
Prognostic Significance of CD11b-, CD8-, and CD163-Positive Tumor-Infiltrating Immune Cells in Distal Bile Duct Cancer

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Immunohistochemistry
2.3. Analysis of Tumor-Infiltrating Immune Cells According to CD11b, CD8, and CD163 Expression
2.4. Statistical Analyses
3. Results
3.1. Clinicopathologic Characteristics
3.2. Correlation of CD11b+, CD8+, and CD163+ TIICs with Clinicopathologic Characteristics
3.3. Survival Effects with Respect to CD11b+, CD8+, and CD163+ TIICs
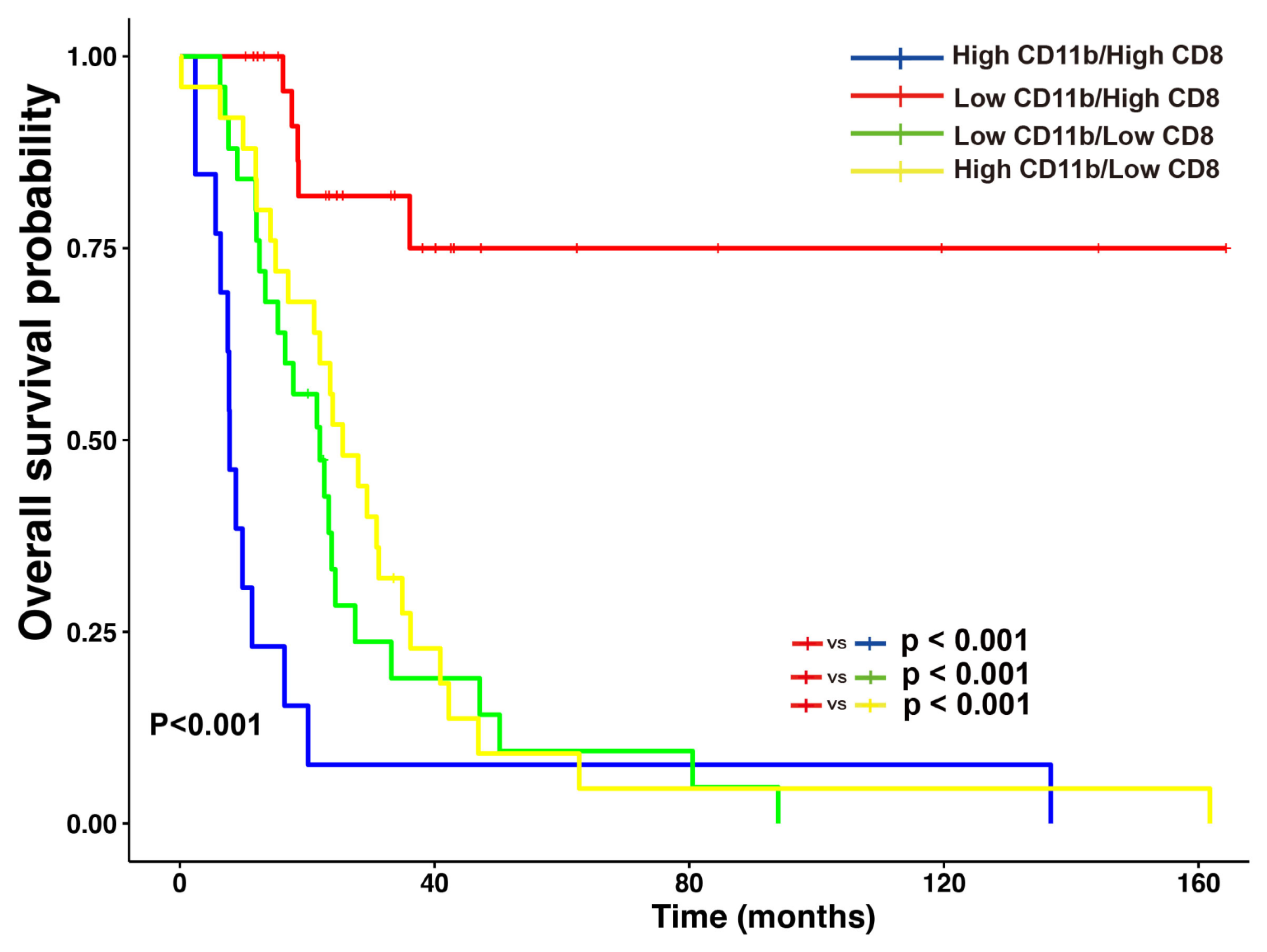
3.4. Clinicopathologic Features and Survival Effects with Respect to Concomitant Low CD11b+ and High CD8+ TIICs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| TICC | Tumor-infiltrating immune cells |
| TIM | Tumor-infiltrating myeloid cell |
| TAM | Tumor-infiltrating macrophages |
| TIL | Tumor-infiltrating lymphocytes |
| OS | Overall survival |
| TMA | Tissue microarray |
| pT | The pathologic primary tumor stage |
| pN | The pathologic regional lymph node stage |
References
- Razumilava, N.; Gores, G.J. Cholangiocarcinoma. Lancet 2014, 383, 2168–2179. [Google Scholar] [CrossRef] [PubMed]
- Brindley, P.J.; Bachini, M.; Ilyas, S.I.; Khan, S.A.; Loukas, A.; Sirica, A.E.; Teh, B.T.; Wongkham, S.; Gores, G.J. Cholangiocarcinoma. Nat. Rev. Dis. Primers 2021, 7, 65. [Google Scholar] [CrossRef]
- Zhou, Y.; Liu, S.; Wu, L.; Wan, T. Survival after surgical resection of distal cholangiocarcinoma: A systematic review and meta-analysis of prognostic factors. Asian J. Surg. 2017, 40, 129–138. [Google Scholar] [CrossRef]
- Jang, J.-Y.; Kim, S.-W.; Park, D.J.; Ahn, Y.J.; Yoon, Y.-S.; Choi, M.G.; Suh, K.-S.; Lee, K.U.; Park, Y.-H. Actual Long-term Outcome of Extrahepatic Bile Duct Cancer After Surgical Resection. Ann. Surg. 2005, 241, 77–84. [Google Scholar] [CrossRef]
- Zugman, M.; Botrus, G.; Pestana, R.C.; Uson Junior, P.L.S. Precision Medicine Targeting FGFR2 Genomic Alterations in Advanced Cholangiocarcinoma: Current State and Future Perspectives. Front. Oncol. 2022, 12, 860453. [Google Scholar] [CrossRef] [PubMed]
- Wheless, M.; Agarwal, R.; Goff, L.; Lockney, N.; Padmanabhan, C.; Heumann, T. Current Standards, Multidisciplinary Approaches, and Future Directions in the Management of Extrahepatic Cholangiocarcinoma. Curr. Treat. Options Oncol. 2024, 25, 127–160. [Google Scholar] [CrossRef]
