
Accuracy of Conventional and Digital Impressions for Full-Arch Implant-Supported Prostheses: An In Vitro Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
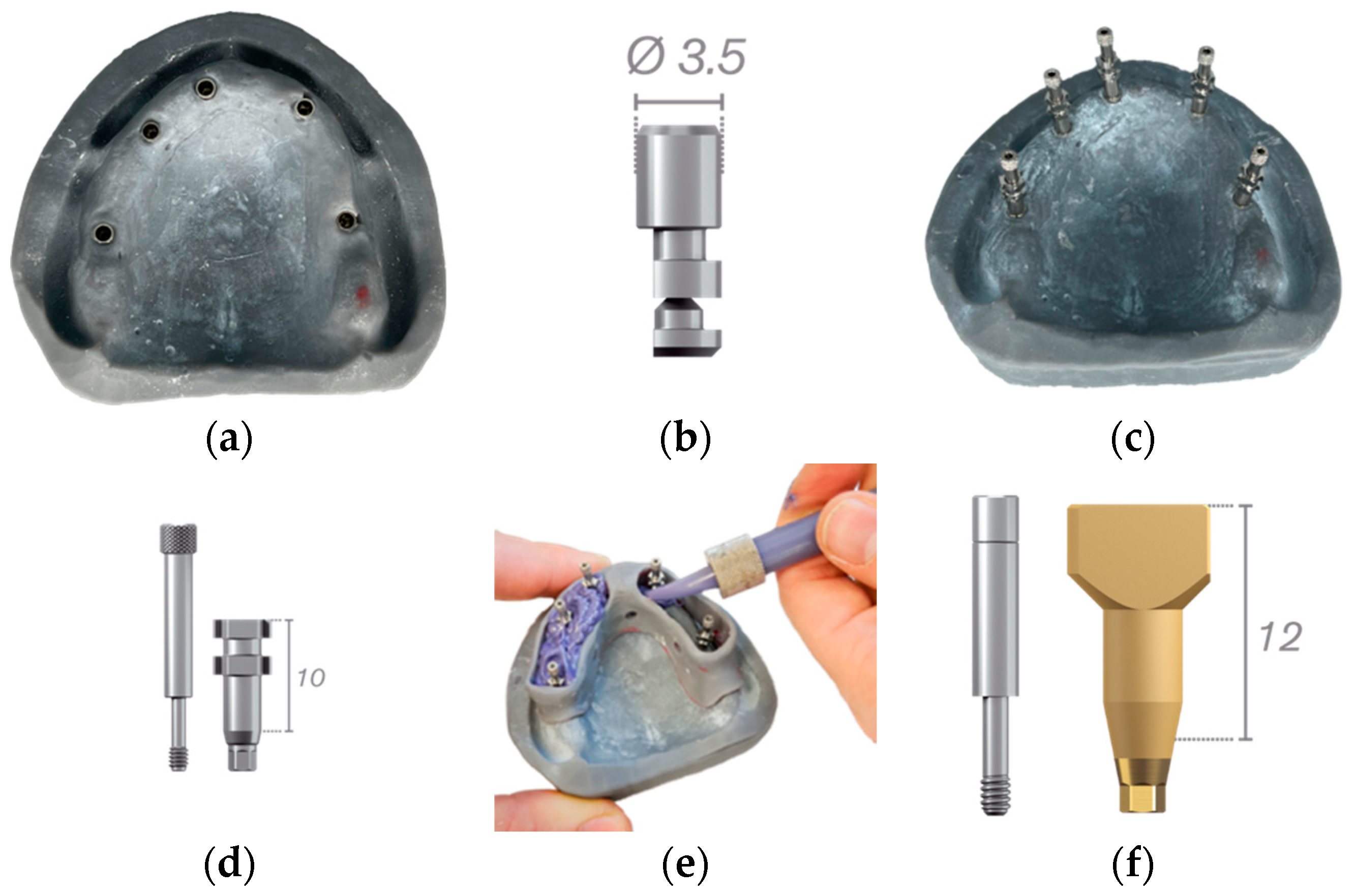
2.2. Working Model
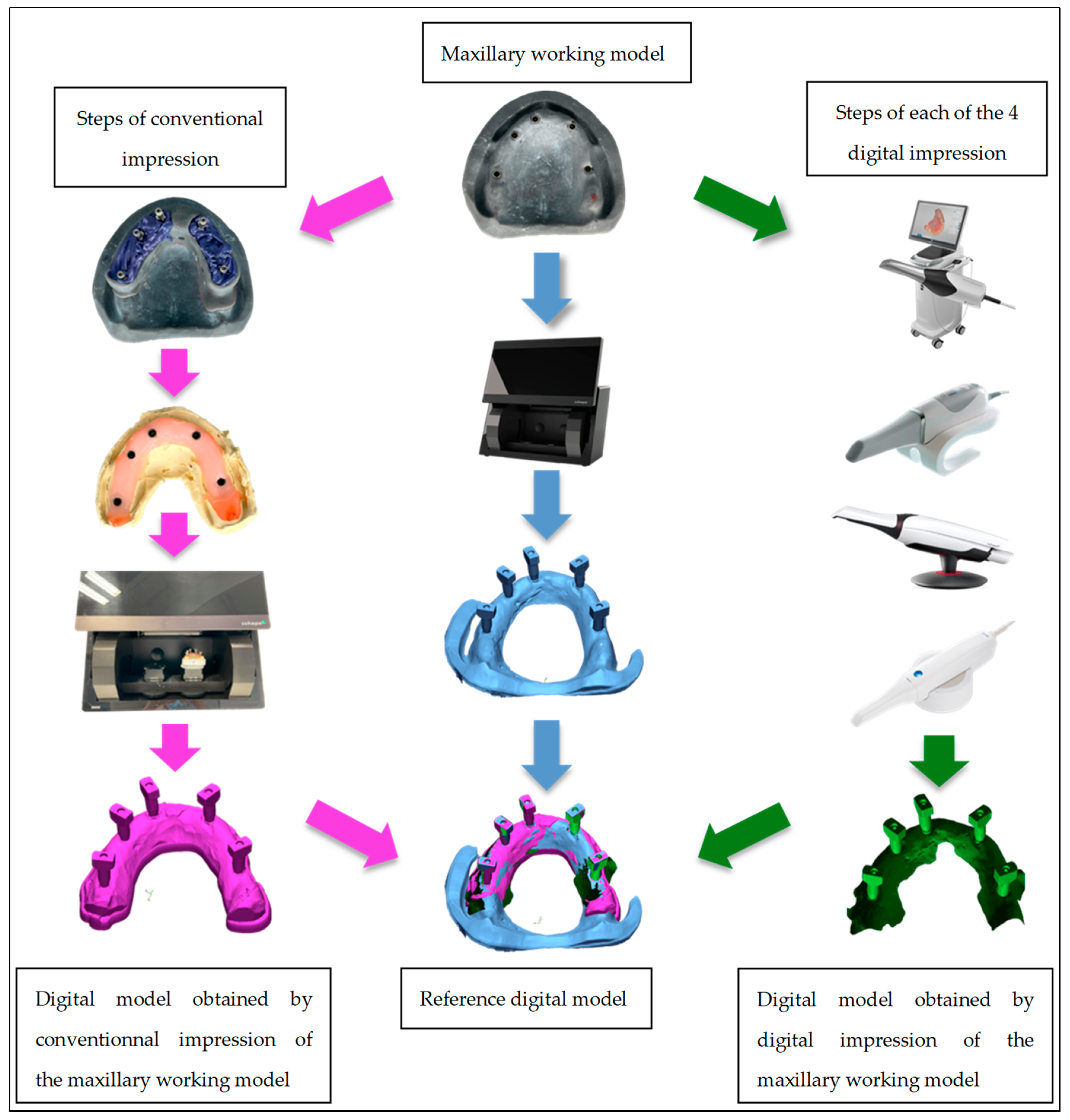
2.3. Conventional Impression
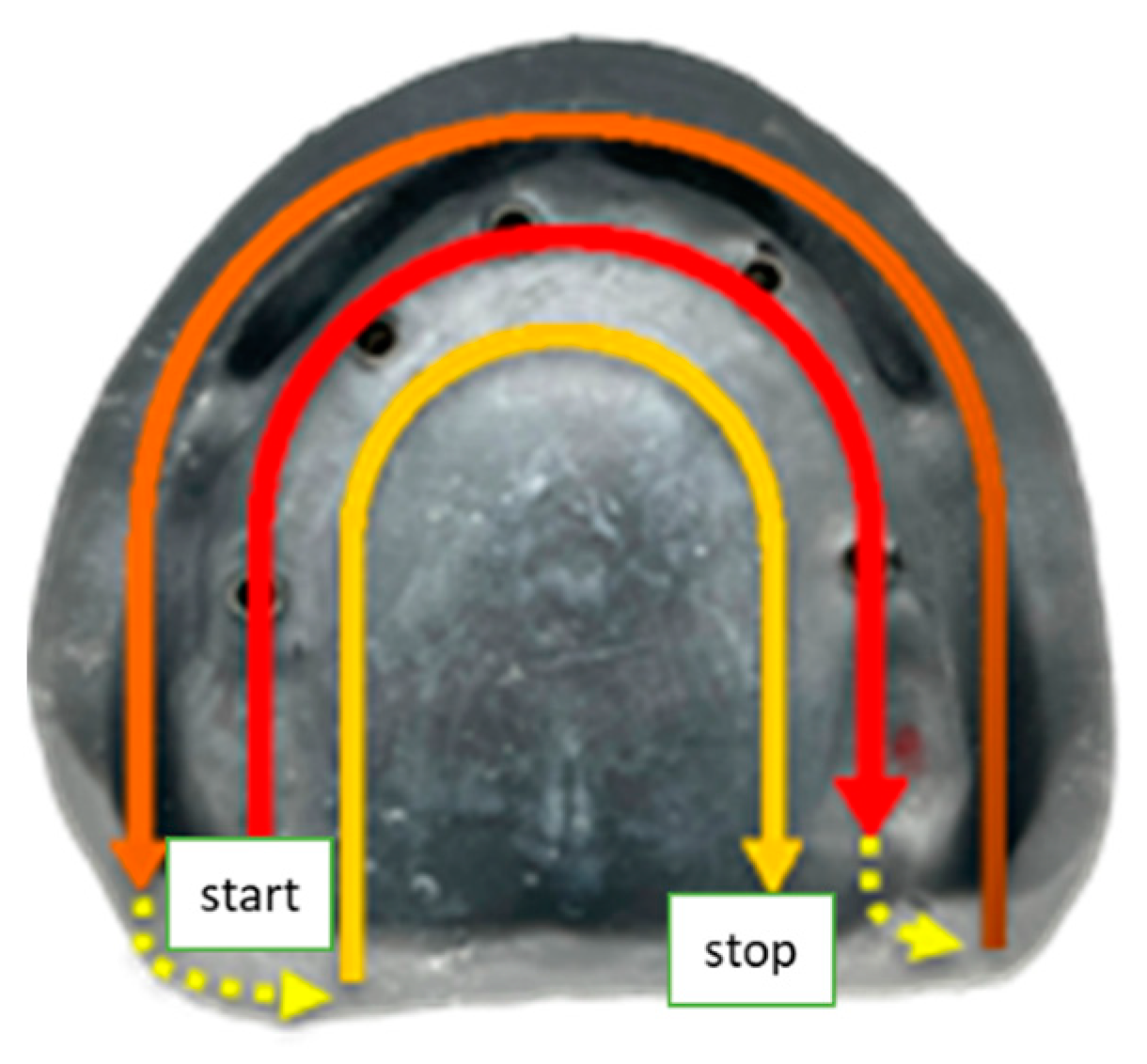
2.4. Digital Impression
2.5. Comparison of Digital Models
3. Results
3.1. Trueness
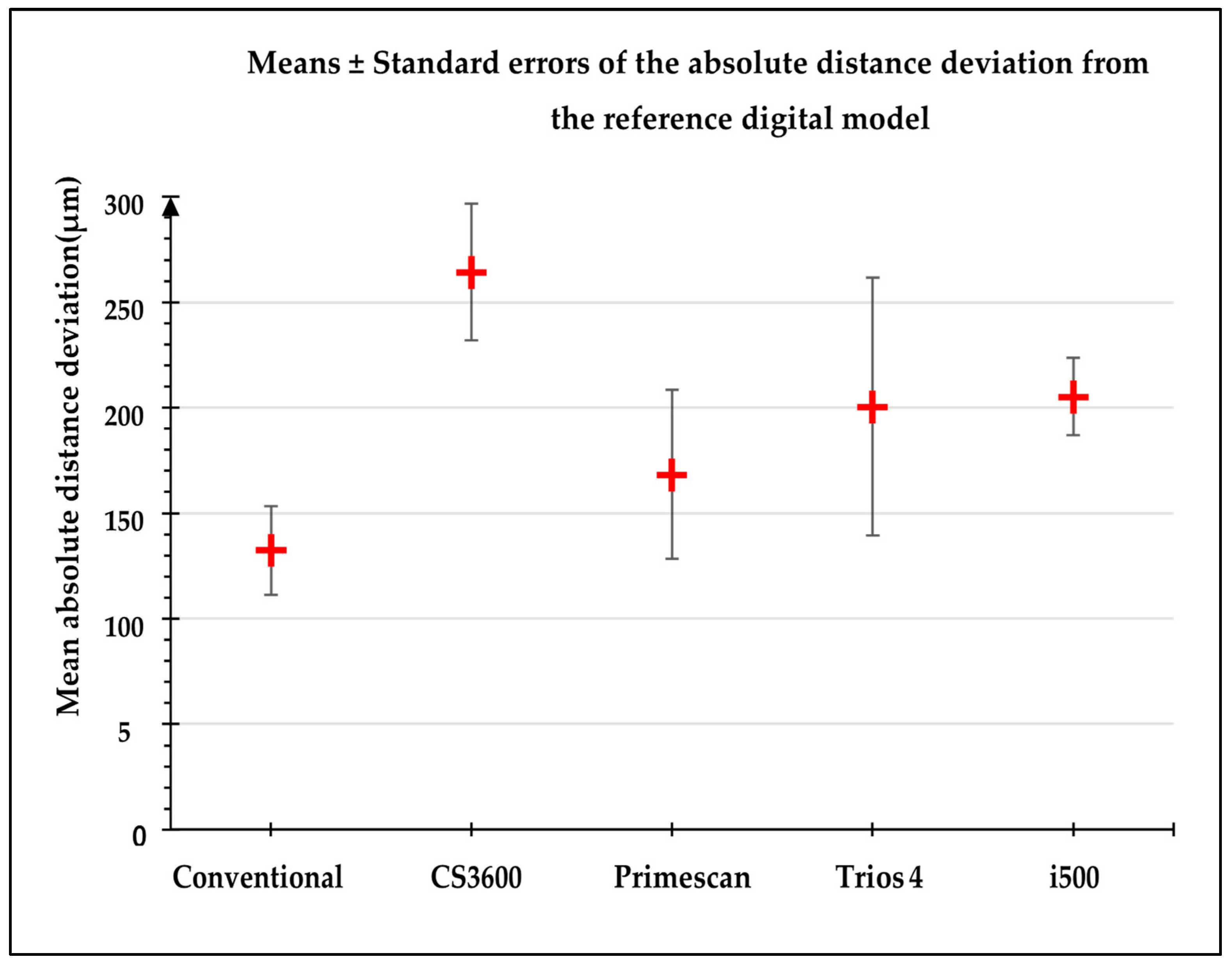
3.1.1. Distances Deviation in Absolute Value According to the Impression Type
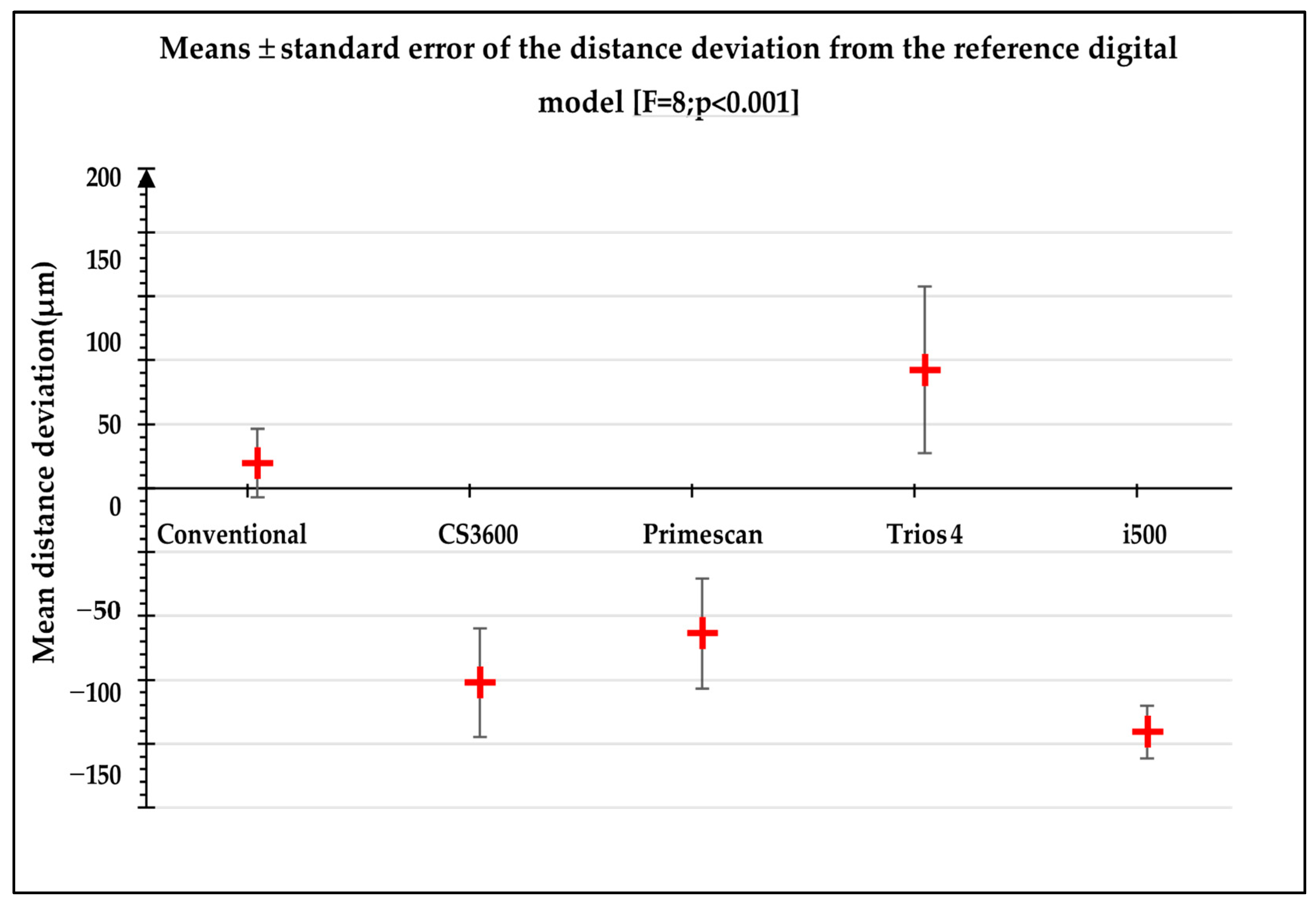
