
Single-Setting 3D MRI/US-Guided Frozen Sectioning and Cryoablation of the Index Lesion: Mid-Term Oncologic and Functional Outcomes from a Pilot Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Preoperative Preparation
2.3. Surgical Technique
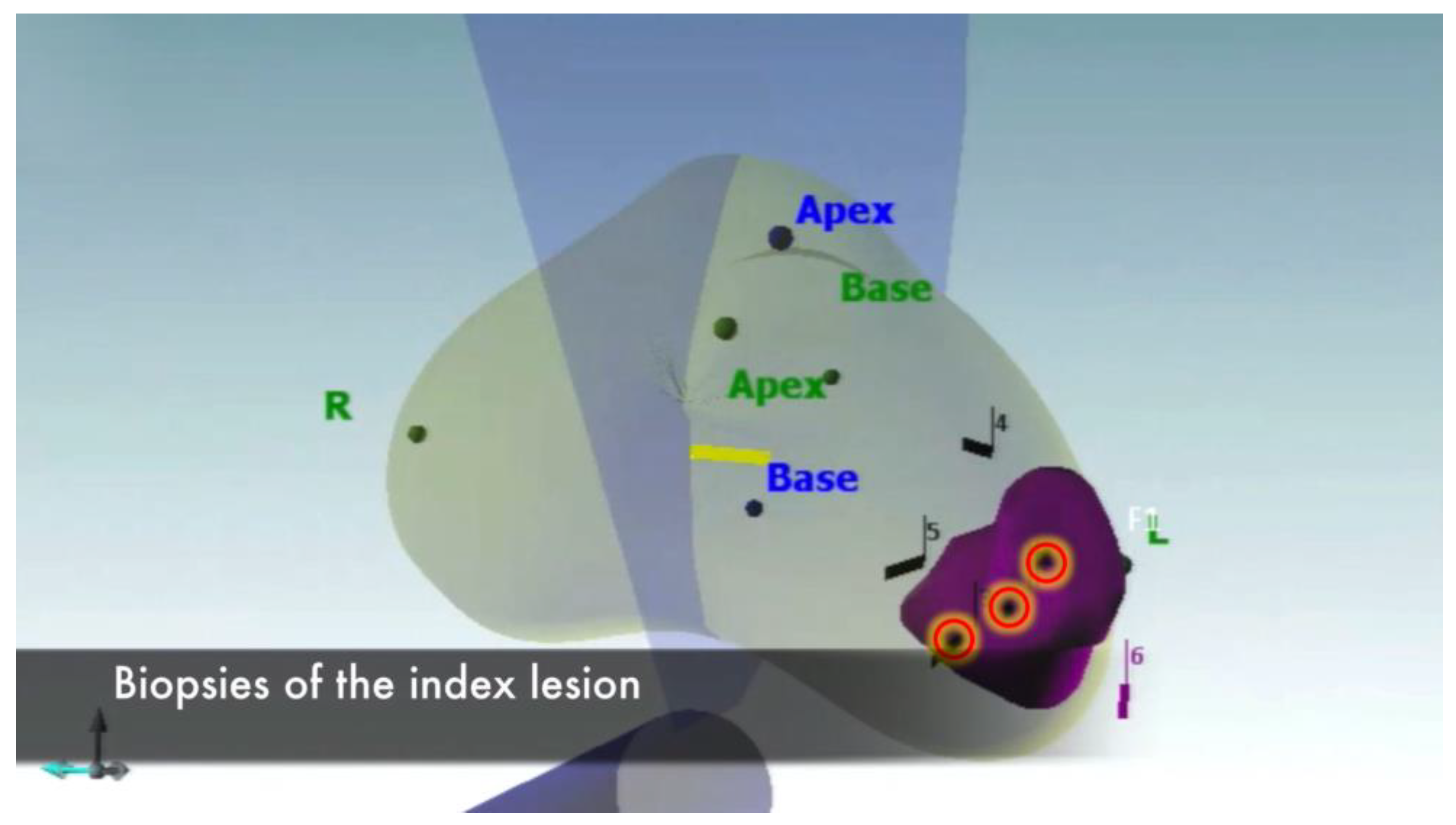
2.3.1. MRI–US Fusion Biopsies of the Index Lesion
2.3.2. Biopsies of the Area Surrounding the Index Lesion
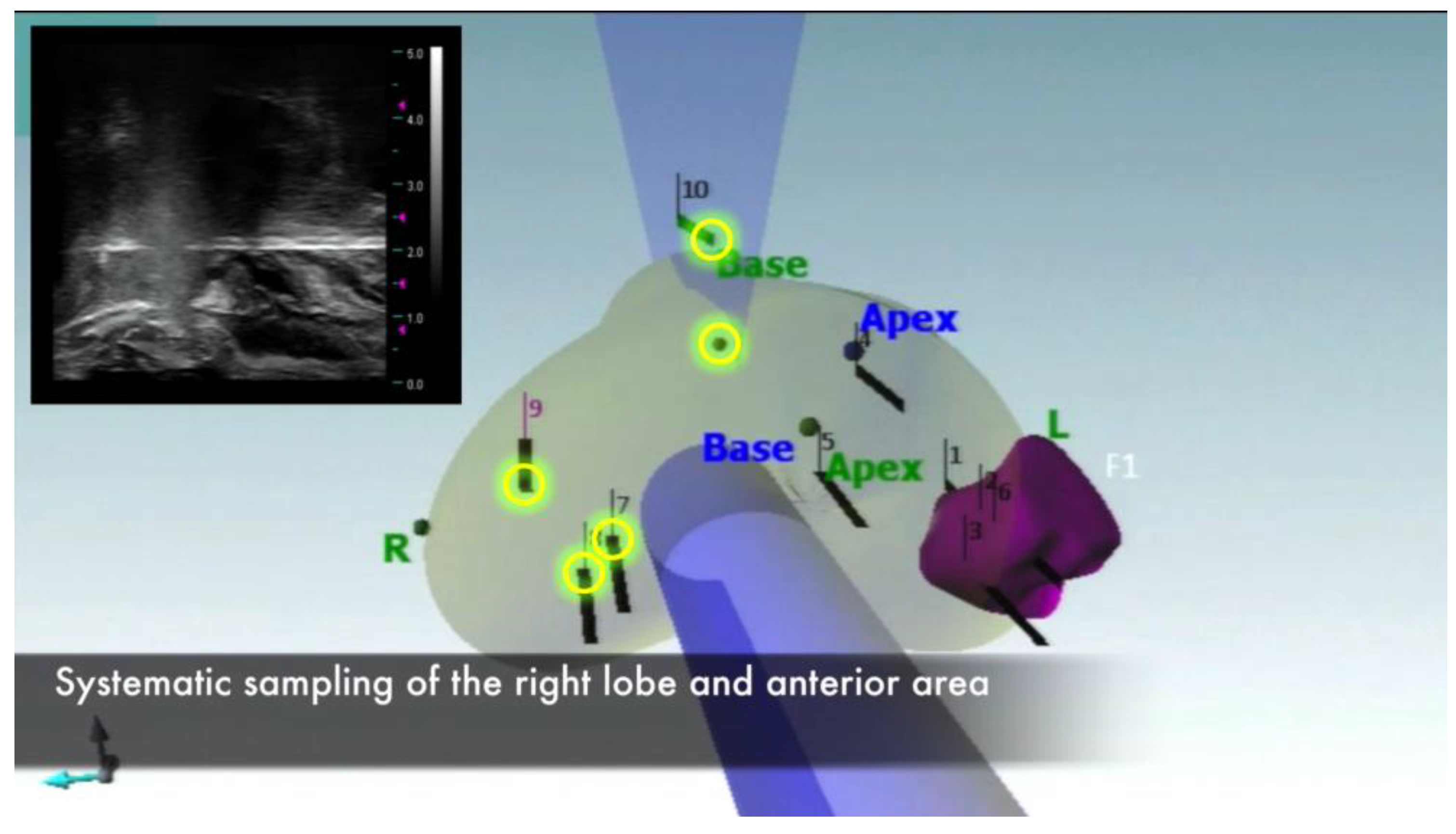
2.3.3. Systematic Prostate Biopsy
2.3.4. Frozen Section
2.3.5. Procedure Planning
2.3.6. Cryoprobe and Thermocouple Placement
2.3.7. Urethral Warming Catheter Placement
2.3.8. Focal Cryoablation
2.4. Postoperative Course and Follow-Up
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mottet, N.; van den Bergh, R.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.; De Santis, M.; Fanti, S. EAU Guidelines of Prostate Cancer. 2022. Available online: Https://Uroweb.Org/Guidelines/Prostate-Cancer (accessed on 20 March 2023).
