3.1. Patients’ Demographics and Medical History
The patients’ demographics and medical history for both cases and controls are described in
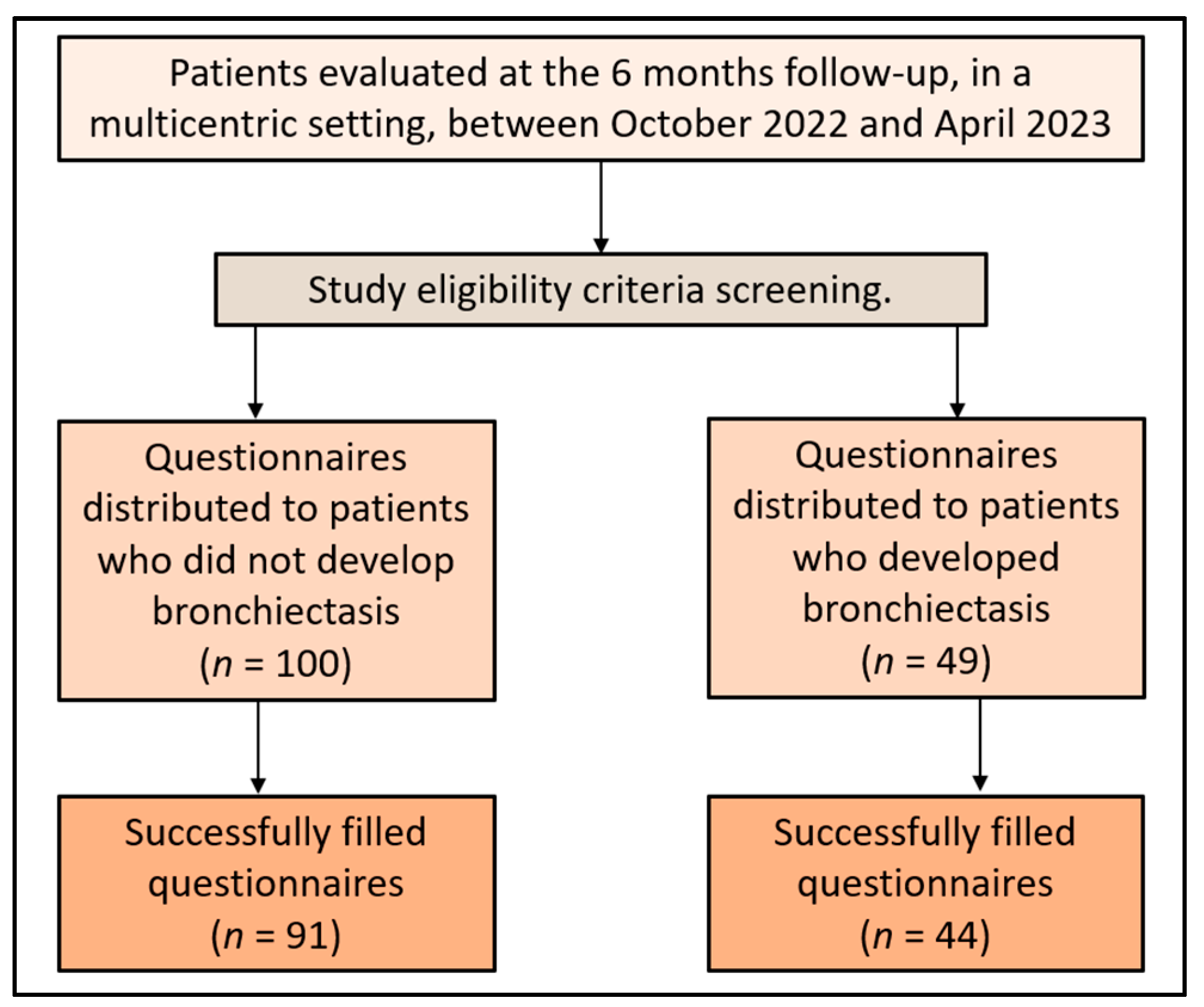
Table 1. There were 44 cases who developed bronchiectasis after lung resection and 91 controls who did not develop bronchiectasis postoperatively. The average age of the patients in the case group was 56.2 years old, while in the control group it was 55.6 years old (
p = 0.656), indicating a similar age distribution among both the groups. The gender distribution between the cases and controls did not differ significantly either, with 65.9% of the cases and 70.3% of the controls being men (
p = 0.603). The area of residence, whether urban or rural, was also comparable between the two groups (47.7% of cases and 46.2% of controls resided in urban areas,
p = 0.863).
Smoking status was assessed in both groups, with 38.6% of cases and 33.0% of controls identified as smokers (p = 0.516). Similarly, there was no significant difference in the median pack-year smoking history between the two groups (24.5 vs. 21.0, p = 0.219). In terms of exposure to respiratory hazards, 20.5% of the cases and 15.4% of the controls had such exposure in their history (p = 0.462). The prevalence of obesity was higher in cases (36.4%) than in controls (24.2%); however, this difference did not reach statistical significance (p = 0.139). Lastly, regarding the Charlson comorbidity index (CCI), 22.7% of the cases and 17.6% of the controls had a CCI higher than 3, indicating a high burden of comorbidity; however, this difference was not statistically significant.