3.1.2. Direction of the Distance Deviations According to the Impression Type
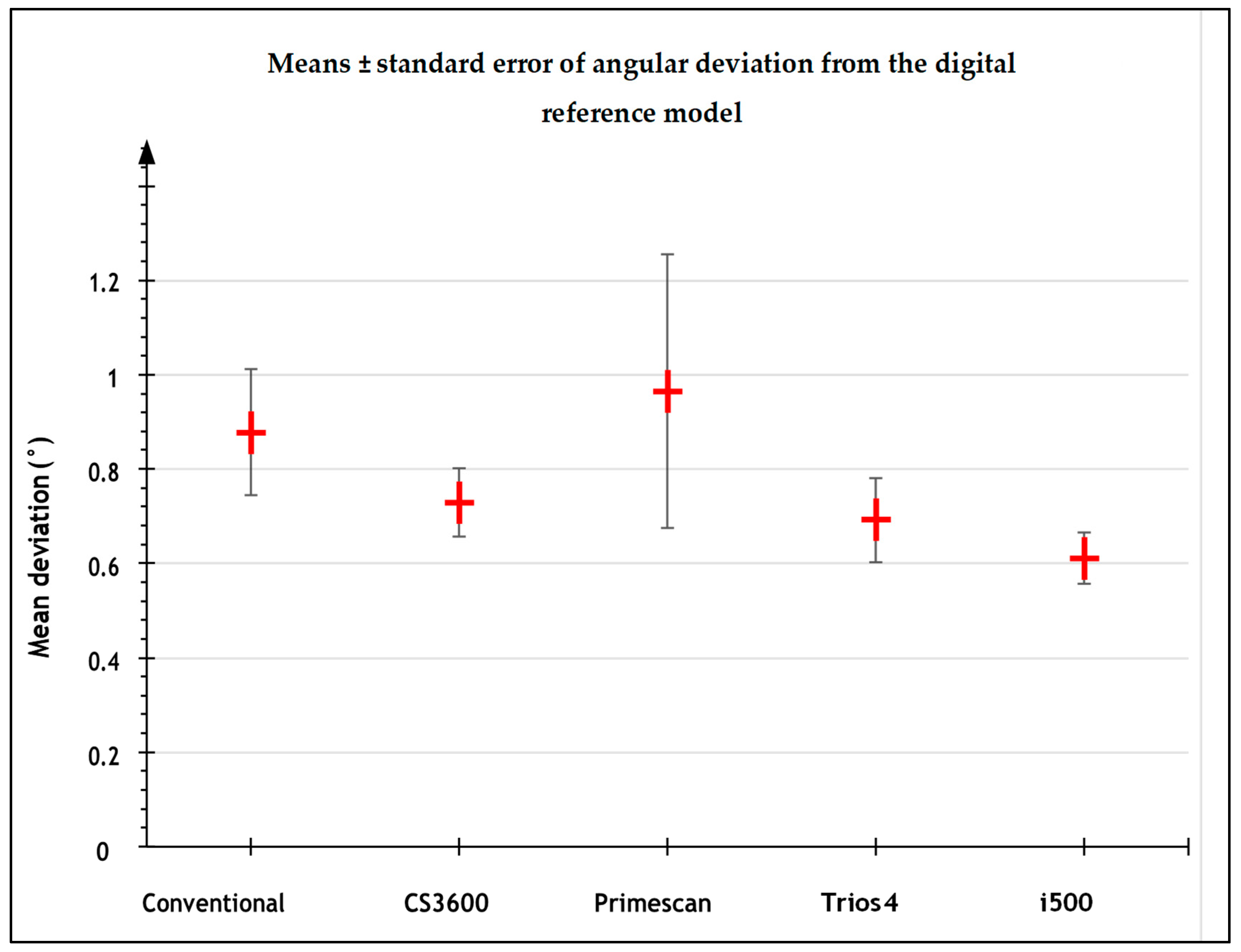
3.1.3. Angular Deviations According to the Type of Impression
3.2. Precision
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baldissara, P.; Koci, B.; Messias, A.M.; Meneghello, R.; Ghelli, F.; Gatto, M.R.; Ciocca, L. Assessment of impression material accuracy in complete-arch restorations on four implants. J. Prosthet. Dent. 2021, 126, 763–771. [Google Scholar] [CrossRef]
- Baig, M.R. Multi-unit implant impression accuracy: A review of the literature. Quintessence Int. 2014, 45, 39–51. [Google Scholar] [CrossRef]