- Haas, G.P.; Delongchamps, N.; Brawley, O.W.; Wang, C.Y.; de la Roza, G. The Worldwide Epidemiology of Prostate Cancer: Perspectives from Autopsy Studies. Can. J. Urol. 2008, 15, 3866–3871. [Google Scholar]
- Kim, M.; Choi, S.-K.; Park, M.; Shim, M.; Song, C.; Jeong, I.G.; Hong, J.H.; Kim, C.-S.; Ahn, H. Characteristics of Anteriorly Located Prostate Cancer and the Usefulness of Multiparametric Magnetic Resonance Imaging for Diagnosis. J. Urol. 2016, 196, 367–373. [Google Scholar] [CrossRef]
- Schouten, M.G.; van der Leest, M.; Pokorny, M.; Hoogenboom, M.; Barentsz, J.O.; Thompson, L.C.; Fütterer, J.J. Why and Where Do We Miss Significant Prostate Cancer with Multi-Parametric Magnetic Resonance Imaging Followed by Magnetic Resonance-Guided and Transrectal Ultrasound-Guided Biopsy in Biopsy-Naïve Men? Eur. Urol. 2017, 71, 896–903. [Google Scholar] [CrossRef] [PubMed]
- de Marini, P.; Cazzato, R.L.; Garnon, J.; Shaygi, B.; Koch, G.; Auloge, P.; Tricard, T.; Lang, H.; Gangi, A. Percutaneous MR-Guided Prostate Cancer Cryoablation Technical Updates and Literature Review. BJR Open 2019, 1, 20180043. [Google Scholar] [CrossRef] [PubMed]
- van der Poel, H.G.; van den Bergh, R.C.N.; Briers, E.; Cornford, P.; Govorov, A.; Henry, A.M.; Lam, T.B.; Mason, M.D.; Rouvière, O.; De Santis, M.; et al. Focal Therapy in Primary Localised Prostate Cancer: The European Association of Urology Position in 2018. Eur. Urol. 2018, 74, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Valerio, M.; Cerantola, Y.; Eggener, S.E.; Lepor, H.; Polascik, T.J.; Villers, A.; Emberton, M. New and Established Technology in Focal Ablation of the Prostate: A Systematic Review. Eur. Urol. 2017, 71, 17–34. [Google Scholar] [CrossRef]
- Fahmy, W.E.; Bissada, N.K. Cryosurgery for Prostate Cancer. Arch. Androl. 2003, 49, 397–407. [Google Scholar] [CrossRef] [PubMed]
- Rees, J.; Patel, B.; MacDonagh, R.; Persad, R. Cryosurgery for Prostate Cancer. BJU Int. 2004, 93, 710–714. [Google Scholar] [CrossRef] [PubMed]
- Han, K.-R.; Belldegrun, A.S. Third-Generation Cryosurgery for Primary and Recurrent Prostate Cancer. BJU Int. 2004, 93, 14–18. [Google Scholar] [CrossRef]
- Onik, G. Percutaneous Image-Guided Prostate Cancer Treatment: Cryoablation as a Successful Example. Tech. Vasc. Interv. Radiol. 2007, 10, 149–158. [Google Scholar] [CrossRef]
- Morrison, P.R.; Silverman, S.G.; Tuncali, K.; Tatli, S. MRI-Guided Cryotherapy. J. Magn. Reson. Imaging 2008, 27, 410–420. [Google Scholar] [CrossRef] [PubMed]
- Cazzato, R.L.; Garnon, J.; Shaygi, B.; Tsoumakidou, G.; Caudrelier, J.; Koch, G.; Gangi, A. How to Perform a Routine Cryoablation Under MRI Guidance. Top. Magn. Reson. Imaging 2018, 27, 33–38. [Google Scholar] [CrossRef]