- Cohen, E.E.W.; Bell, R.B.; Bifulco, C.B.; Burtness, B.; Gillison, M.L.; Harrington, K.J.; Le, Q.T.; Lee, N.Y.; Leidner, R.; Lewis, R.L.; et al. The Society for Immunotherapy of Cancer consensus statement on immunotherapy for the treatment of squamous cell carcinoma of the head and neck (HNSCC). J. ImmunoTherapy Cancer 2019, 7, 184. [Google Scholar] [CrossRef]
- Ralli, M.; Botticelli, A.; Visconti, I.C.; Angeletti, D.; Fiore, M.; Marchetti, P.; Lambiase, A.; de Vincentiis, M.; Greco, A. Immunotherapy in the Treatment of Metastatic Melanoma: Current Knowledge and Future Directions. J. Immunol. Res. 2020, 2020, 9235638. [Google Scholar] [CrossRef]
- U Gandhy, S.; Madan, R.A.; Aragon-Ching, J.B. The immunotherapy revolution in genitourinary malignancies. Immunotherapy 2020, 12, 819–831. [Google Scholar] [CrossRef] [PubMed]
- Lahiri, A.; Maji, A.; Potdar, P.D.; Singh, N.; Parikh, P.; Bisht, B.; Mukherjee, A.; Paul, M.K. Lung cancer immunotherapy: Progress, pitfalls, and promises. Mol. Cancer 2023, 22, 40. [Google Scholar] [CrossRef]
- Lv, B.; Wang, Y.; Ma, D.; Cheng, W.; Liu, J.; Yong, T.; Chen, H.; Wang, C. Immunotherapy: Reshape the Tumor Immune Microenvironment. Front. Immunol. 2022, 13, 844142. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi Rad, H.; Monkman, J.; Warkiani, M.E.; Ladwa, R.; O’Byrne, K.; Rezaei, N.; Kulasinghe, A. Understanding the tumor microenvironment for effective immunotherapy. Med. Res. Rev. 2021, 41, 1474–1498. [Google Scholar] [CrossRef]
- Binnewies, M.; Roberts, E.W.; Kersten, K.; Chan, V.; Fearon, D.F.; Merad, M.; Coussens, L.M.; Gabrilovich, D.I.; Ostrand-Rosenberg, S.; Hedrick, C.C. Understanding the tumor immune microenvironment (TIME) for effective therapy. Nat. Med. 2018, 24, 541–550. [Google Scholar] [CrossRef]
- Anderson, N.M.; Simon, M.C. The tumor microenvironment. Curr. Biol. 2020, 30, R921–R925. [Google Scholar] [CrossRef] [PubMed]
- Katsuta, E.; Rashid, O.M.; Takabe, K. Clinical relevance of tumor microenvironment: Immune cells, vessels, and mouse models. Hum. Cell 2020, 33, 930–937. [Google Scholar] [CrossRef]
- Tiwari, A.; Trivedi, R.; Lin, S.-Y. Tumor microenvironment: Barrier or opportunity towards effective cancer therapy. J. Biomed. Sci. 2022, 29, 83. [Google Scholar] [CrossRef]
