
Pancreatic Adenocarcinoma: Real World Evidence of Care Delivery in AccessHope Data

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Case Identification
2.2. Case Review
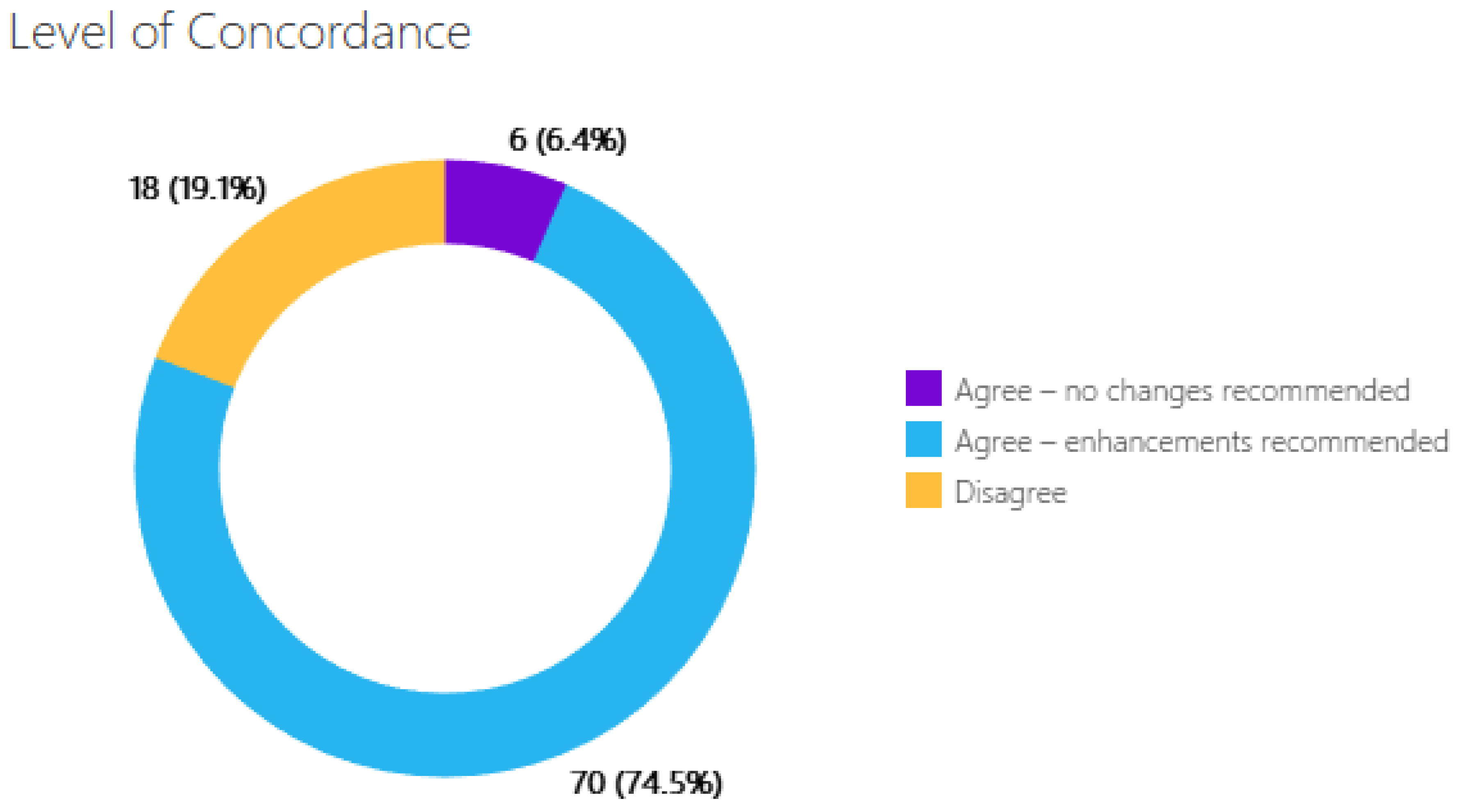
2.3. Case Evaluation
- Complete agreement with the care that is planned and delivered, labeled as “Agree”.
- Disagreement with the ongoing or planned cancer-directed care, with provision for recommendations for evidence-based care that confers safer and/or more effective and timely management, labeled as “Disagree”.
- Agreement with the overall cancer-directed therapy, yet with provision for recommendations for additional evaluation and/or interventions that would make care more efficient, patient-centered, and equitable. These cases are labeled as “Agree, with care enhancements”.
- Cancer-directed therapy;
- Improved member well-being;
- Benefit to family due to germline testing;
- Recommendations for relevant clinical trials.