- Rosen, R.C.; Riley, A.; Wagner, G.; Osterloh, I.H.; Kirkpatrick, J.; Mishra, A. The International Index of Erectile Function (IIEF): A Multidimensional Scale for Assessment of Erectile Dysfunction. Urology 1997, 49, 822–830. [Google Scholar] [CrossRef] [Green Version]
- Barry, M.J.; Fowler, F.J.; O’Leary, M.P.; Bruskewitz, R.C.; Holtgrewe, H.L.; Mebust, W.K.; Cockett, A.T.K. The Measurement Committee of the American Urological Association the American Urological Association Symptom Index for Benign Prostatic Hyperplasia. J. Urol. 1992, 148, 1549–1557. [Google Scholar] [CrossRef]
- Van der Kwast, T.H.; Roobol, M.J. Defining the Threshold for Significant versus Insignificant Prostate Cancer. Nat. Rev. Urol. 2013, 10, 473–482. [Google Scholar] [CrossRef] [PubMed]
- European Association of Urology (EAU) Guidelines. 2023. Available online: Https://Uroweb.Org/Guidelines (accessed on 20 March 2023).
- Cohen, J.K.; Miller, R.J.; Shuman, B.A. Urethral Warming Catheter for Use during Cryoablation of the Prostate. Urology 1995, 45, 861–864. [Google Scholar] [CrossRef]
- Alfarone, A.; Panebianco, V.; Schillaci, O.; Salciccia, S.; Cattarino, S.; Mariotti, G.; Gentilucci, A.; Von Heland, M.; Passariello, R.; Gentile, V.; et al. Comparative Analysis of Multiparametric Magnetic Resonance and PET-CT in the Management of Local Recurrence after Radical Prostatectomy for Prostate Cancer. Crit. Rev. Oncol. Hematol. 2012, 84, 109–121. [Google Scholar] [CrossRef]
- Sathianathen, N.J.; Omer, A.; Harriss, E.; Davies, L.; Kasivisvanathan, V.; Punwani, S.; Moore, C.M.; Kastner, C.; Barrett, T.; Van Den Bergh, R.C.; et al. Negative Predictive Value of Multiparametric Magnetic Resonance Imaging in the Detection of Clinically Significant Prostate Cancer in the Prostate Imaging Reporting and Data System Era: A Systematic Review and Meta-Analysis. Eur. Urol. 2020, 78, 402–414. [Google Scholar] [CrossRef] [PubMed]
- Panebianco, V.; Barchetti, G.; Simone, G.; Del Monte, M.; Ciardi, A.; Grompone, M.D.; Campa, R.; Indino, E.L.; Barchetti, F.; Sciarra, A.; et al. Negative Multiparametric Magnetic Resonance Imaging for Prostate Cancer: What’s Next? Eur. Urol. 2018, 74, 48–54. [Google Scholar] [CrossRef] [Green Version]
- van den Bos, W.; Muller, B.G.; Ahmed, H.; Bangma, C.H.; Barret, E.; Crouzet, S.; Eggener, S.E.; Gill, I.S.; Joniau, S.; Kovacs, G.; et al. Focal Therapy in Prostate Cancer: International Multidisciplinary Consensus on Trial Design. Eur. Urol. 2014, 65, 1078–1083. [Google Scholar] [CrossRef]
- Arcot, R.; Potts, B.A.; Polascik, T.J. Focal Cryoablation of Image-Localized Prostate Cancer. J. Endourol. 2021, 35, S17–S23. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.T.; Dunn, R.L.; Litwin, M.S.; Sandler, H.M.; Sanda, M.G. Development and Validation of the Expanded Prostate Cancer Index Composite (EPIC) for Comprehensive Assessment of Health-Related Quality of Life in Men with Prostate Cancer. Urology 2000, 56, 899–905. [Google Scholar] [CrossRef] [Green Version]