- Ni, L.; Xu, J.; Li, Q.; Ge, X.; Wang, F.; Deng, X.; Miao, L. Focusing on the Immune Cells: Recent Advances in Immunotherapy for Biliary Tract Cancer. Cancer Manag. Res. 2024, 16, 941–963. [Google Scholar] [CrossRef]
- Chellappa, S.; Hugenschmidt, H.; Hagness, M.; Subramani, S.; Melum, E.; Line, P.D.; Labori, K.-J.; Wiedswang, G.; Taskén, K.; Aandahl, E.M. CD8+ T Cells That Coexpress RORγt and T-bet Are Functionally Impaired and Expand in Patients with Distal Bile Duct Cancer. J. Immunol. 2017, 198, 1729–1739. [Google Scholar] [CrossRef]
- Miyahara, Y.; Takashi, S.; Shimizu, Y.; Ohtsuka, M. The prognostic impact of neutrophil-to-lymphocyte ratio (NLR) and lymphocyte-to-monocyte ratio (LMR) in patients with distal bile duct cancer. World J. Surg. Oncol. 2020, 18, 78. [Google Scholar] [CrossRef]
- Balermpas, P.; Rödel, F.; Liberz, R.; Oppermann, J.; Wagenblast, J.; Ghanaati, S.; Harter, P.N.; Mittelbronn, M.; Weiss, C.; Rödel, C.; et al. Head and neck cancer relapse after chemoradiotherapy correlates with CD163+ macrophages in primary tumour and CD11b+ myeloid cells in recurrences. Br. J. Cancer 2014, 111, 1509–1518. [Google Scholar] [CrossRef]
- Schmid, M.C.; Khan, S.Q.; Kaneda, M.M.; Pathria, P.; Shepard, R.; Louis, T.L.; Anand, S.; Woo, G.; Leem, C.; Faridi, M.H.; et al. Integrin CD11b activation drives anti-tumor innate immunity. Nat. Commun. 2018, 9, 5379. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.-Q.; Hu, X.-W.; Liu, Y.-L.; Ye, Z.-J.; Gui, Y.-H.; Zhou, D.-L.; Qi, C.-L.; He, X.-D.; Wang, H.; Wang, L.-J. CD11b deficiency suppresses intestinal tumor growth by reducing myeloid cell recruitment. Sci. Rep. 2015, 5, 15948. [Google Scholar] [CrossRef] [PubMed]
- Kudo-Saito, C.; Ogiwara, Y.; Imazeki, H.; Boku, N.; Uemura, Y.; Zhang, R.; Kawano-Nagatsuma, A.; Kojima, M.; Ochiai, A. CD11b+ DIP2A+ LAG3+ cells facilitate immune dysfunction in colorectal cancer. Am. J. Cancer Res. 2021, 11, 5428. [Google Scholar]
- Okita, Y.; Tanaka, H.; Ohira, M.; Muguruma, K.; Kubo, N.; Watanabe, M.; Fukushima, W.; Hirakawa, K. Role of tumor-infiltrating CD11b+ antigen-presenting cells in the progression of gastric cancer. J. Surg. Res. 2014, 186, 192–200. [Google Scholar] [CrossRef]
- Jiang, Y.; Wang, C.; Wang, Y.; Zhang, W.; Liu, L.; Cheng, J. Prognostic role of CD11b+ myeloid-derived suppressor cells in oral squamous cell carcinoma. Arch. Med. Sci. 2021, 19, 171–179. [Google Scholar] [CrossRef]