3. Results
3.1. Case Characteristics
3.2. Case Evaluations
3.3. Gaps in Care by Stage
3.4. Differences between Academia vs. Community
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Luo, G.; Fan, Z.; Gong, Y.; Jin, K.; Yang, C.; Cheng, H.; Huang, D.; Ni, Q.; Liu, C.; Yu, X. Characteristics and Outcomes of Pancreatic Cancer by Histological Subtypes. Pancreas 2019, 48, 817–822. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Rawla, P.; Sunkara, T.; Gaduputi, V. Epidemiology of Pancreatic Cancer: Global Trends, Etiology and Risk Factors. World J. Oncol. 2019, 10, 10–27. [Google Scholar] [CrossRef] [PubMed]
- Jaap, K.; Fluck, M.B.; Dove, J.T.; Hunsinger, M.A.; Arora, T.K.; Shabahang, M.; Blansfield, J.A. Quality assessment in pancreatic cancer care: A review of the National Cancer Database. J. Am. Coll. Surg. 2015, 221, e103. [Google Scholar] [CrossRef]
- Wolfson, J.A.; Sun, C.L.; Wyatt, L.P.; Hurria, A.; Bhatia, S. Impact of care at comprehensive cancer centers on outcome: Results from a population-based study. Cancer 2015, 121, 3885–3893. [Google Scholar] [CrossRef]
- Pfister, D.G.; Rubin, D.M.; Elkin, E.B.; Neill, U.S.; Duck, E.; Radzyner, M.; Bach, P.B. Risk Adjusting Survival Outcomes in Hospitals That Treat Patients with Cancer without Information on Cancer Stage. JAMA Oncol. 2015, 1, 1303–1310. [Google Scholar] [CrossRef]
- McCulloch, P.; Altman, D.G.; Campbell, W.B.; Flum, D.R.; Glasziou, P.; Marshall, J.C.; Nicholl, J.; Balliol, C.; Aronson, J.K.; Barkun, J.S.; et al. No surgical innovation without evaluation: The IDEAL recommendations. Lancet 2009, 374, 1105–1112. [Google Scholar] [CrossRef]
- Fecso, A.B.; Szasz, P.; Kerezov, G.; Grantcharov, T.P. The Effect of Technical Performance on Patient Outcomes in Surgery: A Systematic Review. Ann. Surg. 2017, 265, 492–501. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; Kay, N.E.; Rabe, K.G.; Inwards, D.J.; Zent, C.S.; Leis, J.F.; Schwager, S.M.; Thompson, C.A.; Bowen, D.A.; Witzig, T.E.; et al. Hematologist/oncologist disease-specific expertise and survival: Lessons from chronic lymphocytic leukemia (CLL)/small lymphocytic lymphoma (SLL). Cancer 2012, 118, 1827–1837. [Google Scholar] [CrossRef]
- Varon, M.L.; Baker, E.; Byers, E.; Cirolia, L.; Bogler, O.; Bouchonville, M.; Schmeler, K.; Hariprasad, R.; Pramesh, C.S.; Arora, S. Project ECHO Cancer Initiative: A Tool to Improve Care and Increase Capacity Along the Continuum of Cancer Care. J. Cancer Educ. 2021, 36, 25–38. [Google Scholar] [CrossRef]
- West, H.J.; Tan, Y.A.; Barzi, A.; Wong, D.; Parsley, R.; Sachs, T. Novel Program Offering Remote, Asynchronous Subspecialist Input in Thoracic Oncology: Early Experience and Insights Gained During the COVID-19 Pandemic. JCO Oncol. Pract. 2022, 18, e537–e550. [Google Scholar] [CrossRef]
- Bilimoria, K.Y.; Bentrem, D.J.; Lillemoe, K.D.; Talamonti, M.S.; Ko, C.Y.; on behalf of the American College of Surgeons’ Pancreatic Cancer Quality Indicator Development Expert Panel. Assessment of pancreatic cancer care in the United States based on formally developed quality indicators. J. Natl. Cancer Inst. 2009, 101, 848–859. [Google Scholar] [CrossRef] [PubMed]
- Six Domains of Health Care Quality. Available online: https://www.ahrq.gov/talkingquality/measures/six-domains.html (accessed on 29 November 2022).
- Institute of Medicine Committee on Quality of Health Care in, A. Crossing the Quality Chasm: A New Health System for the 21st Century; National Academies Press: Washington, DC, USA, 2001. [Google Scholar]
- Annual Report to the Nation: Cancer Deaths Continue Downward Trend; Modest Improvements in Survival for Pancreatic Cancer. Available online: https://www.cdc.gov/media/releases/2022/p1027-annual-cancer-report.html (accessed on 25 November 2022).