3.3. Analysis of Unstandardized and Standardized Questionnaires
Table 3 displays the unstandardized questionnaire responses of the study cohort. Regarding the overall health status after the surgery, the mean score for the cases was 6.6, while for the controls, it was 7.8 (
p = 0.016), suggesting that patients who developed bronchiectasis after surgery rated their health status lower than those who did not. In relation to symptom improvement, a significantly higher percentage of cases (27.3%) reported the worsening of their respiratory symptoms post-surgery compared to the controls (12.1%,
p = 0.027). As for adherence to post-surgical care recommendations, 43.2% of cases reported compliance compared to 28.6% of the controls; however, this difference did not reach statistical significance.
When evaluating smoking status, a lower percentage of cases (15.9%) reported a decrease in smoking frequency compared to the controls (31.9%, p = 0.049), suggesting more controls reduced their smoking post-surgery. The level of physical activity decreased significantly more in cases (47.7%) than in controls (19.8%) post-surgery (p < 0.001). In terms of the post-operative complications, 22.7% of cases reported experiencing complications or unexpected health issues post-surgery compared to 14.3% of controls (p = 0.221). Patients who developed bronchiectasis rated their mental/emotional well-being significantly lower post-surgery (mean 7.0) than the controls (mean 8.1) (p = 0.040). Lastly, cases were slightly less satisfied with the follow-up care they received (mean 7.3) than controls (mean 7.9); although, the difference was not statistically significant.
Table 4 presents the analysis of the World Health Organization Quality of Life Questionnaire—Brief Version (WHOQOL-BREF) at the six-month follow-up point. In this analysis, lower scores denoted a more negative quality of life. In the physical domain, the mean score was significantly lower in cases (14.0) than in controls (15.9), with a
p-value of 0.043, implying that the cases reported a poorer physical quality of life than the controls. Similarly, the mean score in the mental domain was significantly lower for cases (11.5) compared to controls (13.0), with a
p-value of 0.044, indicating that those who developed bronchiectasis had a worse mental quality of life than those who did not develop the condition.
In the social domain, cases had a mean score of 10.2, which was significantly lower than the mean score for the controls (12.8), with a
p-value of 0.007, suggesting a more negatively impacted social quality of life in cases, as presented in
Figure 2. In contrast, in the environmental domain, the difference in the mean scores between cases (14.7) and controls (16.3) was not statistically significant, suggesting that there was no significant difference in environmental quality of life between the two groups.
Table 5 provides an analysis of the 36-Item Short Form Survey (SF-36) questionnaire at the six-month follow-up. The score for each domain of this survey was indirectly proportional to the degree of disability experienced by the patient. In the physical domain of the SF-36, the mean score was significantly lower for cases (51.0) than for controls (53.9. This suggests that patients who developed bronchiectasis after pulmonary resection experienced a higher degree of physical disability than those who did not develop bronchiectasis. The mean score in the mental domain was lower for cases (52.1) compared to controls (54.5); although, this difference did not reach statistical significance. This indicates that patients who developed bronchiectasis may have experienced a higher level of mental disability; however, the difference was not statistically significant. In terms of the total score, the mean for cases was 54.9 compared to 56.7 for controls, as presented in
Figure 3.
Table 6 presents the analysis of the Hospital Anxiety and Depression Scale (HADS) questionnaire at the six-month follow-up. HADS is a measure where higher scores indicate more severe symptoms of anxiety and depression. The mean anxiety score was significantly higher in cases (7.52) than in controls (6.15), with a
p-value of 0.037. This result suggests that patients who develop bronchiectasis after surgery experience more severe anxiety symptoms compared to patients who do not develop bronchiectasis.
In terms of depression, the mean score was higher in cases (6.94) than controls (6.00); however, this difference did not reach statistical significance. Although patients who developed bronchiectasis appeared to exhibit more severe depression symptoms, the difference was not statistically significant. The total HADS score, which sums the anxiety and depression scores, was significantly higher in cases (12.95) than in controls (10.36), with a
p-value of 0.015, as described in
Figure 4. This indicates that patients who develop bronchiectasis after surgery have a higher overall burden of anxiety and depression symptoms.
Table 7 reports the analysis of the Perceived Stress Scale (PSS-10) questionnaire at the six-month follow-up. The PSS-10 is a measure where higher scores indicate a greater degree of perceived stress. When it came to positive aspects of the questionnaire, the mean score for cases was 6.71, slightly higher than the control group with 6.08 (
p-value = 0.369). In contrast, the negative dimension of perceived stress was significantly higher in cases (6.48) compared to controls (4.92), with a
p-value of 0.013. This suggests that patients who develop bronchiectasis after surgery perceive their stress to be more negative than those who do not develop bronchiectasis. Moreover, the total PSS-10 score was significantly higher in cases (10.94) than controls (9.06), with a
p-value of 0.035, as can be observed in
Figure 5. This indicates that patients who develop bronchiectasis after surgery have a greater overall degree of perceived stress compared to those who do not develop bronchiectasis.