- Yang, C.; Li, L.; Ye, Z.; Zhang, A.; Bao, Y.; Wu, X.; Ren, G.; Jiang, C.; Wang, O.; Wang, Z. Mechanisms underlying neutrophils adhesion to triple-negative breast cancer cells via CD11b-ICAM1 in promoting breast cancer progression. Cell Commun. Signal. 2024, 22, 340. [Google Scholar] [CrossRef]
- Sahin, U.; Türeci, Ö. Personalized vaccines for cancer immunotherapy. Science 2018, 359, 1355–1360. [Google Scholar] [CrossRef]
- Jenkins, R.W.; Barbie, D.A.; Flaherty, K.T. Mechanisms of resistance to immune checkpoint inhibitors. Br. J. Cancer 2018, 118, 9–16. [Google Scholar] [CrossRef]
- Xue, D.; Hsu, E.; Fu, Y.-X.; Peng, H. Next-generation cytokines for cancer immunotherapy. Antib. Ther. 2021, 4, 123–133. [Google Scholar] [CrossRef]
- Chen, M.-H.; Atenafu, E.; Craddock, K.J.; Brandwein, J.; Chang, H. CD11b expression correlates with monosomal karyotype and predicts an extremely poor prognosis in cytogenetically unfavorable acute myeloid leukemia. Leuk. Res. 2013, 37, 122–128. [Google Scholar] [CrossRef]
- Saed, G.M.; Fletcher, N.M.; Diamond, M.P.; Morris, R.T.; Gomez-Lopez, N.; Memaj, I. Novel expression of CD11b in epithelial ovarian cancer: Potential therapeutic target. Gynecol. Oncol. 2018, 148, 567–575. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.-Y.; Wang, Y.-M.; Wang, C.-L.; Feng, P.-H.; Ko, H.-W.; Liu, Y.-H.; Wu, Y.-C.; Chu, Y.; Chung, F.-T.; Kuo, C.-H.; et al. Population alterations of l-arginase- and inducible nitric oxide synthase-expressed CD11b+/CD14−/CD15+/CD33+ myeloid-derived suppressor cells and CD8+ T lymphocytes in patients with advanced-stage non-small cell lung cancer. J. Cancer Res. Clin. Oncol. 2009, 136, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Daurkin, I.; Eruslanov, E.; Vieweg, J.; Kusmartsev, S. Generation of antigen-presenting cells from tumor-infiltrated CD11b myeloid cells with DNA demethylating agent 5-aza-2′-deoxycytidine. Cancer Immunol. Immunother. 2009, 59, 697–706. [Google Scholar] [CrossRef]
- Ahn, G.O.; Tseng, D.; Liao, C.-H.; Dorie, M.J.; Czechowicz, A.; Brown, J.M. Inhibition of Mac-1 (CD11b/CD18) enhances tumor response to radiation by reducing myeloid cell recruitment. Proc. Natl. Acad. Sci. USA 2010, 107, 8363–8368. [Google Scholar] [CrossRef]
