
Advancing the Management of Skull Base Chondrosarcomas: A Systematic Review of Targeted Therapies

 ,
,  ,
, 
 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Review
2.2. Data Extraction
2.3. Outcomes
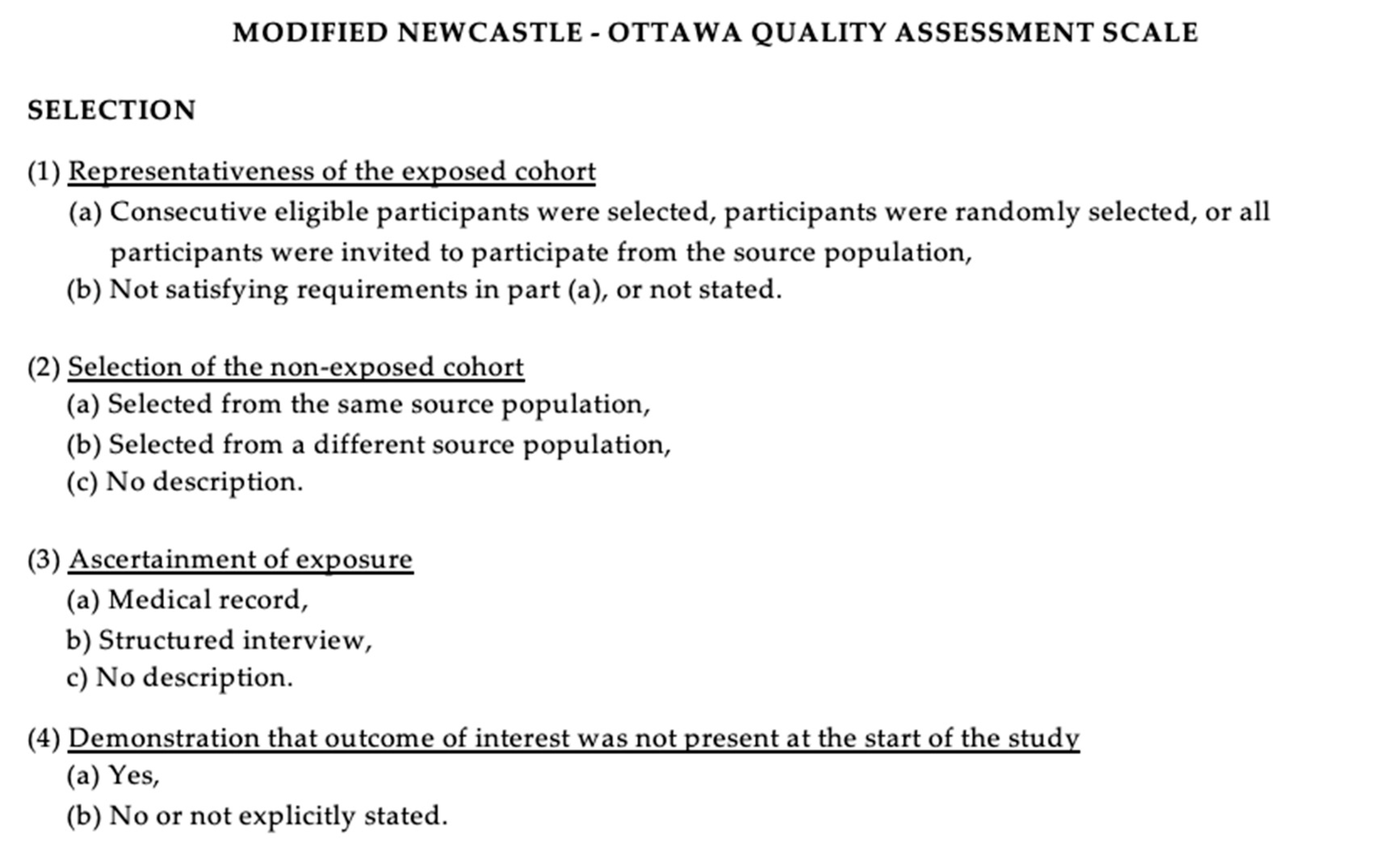
2.4. Risk of Bias Assessment
2.5. Statistical Analysis
3. Results
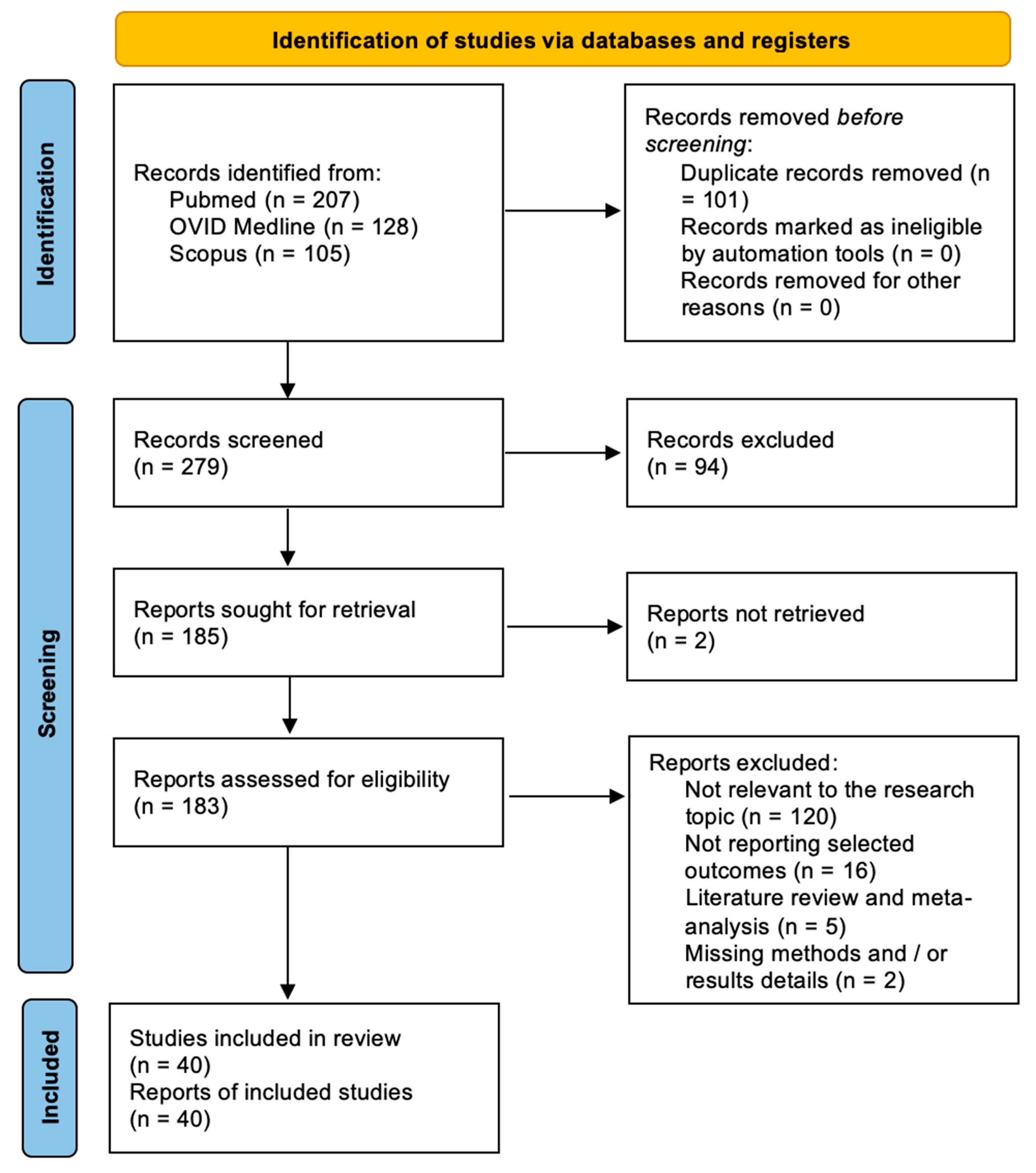
3.1. Literature Review
3.2. Data Analysis
3.2.1. Clinical Studies

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Patients (N) | Age (Mean–Range) | Sex (F: M Ration) | Prior Treatment | Systemic Targeted Treatment | Next Treatment | Outcome | Adverse Effect | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Target | Agent | Dosage | Duration (Months) | ||||||||
| Herbst et al. [13] 2010 | 2 | 56 (53–59) | 1:1 | Surgery, CT (Irinotecan, Gemcitabine/Docetaxel, and Thalidomide), RT | DR4 and DR5 | rhApo2L/TRAIL | 8 mg/kg and 30 mg/kg | N/A | N/A | PR (3 mo and 10 mo after starting target therapy) | N/A |
| Grignani et al. [14] 2010 | 26 | 52 (23–81) | 9:17 | CT (Doxorubicine 20 pts, Cisplatin/Ifosfamide 6 pts) | PDGFR-α and PDGFR-β | Imatinib | 400 mg BID | 24 | N/A | PD (18 pts) SD (8 pts) | N/A |
| Subbahia et al. [15] 2012 | 1 | 65 | 0:1 | Surgery, RT, CT (6 cycles of Irinotecan) | DR4 and DR5 | Dulanermin | 8 mg/kg IV on days 1 through 5 in a 21-day cycle | N/A | Surgery, Dulanermin (16 mo) | NED | N/A |
| Schwartz et al. [16] 2013 | 17 | 45.5 (18–73) | 10:7 | Surgery | IGFIR, TOR | Cixutumumab/Temsirolimus | 6 mg/kg IV/25 mg IV | 12 | N/A | mPFS: 6 mo; 3 mo PFS 31% in IGFR+ pt/ 39% in IGFR—pt, | Anemia (16 pts), hyperglycemia (18 pt), hypophosphatemia (16 pts), lymphopenia (25 pts), oral mucositis (19 pts), thrombocytopenia (19 pts) |
| Italiano et al. [17] 2013 | 45 | 56 (27–85) | 14:31 | N/A | Hh signal pathway | GDC-0449 | 150 mg per os, QD, in a 28-day cycle. | 6 | N/A | SD ≥ 6 mo (10 pts) PD (29 pts) | Dysgeusia (29 pts), fatigue (22 pts), myalgia (22 pts), alopecia (18 pts), ALT or AST increase (2 pts). |
| Paoluzzi et al. [18] 2016 | 1 | 74 | N/A | N/A | PD-1 | Nivolumab | 3 mg/kg IV every 2 weeks | 12 | N/A | PR | N/A |
| Schuetze et al. [11] 2016 | 11 | 54 (22–87) | 6:5 | N/A | c-KIT, BCR-ABL, PDGFR-α and PDGFR-β | Dasatinib | 70–100 mg BID per os. | 1–87 | N/A | mPFS: 5.5 mo, 6-mo PFS: 47%, | Fatigue, fever, anorexia, weight loss, rash, nausea, vomiting, constipation (1 pt) |
| Tawbi et al. [19] 2017 | 5 | 35 (22–48) | 2:3 | N/A | PD-L1 | Pembrolizumab | 200 mg | 12 | N/A | PR (1 pt), SD (1 pt), PD (3 pts) | Anemia (1 pt), decreased lymphocyte count (1 pt), prolonged APTT (1 pt), decreased platelet count (1pts) |
| Bupathi et al. [20] 2017 | 2 | N/A | N/A | ST (Sunitinib, Nivolumab, Everolimus), RT | VEGFR-1/2/3, PDGFR, cKIT | Pazopanib | 800 mg per os QD | 15–19 | Pazopanib (400 mg/day → 800 mg/day) QD and Temozolomide (150 mg/m2, 7 days on with 7 days off) in a 28-day cycle | PD, SD | Fatigue (1 pt), anorexia (1 pt), constipation (1 pt), hypertension (2 pts), thrombocytopenia (1 pt) |