- Chung, V.; Sun, V.; Ruel, N.; Smith, T.J.; Ferrell, B.R. Improving Palliative Care and Quality of Life in Pancreatic Cancer Patients. J. Palliat. Med. 2022, 25, 720–727. [Google Scholar] [CrossRef] [PubMed]
- Hillen, M.A.; Medendorp, N.M.; Daams, J.G.; Smets, E.M.A. Patient-Driven Second Opinions in Oncology: A Systematic Review. Oncologist 2017, 22, 1197–1211. [Google Scholar] [CrossRef] [PubMed]
- Olver, I.; Carey, M.; Bryant, J.; Boyes, A.; Evans, T.; Sanson-Fisher, R. Second opinions in medical oncology. BMC Palliat. Care 2020, 19, 112. [Google Scholar] [CrossRef] [PubMed]
- Loeb, S.; Li, R.; Sanchez Nolasco, T.; Byrne, N.; Cheng, H.H.; Becker, D.; Leader, A.E.; Giri, V.N. Barriers and facilitators of germline genetic evaluation for prostate cancer. Prostate 2021, 81, 754–764. [Google Scholar] [CrossRef]
- Bokkers, K.; Vlaming, M.; Engelhardt, E.G.; Zweemer, R.P.; van Oort, I.M.; Kiemeney, L.; Bleiker, E.M.A.; Ausems, M. The Feasibility of Implementing Mainstream Germline Genetic Testing in Routine Cancer Care—A Systematic Review. Cancers 2022, 14, 1059. [Google Scholar] [CrossRef]
- Sawhney, M.S.; Calderwood, A.H.; Thosani, N.C.; Rebbeck, T.R.; Wani, S.; Canto, M.I.; Fishman, D.S.; Golan, T.; Hidalgo, M.; Kwon, R.S.; et al. ASGE guideline on screening for pancreatic cancer in individuals with genetic susceptibility: Summary and recommendations. Gastrointest. Endosc. 2022, 95, 817–826. [Google Scholar] [CrossRef] [PubMed]
- Chittenden, A.; Haraldsdottir, S.; Ukaegbu, C.; Underhill-Blazey, M.; Gaonkar, S.; Uno, H.; Brais, L.K.; Perez, K.; Wolpin, B.M.; Syngal, S.; et al. Implementing Systematic Genetic Counseling and Multigene Germline Testing for Individuals with Pancreatic Cancer. JCO Oncol. Pract. 2021, 17, e236–e247. [Google Scholar] [CrossRef]
- Esplin, E.D.; Nielsen, S.M.; Bristow, S.L.; Garber, J.E.; Hampel, H.; Rana, H.Q.; Samadder, N.J.; Shore, N.D.; Nussbaum, R.L. Universal Germline Genetic Testing for Hereditary Cancer Syndromes in Patients with Solid Tumor Cancer. JCO Precis. Oncol. 2022, 6, e2100516. [Google Scholar] [CrossRef] [PubMed]
- Moffat, G.T.; Epstein, A.S.; O’Reilly, E.M. Pancreatic cancer—A disease in need: Optimizing and integrating supportive care. Cancer 2019, 125, 3927–3935. [Google Scholar] [CrossRef] [PubMed]
- Hussain, T.; Chang, H.Y.; Veenstra, C.M.; Pollack, C.E. Fragmentation in specialist care and stage III colon cancer. Cancer 2015, 121, 3316–3324. [Google Scholar] [CrossRef] [PubMed]
- Hester, C.A.; Karbhari, N.; Rich, N.E.; Augustine, M.; Mansour, J.C.; Polanco, P.M.; Porembka, M.R.; Wang, S.C.; Zeh, H.J., 3rd; Singal, A.G.; et al. Effect of fragmentation of cancer care on treatment use and survival in hepatocellular carcinoma. Cancer 2019, 125, 3428–3436. [Google Scholar] [CrossRef] [PubMed]
- Isaji, S.; Mizuno, S.; Windsor, J.A.; Bassi, C.; Fernandez-Del Castillo, C.; Hackert, T.; Hayasaki, A.; Katz, M.H.G.; Kim, S.W.; Kishiwada, M.; et al. International consensus on definition and criteria of borderline resectable pancreatic ductal adenocarcinoma 2017. Pancreatology 2018, 18, 2–11. [Google Scholar] [CrossRef]
- Gilbert, J.W.; Wolpin, B.; Clancy, T.; Wang, J.; Mamon, H.; Shinagare, A.B.; Jagannathan, J.; Rosenthal, M. Borderline resectable pancreatic cancer: Conceptual evolution and current approach to image-based classification. Ann. Oncol. 2017, 28, 2067–2076. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.B.; Lee, S.S.; Kim, J.H.; Kim, H.J.; Byun, J.H.; Hong, S.M.; Song, K.B.; Kim, S.C. Pancreatic Cancer CT: Prediction of Resectability according to NCCN Criteria. Radiology 2018, 289, 710–718. [Google Scholar] [CrossRef]