- Mizutani, K.; Sud, S.; Pienta, K.J. Prostate cancer promotes CD11b positive cells to differentiate into osteoclasts. J. Cell. Biochem. 2009, 106, 563–569. [Google Scholar] [CrossRef]
- Roche, V.; Sandoval, V.; Wolford, C.; Senders, Z.; Kim, J.A.; Ribeiro, S.P.; Huang, A.Y.; Sekaly, R.-P.; Lyons, J.; Zhang, M. Carbohydrate ligand engagement with CD11b enhances differentiation of tumor-associated myeloid cells for immunotherapy of solid cancers. J. ImmunoTherapy Cancer 2023, 11, e006205. [Google Scholar] [CrossRef]
- Panni, R.Z.; Herndon, J.M.; Zuo, C.; Hegde, S.; Hogg, G.D.; Knolhoff, B.L.; Breden, M.A.; Li, X.; Krisnawan, V.E.; Khan, S.Q.; et al. Agonism of CD11b reprograms innate immunity to sensitize pancreatic cancer to immunotherapies. Sci. Transl. Med. 2019, 11, eaau9240. [Google Scholar] [CrossRef]
- Kinoshita, J.; Fushida, S.; Yamaguchi, T.; Moriyama, H.; Saito, H.; Shimada, M.; Terai, S.; Okamoto, K.; Nakamura, K.; Ninomiya, I.; et al. Prognostic value of tumor-infiltrating CD163+macrophage in patients with metastatic gastric cancer undergoing multidisciplinary treatment. BMC Cancer 2022, 22, 608. [Google Scholar] [CrossRef]
- Ni, C.; Yang, L.; Xu, Q.; Yuan, H.; Wang, W.; Xia, W.; Gong, D.; Zhang, W.; Yu, K. CD68- and CD163-positive tumor infiltrating macrophages in non-metastatic breast cancer: A retrospective study and meta-analysis. J. Cancer 2019, 10, 4463–4472. [Google Scholar] [CrossRef]
- Miura, T.; Yoshizawa, T.; Hirai, H.; Seino, H.; Morohashi, S.; Wu, Y.; Wakiya, T.; Kimura, N.; Kudo, D.; Ishido, K.; et al. Prognostic Impact of CD163+ Macrophages in Tumor Stroma and CD8+ T-Cells in Cancer Cell Nests in Invasive Extrahepatic Bile Duct Cancer. Anticancer Res. 2017, 37, 183–190. [Google Scholar] [CrossRef]
- Norian, L.A.; Rodriguez, P.C.; O’Mara, L.A.; Zabaleta, J.; Ochoa, A.C.; Cella, M.; Allen, P.M. Tumor-Infiltrating Regulatory Dendritic Cells Inhibit CD8+ T Cell Function via l-Arginine Metabolism. Cancer Res. 2009, 69, 3086–3094. [Google Scholar] [CrossRef]
- Hong, S.A.; Hwang, H.W.; Kim, M.K.; Lee, T.J.; Yim, K.; Won, H.S.; Sun, D.S.; Kim, E.Y.; Ko, Y.H. High endothelial venule with concomitant high CD8+ tumor-infiltrating lymphocytes is associated with a favorable prognosis in resected gastric cancer. J. Clin. Med. 2020, 9, 2628. [Google Scholar] [CrossRef]