- Amin, S.; Weber, H.P.; Finkelman, M.; El Rafie, K.; Kudara, Y.; Papaspyridakos, P. Digital vs. conventional full-arch implant impressions: A comparative study. Clin. Oral. Implants Res. 2017, 28, 1360–1367. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; So, J.S.; Hochstedler, J.L.; Ercoli, C. The accuracy of implant impressions: A systematic review. J. Prosthet. Dent. 2008, 100, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Renne, W.; Ludlow, M.; Fryml, J.; Schurch, Z.; Mennito, A.; Kessler, R.; Lauer, A. Evaluation of the accuracy of 7 digital scanners: An in vitro analysis based on 3-dimensional comparisons. J. Prosthet. Dent. 2017, 118, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Ender, A.; Mehl, A. Accuracy of complete-arch dental impressions: A new method of measuring trueness and precision. J. Prosthet. Dent. 2013, 109, 121–128. [Google Scholar] [CrossRef]
- Cervino, G.; Fiorillo, L.; Herford, A.S.; Laino, L.; Troiano, G.; Amoroso, G.; Crimi, S.; Matarese, M.; D’Amico, C.; Nastro Siniscalchi, E.; et al. Alginate Materials and Dental Impression Technique: A Current State of the Art and Application to Dental Practice. Mar. Drugs 2018, 17, 18. [Google Scholar] [CrossRef]
