
Pooled Analysis of Mesenchymal Stromal Cell-Derived Extracellular Vesicle Therapy for Liver Disease in Preclinical Models
 and
and
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy and Study Selection
2.2. Selection Criteria
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Study Selection
3.2. Characteristics of the Eligible Studies
3.3. Meta-Analyses of MSC-EV vs. Placebo Control
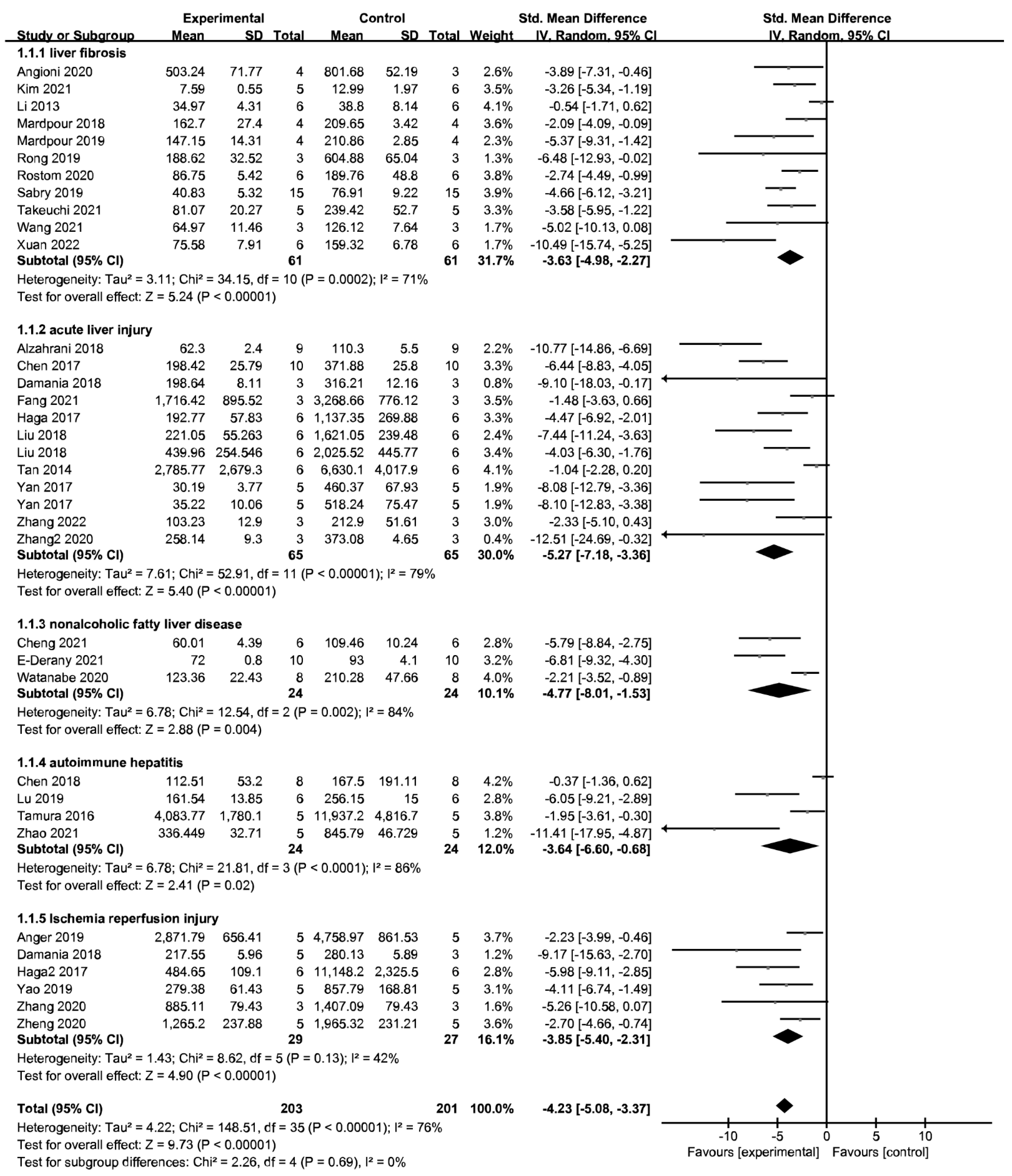
3.3.1. MSC-EV Therapy Improves Liver Function
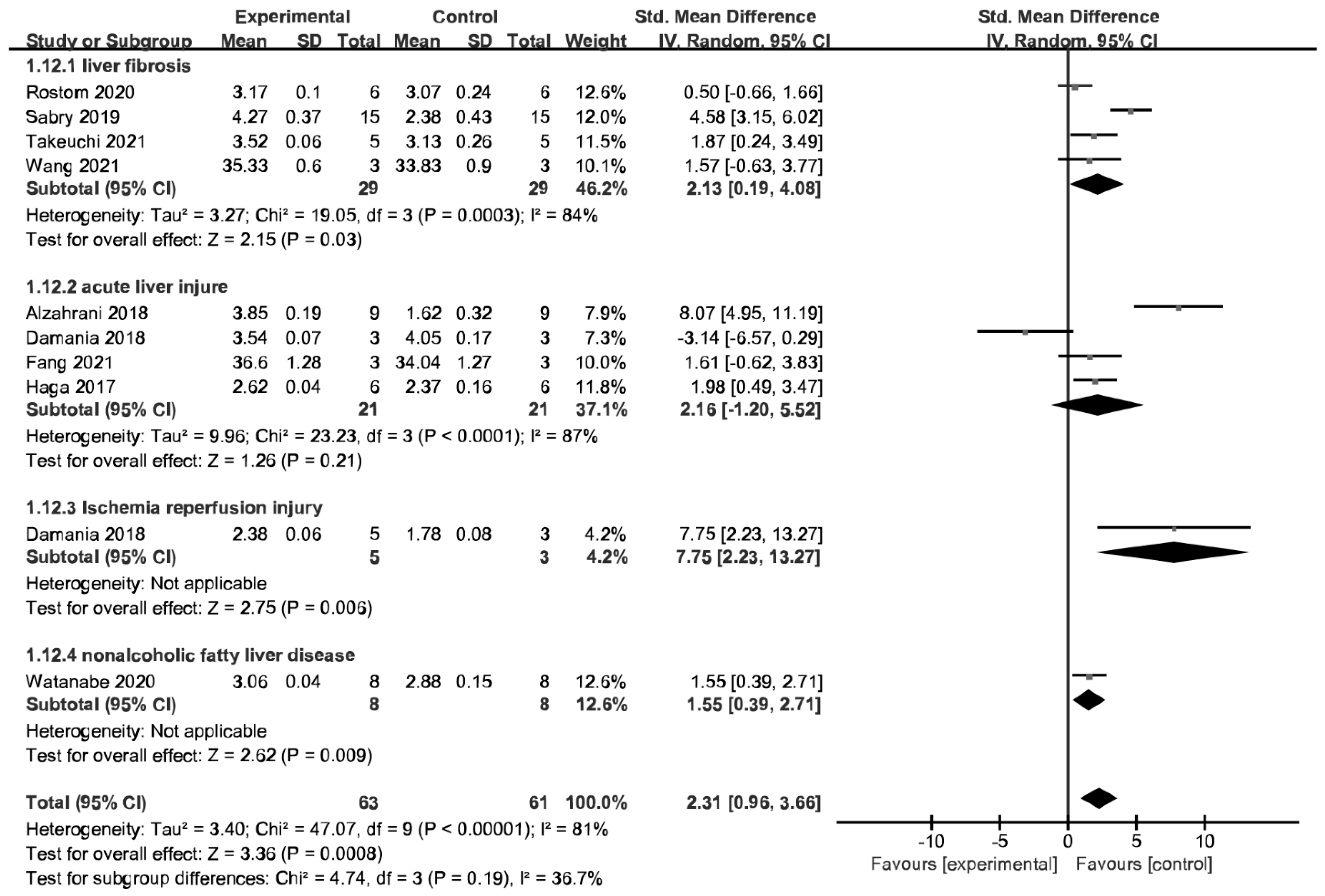
3.3.2. MSC-EV Therapy Achieve Histological Improvement
3.3.3. MSC-EV Therapy Mitigates Excessive Inflammatory Response
3.3.4. Further Subgroup Analyses
3.4. MSC-EV Therapy Displays No Inferior Performance to MSC
3.5. Sensitivity Analysis and Quality Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Byass, P. The global burden of liver disease: A challenge for methods and for public health. BMC Med. 2014, 12, 159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mokdad, A.A.; Lopez, A.D.; Shahraz, S.; Lozano, R.; Stanaway, J.; Murray, C.J.; Naghavi, M. Liver cirrhosis mortality in 187 countries between 1980 and 2010: A systematic analysis. BMC Med. 2014, 12, 145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, J.; Wang, F.; Wong, N.-K.; He, J.; Zhang, R.; Sun, R.; Xu, Y.; Liu, Y.; Li, W.; Koike, K.; et al. Global liver disease burdens and research trends: Analysis from a Chinese perspective. J. Hepatol. 2019, 71, 212–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Udompap, P.; Kim, D.; Kim, W.R. Current and Future Burden of Chronic Nonmalignant Liver Disease. Clin. Gastroenterol. Hepatol. 2015, 13, 2031–2041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asrani, S.K.; Devarbhavi, H.; Eaton, J.; Kamath, P.S. Burden of liver diseases in the world. J. Hepatol. 2019, 70, 151–171. [Google Scholar] [CrossRef]
- Naji, A.; Eitoku, M.; Favier, B.; Deschaseaux, F.; Rouas-Freiss, N.; Suganuma, N. Biological functions of mesenchymal stem cells and clinical implications. Cell. Mol. Life Sci. 2019, 76, 3323–3348. [Google Scholar] [CrossRef]
- Zhao, L.; Chen, S.; Shi, X.; Cao, H.; Li, L. A pooled analysis of mesenchymal stem cell-based therapy for liver disease. Stem Cell Res. Ther. 2018, 9, 72. [Google Scholar] [CrossRef]
- Varderidou-Minasian, S.; Lorenowicz, M.J. Mesenchymal stromal/stem cell-derived extracellular vesicles in tissue repair: Challenges and opportunities. Theranostics 2020, 10, 5979–5997. [Google Scholar] [CrossRef]
- Lin, F.; Chen, W.; Zhou, J.; Zhu, J.; Yao, Q.; Feng, B.; Feng, X.; Shi, X.; Pan, Q.; Yu, J.; et al. Mesenchymal stem cells protect against ferroptosis via exosome-mediated stabilization of SLC7A11 in acute liver injury. Cell Death Dis. 2022, 13, 271. [Google Scholar] [CrossRef]
- Yang, L.; Zhu, J.; Zhang, C.; Wang, J.; Yue, F.; Jia, X.; Liu, H. Stem cell-derived extracellular vesicles for myocardial infarction: A meta-analysis of controlled animal studies. Aging 2019, 11, 1129–1150. [Google Scholar] [CrossRef]
- Tieu, A.; Hu, K.; Gnyra, C.; Montroy, J.; Fergusson, D.A.; Allan, D.S.; Stewart, D.J.; Thébaud, B.; Lalu, M.M. Mesenchymal stromal cell extracellular vesicles as therapy for acute and chronic respiratory diseases: A meta-analysis. J. Extracell. Vesicles 2021, 10, e12141. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Wang, J.; Hu, J.; Fu, B.; Mao, Z.; Zhang, H.; Cai, G.; Chen, X.; Sun, X. Extracellular vesicles for acute kidney injury in preclinical rodent models: A meta-analysis. Stem Cell Res. Ther. 2020, 11, 11. [Google Scholar] [CrossRef] [Green Version]
- Zhang, B.; Tian, X.; Qu, Z.; Liu, J.; Yang, L.; Zhang, W. Efficacy of extracellular vesicles from mesenchymal stem cells on osteoarthritis in animal models: A systematic review and meta-analysis. Nanomedicine 2021, 16, 1297–1310. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Yan, Y.; Wang, B.; Qian, H.; Zhang, X.; Shen, L.; Wang, M.; Zhou, Y.; Zhu, W.; Li, W.; et al. Exosomes Derived from Human Umbilical Cord Mesenchymal Stem Cells Alleviate Liver Fibrosis. Stem Cells Dev. 2013, 22, 845–854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamura, R.; Uemoto, S.; Tabata, Y. Immunosuppressive effect of mesenchymal stem cell-derived exosomes on a concanavalin A-induced liver injury model. Inflamm. Regen. 2016, 36, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiabotto, G.; Pasquino, C.; Camussi, G.; Bruno, S. Molecular Pathways Modulated by Mesenchymal Stromal Cells and Their Extracellular Vesicles in Experimental Models of Liver Fibrosis. Front. Cell Dev. Biol. 2020, 8, 594794. [Google Scholar] [CrossRef] [PubMed]