| Chow et al. [21] 2020 | 47 | 58 (32–87) | 18:29 | Surgery, CT, RT | VEGFR-1/2/3, PDGRF, cKIT | Pazopanib | 800 mg per os QD in a 28-day cycle | 48 | N/A | PR (1 pt), SD (30 pts), PD (11 pts) mPFS:7,9 mo, 3-mo PFS: 40% | ARF (1 pt), ALT elevation (4 pts), anemia (1 pt) diarrhea (1 pt) dyspnea (1 pt), fatigue (1 pt), hemorrhage CNSa (1 pt), hyperbilirubinemia (1 pt), hypertension (12 pts), hyponatremia (1 pt), left pulmonary vein thrombosis (1 pt), proteinuria(1 pt), pulmonary emboli (2 pt), thromboembolic event (1 pt) |
| Xie et al. [22] 2020 | 33 | 44,5 (17–72) | 9:24 | Surgery, CT (Doxorubicin, Ifosfamide in 13 pts) | VEGFR-2 | Apatinib | 500 mg per os QD, 30 min after the meal | N/A | N/A | PR (6 pts), SD (23 pts), PD (4 pts), mPFS of 7 mo, 6-mo PFS: 47%, | Anorexia (12 pts), wound dehiscence and infections (9 pts), platelet decrease (3 pts) hypertension (2 pts) |
| Tap W.D. et al. [23] 2020 | 21 | 55 (30–88) | 8:13 | Surgery (16 pts), ST (11 pts), RT (7 pts) | mutant IDH1 | Ivosidenib | 100 mg BID and 300–1200 mg QD per os in 28-day cycles | >47 | N/A | SD 11 pts PD 6 pts mPFS: 5,6 mo 6 mo PFS: 39.5% | Diarrhea (9 pts), nausea (7 pts), fatigue (6 pts), edema peripheral (6 pts), upper respiratory tract infection (5 pts), constipation (4 pts), decreased appetite (4 pts), pain in extremity (5 pts), anemia (4 pts), arthralgia (3 pts), headache (3 pts), dizziness (3 pts), dyspnea (3 pts), vomiting (3 pts). |
| Duffaud et al. [12] 2021 | 40 | 64 (37.5–67.5) | 15:25 | CT (Doxorubicine, Ifosfamide, Cisplatin) | VEGFR1-3, TIE2, PDGFRβ, FGF, KIT, RET, RAF | Regorafenib/ Placebo | 160 mg per os | 53 | N/A | PR 2 pts SD 16 pts PD 21 pts mPFS: 19,9/8 mo 6 mo PFS: 43/25% | Pain (31 pts), hypertension (13 pts), asthenia (24 pts), thrombocytopenia (5 pts), diarrhea (18 pts) |
3.2.2. Preclinical Studies
| Author, Year | Study Type | Targeted Treatment | Study Purpose | Results | ||
|---|---|---|---|---|---|---|
| Target | Agent | Dosage | ||||
| Tomek et al. [24] 2003 | In vitro | DR4, DR5, TRID, TRUNDD, osteoprotegerin | TRAIL | 100–1000 ng/mL | Proapoptotic effect of TRAIL alone or in combination with conventional CT | TRAIL: 20% apoptotic rate TRAIL-DOX: 90–95% apoptotic rate |
| Fong et al. [25] 2006 | In vitro | HIF-1α | 2-ME | 0–20 μM | Mechanism of antitumor activity of 2 ME on human chondrosarcoma | Cells accumulated in the G0/G1 phase in response to 2 ME and DAPI stain indicated an induction of apoptosis |
| Schrage et al. [26] 2009 | In vitro | PDGFR | Imatinib, Dasatinib | 1.0–100 μmol/L, 5.0–1.0 μmol/L | Molecular targets for systemic treatment of chondrosarcoma using kinome profiling | Dasatinib: 50% apoptotic rate chondrosarcoma does not respond to imatinib treatment in vitro |
| Schrage et al. [27] 2009 | In vitro | COX-2 | Celecoxib | 5–25 μM | Effect of selective COX-2 inhibition on chondrosarcoma growth | COX-2 inhibitors decrease the proliferation of chondrosarcoma in vitro |
