
AI-ADC: Channel and Spatial Attention-Based Contrastive Learning to Generate ADC Maps from T2W MRI for Prostate Cancer Detection

 , , , and
, , , and
Abstract
1. Introduction
- -
- Unpaired image-to-image translation: to generate ADC maps from T2W MRI without requiring explicit image pairing and annotation.
- -
- A hybrid attention module: to drive the network attention to tumor-specific regions in the prostate by optimizing the future space.
- -
- A self-regularization loss: to ensure that prostate boundary and other anatomical regions are reflected accurately in the synthesized ADC maps.
2. Materials and Methods
2.1. Prostate MRI Dataset
2.2. AI-ADC Method
2.3. Performance Metrics
2.3.1. Peak Signal-to-Noise Ratio
2.3.2. Structural Similarity Index
2.3.3. Frechet Inception Distance
2.3.4. Dice Scores
3. Results
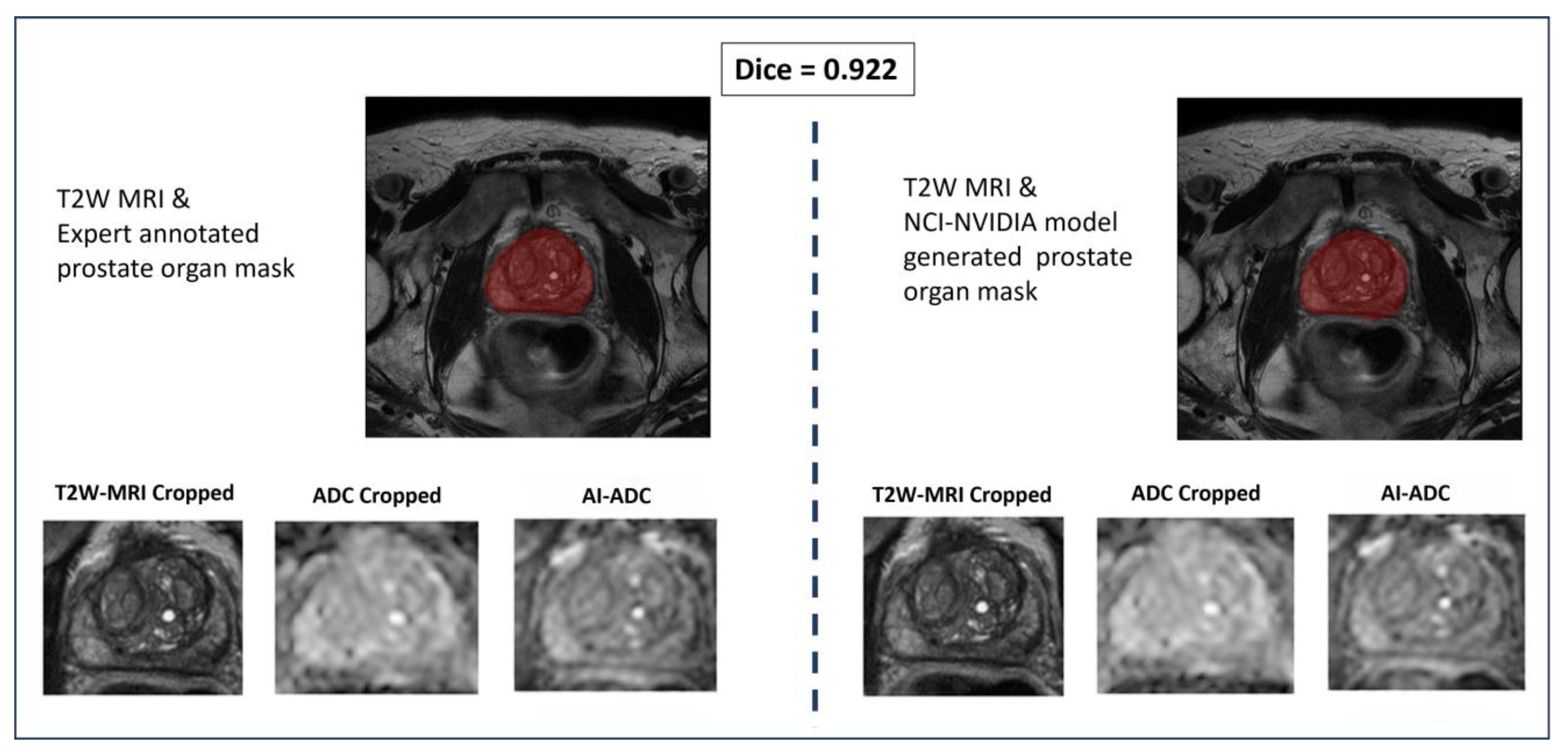
In-House Prostate Organ Segmentor vs. Expert Annotation
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yang, E.; Nucifora, P.G.; Melhem, E.R. Diffusion MR Imaging: Basic Principles. Neuroimaging Clin. N. Am. 2011, 21, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Tavakoli, A.A.; Hielscher, T.; Badura, P.; Görtz, M.; Kuder, T.A.; Gnirs, R.; Schwab, C.; Hohenfellner, M.; Schlemmer, H.P.; Bonekamp, D. Contribution of Dynamic Contrast-enhanced and Diffusion MRI to PI-RADS for Detecting Clinically Significant Prostate Cancer. Radiology 2023, 306, 186–199. [Google Scholar] [CrossRef] [PubMed]
- Hori, M.; Kamiya, K.; Murata, K. Technical Basics of Diffusion-Weighted Imaging. Magn. Reson. Imaging Clin. N. Am. 2021, 29, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Tamada, T.; Ueda, Y.; Ueno, Y.; Kojima, Y.; Kido, A.; Yamamoto, A. Diffusion-weighted imaging in prostate cancer. Magn. Reson. Mater. Phys. Biol. Med. 2022, 35, 533–547. [Google Scholar] [CrossRef] [PubMed]
- Turkbey, B.; Shah, V.; Pang, Y.; Bernardo, M.; Xu, S.; Kruecker, J.; Locklin, J.; Baccala, A.; Rastinehad, A.; Merino, M.; et al. Is Apparent Diffusion Coefficient Associated with Clinical Risk Scores for Prostate Cancers that Are Visible on 3-T MR Images? Radiology 2011, 258, 488–495. [Google Scholar] [CrossRef] [PubMed]
- McPartlin, A.; Kershaw, L.; McWilliam, A.; Taylor, M.B.; Hodgson, C.; van Herk, M.; Choudhury, A. Changes in prostate apparent diffusion coefficient values during radiotherapy after neoadjuvant hormones. Ther. Adv. Urol. 2018, 10, 359–364. [Google Scholar] [CrossRef]
- Dinis Fernandes, C.; Houdt, P.; Heijmink, S.; Walraven, I.; Keesman, R.; Smolic, M.; Ghobadi, G.; Poel, H.; Schoots, I.; Pos, F.; et al. Quantitative 3T multiparametric MRI of benign and malignant prostatic tissue in patients with and without local recurrent prostate cancer after external-beam radiation therapy. J. Magn. Reson. Imaging 2018, 50, 269–278. [Google Scholar] [CrossRef]