- MacLeod, M.R.; O’Collins, T.; Howells, D.; Donnan, G. Pooling of Animal Experimental Data Reveals Influence of Study Design and Publication Bias. Stroke 2004, 35, 1203–1208. [Google Scholar] [CrossRef]
- Alhomrani, M.; Correia, J.; Zavou, M.; Leaw, B.; Kuk, N.; Xu, R.; Saad, M.I.; Hodge, A.; Greening, D.W.; Lim, R.; et al. The Human Amnion Epithelial Cell Secretome Decreases Hepatic Fibrosis in Mice with Chronic Liver Fibrosis. Front. Pharmacol. 2017, 8, 748. [Google Scholar] [CrossRef]
- Angioni, R.; Calì, B.; Vigneswara, V.; Crescenzi, M.; Merino, A.; Sánchez-Rodríguez, R.; Liboni, C.; Hoogduijn, M.J.; Newsome, P.N.; Muraca, M.; et al. Administration of Human MSC-Derived Extracellular Vesicles for the Treatment of Primary Sclerosing Cholangitis: Preclinical Data in MDR2 Knockout Mice. Int. J. Mol. Sci. 2020, 21, 8874. [Google Scholar] [CrossRef]
- Gupta, S.; Pinky; Vishal; Sharma, H.; Soni, N.; Rao, E.P.; Dalela, M.; Yadav, A.; Nautiyal, N.; Kumar, A.; et al. Comparative Evaluation of Anti-Fibrotic Effect of Tissue Specific Mesenchymal Stem Cells Derived Extracellular Vesicles for the Amelioration of CCl4 Induced Chronic Liver Injury. Stem Cell Rev. Rep. 2021, 18, 1097–1112. [Google Scholar] [CrossRef]
- Han, H.S.; Lee, H.; You, D.; Nguyen, V.Q.; Song, D.-G.; Oh, B.H.; Shin, S.; Choi, J.S.; Kim, J.D.; Pan, C.-H.; et al. Human adipose stem cell-derived extracellular nanovesicles for treatment of chronic liver fibrosis. J. Control. Release 2020, 320, 328–336. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Lee, C.; Shin, Y.; Wang, S.; Han, J.; Kim, M.; Kim, J.M.; Shin, S.-C.; Lee, B.-J.; Kim, T.-J.; et al. sEVs from tonsil-derived mesenchymal stromal cells alleviate activation of hepatic stellate cells and liver fibrosis through miR-486-5p. Mol. Ther. 2020, 29, 1471–1486. [Google Scholar] [CrossRef] [PubMed]
- Mardpour, S.; Hassani, S.; Mardpour, S.; Sayahpour, F.; Vosough, M.; Ai, J.; Aghdami, N.; Hamidieh, A.A.; Baharvand, H. Extracellular vesicles derived from human embryonic stem cell-MSCs ameliorate cirrhosis in thioacetamide-induced chronic liver injury. J. Cell. Physiol. 2017, 233, 9330–9344. [Google Scholar] [CrossRef] [PubMed]
- Mardpour, S.; Ghanian, M.H.; Sadeghi-Abandansari, H.; Mardpour, S.; Nazari, A.; Shekari, F.; Baharvand, H. Hydrogel-Mediated Sustained Systemic Delivery of Mesenchymal Stem Cell-Derived Extracellular Vesicles Improves Hepatic Regeneration in Chronic Liver Failure. ACS Appl. Mater. Interfaces 2019, 11, 37421–37433. [Google Scholar] [CrossRef] [PubMed]
- Ohara, M.; Ohnishi, S.; Hosono, H.; Yamamoto, K.; Yuyama, K.; Nakamura, H.; Fu, Q.; Maehara, O.; Suda, G.; Sakamoto, N. Extracellular Vesicles from Amnion-Derived Mesenchymal Stem Cells Ameliorate Hepatic Inflammation and Fibrosis in Rats. Stem Cells Int. 2018, 2018, 3212643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rong, X.; Liu, J.; Yao, X.; Jiang, T.; Wang, Y.; Xie, F. Human bone marrow mesenchymal stem cells-derived exosomes alleviate liver fibrosis through the Wnt/β-catenin pathway. Stem Cell Res. Ther. 2019, 10, 98. [Google Scholar] [CrossRef] [Green Version]
- Rostom, D.M.; Attia, N.; Khalifa, H.M.; Nazel, M.W.A.; El Sabaawy, E.A. The Therapeutic Potential of Extracellular Vesicles Versus Mesenchymal Stem Cells in Liver Damage. Tissue Eng. Regen. Med. 2020, 17, 537–552. [Google Scholar] [CrossRef]
- Sabry, D.; Mohamed, A.; Monir, M.; Ibrahim, H.A. The Effect of Mesenchymal Stem Cells Derived Microvesicles on the Treatment of Experimental CCL4 Induced Liver Fibrosis in Rats. Int. J. Stem Cells 2019, 12, 400–409. [Google Scholar] [CrossRef] [Green Version]