| Cheong et al. [28] 2011 | In vitro | DR4, DR5, TRID, TRUNDD, osteoprotegerin | TRAIL | 10–20 ng/mL | Proapoptotic effect of TRAIL alone or in combination with proteosome inhibitor MG132 | TRAIL: 20% apoptotic rate TRAIL-MG132: 60% apoptotic rate |
| Miladi et al. [29] 2017 | In vitro | MMP | QA-Dox | 25–300 µM | MMP inhibitors were conjugated with a QA function as a targeting ligand to proteoglycans of the chondrosarcoma extracellular matrix | In the chondrosarcoma model, the MMP13 inhibitor Dox and its QA derivative are promising as adjuvant therapies for chondrosarcoma management |
| Higuchi et al. [30] 2022 | In vitro | COX-1 and COX-2 | Zaltoprofen | 0–400 µmol/L | Expression of PPARγ at the mRNA and protein levels, following the induction of PPARγ-activating factors | Inhibition of proliferation of H-EMC-S5 cells observed in vitro |
| NCT Number | Year | Phase | Agent Classes | Agents | Target |
|---|---|---|---|---|---|
| NCT01267955 | 2010 | II | Hh pathway inhibitor | Vismodegib | Smo |
| NCT01883518 | 2013 | I–II | Cell therapy | Autologous dendritic cell vaccine | TA |
| NCT02821507 | 2014 | II | mTOR inhibitor, CT | Sirolimus, Cyclophosphamide | mTOR |
| NCT03277924 | 2017 | I–II | Antiangiogenic, PD-L1 inhibitor, CT | Sunitinib, Nivolumab, Epirubicin, Ifosfamide, Doxorubicin, Dacarbazine, Cisplatin, Methotrexate | RTKs PD-1 |
| NCT02982486 | 2017 | II | CTLA-4 inhibitor, PD-L1 inhibitor | Ipilimumab Nivolumab | CTLA-4, PD-L1 |
| NCT03474640 | 2018 | I | PD-1 inhibitor | Toripalimab | PD-1 |
| NCT03449108 | 2018 | II | Recombinant IL-2, cell therapy, CT, CTLA-4 inhibitor, PD-L1 inhibitor | Aldesleukin, Autologous tumor-infiltrating lymphocytes LN-145, Autologous tumor-infiltrating lymphocytes LN-145-S1, Cyclophosphamide, Fludarabine, Ipilimumab, Nivolumab | IL-2Rβ CTLA-4 PD-L1 |
| NCT03715933 | 2018 | I | Antibody targeting DR5, CT | INBRX-109 Carboplatin Cisplatin Pemetrexed 5-fluorouracil Irinotecan Temozolomide | DR5 |
| NCT03684811 | 2018 | I–II | IDH1 inhibitor | FT-2102 + azacitidine | IDH1 |
| NCT03670069 | 2019 | I | JAK-1 inhibitor | Itacitinib | JAK-1 |
| NCT04040205 | 2019 | II | CDK4/6 inhibitor | Abemaciclib | CDK4/6 |
| NCT04278781 | 2020 | II | IDH1 inhibitor | AG-120 | IDH1 |
| NCT04340843 | 2020 | II | HDAC inhibitor, antimetabolites | Belinostat, Decitabine, Cedazuridine, Guadecitabine | HDAC |
| NCT04553692 | 2020 | I | Antibody targeting DR5, CT SMAC, inhibitor of IAP, BCL2 inhibitor | IGM-8444 (Aplitibart) FOLFIRI Bevacizumab (and approved biosimilars) Birinapant Venetoclax Gemcitabine Docetaxel Azacitidine | DR5 IAP BCL2 |
| NCT04690725 | 2020 | I–II | PI3Ka inhibitor | TQB3525 | PI3Ka |
| NCT04521686 | 2020 | I | IDH1 and IDH2 inhibitor | LY3410738 | IDH1 and IDH2 |
| NCT05131386 | 2021 | II | CT | Trabectedin | DNA |
| NCT04762602 | 2021 | I | IDH1 and IDH2 inhibitor | HMPL-306 | IDH1 and IDH2 |