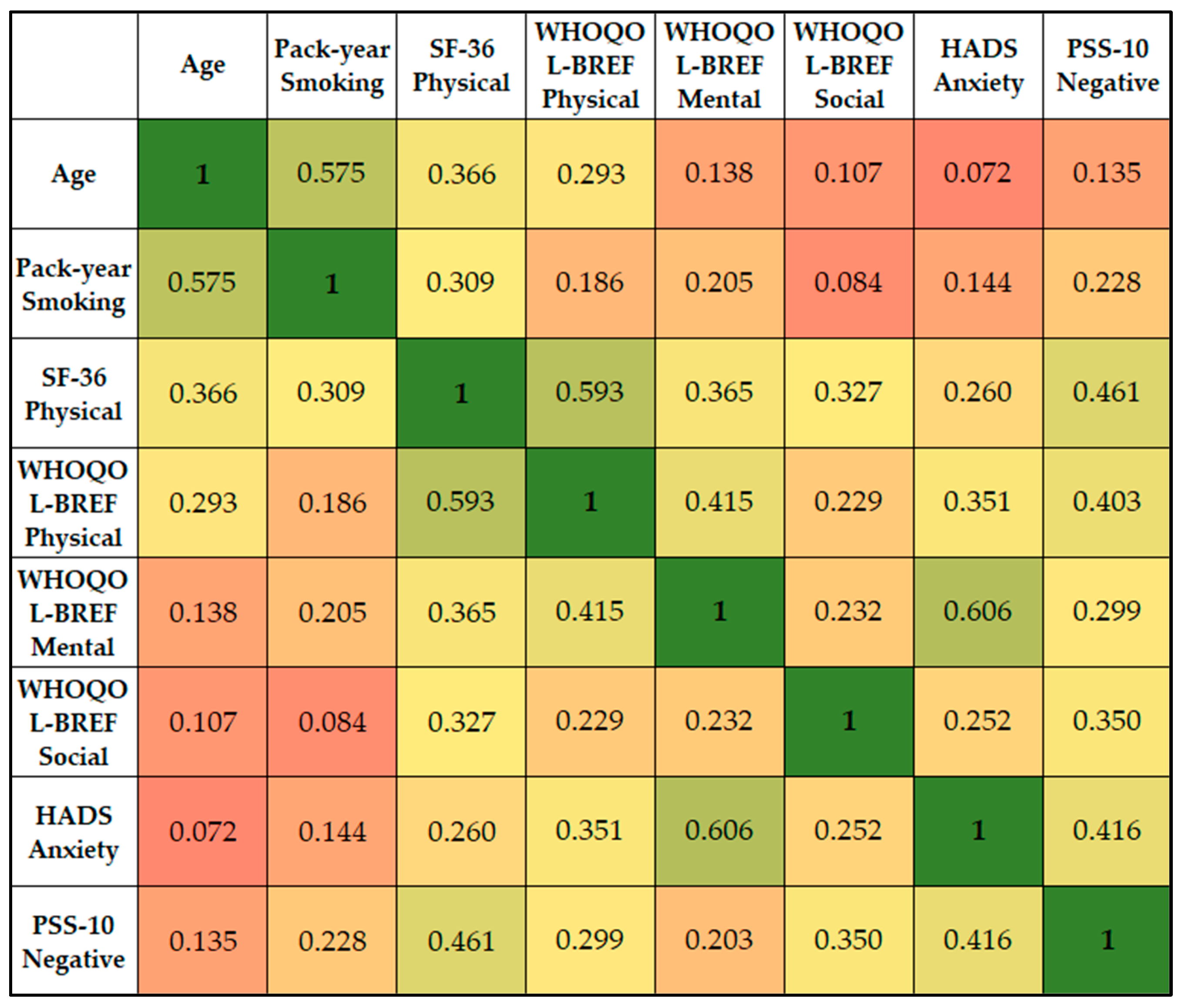
Age demonstrated a positive correlation with the SF-36 Physical (r = 0.366), suggesting that older patients tended to report better physical functioning. The SF-36 Physical score showed a strong positive correlation with the WHOQOL-BREF Physical score (r = 0.593), indicating that patients who scored higher on physical functioning also tended to report a better physical quality of life. It also had a significant correlation with the PSS-10 Negative score (r = 0.461), indicating that better physical functioning was associated with a higher degree of perceived negative stress.
The WHOQOL-BREF Physical score had a moderate correlation with HADS Anxiety (r = 0.351), indicating that a higher physical quality of life was associated with higher anxiety scores. The WHOQOL-BREF Mental score showed the strongest correlation with HADS Anxiety (r = 0.606), suggesting that greater mental/emotional well-being was associated with higher anxiety levels. The PSS-10 Negative score showed significant correlations with SF-36 Physical (r = 0.461), WHOQOL-BREF Physical (r = 0.403), WHOQOL-BREF Social (r = 0.350), and HADS Anxiety (r = 0.416), as presented in
Figure 6. This indicates that a higher degree of perceived negative stress is associated with better physical functioning, higher physical and social quality of life, and higher anxiety levels.





 ,
, 







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}