1. Introduction
Depression is a common mental disorder, with 5.0% of adults affected worldwide and 5.7% among the elderly [
1]. “Depression” references in scientific documents have increased exponentially since 1950, and documents mentioning “selective serotonin reuptake inhibitors (SSRIs)” have increased at a rate of approximately 41 per year in the past 40 years [
2], being the most common therapeutic class for its treatment in early ages [
3].
Fluoxetine is one of the SSRI-class antidepressants, with oral formulations ranging from 20 mg to 90 mg. Its metabolism is mainly performed in the liver by the highly polymorphic CYP2D6. The contribution from other CYPs, such as CYP2C19, CYP2C9, and CYP3A4, is relevant in subjects with chronic exposure to fluoxetine since the drug inhibits its metabolism [
4]. The pharmacogenomics of antidepressants is of interest given 48% therapeutic failures, 40% remission rate, and 25% frequency of adverse events [
3,
5]. Understanding the pharmacokinetic and pharmacodynamic genes’ contribution to SSRI function is currently an active research area, with above 900 studies reported [
3]. Some of these studies have found solid clinical evidence, enough to generate regulatory guidance for pharmacogenomic testing for treatment selection and dose adjustments, such as those of the Food and Drugs Administration (FDA) and European Medicines Agency (EMA).
International pharmacogenomics groups, such as the Clinical Pharmacogenetics Implementation Consortium (CPIC), have developed recommendations and calculator tools to predict the phenotype of actionable genes for CYP2D6 and CYP2C19, main cytochromes on the metabolism of antidepressants [
6,
7]. These tools, together with clinical evidence, allow clinicians to improve the therapeutics of antidepressants. Nevertheless, details and validation across different populations are advisable to strengthen the clinical evidence.
Bioequivalence trials can ensure quality to speed up the registration of generic medications by several regulatory agencies across the world, such as the FDA, EMA, and the Mexican regulatory agency, COFEPRIS [
8]. In these studies, pharmacokinetic (PK) profiles are evaluated between test and reference formulations to compare their bioavailability, i.e., to test whether the geometric ratios of the PK parameters are—unless otherwise stated—inside an 80–125% confidence interval. Since two-sequence two-period two-formulation crossover trials are the most convenient designs for bioequivalence evaluation, intrasubject (within-subject) variability is required to estimate a sufficient sample size for assessing the confidence intervals with targeted error and statistical power.
In the world, there are 394 protocols reported in clinicaltrials.gov with the active principle fluoxetine, ranging from phase 1 to 4, 12 of them PK or bioequivalence studies [
9]. In the Mexican National Registry of Clinical Trials (RNEC), there are 15 protocols registered with this drug [
10]. Of those, 13 are bioequivalence/comparative bioavailability studies, the 20 mg capsule formulation being the most frequently studied. These studies, overall, had a crossover two-sequence two-period design, with a sample size ranging from 24 to 36 subjects.