- Takeuchi, S.; Tsuchiya, A.; Iwasawa, T.; Nojiri, S.; Watanabe, T.; Ogawa, M.; Yoshida, T.; Fujiki, K.; Koui, Y.; Kido, T.; et al. Small extracellular vesicles derived from interferon-γ pre-conditioned mesenchymal stromal cells effectively treat liver fibrosis. npj Regen. Med. 2021, 6, 19. [Google Scholar] [CrossRef]
- Wang, N.; Li, X.; Zhong, Z.; Qiu, Y.; Liu, S.; Wu, H.; Tang, X.; Chen, C.; Fu, Y.; Chen, Q.; et al. 3D hESC exosomes enriched with miR-6766-3p ameliorates liver fibrosis by attenuating activated stellate cells through targeting the TGFβRII-SMADS pathway. J. Nanobiotechnol. 2021, 19, 437. [Google Scholar] [CrossRef]
- Xuan, J.; Xu, H.; Li, H.; Chen, D.; Qiu, Y.; Chen, X.; Shao, M.; Xia, X. Extracellular Vesicles from miR-148a-5p-Enriched Bone Marrow Mesenchymal Stem Cells Relieve Hepatic Fibrosis by Targeting Smad4. Mol. Biotechnol. 2022, 64, 535–545. [Google Scholar] [CrossRef]
- You, D.G.; Oh, B.H.; Nguyen, V.Q.; Lim, G.T.; Um, W.; Jung, J.M.; Jeon, J.; Choi, J.S.; Choi, Y.C.; Jung, Y.J.; et al. Vitamin A-coupled stem cell-derived extracellular vesicles regulate the fibrotic cascade by targeting activated hepatic stellate cells in vivo. J. Control. Release 2021, 336, 285–295. [Google Scholar] [CrossRef]
- Abdelrahma, F.; Alkarim, S.; Sa, I.M. Ameliorative Effect of Mesenchymal Stem Cells-derived Exosomes on Diethylnitrosamine-induced Liver Injury in Albino Rats. Int. J. Pharmacol. 2018, 14, 1128–1135. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Xiang, B.; Wang, X.; Xiang, C. Exosomes derived from human menstrual blood-derived stem cells alleviate fulminant hepatic failure. Stem Cell Res. Ther. 2017, 8, 9. [Google Scholar] [CrossRef] [Green Version]
- Damania, A.; Jaiman, D.; Teotia, A.K.; Kumar, A. Mesenchymal stromal cell-derived exosome-rich fractionated secretome confers a hepatoprotective effect in liver injury. Stem Cell Res. Ther. 2018, 9, 31. [Google Scholar] [CrossRef] [Green Version]
- Fang, J.; Liang, W. ASCs -derived exosomes loaded with vitamin A and quercetin inhibit rapid senescence-like response after acute liver injury. Biochem. Biophys. Res. Commun. 2021, 572, 125–130. [Google Scholar] [CrossRef]
- Haga, H.; Yan, I.K.; Takahashi, K.; Matsuda, A.; Patel, T. Extracellular Vesicles from Bone Marrow-Derived Mesenchymal Stem Cells Improve Survival from Lethal Hepatic Failure in Mice. Stem Cells Transl. Med. 2017, 6, 1262–1272. [Google Scholar] [CrossRef]
- Jiang, L.; Zhang, S.; Hu, H.; Yang, J.; Wang, X.; Ma, Y.; Jiang, J.; Wang, J.; Zhong, L.; Chen, M.; et al. Exosomes derived from human umbilical cord mesenchymal stem cells alleviate acute liver failure by reducing the activity of the NLRP3 inflammasome in macrophages. Biochem. Biophys. Res. Commun. 2018, 508, 735–741. [Google Scholar] [CrossRef]
- Liu, Y.; Lou, G.; Li, A.; Zhang, T.; Qi, J.; Ye, D.; Zheng, M.; Chen, Z. AMSC-derived exosomes alleviate lipopolysaccharide/d-galactosamine-induced acute liver failure by miR-17-mediated reduction of TXNIP/NLRP3 inflammasome activation in macrophages. Ebiomedicine 2018, 36, 140–150. [Google Scholar] [CrossRef] [Green Version]
- Tan, C.Y.; Lai, R.C.; Wong, W.; Dan, Y.Y.; Lim, S.-K.; Ho, H.K. Mesenchymal stem cell-derived exosomes promote hepatic regeneration in drug-induced liver injury models. Stem Cell Res. Ther. 2014, 5, 76. [Google Scholar] [CrossRef] [Green Version]
- Yan, Y.; Jiang, W.; Tan, Y.; Zou, S.; Zhang, H.; Mao, F.; Gong, A.; Qian, H.; Xu, W. hucMSC Exosome-Derived GPX1 Is Required for the Recovery of Hepatic Oxidant Injury. Mol. Ther. 2016, 25, 465–479. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Zhang, X.; Zhang, H.; Song, P.; Pan, W.; Xu, P.; Wang, G.; Hu, P.; Wang, Z.; Huang, K.; et al. Mesenchymal Stem Cells Derived Extracellular Vesicles Alleviate Traumatic Hemorrhagic Shock Induced Hepatic Injury via IL-10/PTPN22-Mediated M2 Kupffer Cell Polarization. Front. Immunol. 2022, 12, 31. [Google Scholar] [CrossRef]
- Zhang, S.; Jiang, L.; Hu, H.; Wang, H.; Wang, X.; Jiang, J.; Ma, Y.; Yang, J.; Hou, Y.; Xie, D.; et al. Pretreatment of exosomes derived from hUCMSCs with TNF-α ameliorates acute liver failure by inhibiting the activation of NLRP3 in macrophage. Life Sci. 2020, 246, 117401. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; Yu, P.; Li, F.; Jiang, X.; Jiao, X.; Shen, Y.; Lai, X. Human umbilical cord-derived mesenchymal stem cell-exosomal miR-627-5p ameliorates non-alcoholic fatty liver disease by repressing FTO expression. Hum. Cell 2021, 34, 1697–1708. [Google Scholar] [CrossRef] [PubMed]