| NCT05039801 | 2021 | I | Glutaminase-1 inhibitor, PD-1 inhibitor | IPN60090 Bevacizumab Paclitaxel Capivasertib | Glutaminase-1 PD-1 |
| NCT04950075 | 2021 | II | Tetravalent DR5 agonistic antibody | INBRX-109 | DR5 |
3.2.3. Ongoing Clinical Trials
4. Discussion
4.1. Targeted Therapies for Skull Base Chondrosarcomas
4.1.1. Trabectedin and Genomic Landscapes
4.1.2. Angiogenesis and Anti-Angiogenic Therapies
4.1.3. Growth Factor Receptors: Therapeutic Target
4.1.4. Immunotherapy Approaches
4.1.5. IDH Mutations and Related Pathways Alteration
4.1.6. Epigenetic Vulnerabilities
4.1.7. Hippo-YAP/TAZ Signaling Pathway
4.2. Challenges, Considerations, and Future Developments
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

References
- Gazendam, A.; Popovic, S.; Parasu, N.; Ghert, M. Chondrosarcoma: A Clinical Review. J. Clin. Med. 2023, 12, 2506. [Google Scholar] [CrossRef]
- Kremenevski, N.; Schlaffer, S.-M.; Coras, R.; Kinfe, T.M.; Graillon, T.; Buchfelder, M. Skull Base Chordomas and Chondrosarcomas. Neuroendocrinology 2020, 110, 836–847. [Google Scholar] [CrossRef] [PubMed]
- Jami, S.A.; Jiandang, S.; Hao, L.C.; Xi, Z.; Wenqi, Y.; Zhou, Z. Comparison of chondrosarcoma cases: Current clinical situations among institutions. Int. J. Health Sci. 2021, 15, 42–49. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8265302/ (accessed on 1 February 2024).
- Palmisciano, P.; Haider, A.S.; Sabahi, M.; Nwagwu, C.D.; Bin Alamer, O.; Scalia, G.; Umana, G.E.; Cohen-Gadol, A.A.; El Ahmadieh, T.Y.; Yu, K.; et al. Primary Skull Base Chondrosarcomas: A Systematic Review. Cancers 2021, 13, 5960. [Google Scholar] [CrossRef]
- Sbaihat, A.; Bacciu, A.; Pasanisi, E.; Sanna, M. Skull base chondrosarcomas: Surgical treatment and results. Ann. Otol. Rhinol. Laryngol. 2013, 122, 763–770. [Google Scholar] [CrossRef] [PubMed]
- Zając, A.E.; Kopeć, S.; Szostakowski, B.; Spałek, M.J.; Fiedorowicz, M.; Bylina, E.; Filipowicz, P.; Szumera-Ciećkiewicz, A.; Tysarowski, A.; Czarnecka, A.M.; et al. Chondrosarcoma-from Molecular Pathology to Novel Therapies. Cancers 2021, 13, 2390. [Google Scholar] [CrossRef]
- Micaily, I.; Roche, M.; Ibrahim, M.Y.; Martinez-Outschoorn, U.; Mallick, A.B. Metabolic Pathways and Targets in Chondrosarcoma. Front. Oncol. 2021, 11, 772263. [Google Scholar] [CrossRef] [PubMed]
- Miwa, S.; Yamamoto, N.; Hayashi, K.; Takeuchi, A.; Igarashi, K.; Tsuchiya, H. Therapeutic Targets and Emerging Treatments in Advanced Chondrosarcoma. Int. J. Mol. Sci. 2022, 23, 1096. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews Systematic reviews and Meta-Analyses. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- The Newcastle–Ottawa Scale (NOS) for Assessing the Quality of Non-Randomized Studies in Meta-Analysis. Available online: https://www.researchgate.net/publication/261773681_The_Newcastle-Ottawa_Scale_NOS_for_Assessing_the_Quality_of_Non-Randomized_Studies_in_Meta-Analysis (accessed on 19 July 2023).