- Fütterer, J.J.; Briganti, A.; De Visschere, P.; Emberton, M.; Giannarini, G.; Kirkham, A.; Taneja, S.S.; Thoeny, H.; Villeirs, G.; Villers, A. Can Clinically Significant Prostate Cancer Be Detected with Multiparametric Magnetic Resonance Imaging? A Systematic Review of the Literature. Eur. Urol. 2015, 68, 1045–1053. [Google Scholar] [CrossRef] [PubMed]
- Mottet, N.; Bellmunt, J.; Bolla, M.; Briers, E.; Cumberbatch, M.G.; De Santis, M.; Fossati, N.; Gross, T.; Henry, A.M.; Joniau, S.; et al. EAU-ESTRO-SIOG Guidelines on Prostate Cancer. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2017, 71, 618–629. [Google Scholar] [CrossRef] [PubMed]
- Loeb, S.; Vellekoop, A.; Ahmed, H.U.; Catto, J.; Emberton, M.; Nam, R.; Rosario, D.J.; Scattoni, V.; Lotan, Y. Systematic Review of Complications of Prostate Biopsy. Eur. Urol. 2013, 64, 876–892. [Google Scholar] [CrossRef] [Green Version]
- Ukimura, O.; Marien, A.; Palmer, S.; Villers, A.; Aron, M.; de Castro Abreu, A.L.; Leslie, S.; Shoji, S.; Matsugasumi, T.; Gross, M.; et al. Trans-Rectal Ultrasound Visibility of Prostate Lesions Identified by Magnetic Resonance Imaging Increases Accuracy of Image-Fusion Targeted Biopsies. World J. Urol. 2015, 33, 1669–1676. [Google Scholar] [CrossRef] [PubMed]
- Kasivisvanathan, V.; Rannikko, A.S.; Borghi, M.; Panebianco, V.; Mynderse, L.A.; Vaarala, M.H.; Briganti, A.; Budäus, L.; Hellawell, G.; Hindley, R.G.; et al. MRI-Targeted or Standard Biopsy for Prostate-Cancer Diagnosis. N. Engl. J. Med. 2018, 378, 1767–1777. [Google Scholar] [CrossRef]
- McCulloch, P.; Altman, D.G.; Campbell, W.B.; Flum, D.R.; Glasziou, P.; Marshall, J.C.; Nicholl, J. No surgical innovation without evaluation: The IDEAL recommendations. Lancet 2009, 374, 1105–1112. [Google Scholar] [CrossRef]
- Palakkan, S.; Augestine, T.; Valsan, M.; Vahab, K.A.; Nair, L. Role of Frozen Section in Surgical Management of Ovarian Neoplasm. Gynecol. Minim. Invasive Ther. 2020, 9, 13. [Google Scholar] [CrossRef]
- Alcazar, J.L.; Dominguez-Piriz, J.; Juez, L.; Caparros, M.; Jurado, M. Intraoperative Gross Examination and Intraoperative Frozen Section in Patients with Endometrial Cancer for Detecting Deep Myometrial Invasion: A Systematic Review and Meta-Analysis. Int. J. Gynecol. Cancer 2016, 26, 407–415. [Google Scholar] [CrossRef]
- Dinneen, E.P.; Van Der Slot, M.; Adasonla, K.; Tan, J.; Grierson, J.; Haider, A.; Freeman, A.; Oakley, N.; Shaw, G. Intraoperative Frozen Section for Margin Evaluation During Radical Prostatectomy: A Systematic Review. Eur. Urol. Focus 2020, 6, 664–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez-Salas, R.; Desai, M. A Joint SIU-ICUD International Consultation Image-Guided Therapies for Prostate and Kidney Cancers. Available online: www.Siu-Urology.Org (accessed on 25 April 2023).