- Guerra, A.; Flor-de-Lima, B.; Freire, G.; Lopes, A.; Cassis, J. Radiologic-pathologic correlation of prostatic cancer extracapsular extension (ECE). Insights Imaging 2023, 14, 88. [Google Scholar] [CrossRef]
- Zaitsev, M.; Maclaren, J.; Herbst, M. Motion artifacts in MRI: A complex problem with many partial solutions. J. Magn. Reson. Imaging 2015, 42, 887–901. [Google Scholar] [CrossRef]
- Hu, L.; Zhou, D.-W.; Zha, Y.-F.; Li, L.; He, H.; Xu, W.-H.; Qian, L.; Zhang, Y.-K.; Fu, C.-X.; Hu, H.; et al. Synthesizing High-b-Value Diffusion-weighted Imaging of the Prostate Using Generative Adversarial Networks. Radiol. Artif. Intell. 2021, 3, e200237. [Google Scholar] [CrossRef]
- Hu, L.; Zhou, D.W.; Fu, C.X.; Benkert, T.; Xiao, Y.F.; Wei, L.M.; Zhao, J.G. Calculation of Apparent Diffusion Coefficients in Prostate Cancer Using Deep Learning Algorithms: A Pilot Study. Front. Oncol. 2021, 11, 697721. [Google Scholar] [CrossRef] [PubMed]
- Costa, P.; Galdran, A.; Meyer, M.I.; Niemeijer, M.; Abràmoff, M.; Mendonça, A.M.; Campilho, A. End-to-End Adversarial Retinal Image Synthesis. IEEE Trans. Med. Imaging 2018, 37, 781–791. [Google Scholar] [CrossRef] [PubMed]
- Isola, P.; Zhu, J.Y.; Zhou, T.; Efros, A.A. Image-to-Image Translation with Conditional Adversarial Networks. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 5967–5976. [Google Scholar]
- Yu, B.; Zhou, L.; Wang, L.; Shi, Y.; Fripp, J.; Bourgeat, P. Ea-GANs: Edge-Aware Generative Adversarial Networks for Cross-Modality MR Image Synthesis. IEEE Trans. Med. Imaging 2019, 38, 1750–1762. [Google Scholar] [CrossRef] [PubMed]
- He, K.; Fan, H.; Wu, Y.; Xie, S.; Girshick, R. Momentum Contrast for Unsupervised Visual Representation Learning. In Proceedings of the 2020 IEEE/CVF Conference on Computer Vision and Pattern Recognition (CVPR), Seattle, WA, USA, 13–19 June 2020; pp. 9726–9735. [Google Scholar]
- Chen, T.; Kornblith, S.; Norouzi, M.; Hinton, G. A simple framework for contrastive learning of visual representations. In Proceedings of the 37th International Conference on Machine Learning, Virtual, 13–18 July 2020; p. 149. [Google Scholar]
- Goodfellow, I.J.; Pouget-Abadie, J.; Mirza, M.; Xu, B.; Warde-Farley, D.; Ozair, S.; Courville, A.; Bengio, Y. Generative adversarial nets. In Proceedings of the 27th International Conference on Neural Information Processing Systems, Bangkok, Thailand, 18–22 November 2022; Volume 2, pp. 2672–2680. [Google Scholar]