- Goracci, C.; Franchi, L.; Vichi, A.; Ferrari, M. Accuracy, reliability, and efficiency of intraoral scanners for full-arch impressions: A systematic review of the clinical evidence. Eur. J. Orthod. 2016, 38, 422–428. [Google Scholar] [CrossRef] [PubMed]
- Nulty, A.B. A Comparison of Full Arch Trueness and Precision of Nine Intra-Oral Digital Scanners and Four Lab Digital Scanners. Dent. J. 2021, 9, 75. [Google Scholar] [CrossRef] [PubMed]
- Di Fiore, A.; Meneghello, R.; Graiff, L.; Savio, G.; Vigolo, P.; Monaco, C.; Stellini, E. Full arch digital scanning systems performances for implant-supported fixed dental prostheses: A comparative study of 8 intraoral scanners. J. Prosthodont. Res. 2019, 63, 396–403. [Google Scholar] [CrossRef]
- Yuzbasioglu, E.; Kurt, H.; Turunc, R.; Bilir, H. Comparison of digital and conventional impression techniques: Evaluation of patients’ perception, treatment comfort, effectiveness and clinical outcomes. BMC Oral. Health 2014, 14, 10. [Google Scholar] [CrossRef] [PubMed]
- A Quick Start Guide for the First Scan Using the i500. Available online: https://support.medit.com/hc/en-us/articles/360042009112-A-quick-start-guide-for-the-first-scan-using-the-i500 (accessed on 25 March 2023).