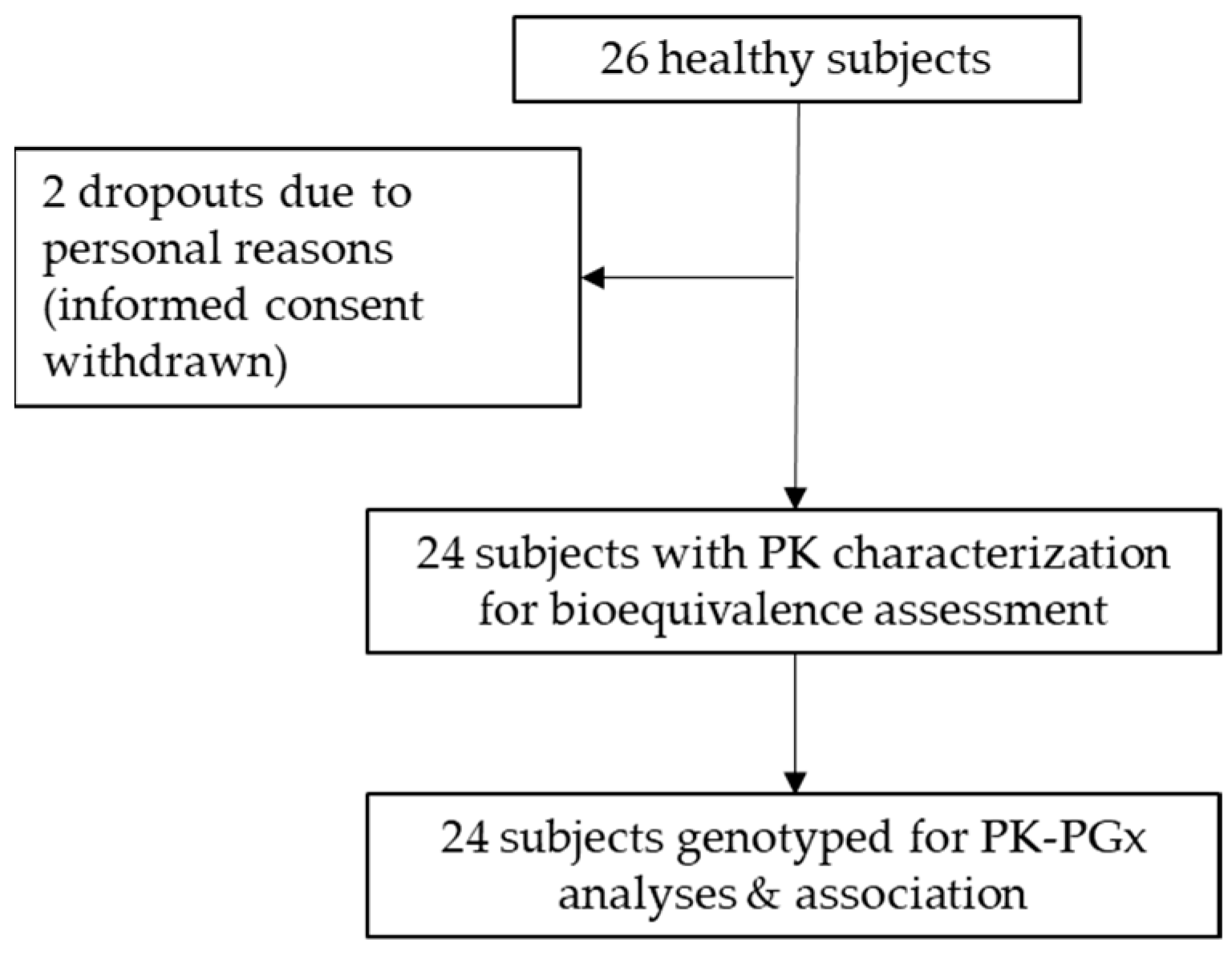
In this work, we report a clinical trial with fluoxetine 20 mg capsules performed in 24 healthy Mexican volunteers, where the pharmacokinetics was evaluated in a crossover randomized study, exploring relationships with the genotype of the participants. We aimed to test bioequivalence between two fluoxetine formulations, and to associate the genotype of participant subjects with the metabolizing phenotypes (pharmacokinetics) of fluoxetine, quantifying the potential impact of selected CYPs in the metabolism of fluoxetine. So, the bioequivalence evaluation was independent from the pharmacogenetic analyses performed for exploratory purposes.
2. Methods
2.1. Bioequivalence Clinical Trial
The clinical trial was a randomized controlled, open-label, crossover 2 × 2 (two-sequences, two-periods) design, with a single administration per period in fasting conditions in healthy subjects. Products administered were fluoxetine hydrochloride 20 mg capsules, Apotex, Inc. Toronto, ON, Canada (test product), and Prozac® 20, Eli Lilly and Company (reference product). Blood sampling was performed up to 72 h after drug administration, with an 8-week washout between periods.
The sample size for the bioequivalence trial was based on an expected intrasubject variation of 18% for fluoxetine PK parameters [
11], α of 0.05, and a power of 90% (β of 0.10), with 80–125% acceptance limits for the 90% confidence intervals, evaluated with Schuirmann’s two one-sided
t-tests (TOST), in compliance with standard bioequivalence analysis methodology and national regulation [
8,
12]. This calculation resulted in a minimum sample size of 22 + 4 subjects due to potential dropouts.
Inclusion criteria were age from 18 to 55 years, body mass index (BMI) between 18 and 27 kg/m2, and clinical examination and laboratory data within normal ranges. Exclusion criteria were pregnancy or lactation; history of alcoholism, drug abuse, or heavy smoking; documented hypersensitivity to the study drug or to any drug in the same therapeutic group; receiving any medication within less than 14 days (or 7 half-lives) of the study starting date; subjects who had donated blood or had more than 450 mL of blood withdrawn 60 days before the study starting; history or evidence of medical conditions including, but not limited to, gastrointestinal, renal, hepatic, cardiovascular, and endocrine diseases; and consumption of grapefruit juice and/or xanthine-containing beverages, such as coffee, tea, chocolate, cola soft drinks, etc., 10 h before the study start-up.
The study was conducted in a bioequivalence laboratory facility in Mexico City, Axis Clinicals Latina, authorized as a clinical and bioanalytical unit for bioavailability and bioequivalence studies according to national requirements [
8]. The clinical trial protocol was reviewed by an institutional review board (IRB) authorized by COFEPRIS and the National Commission of Bioethics (CONBIOETICA); then the protocol was submitted to the federal agency COFEPRIS for its approval.