- Giganti, F.; Kirkham, A.; Kasivisvanathan, V.; Papoutsaki, M.-V.; Punwani, S.; Emberton, M.; Moore, C.M.; Allen, C. Understanding PI-QUAL for prostate MRI quality: A practical primer for radiologists. Insights Imaging 2021, 12, 59. [Google Scholar] [CrossRef] [PubMed]
- Sanford, T.H.; Zhang, L.; Harmon, S.A.; Sackett, J.; Yang, D.; Roth, H.; Xu, Z.; Kesani, D.; Mehralivand, S.; Baroni, R.H.; et al. Data Augmentation and Transfer Learning to Improve Generalizability of an Automated Prostate Segmentation Model. AJR Am. J. Roentgenol. 2020, 215, 1403–1410. [Google Scholar] [CrossRef]
- Armato Iii, S.; Huisman, H.; Drukker, K.; Hadjiiski, L.; Kirby, J.; Petrick, N.; Redmond, G.; Giger, M.; Cha, K.; Mamonov, A.; et al. PROSTATEx Challenges for computerized classification of prostate lesions from multiparametric magnetic resonance images. J. Med. Imaging 2018, 5, 044501. [Google Scholar] [CrossRef]
- Litjens, G.; Debats, O.; Barentsz, J.; Karssemeijer, N.; Huisman, H. Computer-Aided Detection of Prostate Cancer in MRI. IEEE Trans. Med. Imaging 2014, 33, 1083–1092. [Google Scholar] [CrossRef]
- Woo, S.; Park, J.; Lee, J.-Y.; Kweon, I.S. CBAM: Convolutional Block Attention Module. In Proceedings of the European Conference on Computer Vision (ECCV), Munich, Germany, 8–14 September 2018; pp. 3–19. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Mao, X.; Li, Q.; Xie, H.; Lau, R.Y.K.; Wang, Z.; Smolley, S.P. Least Squares Generative Adversarial Networks. In Proceedings of the 2017 IEEE International Conference on Computer Vision (ICCV), Venice, Italy, 22–29 October 2017; pp. 2813–2821. [Google Scholar]
- Park, T.; Efros, A.A.; Zhang, R.; Zhu, J.-Y. Contrastive Learning for Unpaired Image-to-Image Translation. In Proceedings of the Computer Vision—ECCV 2020, Cham, Switherland, 23–28 August 2020; pp. 319–345. [Google Scholar]
- Ozyoruk, K.B.; Can, S.; Darbaz, B.; Başak, K.; Demir, D.; Gokceler, G.I.; Serin, G.; Hacisalihoglu, U.P.; Kurtuluş, E.; Lu, M.Y.; et al. A deep-learning model for transforming the style of tissue images from cryosectioned to formalin-fixed and paraffin-embedded. Nat. Biomed. Eng. 2022, 6, 1407–1419. [Google Scholar] [CrossRef]
- Zhu, J.Y.; Park, T.; Isola, P.; Efros, A.A. Unpaired Image-to-Image Translation Using Cycle-Consistent Adversarial Networks. In Proceedings of the 2017 IEEE International Conference on Computer Vision (ICCV), Venice, Italy, 22–29 October 2017; pp. 2242–2251. [Google Scholar]
- Deng, Y.; Tang, F.; Dong, W.; Ma, C.; Pan, X.; Wang, L.; Xu, C. StyTr2: Image Style Transfer with Transformers. In Proceedings of the 2022 IEEE/CVF Conference on Computer Vision and Pattern Recognition (CVPR), New Orleans, LA, USA, 18–24 June 2022; pp. 11316–11326. [Google Scholar]