- Carestream DENTAL CS 3600 User and Installation Manual (Page 8 of 22)|ManualsLib. Available online: https://www.manualslib.com/manual/2313009/Carestream-Dental-Cs-3600.html?page=8 (accessed on 25 March 2023).
- Caméra Primescan|Dentsply Sirona France. Available online: https://www.dentsplysirona.com/content/dentsply-sirona/fr-fr/decouvrez-nos-produits/impression-numerique/primescan.html (accessed on 25 March 2023).
- ISO 5725-1; Accuracy (Trueness and Precision) of Measuring Methods and Results. Part-I: General Principles and Definitions. Beuth Verlag GmbH: Berlin, Germany, 1994.
- Katsoulis, J.; Takeichi, T.; Sol Gaviria, A.; Peter, L.; Katsoulis, K. Misfit of implant prostheses and its impact on clinical outcomes. Definition, assessment and a systematic review of the literature. Eur. J. Oral. Implantol. 2017, 10 (Suppl. 1), 121–138. [Google Scholar] [PubMed]
- Papaspyridakos, P.; Chen, C.-J.; Gallucci, G.O.; Doukoudakis, A.; Weber, H.-P.; Chronopoulos, V. Accuracy of implant impressions for partially and completely edentulous patients: A systematic review. Int. J. Oral. Maxillofac. Implants 2014, 29, 836–845. [Google Scholar] [CrossRef]
- Toia, M.; Stocchero, M.; Jinno, Y.; Wennerberg, A.; Becktor, J.P.; Jimbo, R.; Halldin, A. Effect of Misfit at Implant-Level Framework and Supporting Bone on Internal Connection Implants: Mechanical and Finite Element Analysis. Int. J. Oral. Maxillofac. Implants 2019, 34, 320–328. [Google Scholar] [CrossRef]
- Heckmann, S.M.; Karl, M.; Wichmann, M.G.; Winter, W.; Graef, F.; Taylor, T.D. Cement fixation and screw retention: Parameters of passive fit. An in vitro study of three-unit implant-supported fixed partial dentures. Clin. Oral. Implants Res. 2004, 15, 466–473. [Google Scholar] [CrossRef]
- Giachetti, L.; Sarti, C.; Cinelli, F.; Russo, D.S. Accuracy of Digital Impressions in Fixed Prosthodontics: A Systematic Review of Clinical Studies. Int. J. Prosthodont. 2020, 33, 192–201. [Google Scholar] [CrossRef]
- Chebib, N.; Kalberer, N.; Srinivasan, M.; Maniewicz, S.; Perneger, T.; Müller, F. Edentulous jaw impression techniques: An in vivo comparison of trueness. J. Prosthet. Dent. 2019, 121, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Sawase, T.; Kuroshima, S. The current clinical relevancy of intraoral scanners in implant dentistry. Dent. Mater. J. 2020, 39, 57–61. [Google Scholar] [CrossRef]
- Li, H.; Lyu, P.; Wang, Y.; Sun, Y. Influence of object translucency on the scanning accuracy of a powder-free intraoral scanner: A laboratory study. J. Prosthet. Dent. 2017, 117, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Revilla-León, M.; Jiang, P.; Sadeghpour, M.; Piedra-Cascón, W.; Zandinejad, A.; Özcan, M.; Krishnamurthy, V.R. Intraoral digital scans-Part 1: Influence of ambient scanning light conditions on the accuracy (trueness and precision) of different intraoral scanners. J. Prosthet. Dent. 2020, 124, 372–378. [Google Scholar] [CrossRef]