- Schuetze, S.M.; Bolejack, V.; Choy, E.; Ganjoo, K.N.; Staddon, A.P.; Chow, W.A.; Tawbi, H.A.; Samuels, B.L.; Patel, S.R.; von Mehren, M.; et al. Phase 2 study of dasatinib in patients with alveolar soft part sarcoma, chondrosarcoma, chordoma, epithelioid sarcoma, or solitary fibrous tumor. Cancer 2017, 123, 90–97. [Google Scholar] [CrossRef]
- Duffaud, F.; Italiano, A.; Bompas, E.; Rios, M.; Penel, N.; Mir, O.; Piperno-Neumann, S.; Chevreau, C.; Delcambre, C.; Bertucci, F.; et al. Efficacy and safety of regorafenib in patients with metastatic or locally advanced chondrosarcoma: Results of a non-comparative, randomised, double-blind, placebo controlled, multicentre phase II study. Eur. J. Cancer 2021, 150, 108–118. [Google Scholar] [CrossRef] [PubMed]
- Herbst, R.S.; Eckhardt, S.G.; Kurzrock, R.; Ebbinghaus, S.; O’Dwyer, P.J.; Gordon, M.S.; Novotny, W.; Goldwasser, M.A.; Tohnya, T.M.; Lum, B.L.; et al. Phase I dose-escalation study of recombinant human Apo2L/TRAIL, a dual proapoptotic receptor agonist, in patients with advanced cancer. J. Clin. Oncol. 2010, 28, 2839–2846. [Google Scholar] [CrossRef] [PubMed]
- Grignani, G.; Palmerini, E.; Stacchiotti, S.; Boglione, A.; Ferraresi, V.; Frustaci, S.; Comandone, A.; Casali, P.G.; Ferrari, S.; Aglietta, M. A phase 2 trial of imatinib mesylate in patients with recurrent nonresectable chondrosarcomas expressing platelet-derived growth factor receptor-α or -β: An Italian Sarcoma Group study. Cancer 2011, 117, 826–831. [Google Scholar] [CrossRef] [PubMed]
- Subbiah, V.; Brown, R.E.; Buryanek, J.; Trent, J.; Ashkenazi, A.; Herbst, R.; Kurzrock, R. Targeting the apoptotic pathway in chondrosarcoma using recombinant human Apo2L/TRAIL (dulanermin), a dual proapoptotic receptor (DR4/DR5) agonist. Mol. Cancer Ther. 2012, 11, 2541–2546. [Google Scholar] [CrossRef] [PubMed]
- Cixutumumab and Temsirolimus for Patients with Bone and Soft-Tissue Sarcoma: A Multicentre, Open-Label, Phase 2 Trial—PubMed. Available online: https://pubmed-ncbi-nlm-nih-gov.proxy.unibs.it/23477833/ (accessed on 31 January 2024).
- Italiano, A.; Le Cesne, A.; Bellera, C.; Piperno-Neumann, S.; Duffaud, F.; Penel, N.; Cassier, P.; Domont, J.; Takebe, N.; Kind, M.; et al. GDC-0449 in patients with advanced chondrosarcomas: A French Sarcoma Group/US and French National Cancer Institute Single-Arm Phase II Collaborative Study. Ann. Oncol. 2013, 24, 2922–2926. [Google Scholar] [CrossRef] [PubMed]
- Paoluzzi, L.; Cacavio, A.; Ghesani, M.; Karambelkar, A.; Rapkiewicz, A.; Weber, J.; Rosen, G. Response to anti-PD1 therapy with nivolumab in metastatic sarcomas. Clin. Sarcoma Res. 2016, 6, 24. [Google Scholar] [CrossRef] [PubMed]
- Tawbi, H.A.; Burgess, M.; Bolejack, V.; Van Tine, B.A.; Schuetze, S.M.; Hu, J.; D’Angelo, S.; Attia, S.; Riedel, R.F.; Priebat, D.A.; et al. Pembrolizumab in advanced soft-tissue sarcoma and bone sarcoma (SARC028): A multicentre, two-cohort, single-arm, open-label, phase 2 trial. Lancet Oncol. 2017, 18, 1493–1501. [Google Scholar] [CrossRef] [PubMed]
- Bupathi, M.; Hays, J.L.; Chen, J.L. Temozolomide post pazopanib treatment failure in patients with advanced sarcoma: A case series. PLoS ONE 2017, 12, e0188116. [Google Scholar] [CrossRef]
- Chow, W.; Frankel, P.; Ruel, C.; Araujo, D.M.; Milhem, M.; Okuno, S.; Hartner, L.; Undevia, S.; Staddon, A. Results of a prospective phase 2 study of pazopanib in patients with surgically unresectable or metastatic chondrosarcoma. Cancer 2020, 126, 105–111. [Google Scholar] [CrossRef]
- Xie, L.; Xu, J.; Sun, X.; Liu, K.; Li, X.; He, F.; Liu, X.; Gu, J.; Lv, Z.; Yang, R.; et al. Apatinib for Treatment of Inoperable Metastatic or Locally Advanced Chondrosarcoma: What We Can Learn about the Biological Behavior of Chondrosarcoma from a Two-Center Study. Cancer Manag. Res. 2020, 12, 3513–3525. [Google Scholar] [CrossRef]
- Tap, W.D.; Villalobos, V.M.; Cote, G.M.; Burris, H.; Janku, F.; Mir, O.; Beeram, M.; Wagner, A.J.; Jiang, L.; Wu, B.; et al. Phase I Study of the Mutant IDH1 Inhibitor Ivosidenib: Safety and Clinical Activity in Patients with Advanced Chondrosarcoma. J. Clin. Oncol. 2020, 38, 1693–1701. [Google Scholar] [CrossRef] [PubMed]