- van der Poel, H.; Klotz, L.; Andriole, G.; Azzouzi, A.-R.; Bjartell, A.; Cussenot, O.; Hamdy, F.; Graefen, M.; Palma, P.; Rivera, A.R.; et al. Role of Active Surveillance and Focal Therapy in Low- and Intermediate-Risk Prostate Cancers. World J. Urol. 2015, 33, 907–916. [Google Scholar] [CrossRef]
- Pushkarev, A.V.; Ryabikin, S.S.; Saakyan, N.Y.; Tsiganov, D.I.; Burkov, I.A.; Vasilev, A.O. A Study of Prostate Multiprobe Cryoablation near Urethra for Precision Treatment Planning. Cryobiology 2022, 109, 10–19. [Google Scholar] [CrossRef]
- Peters, I.; Derlin, K.; Peperhove, M.J.; Hensen, B.; Pertschy, S.; Wolters, M.; von Klot, C.-A.J.; Wacker, F.; Hellms, S. First Experiences and Results after Cryoablation of Prostate Cancer with Histopathological Evaluation and Imaging-Based Follow-Up. Future Oncol. Lond. Engl. 2022, 18, 1705–1716. [Google Scholar] [CrossRef]
- Ahmed, H.U.; Dickinson, L.; Charman, S.; Weir, S.; McCartan, N.; Hindley, R.G.; Freeman, A.; Kirkham, A.P.; Sahu, M.; Scott, R.; et al. Focal Ablation Targeted to the Index Lesion in Multifocal Localised Prostate Cancer: A Prospective Development Study. Eur. Urol. 2015, 68, 927–936. [Google Scholar] [CrossRef]
- Bossier, R.; Sanguedolce, F.; Territo, A.; Vanacore, D.; Martínez, C.; Regis, F.; Gallioli, A.; Mercade, A.; Mosquera, L.; Aumatell, J.; et al. Whole and Hemi-Gland Cryoablation for Primary Localized Prostate Cancer: Short and Medium-Term Oncological and Functional Outcomes. Actas Urol. Esp. 2020, 44, 172–178. [Google Scholar] [CrossRef]
- Mendez, M.H.; Passoni, N.M.; Pow-Sang, J.; Jones, J.S.; Polascik, T.J. Comparison of Outcomes Between Preoperatively Potent Men Treated with Focal Versus Whole Gland Cryotherapy in a Matched Population. J. Endourol. 2015, 29, 1193–1198. [Google Scholar] [CrossRef]
- Haffner, M.C.; Mosbruger, T.; Esopi, D.M.; Fedor, H.; Heaphy, C.M.; Walker, D.A.; Adejola, N.; Gürel, M.; Hicks, J.; Meeker, A.K.; et al. Tracking the Clonal Origin of Lethal Prostate Cancer. J. Clin. Invest. 2013, 123, 4918–4922. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hopstaken, J.S.; Bomers, J.G.R.; Sedelaar, M.J.P.; Valerio, M.; Fütterer, J.J.; Rovers, M.M. An Updated Systematic Review on Focal Therapy in Localized Prostate Cancer: What Has Changed over the Past 5 Years? Eur. Urol. 2022, 81, 5–33. [Google Scholar] [CrossRef] [PubMed]
- Manfredi, M.; Mele, F.; Garrou, D.; Walz, J.; Fütterer, J.J.; Russo, F.; Vassallo, L.; Villers, A.; Emberton, M.; Valerio, M. Multiparametric Prostate MRI: Technical Conduct, Standardized Report and Clinical Use. Minerva Urol. Nephrol. 2018, 70, 21–40. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Patient 1 | Patient 2 | Patient 3 |
|---|---|---|---|
| Age, y | 49 | 79 | 76 |
| PSA, ng/mL | 11.69 | 11.42 | 14.51 |
| Body mass index, kg/m2 | 26.7 | 24.6 | 28.3 |