- Bratlie, S.O.; Biörserud, C.; Björnsson, B.; Bringeland, E.; Elander, N.; Grønbech, J.E.; Haux, J.; Hemmingsson, O.; Nymo, L.; Pfeiffer, P.; et al. Short-course neoadjuvant FOLFIRINOX versus upfront surgery for resectable pancreatic head cancer: A multicenter randomized phase-II trial (NORPACT-1). J. Clin. Oncol. 2023, 41, LBA4005. [Google Scholar] [CrossRef]
- Sohal, D.P.S.; Duong, M.; Ahmad, S.A.; Gandhi, N.S.; Beg, M.S.; Wang-Gillam, A.; Wade, J.L., 3rd; Chiorean, E.G.; Guthrie, K.A.; Lowy, A.M.; et al. Efficacy of Perioperative Chemotherapy for Resectable Pancreatic Adenocarcinoma: A Phase 2 Randomized Clinical Trial. JAMA Oncol. 2021, 7, 421–427. [Google Scholar] [CrossRef]
- Zengerling, F.; Hartmann, M.; Heidenreich, A.; Krege, S.; Albers, P.; Karl, A.; Weissbach, L.; Wagner, W.; Bedke, J.; Retz, M.; et al. German second-opinion network for testicular cancer: Sealing the leaky pipe between evidence and clinical practice. Oncol. Rep. 2014, 31, 2477–2481. [Google Scholar] [CrossRef]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouche, O.; Guimbaud, R.; Becouarn, Y.; Adenis, A.; Raoul, J.L.; Gourgou-Bourgade, S.; de la Fouchardiere, C.; et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef]
- Conroy, T.; Hammel, P.; Hebbar, M.; Ben Abdelghani, M.; Wei, A.C.; Raoul, J.L.; Chone, L.; Francois, E.; Artru, P.; Biagi, J.J.; et al. FOLFIRINOX or Gemcitabine as Adjuvant Therapy for Pancreatic Cancer. N. Engl. J. Med. 2018, 379, 2395–2406. [Google Scholar] [CrossRef] [PubMed]
- QOPI Certification Program. Available online: https://practice.asco.org/quality-improvement/quality-programs/qopi-certification-program (accessed on 27 March 2023).



{kind=link}
{kind=link}
| Clinical Case Characteristics of the Cohort | |
|---|---|
| Age, Median (range) | 58 years (38–81) |
| Gender, Male (%) | 55% |
| Stage, Metastatic (%) | 63% |
| Treating Physician, Academic (%) | 34% |
| Germline Testing | Somatic Testing | Supportive Care Integration | ||||
|---|---|---|---|---|---|---|
| Academic | Community | Academic | Community | Academic | Community | |
| Missing | 13 (41%) | 25 (40%) | 8 (39%) | 12 (28%) | 24 (75%) | 52 (84%) |
| Completed | 19 (59%) | 37 (60%) | 14 (64%) | 31 (72%) | 8 (25%) | 10 (16%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barzi, A.; Kim, A.J.; Liang, C.K.; West, H.; Wong, D.; Wright, C.; Nathwani, N.; Vasko, C.M.; Chung, V.; Rubinson, D.A.; et al. Pancreatic Adenocarcinoma: Real World Evidence of Care Delivery in AccessHope Data. J. Pers. Med. 2023, 13, 1377. https://doi.org/10.3390/jpm13091377
Barzi A, Kim AJ, Liang CK, West H, Wong D, Wright C, Nathwani N, Vasko CM, Chung V, Rubinson DA, et al. Pancreatic Adenocarcinoma: Real World Evidence of Care Delivery in AccessHope Data. Journal of Personalized Medicine. 2023; 13(9):1377. https://doi.org/10.3390/jpm13091377
Chicago/Turabian StyleBarzi, Afsaneh, Angela J. Kim, Crystal K. Liang, Howard West, D. Wong, Carol Wright, Nitya Nathwani, Catherine M. Vasko, Vincent Chung, Douglas A. Rubinson, and et al. 2023. "Pancreatic Adenocarcinoma: Real World Evidence of Care Delivery in AccessHope Data" Journal of Personalized Medicine 13, no. 9: 1377. https://doi.org/10.3390/jpm13091377
APA StyleBarzi, A., Kim, A. J., Liang, C. K., West, H., Wong, D., Wright, C., Nathwani, N., Vasko, C. M., Chung, V., Rubinson, D. A., & Sachs, T. (2023). Pancreatic Adenocarcinoma: Real World Evidence of Care Delivery in AccessHope Data. Journal of Personalized Medicine, 13(9), 1377. https://doi.org/10.3390/jpm13091377