- Raskov, H.; Orhan, A.; Christensen, J.P.; Gögenur, I. Cytotoxic CD8+ T cells in cancer and cancer immunotherapy. Br. J. Cancer 2020, 124, 359–367. [Google Scholar] [CrossRef]
- Yu, J.; Green, M.D.; Li, S.; Sun, Y.; Journey, S.N.; Choi, J.E.; Rizvi, S.M.; Qin, A.; Waninger, J.J.; Lang, X.; et al. Liver metastasis restrains immunotherapy efficacy via macrophage-mediated T cell elimination. Nat. Med. 2021, 27, 152–164. [Google Scholar] [CrossRef]
- Gallina, G.; Dolcetti, L.; Serafini, P.; De Santo, C.; Marigo, I.; Colombo, M.P.; Basso, G.; Brombacher, F.; Borrello, I.; Zanovello, P.; et al. Tumors induce a subset of inflammatory monocytes with immunosuppressive activity on CD8+ T cells. J. Clin. Investig. 2006, 116, 2777–2790. [Google Scholar] [CrossRef]
- Duong, E.; Fessenden, T.B.; Lutz, E.; Dinter, T.; Yim, L.; Blatt, S.; Bhutkar, A.; Wittrup, K.D.; Spranger, S. Type I interferon activates MHC class I-dressed CD11b+ conventional dendritic cells to promote protective anti-tumor CD8+ T cell immunity. Immunity 2022, 55, 308–323.e309. [Google Scholar] [CrossRef] [PubMed]
- Thorsson, V.; Gibbs, D.L.; Brown, S.D.; Wolf, D.; Bortone, D.S.; Ou Yang, T.H.; Porta-Pardo, E.; Gao, G.F.; Plaisier, C.L.; Eddy, J.A.; et al. The Immune Landscape of Cancer. Immunity 2018, 48, 812–830.e814. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CD11b | CD8 | CD163 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | High (n = 38) (%) | Low (n = 52) (%) | p-Value | High (n = 40) (%) | Low (n = 50) (%) | p-Value | High (n = 70) (%) | Low (n = 20) (%) | p-Value |
| Age (mean ± SD) | 66.7 ± 10.4 | 68.0 ± 9.6 | 0.557 * | 66.1 ± 9.4 | 68.5 ± 10.3 | 0.247 * | 66.9± 10.0 | 69.4 ± 9.5 | 0.317 * |
| Gender | 0.626 | 0.981 | 0.510 | ||||||
| Male | 24 (63.2) | 29 (55.8) | 23 (57.5) | 30 (60.0) | 43 (61.4) | 10 (50.0) | |||
| Female | 14 (36.8) | 23 (44.2) | 17 (42.5) | 20 (40.0) | 27 (38.6) | 10 (50.0) | |||
| Tumor size (mean ± SD) | 3.2± 1.5 | 3.0 ± 1.3 | 0.726 * | 3.0 ± 1.3 | 3.2 ± 1.5 | 0.549 * | 3.1 ± 1.3 | 3.1 ± 1.5 | 0.936 * |
| Histologic grade | 0.358 | 0.707 | 0.206 | ||||||
| Well | 8 (21.1) | 16 (30.8) | 9 (22.5) | 15(30.0) | 16 (22.9) | 8 (40.0) | |||
| Moderate Poorly | 23 (60.5) 7 (18.4) | 31 (59.6) 5 (9.6) | 25 (62.5) 6 (15.0) | 29(58.0) 6 (12.0) | 43 (61.4) 11 (15.7) | 11 (55.0) 1 (5.0) | |||