| Digital rectal examination | Negative | Negative | Negative |
| MRI findings | PIRADS-5 | PIRADS-4 | PIRADS-4 |
| cT stage | cT3a | cT2b | cT2a |
| ASA score | 1 | 2 | 2 |
| Index lesion volume, cc | 17 | 25 | 16 |
| IIEF-5 score | 19 | 16 | 21 |
| I-PSS score | 4 | 10 | 12 |
| Characteristics | Patient 1 | Patient 2 | Patient 3 |
|---|---|---|---|
| PSA, ng/mL | 0.8 | 1.23 | 3.15 |
| Digital rectal examination | Negative | Negative | Negative |
| MRI findings | Negative | Negative | Negative |
| Continence, yes/no | Yes | Yes | Yes |
| IIEF-5 score | 21 | 16 | 18 |
| IPSS score | 5 | 12 | 9 |
| Characteristics | Patient 1 | Patient 2 | Patient 3 |
|---|---|---|---|
| PSA, ng/mL | 1.63 | 1.34 | 3.96 |
| Digital rectal examination | Negative | Negative | Negative |
| MRI findings | Negative | Negative | PIRADS-4 |
| Repeated biopsy | Negative | Negative | 4 + 3 |
| Continence, yes/no | Yes | Yes | Yes |
| IIEF-5 score | 20 | 18 | 16 |
| IPSS score | 4 | 11 | 10 |
| Characteristics | Patient 1 | Patient 2 | Patient 3 |
|---|---|---|---|
| PSA, ng/mL | 1.87 | 2.11 | 2.87 |
| Digital rectal examination | Negative | Negative | Negative |
| MRI findings | Negative | Negative | Negative |
| Continence, yes/no | Yes | Yes | Yes |
| IIEF-5 score | 19 | 15 | 15 |
| IPSS score | 7 | 13 | 9 |
| Characteristics | Patient 1 | Patient 2 | Patient 3 |
|---|---|---|---|
| PSA, ng/mL | 2.51 | 3.16 | 2.47 |
| Digital rectal examination | Negative | Negative | Negative |
| MRI findings | Negative | Negative | Negative |
| Continence, yes/no | Yes | Yes | Yes |
| IIEF-5 score | 18 | 15 | 12 |
| IPSS score | 8 | 14 | 6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Misuraca, L.; Lugnani, F.; Brassetti, A.; Cacciatore, L.; Tedesco, F.; Anceschi, U.; Bove, A.M.; D’Annunzio, S.; Ferriero, M.; Guaglianone, S.; et al. Single-Setting 3D MRI/US-Guided Frozen Sectioning and Cryoablation of the Index Lesion: Mid-Term Oncologic and Functional Outcomes from a Pilot Study. J. Pers. Med. 2023, 13, 978. https://doi.org/10.3390/jpm13060978
Misuraca L, Lugnani F, Brassetti A, Cacciatore L, Tedesco F, Anceschi U, Bove AM, D’Annunzio S, Ferriero M, Guaglianone S, et al. Single-Setting 3D MRI/US-Guided Frozen Sectioning and Cryoablation of the Index Lesion: Mid-Term Oncologic and Functional Outcomes from a Pilot Study. Journal of Personalized Medicine. 2023; 13(6):978. https://doi.org/10.3390/jpm13060978
Chicago/Turabian StyleMisuraca, Leonardo, Franco Lugnani, Aldo Brassetti, Loris Cacciatore, Francesco Tedesco, Umberto Anceschi, Alfredo Maria Bove, Simone D’Annunzio, Mariaconsiglia Ferriero, Salvatore Guaglianone, and et al. 2023. "Single-Setting 3D MRI/US-Guided Frozen Sectioning and Cryoablation of the Index Lesion: Mid-Term Oncologic and Functional Outcomes from a Pilot Study" Journal of Personalized Medicine 13, no. 6: 978. https://doi.org/10.3390/jpm13060978