- El-Derany, M.O.; AbdelHamid, S.G. Upregulation of miR-96-5p by bone marrow mesenchymal stem cells and their exosomes alleviate non-alcoholic steatohepatitis: Emphasis on caspase-2 signaling inhibition. Biochem. Pharmacol. 2021, 190, 114624. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Tsuchiya, A.; Takeuchi, S.; Nojiri, S.; Yoshida, T.; Ogawa, M.; Itoh, M.; Takamura, M.; Suganami, T.; Ogawa, Y.; et al. Development of a non-alcoholic steatohepatitis model with rapid accumulation of fibrosis, and its treatment using mesenchymal stem cells and their small extracellular vesicles. Regen. Ther. 2020, 14, 252–261. [Google Scholar] [CrossRef]
- Chen, L.; Lu, F.-B.; Chen, D.-Z.; Wu, J.-L.; Hu, E.-D.; Xu, L.-M.; Zheng, M.-H.; Li, H.; Huang, Y.; Jin, X.-Y.; et al. BMSCs-derived miR-223-containing exosomes contribute to liver protection in experimental autoimmune hepatitis. Mol. Immunol. 2018, 93, 38–46. [Google Scholar] [CrossRef]
- Lu, F.-B.; Chen, D.-Z.; Chen, L.; Hu, E.-D.; Wu, J.-L.; Li, H.; Gong, Y.-W.; Lin, Z.; Wang, X.-D.; Li, J.; et al. Attenuation of Experimental Autoimmune Hepatitis in Mice with Bone Mesenchymal Stem Cell-Derived Exosomes Carrying MicroRNA-223-3p. Mol. Cells 2019, 42, 906–918. [Google Scholar] [CrossRef]
- Zhao, J.; Li, Y.; Jia, R.; Wang, J.; Shi, M.; Wang, Y. Mesenchymal Stem Cells-Derived Exosomes as Dexamethasone Delivery Vehicles for Autoimmune Hepatitis Therapy. Front. Bioeng. Biotechnol. 2021, 9, 650376. [Google Scholar] [CrossRef]
- Anger, F.; Camara, M.; Ellinger, E.; Germer, C.-T.; Schlegel, N.; Otto, C.; Klein, I. Human Mesenchymal Stromal Cell-Derived Extracellular Vesicles Improve Liver Regeneration After Ischemia Reperfusion Injury in Mice. Stem Cells Dev. 2019, 28, 1451–1462. [Google Scholar] [CrossRef]
- Haga, H.; Yan, I.K.; Borrelli, D.A.; Matsuda, A.; Parasramka, M.; Shukla, N.; Lee, D.D.; Patel, T. Extracellular vesicles from bone marrow–derived mesenchymal stem cells protect against murine hepatic ischemia/reperfusion injury. Liver Transplant. 2017, 23, 791–803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, J.; Zheng, J.; Cai, J.; Zeng, K.; Zhou, C.; Zhang, J.; Li, S.; Li, H.; Chen, L.; He, L.; et al. Extracellular vesicles derived from human umbilical cord mesenchymal stem cells alleviate rat hepatic ischemia-reperfusion injury by suppressing oxidative stress and neutrophil inflammatory response. FASEB J. 2018, 33, 1695–1710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Song, Y.; Chen, L.; Li, D.; Feng, H.; Lu, Z.; Fan, T.; Chen, Z.; Livingston, M.J.; Geng, Q. MiR-20a-containing exosomes from umbilical cord mesenchymal stem cells alleviates liver ischemia/reperfusion injury. J. Cell. Physiol. 2019, 235, 3698–3710. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Lu, T.; Zhou, C.; Cai, J.; Zhang, X.; Liang, J.; Sui, X.; Chen, X.; Chen, L.; Sun, Y.; et al. Extracellular Vesicles Derived from Human Umbilical Cord Mesenchymal Stem Cells Protect Liver Ischemia/Reperfusion Injury by Reducing CD154 Expression on CD4+ T Cells via CCT2. Adv. Sci. 2020, 7, 1903746. [Google Scholar] [CrossRef]
- Woreta, T.A.; Alqahtani, S. Evaluation of Abnormal Liver Tests. Med. Clin. N. Am. 2014, 98, 1–16. [Google Scholar] [CrossRef]
- Kwo, P.Y.; Cohen, S.M.; Lim, J.K. ACG Clinical Guideline: Evaluation of Abnormal Liver Chemistries. Am. J. Gastroenterol. 2017, 112, 18–35. [Google Scholar] [CrossRef]
- Iluz-Freundlich, D.; Zhang, M.; Uhanova, J.; Minuk, G.Y. The relative expression of hepatocellular and cholestatic liver enzymes in adult patients with liver disease. Ann. Hepatol. 2020, 19, 204–208. [Google Scholar] [CrossRef]
- Chowdhury, A.B.; Mehta, K.J. Liver biopsy for assessment of chronic liver diseases: A synopsis. Clin. Exp. Med. 2022. [Google Scholar] [CrossRef]