| T stage | 0.318 | 0.002 | 0.372 | ||||||
| T1 | 7 (18.4) | 17 (32.7) | 15 (37.5) | 9 (18.0) | 21 (30.0) | 3 (15.0) | |||
| T2 | 14 (36.8) | 16 (30.8) | 17(42.5) | 13(26.0) | 23 (32.9) | 7 (35.0) | |||
| T3 | 17 (44.7) | 19 (36.5) | 18(20.0) | 28(56.0) | 26 (37.1) | 10 (50.0) | |||
| N stage | 0.723 | 0.338 | 0.678 | ||||||
| N0 | 24 (63.2) | 37 (71.2) | 30(75.0) | 31(62.0) | 46 (65.7) | 15 (75.0) | |||
| N1 N2 | 12 (31.6) 2 (5.3) | 13 (25.0) 2 (3.8) | 8 (20.0) 2 (5.0) | 17(34.0) 2(4.0%) | 21 (30.0) 3 (4.3) | 4 (20.0) 1 (5.0) | |||
| Lymphovascular invasion | 1 | 0.832 | 1 | ||||||
| Yes | 19 (50.0) | 26 (50.0) | 19(47.5) | 26(52.0) | 35 (50.0) | 10 (50.0) | |||
| No | 19 (50.0) | 26 (50.0) | 21(52.5) | 24 (48.0) | 35 (50.0) | 10 (50.0) | |||
| Perineural invasion | 0.803 | 0.583 | 0.654 | ||||||
| Yes | 29 (76.3) | 42 (80.8) | 30(75.0) | 41 (82.0) | 54 (77.1) | 17 (85.0) | |||
| No | 9 (23.7) | 10 (19.2) | 10(25.0) | 9 (18.0) | 16 (22.9) | 3 (15.0) | |||
| Margin status of the bile duct | 0.386 | 0.189 | 0.560 | ||||||
| R0 | 32 (84.2) | 48 (92.3) | 38(95.0) | 42(84.0) | 61 (87.1) | 19 (95.0) | |||
| R1 | 6 (15.8) | 4 (7.7) | 2 (5.0) | 8 (16.0) | 9 (12.9) | 1 (5.0) | |||
| Low CD11b/ High CD8 | |||
|---|---|---|---|
| Variable | Present (n = 27) (%) | Absent (n = 63) (%) | p-Value |
| Age (mean ± SD) | 66.6 ± 9.6 | 67.8 ± 10.1 | 0.585 |
| Gender | 0.782 | ||
| Male | 15 (55.6) | 38 (60.3) | |
| Female | 12 (44.4) | 25 (39.7) | |
| Tumor size (mean ± SD) | 3.0 ± 1.2 | 3.1 ± 1.5 | 0.633 |
| Histologic grade | 0.902 | ||
| Well | 7 (25.9) | 17 (27.0) | |
| Moderate Poorly | 17 (63.0) 3 (11.1) | 37 (58.7) 9 (14.3) | |
| T stage | <0.001 | ||
| T1 | 13 (48.1) | 11 (17.5) | |
| T2 | 11 (40.7) | 19 (30.2) | |
| T3 | 3 (11.1) | 33 (52.4) | |
| N stage | 0.178 | ||
| N0 | 22 (81.5) | 39 (61.9) | |
| N1 N2 | 4 (14.8) 1 (3.7) | 21 (33.3) 3 (4.8) | |
| Lymphovascular invasion | 0.358 | ||
| Yes | 11 (40.7) | 34 (54.0) | |
| No | 16 (59.3) | 29 (46.0) | |
| Perineural invasion | 0.310 | ||
| Yes | 19 (70.4) | 52 (82.5) | |
| No | 8 (29.6) | 11 (17.5) | |
| Margin status of the bile duct | 0.067 | ||
| R0 | 27 (100) | 53 (84.1) | |
| R1 | 0 (0) | 10 (15.9) | |
| Clinicopathologic Factors | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age (years) | 1.006 | 0.980–1.033 | 0.649 | |||
| Gender | ||||||