- Kingma, D.P.; Ba, J. Adam: A method for stochastic optimization. arXiv 2014, arXiv:1412.6980. [Google Scholar]
- Glorot, X.; Bengio, Y. Understanding the difficulty of training deep feedforward neural networks. In Proceedings of the Thirteenth International Conference On Artificial Intelligence and Statistics, Sardinia, Italy, 13–15 May 2010; pp. 249–256. [Google Scholar]
- Mehralivand, S.; Yang, D.; Harmon, S.A.; Xu, D.; Xu, Z.; Roth, H.; Masoudi, S.; Sanford, T.H.; Kesani, D.; Lay, N.S.; et al. A Cascaded Deep Learning-Based Artificial Intelligence Algorithm for Automated Lesion Detection and Classification on Biparametric Prostate Magnetic Resonance Imaging. Acad. Radiol. 2022, 29, 1159–1168. [Google Scholar] [CrossRef]
- Zhou, H.-Y.; Yu, Y.; Wang, C.; Zhang, S.; Gao, Y.; Pan, J.; Shao, J.; Lu, G.; Zhang, K.; Li, W. A transformer-based representation-learning model with unified processing of multimodal input for clinical diagnostics. Nat. Biomed. Eng. 2023, 7, 743–755. [Google Scholar] [CrossRef] [PubMed]
- Texier, B.; Hémon, C.; Lekieffre, P.; Collot, E.; Tahri, S.; Chourak, H.; Dowling, J.; Greer, P.; Bessieres, I.; Acosta, O.; et al. Computed tomography synthesis from magnetic resonance imaging using cycle Generative Adversarial Networks with multicenter learning. Phys. Imaging Radiat. Oncol. 2023, 28, 100511. [Google Scholar] [CrossRef] [PubMed]
- Conte, G.M.; Weston, A.D.; Vogelsang, D.C.; Philbrick, K.A.; Cai, J.C.; Barbera, M.; Sanvito, F.; Lachance, D.H.; Jenkins, R.B.; Tobin, W.O.; et al. Generative Adversarial Networks to Synthesize Missing T1 and FLAIR MRI Sequences for Use in a Multisequence Brain Tumor Segmentation Model. Radiology 2021, 299, 313–323. [Google Scholar] [CrossRef]
- Yusim, I.; Krenawi, M.; Mazor, E.; Novack, V.; Mabjeesh, N.J. The use of prostate specific antigen density to predict clinically significant prostate cancer. Sci. Rep. 2020, 10, 20015. [Google Scholar] [CrossRef] [PubMed]
- Checcucci, E.; Autorino, R.; Cacciamani, G.E.; Amparore, D.; De Cillis, S.; Piana, A.; Piazzolla, P.; Vezzetti, E.; Fiori, C.; Veneziano, D.; et al. Artificial intelligence and neural networks in urology: Current clinical applications. Minerva Urol. Nefrol. 2020, 72, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Snow, P.B.; Smith, D.S.; Catalona, W.J. Artificial neural networks in the diagnosis and prognosis of prostate cancer: A pilot study. J. Urol. 1994, 152, 1923–1926. [Google Scholar] [CrossRef]
- Djavan, B.; Remzi, M.; Zlotta, A.; Seitz, C.; Snow, P.; Marberger, M. Novel artificial neural network for early detection of prostate cancer. J. Clin. Oncol. 2002, 20, 921–929. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Models On Radiologists’ Masks | PSNR↑ * | SSIM↑ | FID↓ | Inference Time (s) |