- Mohamadnejad, M.; Tavangar, S.M.; Sotoudeh, M.; Kosari, F.; Khosravi, M.; Geramizadeh, B.; Montazeri, G.; Estakhri, A.; Mirnasseri, M.M.; Fazlollahi, A.; et al. Histopathological Study of Chronic Hepatitis B: A Comparative Study of Ishak and METAVIR Scoring Systems. Int. J. Organ Transplant. Med. 2010, 1, 171–176. [Google Scholar] [CrossRef]
- Rozario, R.; Ramakrishna, B. Histopathological study of chronic hepatitis B and C: A comparison of two scoring systems. J. Hepatol. 2003, 38, 223–229. [Google Scholar] [CrossRef]
- Kiecolt-Glaser, J.K.; Gouin, J.-P.; Hantsoo, L. Close relationships, inflammation, and health. Neurosci. Biobehav. Rev. 2010, 35, 33–38. [Google Scholar] [CrossRef] [Green Version]
- Triantafyllou, E.; Woollard, K.J.; McPhail, M.J.W.; Antoniades, C.G.; Possamai, L.A. The Role of Monocytes and Macrophages in Acute and Acute-on-Chronic Liver Failure. Front. Immunol. 2018, 9, 2948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laleman, W.; Claria, J.; Van der Merwe, S.; Moreau, R.; Trebicka, J. Systemic Inflammation and Acute-on-Chronic Liver Failure: Too Much, Not Enough. Can. J. Gastroenterol. Hepatol. 2018, 2018, 1027152. [Google Scholar] [CrossRef] [PubMed]
- Casulleras, M.; Zhang, I.W.; López-Vicario, C.; Clària, J. Leukocytes, Systemic Inflammation and Immunopathology in Acute-on-Chronic Liver Failure. Cells 2020, 9, 2632. [Google Scholar] [CrossRef] [PubMed]
- Zekri, A.-R.N.; Salama, H.; Medhat, E.; Musa, S.; Abdel-Haleem, H.; Ahmed, O.S.; Khedr, H.A.H.; Lotfy, M.M.; Zachariah, K.S.; Bahnassy, A.A. The impact of repeated autologous infusion of haematopoietic stem cells in patients with liver insufficiency. Stem Cell Res. Ther. 2015, 6, 118. [Google Scholar] [CrossRef] [Green Version]
- King, A.; Barton, D.; Beard, H.A.; Than, N.; Moore, J.; Corbett, C.; Thomas, J.; Guo, K.; Guha, I.N.; Hollyman, D.; et al. REpeated AutoLogous Infusions of STem cells In Cirrhosis (REALISTIC): A multicentre, phase II, open-label, randomised controlled trial of repeated autologous infusions of granulocyte colony-stimulating factor (GCSF) mobilised CD133+ bone marrow stem cells in patients with cirrhosis. A study protocol for a randomised controlled trial. BMJ Open 2015, 5, e007700. [Google Scholar] [CrossRef]
- Shi, M.; Li, Y.-Y.; Xu, R.-N.; Meng, F.-P.; Yu, S.-J.; Fu, J.-L.; Hu, J.-H.; Li, J.-X.; Wang, L.-F.; Jin, L.; et al. Mesenchymal stem cell therapy in decompensated liver cirrhosis: A long-term follow-up analysis of the randomized controlled clinical trial. Hepatol. Int. 2021, 15, 1431–1441. [Google Scholar] [CrossRef]
- Liu, Y.; Dong, Y.; Wu, X.; Xu, X.; Niu, J. The assessment of mesenchymal stem cells therapy in acute on chronic liver failure and chronic liver disease: A systematic review and meta-analysis of randomized controlled clinical trials. Stem Cell Res. Ther. 2022, 13, 204. [Google Scholar] [CrossRef]
- Madrigal, M.; Rao, K.S.; Riordan, N.H. A review of therapeutic effects of mesenchymal stem cell secretions and induction of secretory modification by different culture methods. J. Transl. Med. 2014, 12, 260. [Google Scholar] [CrossRef] [Green Version]
- Chen, W.; Zhu, J.; Lin, F.; Xu, Y.; Feng, B.; Feng, X.; Sheng, X.; Shi, X.; Pan, Q.; Yang, J.; et al. Human placenta mesenchymal stem cell-derived exosomes delay H2O2-induced aging in mouse cholangioids. Stem Cell Res. Ther. 2021, 12, 201. [Google Scholar] [CrossRef]
- Cao, H.; Yang, J.; Yu, J.; Pan, Q.; Li, J.; Zhou, P.; Li, Y.; Pan, X.; Li, J.; Wang, Y.; et al. Therapeutic potential of transplanted placental mesenchymal stem cells in treating Chinese miniature pigs with acute liver failure. BMC Med. 2012, 10, 56. [Google Scholar] [CrossRef] [Green Version]
- Alfaifi, M.; Eom, Y.W.; Newsome, P.N.; Baik, S.K. Mesenchymal stromal cell therapy for liver diseases. J. Hepatol. 2018, 68, 1272–1285. [Google Scholar] [CrossRef] [Green Version]
- Kang, S.H.; Kim, M.Y.; Eom, Y.W.; Baik, S.K. Mesenchymal Stem Cells for the Treatment of Liver Disease: Present and Perspectives. Gut Liver 2020, 14, 306. [Google Scholar] [CrossRef] [PubMed]
- Brennan, M.; Layrolle, P.; Mooney, D.J. Biomaterials Functionalized with MSC Secreted Extracellular Vesicles and Soluble Factors for Tissue Regeneration. Adv. Funct. Mater. 2020, 30, 1909125. [Google Scholar] [CrossRef]