| Male | ||||||
| Female | 0.971 | 0.590–1.599 | 0.909 | |||
| Tumor size | 0.993 | 0.828–1.190 | 0.937 | |||
| Histologic grade | ||||||
| Well | ||||||
| Moderate | 1.410 | 0.800–2.484 | 0.235 | |||
| Poorly | 1.372 | 0.615–3.062 | 0.440 | |||
| pT stage | ||||||
| pT1 | ||||||
| PT2 | 4.967 | 2.061–11.974 | <0.001 | 5.221 | 1.989–13.704 | <0.001 |
| PT3 | 9.584 | 4.008–22.920 | <0.001 | 6.785 | 2.646–17.397 | <0.001 |
| pN stage | ||||||
| pN0 | ||||||
| pN1 | 1.760 | 1.019–3.040 | 0.043 | 1.267 | 0.721–2.226 | 0.411 |
| pN2 | 4.565 | 1.334–15.615 | 0.016 | 2.711 | 0.782–9.390 | 0.116 |
| Lymphovascular invasion | ||||||
| No | ||||||
| Yes | 1.595 | 0.970–2.624 | 0.066 | |||
| Margin status of the bile duct | ||||||
| R0 | ||||||
| R1 | 2.046 | 1.030–4.066 | 0.041 | 0.969 | 0.479–1.962 | 0.931 |
| Perineural invasion | ||||||
| No | ||||||
| Yes | 0.764 | 0.406–1.436 | 0.403 | |||
| Low CD11b/ high CD8 | ||||||
| No | ||||||
| Yes | 0.124 | 0.050–0.311 | <0.001 | 0.159 | 0.061–0.410 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, J.H.; Kim, J.Y.; Lee, K.R.; Lee, G.Y.; Hong, M.; Hwang, H.W.; Lee, M.Y.; Kim, M.K.; Hong, S.A. Prognostic Significance of CD11b-, CD8-, and CD163-Positive Tumor-Infiltrating Immune Cells in Distal Bile Duct Cancer. J. Pers. Med. 2024, 14, 1033. https://doi.org/10.3390/jpm14101033
Choi JH, Kim JY, Lee KR, Lee GY, Hong M, Hwang HW, Lee MY, Kim MK, Hong SA. Prognostic Significance of CD11b-, CD8-, and CD163-Positive Tumor-Infiltrating Immune Cells in Distal Bile Duct Cancer. Journal of Personalized Medicine. 2024; 14(10):1033. https://doi.org/10.3390/jpm14101033
Chicago/Turabian StyleChoi, Jae Hyung, Joo Young Kim, Ki Rim Lee, Gyeong Yun Lee, Mineui Hong, Hye Won Hwang, Moo Yeol Lee, Mi Kyung Kim, and Soon Auck Hong. 2024. "Prognostic Significance of CD11b-, CD8-, and CD163-Positive Tumor-Infiltrating Immune Cells in Distal Bile Duct Cancer" Journal of Personalized Medicine 14, no. 10: 1033. https://doi.org/10.3390/jpm14101033
APA StyleChoi, J. H., Kim, J. Y., Lee, K. R., Lee, G. Y., Hong, M., Hwang, H. W., Lee, M. Y., Kim, M. K., & Hong, S. A. (2024). Prognostic Significance of CD11b-, CD8-, and CD163-Positive Tumor-Infiltrating Immune Cells in Distal Bile Duct Cancer. Journal of Personalized Medicine, 14(10), 1033. https://doi.org/10.3390/jpm14101033