|---|---|---|---|---|
| AI-ADC | 18.767 ± 3.357 | 0.870 ± 0.065 | 30.656 | 0.0065 ± 0.013 |
| StyTr2 | 18.289 ± 2.526 | 0.865 ± 0.076 | 61.286 | 0.0197 ± 0.0034 |
| CUT | 17.446 ± 2.315 | 0.801 ± 0.0082 | 174.752 | 0.0048 ± 0.0005 |
| CycleGAN | 17.950 ± 2.669 | 0.856 ± 0.047 | 58.071 | 0.177 ± 0.0028 |
| Models On AI Masks | PSNR↑ * | SSIM↑ | FID↓ | Inference Time (s) |
|---|---|---|---|---|
| AI-ADC | 16.244 ± 2.413 | 0.863 ± 0.068 | 31.992 | 0.0062 ± 0.0126 |
| StyTr2 | 15.538 ± 2.398 | 0.824 ± 0.072 | 58.784 | 0.0196 ± 0.0033 |
| CUT | 14.500 ± 2.266 | 0.797 ± 0.079 | 179.983 | 0.0048 ± 0.0004 |
| CycleGAN | 16.082 ± 2.587 | 0.855 ± 0.071 | 43.458 | 0.0179 ± 0.0032 |
| Models | PSNR↑ * | SSIM↑ | FID↓ | Inference Time (s) |
|---|---|---|---|---|
| AI-ADC | 18.910 ± 1.287 | 0.647 ± 0.045 | 113.876 | 0.0044 ± 0.013 |
| StyTr2 | 16.049 ± 2.760 | 0.534 ± 0.143 | 120.393 | 0.0133 ± 0.0023 |
| CUT | 11.689 ± 2.040 | 0.467 ± 0.123 | 224.678 | 0.0032 ± 0.0004 |
| CycleGAN | 12.974 ± 2.593 | 0.512 ± 0.112 | 140.898 | 0.0120 ± 0.0019 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ozyoruk, K.B.; Harmon, S.A.; Lay, N.S.; Yilmaz, E.C.; Bagci, U.; Citrin, D.E.; Wood, B.J.; Pinto, P.A.; Choyke, P.L.; Turkbey, B. AI-ADC: Channel and Spatial Attention-Based Contrastive Learning to Generate ADC Maps from T2W MRI for Prostate Cancer Detection. J. Pers. Med. 2024, 14, 1047. https://doi.org/10.3390/jpm14101047
Ozyoruk KB, Harmon SA, Lay NS, Yilmaz EC, Bagci U, Citrin DE, Wood BJ, Pinto PA, Choyke PL, Turkbey B. AI-ADC: Channel and Spatial Attention-Based Contrastive Learning to Generate ADC Maps from T2W MRI for Prostate Cancer Detection. Journal of Personalized Medicine. 2024; 14(10):1047. https://doi.org/10.3390/jpm14101047
Chicago/Turabian StyleOzyoruk, Kutsev Bengisu, Stephanie A. Harmon, Nathan S. Lay, Enis C. Yilmaz, Ulas Bagci, Deborah E. Citrin, Bradford J. Wood, Peter A. Pinto, Peter L. Choyke, and Baris Turkbey. 2024. "AI-ADC: Channel and Spatial Attention-Based Contrastive Learning to Generate ADC Maps from T2W MRI for Prostate Cancer Detection" Journal of Personalized Medicine 14, no. 10: 1047. https://doi.org/10.3390/jpm14101047
APA StyleOzyoruk, K. B., Harmon, S. A., Lay, N. S., Yilmaz, E. C., Bagci, U., Citrin, D. E., Wood, B. J., Pinto, P. A., Choyke, P. L., & Turkbey, B. (2024). AI-ADC: Channel and Spatial Attention-Based Contrastive Learning to Generate ADC Maps from T2W MRI for Prostate Cancer Detection. Journal of Personalized Medicine, 14(10), 1047. https://doi.org/10.3390/jpm14101047