- Yang, X.-X.; Sun, C.; Wang, L.; Guo, X.-L. New insight into isolation, identification techniques and medical applications of exosomes. J. Control. Release 2019, 308, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.; Tan, W.-F.; Yang, M.-Q.; Li, J.-Y.; Geller, D.A. The therapeutic potential of exosomes derived from different cell sources in liver diseases. Am. J. Physiol. Liver Physiol. 2022, 322, G397–G404. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Year) Country | Species Sex | Injure Model | Cell Source of EV | Isolation Technique | Diameter (nm) | EV Treatment Group (Method/Dose) | Number | Therapy Time | Measurement Time | Available Outcomes |
|---|---|---|---|---|---|---|---|---|---|---|
| Alhomrani (2017) Australia [18] | C57BL/6 mice male | CCL4 induce liver fibrosis | hAMSC | ultracentrifugation | 40–100 | i.v./1 µg (~24 × 106 particles, 350 µL) | C:6 T:6 | three doses weekly for 4 weeks after injure | 12 weeks after treatment | fibrosis area% (sirius red staining) |
| Alzahrani (2018) China [33] | albino rats male | Diethylnitrosamine induce ALI | Rat-BMSC | ultracentrifugation | 30–100 | i.v./250 µg | C:9 T:9 | single after injure | 4 weeks after therapy | serum ALT, AST, ALB, ALP |
| Anger (2019) Germany [50] | C57BL/6 mice female | I/RI | hBMSC | ultracentrifugation | 160 ± 57 | inferior cava/1 × 109 particles | C:5 T:5 | single before injure | 24 h/48 h/72 h after reperfusion | serum ALT, AST; necrosis area% (hematoxylin and eosin staining).H&E |
| Angioni (2020) Italy [19] | FVB.129P2-Abcb4tm1Bor mice male | PSC | hBMSC | Ultrafiltration | 45–372 | intraperitoneal/9.1 × 109 particles/mL (100 µL) | C:3 T:4 | once a week for 3 weeks after injure | 3 weeks after treatment | Serum of ALT, ALP |
| Chen (2017) China [34] | C57BL/6 mice male | D-GalN/LPS induce FHF | MenSC | commercial kits | 30–100 | tail vein/1 μg/μL | C:10 T:10 | single before injure | after therapy | serum ALT, AST; serum IL-6, IL-1β, TNF-α |
| Chen (2018) China [47] | C57BL/6 mice male | AIH | mouse-BMSC | ultracentrifugation | 30–100 | intraperitoneal/20 μg/mL | C:8 T:8 | day 21/28/35 after injure | 21 days after therapy | serum levels of ALT, AST; serum TNF-α, IL-17, IL-1β |
| Cheng (2021) China [44] | Sprague-Dawley rats male | NAFLD | hUCMSC | commercial kits | 96 | caudal vein/100 μg (500 μL) | C:6 T:6 | once a week for 2 months | 8 weeks after model | serum ALT, AST; liver index |
| Damania (2018) India [35] | Wistar rats male | IRI and CCL4 induce acute liver injury | rat-BMSC | differential centrifugation | 165 ± 3 | hepatic portal vein/50 μg | C:3 T:5 C:3 T:3 | single after injure | 24 h/48 h/72 h after therapy | serum ALT, AST, ALB, TBIL |
| E-Derany (2021) Egypt [45] | Sprague-Dawley rats NA | NAFLD | rat-BMSC | differential centrifugation | NA | tail vein/(15 µg/kg), (30 µg/kg) or (120 µg/kg) | C:10 T:10 | twice weekly for 6 weeks after injure | 12 weeks after model | serum AST, ALT |
| Fang (2021) China [36] | Mice male | CCL4 induce ALI | mouse-ADSC | commercial kits | NA | tail vein/200 mL | C:3 T:3 | single 10 h after CCl4 | 3 day after treatment | LW/BW; serum AST, ALT, ALB, γ-GT; The histopathological score(HE staining ) |
| Gupta (2021) India [20] | Swiss albino mice female | CCL4 induce liver fibrosis | hADSC/WJMSC | commercial kits | 40–120 | tail vein/250 μg | C:5 T:5 | single after injure | day7 after treatment | liver index; Histopathological analysis of Masson’s Trichrome staining and Sirius Red Staining Red area |
| Haga (2017) USA [37] | C57Bl/6 mice male | TNF-α/D-GalN induce ALF | hBMSC/mouse-BMSC | ultracentrifugation | 116 ± 46 | intraperitoneal/2 × 1010 particles/body | C:6 T:6 | single after injure | 6 h after therapy | Serum ALT, AST, ALP |
| Haga2 (2017) USA [51] | C57BL/6 mice male | I/RI | mouse-BMSC | ultracentrifugation | 115 ± 48 | tail vein/2 × 1010 particles | C:6 T:6 | single before injure | 6 h after reperfusion | serum ALT, AST, ALP, TBIL; necrosis area% (H&E) staining |
| Han (2020) Korea [21] | C57BL/6 mice male | TAA induce liver fibrosis | hADSC | tangential flow filtration(TFF) | 94.2 ± 4.7 | tail vein/200 μL (1 × 107; 1 × 108) | C:5 T:5 | single after injure | 24 h after treatment | LW/BW; collagen areas (Masson’s trichrome); Hyp level in tissue |