All participant volunteers met the inclusion criteria and signed written informed consent. The study was conducted under NOM-177-SSA1-2013 [
8], Good Clinical Practices (GCPs) [
13], International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH) Guidelines [
14], and followed the statutes of the Declaration of Helsinki and its amendments [
15].
2.2. Plasma Fluoxetine Determination
The blood samples were collected in sodium heparin tubes at 0.0, 1.0, 2.0, 3.0, 4.0, 5.0, 6.0, 7.0, 8.0, 9.0, 10.0, 12.0, 24.0, 48.0, and 72.0 h post-dose. Once collected, samples were centrifuged at 3500 rpm for 10 min between 2 and 15 °C to separate plasma. Plasma was pipetted into labeled cryogenic tubes for fluoxetine determination. Liquid–liquid extraction and high-performance liquid chromatography coupled to mass/mass spectrometry (LC-MS/MS) with reverse phase column (Gemini, C18, 50 × 4.6 mm, 5 µm) was performed for fluoxetine quantification. Chromatographic conditions were 3 min run at 35 °C, with acetonitrile/ammonium formate 2 mM pH 3.5 (90:10 v/v) mobile phase, in turbo-electro spray ionization (ESI+) positive mode with multiple reaction monitoring (MRM), using paroxetine as internal standard.
2.3. Genetic and Pharmacogenomic Analyses
These analyses were funded and performed at the National Institute for Genomic Medicine (INMEGEN), with microarrays purchased from Código 46. The white blood cells’ buffy coat was pooled into a cryotube for DNA extraction for each subject, using Puregene blood kit (QIAGEN
®), from 3 to 4 blood samples collected for PK to avoid low concentration of genetic material or poor quality. Quantity and quality were verified with spectrophotometry and agarose gel electrophoresis. Genotyping was performed using the Infinium
® Global Screening Array (GSA) 24 v1.0 microarray, including 600,000 variants with more than 22,000 customized clinically relevant genetic variants related to drug response [
16].
2.4. Pharmacokinetics and Statistical Analysis
After fluoxetine determination, the formulation administered in each period for each subject was decoded according to the study randomization. Blood sampling actual times were calculated based on time deviations reported to the planned nominal sampling times. Observed plasma profiles vs. actual times were plotted and their PK parameters were calculated using non-compartmental analysis (NCA) in Phoenix
® WinNonlin
® version 8.1 [
17]. PK parameters included maximum drug concentration (C
max), time to C
max (t
max), area under the curve from pre-dose to last sampling time (AUC
0–t), AUC from pre-dose extrapolated to infinite (AUC
0–∞), elimination parameters such as elimination constant (K
el), half-life time (t
1/2), and apparent distribution volume (Vd).
Statistical analysis for bioequivalence assessment was performed using Schuirmann’s two one-sided
t-test (TOST) for test/reference geometric means ratios of C
max and AUC, applying the conventional acceptance criteria of 80–125% [
12]. Its 90% confidence intervals were calculated following NOM-177-SSA1-2013 regulation. Outlier analysis was performed to identify subjects with extreme values, based on the studentized intrasubject residuals using bear package, BE/BA for R [
18]. Analysis of variance (ANOVA) with a general linear model (GLM) for bioequivalence crossover studies was performed [
12] to evaluate period, sequence, and formulation effects.
2.5. Genotyping and Genotype-Phenotype Association
The pharmacogenetic analyses were performed for scientific research purposes, since bioequivalence was assessed for all the subjects who completed the clinical study, as described in the previous section in accordance with the national regulation [
8]. Analysis of the genomic data was carried out with Illumina
® GenomeStudio 2.0 software, performing quality control, normalization, and allelic discrimination of the variants of the 24 volunteers who concluded the bioequivalence study. Individual fluoxetine PK parameters were used as phenotypic variables. Multivariate association models were generated from data in plain text files with genetic information (.map and .ped), demographic variables (gender, age, weight, height, and BMI), and PK data (C
max, AUC
0–t, AUC
0–∞, t
max, t
1/2), using gPLINK vs2.050. Supporting analyses were performed with IBM SPSS
® 25 [
19] and Phoenix
® WinNonlin
® v.8.1, for the identification of the relevant genetic variants and their association with fluoxetine PK [
20,
21].
4. Discussion
Despite having better therapeutic efficacy than first-generation and other third-generation antidepressants, the clinical response to fluoxetine is still highly variable, with 10.6% of patients discontinuing treatment for major depressive disorder due to a lack of therapeutic efficacy [
28]. Because of that, pharmacological research on fluoxetine is relevant since the lack of therapeutic efficacy could derive from pharmacokinetic causes. Fluoxetine exhibits high intersubject PK variability, as confirmed in our study. Also, the exploration of different ethnicities is important for a better understanding of the pharmacogenomics of antidepressants, assessing both their pharmacokinetics and efficacy [
29,
30,
31].
