 24, 196–200. [Google Scholar] [CrossRef]
- Eijlers, R.; Staals, L.M.; Legerstee, J.S.; Berghmans, J.M.; Strabbing, E.M.; van der Schroeff, M.P.; Wijnen, R.M.H.; Kind, L.S.; Hillegers, M.H.J.; Dierckx, B.; et al. Predicting Intense Levels of Child Anxiety During Anesthesia Induction at Hospital Arrival. J. Clin. Psychol. Med. Settings 2021, 28, 313–322. [Google Scholar] [CrossRef] [Green Version]
- Stewart, B.; Cazzell, M.A.; Pearcy, T. Single-blinded randomized controlled study on use of interactive distraction versus oral midazolam to reduce pediatric preoperative anxiety, emergence delirium, and postanesthesia length of stay. J. PeriAnesth. Nurs. 2019, 34, 567–575. [Google Scholar] [CrossRef]
- Li, L.-Q.; Wang, C.; Xu, H.-Y.; Lu, H.-L.; Zhang, H.-Z. Effects of different doses of intranasal dexmedetomidine on preoperative sedation and postoperative agitation in pediatric with total intravenous anesthesia undergoing adenoidectomy with or without tonsillectomy. Medicine 2018, 97, e12140–e12147. [Google Scholar] [CrossRef] [PubMed]
- Keles, S.; Kocaturk, O. Comparison of oral dexmedetomidine and midazolam for premedication and emergence delirium in children after dental procedures under general anesthesia: A retrospective study. DDDT 2018, 12, 647–653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chauvin, C.; Schalber-Geyer, A.S.; Lefebvre, F.; Bopp, C.; Carrenard, G.; Marcoux, L.; Mayer, J.F.; Schwaab, C.; Joshi, G.P.; Diemunsch, P. Early postoperative oral fluid intake in paediatric day case surgery influences the need for opioids and postoperative vomiting: A controlled randomized trial. BJA 2017, 118, 407–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ringblom, J.; Proczkowska, M.; Korhonen, L.; Wåhlin, I. Experiences of paediatric emergence delirium—From parents’ and a child’s perspective. Scand J. Caring Sci. 2021, 36, 1104–1112. [Google Scholar] [CrossRef]
- Smith, H.A.B.; Brink, E.; Fuchs, C.; Wesley, E.; Pandharipande, P.P. Pediatric delirium: Monitoring and management in the pediatric intensive care unit. Pediatr. Clin North Am. 2013, 60, 741–760. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Somaini, M.; Engelhardt, T.; Ingelmo, P. Emergence from General Anaesthesia: Can We Discriminate between Emergence Delirium and Postoperative Pain? J. Pers. Med. 2023, 13, 435. https://doi.org/10.3390/jpm13030435
Somaini M, Engelhardt T, Ingelmo P. Emergence from General Anaesthesia: Can We Discriminate between Emergence Delirium and Postoperative Pain? Journal of Personalized Medicine. 2023; 13(3):435. https://doi.org/10.3390/jpm13030435
Chicago/Turabian StyleSomaini, Marta, Thomas Engelhardt, and Pablo Ingelmo. 2023. "Emergence from General Anaesthesia: Can We Discriminate between Emergence Delirium and Postoperative Pain?" Journal of Personalized Medicine 13, no. 3: 435. https://doi.org/10.3390/jpm13030435
APA StyleSomaini, M., Engelhardt, T., & Ingelmo, P. (2023). Emergence from General Anaesthesia: Can We Discriminate between Emergence Delirium and Postoperative Pain? Journal of Personalized Medicine, 13(3), 435. https://doi.org/10.3390/jpm13030435