| Jiang (2019) China [38] | C57BL/6 mice male | LPS/D-GalN-induce ALF | hUCMSC | centrifugation | 100 | tail vein/100 μg (250 μL) | C:6 T:6 | single 1 h after injure | 12 h after therapy | ALT, AST; serum levels of IL-6, IL-1β |
| Kim (2021) Korea [22] | C57BL/6 mice Male | CCL4 induce liver fibrosis | hTMSC | differential centrifugation | 50–290 | i.v./150 mg (100 μg/mL) | C:5 T:6 | once a week for 3 weeks after injure | 48 h after last treatment | LW/BW; serum ALT, AST |
| Li (2013) China [14] | mice | CCL4 induce liver fibrosis | hUCMSC | ultracentrifugation | 40–100 | liver directly injected/250 μg (330 μL) | C:6 T:6 | single after injure | 3 weeks after therapy | serum AST, ALT |
| Liu (2018) China [39] | C57BL/6J mice | LPS/D-GalN or TNF-α/D-GalN induce ALF | mouse-ADSC | commercial kits | 40–100 | tail vein/400 μg (300 μL) | C:6 T:6 | single after injure | 6 h after treapy | Serum ALT, AST; serum TNF-α, IFN-γ, IL-1β, IL-6, IL-18 |
| Lu (2019) China [48] | C57BL/6 mice male | AIH | mouce-BMSC | ultracentrifugation | 40–100 | tail vein/2 µg/g (200 µL) | C:6 T:6 | Day 21/35 after injure | 3 weeks after therapy | serum ALT, AST; The histological scoring Ishak; serum IL-1β, IL-6, IL-17, and IL-10 |
| Mardpour (2018) Iran [23] | wistar rats male | TAA induce liver fibrosis | hES-MSC | ultracentrifugation | NA | infused intrasplenicly/350 µg (4 × 106 cells, 400 µL) | C:4 T:4 | single after injure | 4 weeks after therapy | serum ALT, ALP, and GGT (γ-GT); IL-10 and TNF-α in serum; Ishak’s score; fibrous-positive area (masson-trichrome); |
| Mardpour (2019) Iran [24] | wistar rats male | TAA induce liver fibrosis | hES-MSC | ultracentrifugation | 190.8 ± 18 | intraperitoneal/350 μg (400 μL) | C:4 T:4 | single after injure | 4 weeks after therapy | serum ALT, AST, ALP, GGT; serum TNF-α, IL10; Ishak’s score; the positive fibrosis area% (Masson trichrome) |
| Ohara (2018) Japan [25] | Sprague-Dawley rats male | CCL4 induce liver fibrosis | hAMSC | Ultracentrifugation | 80–110 | penile vein/15 μg/kg and 20 μg/kg (200 μL) | C:15 T:15 | single after injure | 4 weeks after therapy | fibrosis area (Masson trichrome staining) |
| Rong (2019) China [26] | Sprague-Dawley rats female | CCL4 induce liver fibrosis | hBMSC | ultracentrifugation | 30–100 | tail vein/250 mg (500 μL) | C:3 T:3 | single after injure | 4 weeks after treatment | serum ALT, AST, ALP, γ-GT; liver index%; Hyp in liver tissue; Ishak scoring; Collagen area% (Masson, and Sirius red) |
| Rostom (2020) Egypt [27] | Sprague-Dawley albino rats male | CCL4 induce liver fibrosis | rat-BMSC | ultracentrifugation | 113.7 | tail vein/80 μg | C:6 T:6 | single after injure | 4 weeks after treatment | serum AST, ALT, ALB; Ishak grade; area percentage of collagen fibers |
| Sabry (2019) Egypt [28] | white albino rats female | CCL4 induce liver fibrosis | rat-BMSC | ultracentrifugation | NA | tail vein/4 μg (1 mL) | C:15 T:15 | twice weekly for 4 weeks after injure | 4 weeks after treatment | serum ALT, ALB |
| Takeuchi (2021) Japan [29] | C57BL/6 mice male | CCL4 induce liver fibrosis | hADSC | ultracentrifugation | NA | i.v./2 μg, or 5 μg | C:5 T:5 | single after injure | 4 weeks after treatment | serum ALT, ALP, ALB; Sirius Red-stained areas; Hyp levels |
| Tamura (2016) Japan [15] | C57B6 mice male | con-A induce AIH | mouse-BMSC | ultracentrifugation | 135 | i.v./10 μg (0.1 mL) | C:5 T:5 | once and three times after injure | after therapy | plasma ALT; necrotic area (hematoxylin-eosin staining) |
| Tan (2014) Singapore [40] | C57BL/6 mice male | CCl4 induce ALI | hESC | tangential flow filtration (TFF) | 55–65 | intrasplenic injection (i.s.)./0.4 μg (100 μL) | C:6 T:6 | 24 h after injure | 24 h after therapy | serum AST, ALT |
| Wang (2021) China [30] | ICR mice Male | CCL4 induce liver fibrosis | hESC | NA | 120–140 | i.v./NA | C:3 T:3 | twice a week for 4 weeks after injure | 1/2/3/4 week after treatment | serum ALT, AST, ALB |