In this bioequivalence study in a Mexican sample, fluoxetine t
1/2 was calculated as 30.7 h and 31.3 h for the test and reference formulations, respectively. These values are lower than those reported in the international literature for the drug, ranging between 4 and 6 days [
32]. Nevertheless, our obtained values match with those reported for extensive metabolizers [
33]. Maximum t
1/2 values in our study sample were 88.9 and 106.9 h (3.7 and 4.5 days), corresponding to a subject with poor CYP2D6 metabolizer phenotype. Mean t
max was found around 1 h before the reported value, confirming a high proportion of extensive metabolizers in the sample studied, which has also been found by other researchers in the Mexican population [
34].
Bioequivalence was concluded between test and reference formulations of fluoxetine 20 mg capsules with a 2 × 2 crossover design, in which each subject serves as its own control. Maximum intrasubject variability was 14.4% for C
max, so the sample size of 24 subjects was enough to achieve the minimum acceptable statistical power of 80%. Nevertheless, intersubject variability was high, up to 57.1% for AUC
0–∞, which is also well known [
35]. It has been previously reported that drugs mainly metabolized by CYP3A4 tend to have higher intrasubject PK variability, while drugs primarily metabolized by CYP2D6 show high intersubject variability in general [
36], which is confirmed for fluoxetine in this study.
The quantitative impact of CYP variants is reported in this study.
CYP2D6 rs28371703 had the greatest impact on the PK parameters of fluoxetine in the regression models. One subject with homozygote allele A/A for SNV rs1065852, associated with decreased CYP2D6 function, was found in our study sample, and we confirmed that the plasmatic t
1/2 increased about three times compared with A/G and G/G alleles. This SNV frequency in our study (
1/
24 = 4.2%) is consistent with reports in the literature, ranging from 2.8% and up to 4.3% in Caucasian, Hispanic, and Afro-American populations [
37]. Together with
CYP2D6 rs11358490, this SNV is part of the
CYP2D6*10 haplotype [
7], known to have decreased cytochrome function along with other gene variants [
38]. Moreover, a phenotype–genotype relationship was identified for three
CYP2D6 variants, confirming the relevance of this cytochrome in fluoxetine metabolism. CYP2C19 activity was found to be associated with differential exposure to the drug based on the genotype, as well as CYPs
1A2,
2C9, and
3A4, confirming previous findings [
39]. Six
CYP2B6 SNVs were found relevant in fluoxetine metabolism. CYP2B6 is also known to participate in antidepressant metabolism [
40], so attention should be also pointed to this cytochrome when administering SSRI, as recently discussed in CPIC guidelines [
41].
In this study, we identified 34 significant gene variants on 10 genes with quantifiable relevance in the pharmacokinetics of fluoxetine, with a candidate gene approach. Out of those, 29 SNVs belong to 7 CYPs (
CYP1A2,
CYP2B6,
CYP2C9,
CYP2C19,
CYP2D6,
CYP3A4, and
CYP3A5), and 5 SNVs to 3 pharmacodynamics (PD)- and efficacy-related genes (
SLC6A4,
TPH1,
ABCB1). These three genes encoding for the serotonin transporter 1,
p-glycoprotein 1, and L-tryptophan hydroxylase 1, respectively, are directly involved in the PD of fluoxetine. These have been researched thoroughly in the past [
42], aiming for a better understanding of the efficacy of antidepressants from the PD perspective. Even though they seem important in fluoxetine PK, the role of PK-related proteins in drug PD is multifactorial, and medication response still cannot be associated purely with single gene variations, as has been explored and evidenced in similar studies for other therapeutic classes [
43].
Regarding the limitations of this study, it is important to note that the sample size required for bioequivalence studies is considerably smaller than that required for pharmacogenetic studies, so we recommend more research into pharmacogenetics in pharmacokinetic studies, considering pharmacogenetics as an exploratory objective. Also, further evidence should be gathered to confirm the differences in fluoxetine PK between genders, as the number of females in this study was considerably lower than males. Finally, this study was conducted in healthy volunteers to explore fluoxetine PK, without the intention of evaluating its efficacy.
With this clinical study with fluoxetine hydrochloride, we confirm that through genotyping participating subjects in bioequivalence studies, the drug exposure can be assessed, and significant reduction of the intersubject variability can be achieved in clinical trials. The latter was evidenced despite the limitation of the sample size for the pharmacogenetic analyses within the context of a bioequivalence study for determining interchangeability between two fluoxetine formulations.


 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}