- Tomek, S.; Koestler, W.; Horak, P.; Grunt, T.; Brodowicz, T.; Pribill, I.; Halaschek, J.; Haller, G.; Wiltschke, C.; Zielinski, C.; et al. Trail-induced apoptosis and interaction with cytotoxic agents in soft tissue sarcoma cell lines. Eur. J. Cancer 2003, 39, 1318–1329. [Google Scholar] [CrossRef] [PubMed]
- Fong, Y.; Yang, W.; Hsu, S.; Hsu, H.; Tseng, K.; Hsu, C.; Lee, C.; Scully, S.P. 2-methoxyestradiol induces apoptosis and cell cycle arrest in human chondrosarcoma cells. J. Orthop. Res. 2007, 25, 1106–1114. [Google Scholar] [CrossRef] [PubMed]
- Schrage, Y.; Machado, I.; Meijer, D.; Bruijn, I.B.-D.; Akker, B.v.D.; Taminiau, A.; Kalinski, T.; Llombart-Bosch, A.; Bovée, J. COX-2 expression in chondrosarcoma: A role for celecoxib treatment? Eur. J. Cancer 2010, 46, 616–624. [Google Scholar] [CrossRef] [PubMed]
- Schrage, Y.M.; Bruijn, I.H.B.-D.; de Miranda, N.F.; van Oosterwijk, J.; Taminiau, A.H.; van Wezel, T.; Hogendoorn, P.C.; Bovée, J.V. Kinome profiling of chondrosarcoma reveals Src-pathway activity and dasatinib as option for treatment. Cancer Res 2009, 69, 6216–6222. [Google Scholar] [CrossRef] [PubMed]
- Cheong, H.-J.; Lee, K.S.; Woo, I.S.; Won, J.-H.; Byun, J.H. Up-regulation of the DR5 expression by proteasome inhibitor MG132 augments TRAIL-induced apoptosis in soft tissue sarcoma cell lines. Cancer Res. Treat. 2011, 43, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Miladi, I.; Vivier, M.; Dauplat, M.-M.; Chatard, M.; Besse, S.; Vidal, A.; Chassain, K.; Jean, B.; Forestier, C.; Chezal, J.-M.; et al. Doxycycline and its quaternary ammonium derivative for adjuvant therapies of chondrosarcoma. Cancer Chemother. Pharmacol. 2017, 80, 517–526. [Google Scholar] [CrossRef]
- Higuchi, T.; Takeuchi, A.; Munesue, S.; Yamamoto, N.; Hayashi, K.; Harashima, A.; Yamamoto, Y.; Tsuchiya, H. A nonsteroidal anti-inflammatory drug, zaltoprofen, inhibits the growth of extraskeletal chondrosarcoma cells by inducing PPARγ, p21, p27, and p53. Cell Cycle 2023, 22, 939–950. [Google Scholar] [CrossRef]
- Morioka, H.; Takahashi, S.; Araki, N.; Sugiura, H.; Ueda, T.; Takahashi, M.; Yonemoto, T.; Hiraga, H.; Hiruma, T.; Kunisada, T.; et al. Results of sub-analysis of a phase 2 study on trabectedin treatment for extraskeletal myxoid chondrosarcoma and mesenchymal chondrosarcoma. BMC Cancer 2016, 16, 479. [Google Scholar] [CrossRef]
- Nacev, B.A.; Sanchez-Vega, F.; Smith, S.A.; Antonescu, C.R.; Rosenbaum, E.; Shi, H.; Tang, C.; Socci, N.D.; Rana, S.; Gularte-Mérida, R.; et al. Clinical sequencing of soft tissue and bone sarcomas delineates diverse genomic landscapes and potential therapeutic targets. Nat. Commun. 2022, 13, 3405. [Google Scholar] [CrossRef]
- Thornton, K. Trabectedin: The evidence for its place in therapy in the treatment of soft tissue sarcoma. Core Évid. 2009, 4, 191–198. [Google Scholar] [CrossRef] [PubMed]
- McGough, R.L.; Aswad, B.I.; Terek, R.M. Pathologic neovascularization in cartilage tumors. Clin. Orthop. Relat. Res. 2002, 397, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Ayala, G.; Liu, C.; Nicosia, R.; Horowitz, S.; Lackman, R. Microvasculature and VEGF expression in cartilaginous tumors. Hum. Pathol. 2000, 31, 341–346. [Google Scholar] [CrossRef] [PubMed]
- van der Graaf, W.T.; Blay, J.-Y.; Chawla, S.P.; Kim, D.-W.; Bui-Nguyen, B.; Casali, P.G.; Schöffski, P.; Aglietta, M.; Staddon, A.P.; Beppu, Y.; et al. Pazopanib for metastatic soft-tissue sarcoma (PALETTE): A randomised, double-blind, placebo-controlled phase 3 trial. Lancet 2012, 379, 1879–1886. [Google Scholar] [CrossRef] [PubMed]
- Li, S. Anlotinib: A Novel Targeted Drug for Bone and Soft Tissue Sarcoma. Front. Oncol. 2021, 11, 664853. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.L.; Katz, D.; Loggers, E.T.; Davidson, D.; Rodler, E.T.; Pollack, S.M. Clinical benefit of antiangiogenic therapy in advanced and metastatic chondrosarcoma. Med. Oncol. 2017, 34, 167. [Google Scholar] [CrossRef] [PubMed]
- Paniagua, R.T.; Sharpe, O.; Ho, P.P.; Chan, S.M.; Chang, A.; Higgins, J.P.; Tomooka, B.H.; Thomas, F.M.; Song, J.J.; Goodman, S.B.; et al. Selective tyrosine kinase inhibition by imatinib mesylate for the treatment of autoimmune arthritis. J. Clin. Investig. 2006, 116, 2633–2642. [Google Scholar] [CrossRef]