| Watanabe (2020) Japan [46] | Mc4r-KO C57BL/6J mice NA | NAFLD | hADSC | ultracentrifugation | NA | tail vein/1.0 mg, 2.5 mg, or 5.0 mg | C:8 T:8 | single after injure | 24 h after therapy | LW/BW; serum ALT, ALP, ALB |
| Xuan (2022) China [31] | C57BL/6 J mice Either sex | TAA induce liver fibrosis | mouse-BMSC | centrifugation and filter | NA | tail vein/5 × 105 cells | C:12 T:12 | single after injure | day 21 after treatment | serum ALT, AST level; positive staining areas (Sirius Red staining) |
| Yan (2017) China [41] | BALB/c-nu/nu mice female | CCl4 induce ALF | hUCMSC | ultracentrifugation | NA | tail vein and oral gavage/8 mg/kg, 16 mg/kg, 32 mg/kg; the final 20 mg/mL | C:20 T:20 | single after injure | 72 h after therapy | Serum AST, ALT; Serum IFN-α, IL-1 α, IL-6, TNF-α |
| Yao (2019) China [52] | Sprague-Dawley rats male | IRI | hUCMSC | ultracentrifugation | 178 ± 64 | tail vein/10 mg/kg | C:5 T:5 | single after injure | after 24 h reperfusion | serum ALT, AST, ALP; necrosis area%(H&E); serum IL-1b, IL-6, and TNF-a |
| You (2021) Korea [32] | C57BL/6 mice male | TAA induce liver fibrosis | ADSC | tangential flow filtration (TFF) | 117 ± 7 | i.v./(1 × 107 particles), or (1 × 108 particles) | C:5 T:5 | single or three times after injure | 24 h after treatment | Serum AST; fibrotic areas (Sirius Red) |
| Zhang (2022) China [42] | C57BL/6 mice Male | THS induce ALI | mouse-BMSC | gradient centrifugation | 90–142 | femoral artery/20 μg | C:5 T:5 | single after resuscitation | 72 h after resuscitation | serum ALT, AST, LDH |
| Zhang1 (2020) China [53] | Sprague Dawley rats male | IRI | hUCMSC | ultracentrifugation | NA | NA | C:3 T:3 | NA | 24 h after reperfusion | serum ALT, AST; |
| Zhang2 (2020) China [43] | C57BL/6 mice male | LPS + D-GalN induce ALF | hUCMSC | ultracentrifugation | 30–150 | tail vein/100 mg | C:3 T:3 | 1 h after injure | 12 h after treatment | Serum ALT; LW/BW; IL-6, IL-1β, IL-18 in serum |
| Zhao (2021) China [49] | BALB/c mice | con-A induce AIH | mouse-BMSC | ultracentrifugation | 120 | i.v./5 mg/kg (100 µL) | C:5 T:5 | single after injure | 8 h after treatment | serum ALT, AST level; inflammatory cytokine levels; TNF-α, INF-γ, IL-1β, IL-6, IL-12 |
| Zheng (2020) China [54] | C57BL/6 mice male | IRI | hUCMSC | ultracentrifugation | 30–150 | i.v./100 µg/100 µL | C:5 T:5 | single after injure | 6 h after reperfusion | sreum ALT, AST, LDH; IFN-γ, IL-6, and TNF-α in serum; |
| Outcomes | Number of Animals | Std. Mean Difference (95%CI) | Test for Effect (P Value) | Heterogeneity, I2 |
|---|---|---|---|---|
| TNF-α | 104 | −4.60 [−6.45, −2.75] | P < 0.01 | I2 = 79% |
| IL-1β | 110 | −4.34 [−6.02, −2.66]; | P < 0.01; | I2 = 77% |
| IL-6 | 102 | −5.26 [−7.07, −3.45]; | P < 0.01 | I2 = 70% |
| IFN-γ | 32 | −2.94 [−4.11, −1.78]; | P < 0.01 | I2 = 0% |
| IL-10 | 28 | 3.66 [2.14, 5.17] | P < 0.01 | I2 = 0% |
| Outcomes | Number of Animals | Std. Mean Difference (95%CI) | Test for Effect (P Value) | Heterogeneity, I2 |
|---|---|---|---|---|
| ALB | 38 | −0.73 [−2.97, 1.51] | P = 0.52 | I2 = 86% |
| ALT | 112 | −0.39 [−1.34, 0.55] | P = 0.41; | I2 = 78% |
| AST | 68 | −0.88 [−2.08, 0.31] | P = 0.15; | I2 = 76% |
| ALP | 34 | −1.17 [−2.54, 0.19] | P = 0.09; | I2 = 60% |
| TNF-α | 28 | 0.01 [−1.11, 1.14] | P = 0.98; | I2 = 50 |
| the damage area | 92 | −1.32 [−2.25, −0.38] | P < 0.01 | I2 = 68% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fang, X.; Gao, F.; Yao, Q.; Xu, H.; Yu, J.; Cao, H.; Li, S. Pooled Analysis of Mesenchymal Stromal Cell-Derived Extracellular Vesicle Therapy for Liver Disease in Preclinical Models. J. Pers. Med. 2023, 13, 441. https://doi.org/10.3390/jpm13030441
Fang X, Gao F, Yao Q, Xu H, Yu J, Cao H, Li S. Pooled Analysis of Mesenchymal Stromal Cell-Derived Extracellular Vesicle Therapy for Liver Disease in Preclinical Models. Journal of Personalized Medicine. 2023; 13(3):441. https://doi.org/10.3390/jpm13030441
Chicago/Turabian StyleFang, Xinru, Feiqiong Gao, Qigu Yao, Haoying Xu, Jiong Yu, Hongcui Cao, and Shibo Li. 2023. "Pooled Analysis of Mesenchymal Stromal Cell-Derived Extracellular Vesicle Therapy for Liver Disease in Preclinical Models" Journal of Personalized Medicine 13, no. 3: 441. https://doi.org/10.3390/jpm13030441