- Revilla-León, M.; Jiang, P.; Sadeghpour, M.; Piedra-Cascón, W.; Zandinejad, A.; Özcan, M.; Krishnamurthy, V.R. Intraoral digital scans: Part 2-influence of ambient scanning light conditions on the mesh quality of different intraoral scanners. J. Prosthet. Dent. 2020, 124, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Kurz, M.; Attin, T.; Mehl, A. Influence of material surface on the scanning error of a powder-free 3D measuring system. Clin. Oral. Investig. 2015, 19, 2035–2043. [Google Scholar] [CrossRef] [PubMed]
- Abduo, J. Accuracy of casts produced from conventional and digital workflows: A qualitative and quantitative analyses. J. Adv. Prosthodont. 2019, 11, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Arcuri, L.; Pozzi, A.; Lio, F.; Rompen, E.; Zechner, W.; Nardi, A. Influence of implant scanbody material, position and operator on the accuracy of digital impression for complete-arch: A randomized in vitro trial. J. Prosthodont. Res. 2020, 64, 128–136. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Distances between Scanbodies | Conventional | CS3600® | Primescan® | i500® | Trios 4® |
|---|---|---|---|---|---|
| 1–2 | 66.6 | 179.6 | 25.7 | 109.8 | 167.8 |
| 1–3 | 62.6 | 168.7 | 35.7 | 118.7 | 149.8 |
| 1–4 | 88.0 | 165.7 | 204.2 | 116.5 | 229.1 |
| 1–5 | 173.7 | 260.8 | 82.7 | 114.6 | 142.5 |
| 2–3 | 47.2 | 85.1 | 35.8 | 35.2 | 18.4 |
| 3–4 | 48.7 | 234.2 | 381.9 | 59.3 | 710.4 |
| 4–5 | 399.0 | 335.9 | 282.0 | 111.3 | 217.4 |
| Mean ± SD | 126.5 ± 128 | 204.3 ± 81 | 149.7 ± 142 | 95.1 ± 34 | 233.6 ± 221 |
| Angles | Conventional | CS3600® | Primescan® | i500® | Trios 4® |
|---|---|---|---|---|---|
| Scanbody 1 | 0.190 | 0.269 | 0.266 | 0.310 | 0.283 |
| Scanbody 2 | 0.077 | 0.266 | 0.304 | 0.138 | 0.210 |
| Scanbody 3 | 0.161 | 0.236 | 0.327 | 0.115 | 0.231 |
| Scanbody 4 | 0.338 | 0.235 | 2.413 | 0.140 | 0.230 |
| Scanbody 5 | 0.818 | 0.571 | 1.517 | 0.355 | 0.661 |
| Mean ± SD | 0.317 ± 0.296 | 0.315 ± 0.144 | 0.965 ± 0.966 | 0.212 ± 0.112 | 0.323 ± 0.191 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drancourt, N.; Auduc, C.; Mouget, A.; Mouminoux, J.; Auroy, P.; Veyrune, J.-L.; El Osta, N.; Nicolas, E. Accuracy of Conventional and Digital Impressions for Full-Arch Implant-Supported Prostheses: An In Vitro Study. J. Pers. Med. 2023, 13, 832. https://doi.org/10.3390/jpm13050832
Drancourt N, Auduc C, Mouget A, Mouminoux J, Auroy P, Veyrune J-L, El Osta N, Nicolas E. Accuracy of Conventional and Digital Impressions for Full-Arch Implant-Supported Prostheses: An In Vitro Study. Journal of Personalized Medicine. 2023; 13(5):832. https://doi.org/10.3390/jpm13050832
Chicago/Turabian StyleDrancourt, Noemie, Chantal Auduc, Aymeric Mouget, Jean Mouminoux, Pascal Auroy, Jean-Luc Veyrune, Nada El Osta, and Emmanuel Nicolas. 2023. "Accuracy of Conventional and Digital Impressions for Full-Arch Implant-Supported Prostheses: An In Vitro Study" Journal of Personalized Medicine 13, no. 5: 832. https://doi.org/10.3390/jpm13050832
APA StyleDrancourt, N., Auduc, C., Mouget, A., Mouminoux, J., Auroy, P., Veyrune, J.-L., El Osta, N., & Nicolas, E. (2023). Accuracy of Conventional and Digital Impressions for Full-Arch Implant-Supported Prostheses: An In Vitro Study. Journal of Personalized Medicine, 13(5), 832. https://doi.org/10.3390/jpm13050832