- Gobin, B.; Moriceau, G.; Ory, B.; Charrier, C.; Brion, R.; Blanchard, F.; Redini, F.; Heymann, D. Imatinib Mesylate Exerts Anti-Proliferative Effects on Osteosarcoma Cells and Inhibits the Tumour Growth in Immunocompetent Murine Models. PLoS ONE 2014, 9, e90795. [Google Scholar] [CrossRef]
- Ettrich, T.J.; Seufferlein, T. Regorafenib. Recent Results Cancer Res. 2018, 211, 45–56. [Google Scholar] [CrossRef]
- Wilhelm, S.M.; Dumas, J.; Adnane, L.; Lynch, M.; Carter, C.A.; Schütz, G.; Thierauch, K.; Zopf, D. Regorafenib (BAY 73-4506): A new oral multikinase inhibitor of angiogenic, stromal and oncogenic receptor tyrosine kinases with potent preclinical antitumor activity. Int. J. Cancer 2011, 129, 245–255. [Google Scholar] [CrossRef]
- Iqbal, N.; Iqbal, N. Imatinib: A Breakthrough of Targeted Therapy in Cancer. Chemother. Res. Pract. 2014, 2014, 357027. [Google Scholar] [CrossRef] [PubMed]
- Blanke, C.D.; Rankin, C.; Demetri, G.D.; Ryan, C.W.; von Mehren, M.; Benjamin, R.S.; Raymond, A.K.; Bramwell, V.H.; Baker, L.H.; Maki, R.G.; et al. Phase III randomized, intergroup trial assessing imatinib mesylate at two dose levels in patients with unresectable or metastatic gastrointestinal stromal tumors expressing the kit receptor tyrosine kinase: S0033. J. Clin. Oncol. 2008, 26, 626–632. [Google Scholar] [CrossRef] [PubMed]
- Traylor, J.I.; Pernik, M.N.; Plitt, A.R.; Lim, M.; Garzon-Muvdi, T. Immunotherapy for Chordoma and Chondrosarcoma: Current Evidence. Cancers 2021, 13, 2408. [Google Scholar] [CrossRef] [PubMed]
- Rock, A.; Ali, S.; Chow, W.A. Systemic Therapy for Chondrosarcoma. Curr. Treat. Options Oncol. 2022, 23, 199–209. [Google Scholar] [CrossRef] [PubMed]
- Schwab, J.H.; Boland, P.J.; Agaram, N.P.; Socci, N.D.; Guo, T.; O’toole, G.C.; Wang, X.; Ostroumov, E.; Hunter, C.J.; Block, J.A.; et al. Chordoma and chondrosarcoma gene profile: Implications for immunotherapy. Cancer Immunol. Immunother. 2009, 58, 339–349. [Google Scholar] [CrossRef] [PubMed]
- Heymann, M.; Schiavone, K.; Heymann, D. Bone sarcomas in the immunotherapy era. Br. J. Pharmacol. 2021, 178, 1955–1972. [Google Scholar] [CrossRef] [PubMed]
- Amary, M.F.; Bacsi, K.; Maggiani, F.; Damato, S.; Halai, D.; Berisha, F.; Pollock, R.; O’Donnell, P.; Grigoriadis, A.; Diss, T.; et al. IDH1 and IDH2 mutations are frequent events in central chondrosarcoma and central and periosteal chondromas but not in other mesenchymal tumours. J. Pathol. 2011, 224, 334–343. [Google Scholar] [CrossRef]
- Schaap, F.G.; French, P.J.; Bovée, J.V.M.G. Mutations in the isocitrate dehydrogenase genes IDH1 and IDH2 in tumors. Adv. Anat. Pathol. 2013, 20, 32–38. [Google Scholar] [CrossRef]
- Yang, H.; Ye, D.; Guan, K.-L.; Xiong, Y. IDH1 and IDH2 mutations in tumorigenesis: Mechanistic insights and clinical perspectives. Clin. Cancer Res. 2012, 18, 5562–5571. [Google Scholar] [CrossRef]
- Pirozzi, C.J.; Yan, H. The implications of IDH mutations for cancer development and therapy. Nat. Rev. Clin. Oncol. 2021, 18, 645–661. [Google Scholar] [CrossRef]
- Tian, W.; Zhang, W.; Wang, Y.; Jin, R.; Wang, Y.; Guo, H.; Tang, Y.; Yao, X. Recent advances of IDH1 mutant inhibitor in cancer therapy. Front. Pharmacol. 2022, 13, 982424. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Zhu, G.; Yang, Z.; Zeng, K.; Liu, F.; Sun, J. Expression of PD-L1/PD-L2 is associated with high proliferation index of Ki-67 but not with TP53 overexpression in chondrosarcoma. Int. J. Biol. Markers 2018, 33, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Richert, I.; Gomez-Brouchet, A.; Bouvier, C.; Pinieux, G.D.B.D.; Karanian, M.; Blay, J.-Y.; Dutour, A. The immune landscape of chondrosarcoma reveals an immunosuppressive environment in the dedifferentiated subtypes and exposes CSFR1+ macrophages as a promising therapeutic target. J. Bone Oncol. 2020, 20, 100271. [Google Scholar] [CrossRef] [PubMed]
- Simard, F.A.; Richert, I.; Vandermoeten, A.; Decouvelaere, A.-V.; Michot, J.-P.; Caux, C.; Blay, J.-Y.; Dutour, A. Description of the immune microenvironment of chondrosarcoma and contribution to progression. OncoImmunology 2017, 6, e1265716. [Google Scholar] [CrossRef] [PubMed]
- Tarpey, P.S.; Behjati, S.; Cooke, S.L.; Van Loo, P.; Wedge, D.C.; Pillay, N.; Marshall, J.; O’Meara, S.; Davies, H.; Nik-Zainal, S.; et al. Frequent mutation of the major cartilage collagen gene COL2A1 in chondrosarcoma. Nat. Genet. 2013, 45, 923–926. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.-X.; van Oosterwijk, J.G.; Sicinska, E.; Moss, S.; Remillard, S.P.; van Wezel, T.; Bühnemann, C.; Hassan, A.B.; Demetri, G.D.; Bovée, J.V.; et al. Functional profiling of receptor tyrosine kinases and downstream signaling in human chondrosarcomas identifies pathways for rational targeted therapy. Clin. Cancer Res. 2013, 19, 3796–3807. [Google Scholar] [CrossRef] [PubMed]
- Gagné, L.M.; Boulay, K.; Topisirovic, I.; Huot, M.-E.; Mallette, F.A. Oncogenic Activities of IDH1/2 Mutations: From Epigenetics to Cellular Signaling. Trends Cell Biol. 2017, 27, 738–752. [Google Scholar] [CrossRef] [PubMed]
- Venneker, S.; Kruisselbrink, A.B.; Baranski, Z.; Palubeckaite, I.; Bruijn, I.H.B.-D.; Oosting, J.; French, P.J.; Danen, E.H.J.; Bovée, J.V.M.G. Beyond the Influence of IDH Mutations: Exploring Epigenetic Vulnerabilities in Chondrosarcoma. Cancers 2020, 12, 3589. [Google Scholar] [CrossRef]
- Bereza, M.; Dembiński, M.; Zając, A.E.; Piątkowski, J.; Dudzisz-Śledź, M.; Rutkowski, P.; Czarnecka, A.M. Epigenetic Abnormalities in Chondrosarcoma. Int. J. Mol. Sci. 2023, 24, 4539. [Google Scholar] [CrossRef]
- Cheng, Y.; He, C.; Wang, M.; Ma, X.; Mo, F.; Yang, S.; Han, J.; Wei, X. Targeting epigenetic regulators for cancer therapy: Mechanisms and advances in clinical trials. Signal Transduct. Target. Ther. 2019, 4, 62. [Google Scholar] [CrossRef]
- Patnaik, E.; Madu, C.; Lu, Y. Epigenetic Modulators as Therapeutic Agents in Cancer. Int. J. Mol. Sci. 2023, 24, 14964. [Google Scholar] [CrossRef] [PubMed]
- Xiao, W.; Zhou, Q.; Wen, X.; Wang, R.; Liu, R.; Wang, T.; Shi, J.; Hu, Y.; Hou, J. Small-Molecule Inhibitors Overcome Epigenetic Reprogramming for Cancer Therapy. Front. Pharmacol. 2021, 12, 702360. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.; Ma, T.; Yu, B. Targeting epigenetic regulators to overcome drug resistance in cancers. Signal Transduct. Target. Ther. 2023, 8, 69. [Google Scholar] [CrossRef] [PubMed]
- Kan, R.L.; Chen, J.; Sallam, T. Crosstalk between epitranscriptomic and epigenetic mechanisms in gene regulation. Trends Genet. 2022, 38, 182–193. [Google Scholar] [CrossRef]
- Moroishi, T.; Park, H.W.; Qin, B.; Chen, Q.; Meng, Z.; Plouffe, S.W.; Taniguchi, K.; Yu, F.-X.; Karin, M.; Pan, D.; et al. A YAP/TAZ-induced feedback mechanism regulates Hippo pathway homeostasis. Genes Dev. 2015, 29, 1271–1284. [Google Scholar] [CrossRef]
- Fullenkamp, C.A.; Hall, S.L.; Jaber, O.I.; Pakalniskis, B.L.; Savage, E.C.; Savage, J.M.; Ofori-Amanfo, G.K.; Lambertz, A.M.; Ivins, S.D.; Stipp, C.S.; et al. TAZ and YAP are frequently activated oncoproteins in sarcomas. Oncotarget 2016, 7, 30094–30108. [Google Scholar] [CrossRef] [PubMed]
- Moya, I.M.; Halder, G. Hippo–YAP/TAZ signalling in organ regeneration and regenerative medicine. Nat. Rev. Mol. Cell Biol. 2019, 20, 211–226. [Google Scholar] [CrossRef] [PubMed]
- Kovar, H.; Bierbaumer, L.; Radic-Sarikas, B. The YAP/TAZ Pathway in Osteogenesis and Bone Sarcoma Pathogenesis. Cells 2020, 9, 972. [Google Scholar] [CrossRef]
- Salguero-Aranda, C.; Olmedo-Pelayo, J.; de Álava, E.; Amaral, A.T.; Díaz-Martín, J. Genetic Alterations and Deregulation of Hippo Pathway as a Pathogenetic Mechanism in Bone and Soft Tissue Sarcoma. Cancers 2022, 14, 6211. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agosti, E.; Zeppieri, M.; Antonietti, S.; Ius, T.; Fontanella, M.M.; Panciani, P.P. Advancing the Management of Skull Base Chondrosarcomas: A Systematic Review of Targeted Therapies. J. Pers. Med. 2024, 14, 261. https://doi.org/10.3390/jpm14030261
Agosti E, Zeppieri M, Antonietti S, Ius T, Fontanella MM, Panciani PP. Advancing the Management of Skull Base Chondrosarcomas: A Systematic Review of Targeted Therapies. Journal of Personalized Medicine. 2024; 14(3):261. https://doi.org/10.3390/jpm14030261
Chicago/Turabian StyleAgosti, Edoardo, Marco Zeppieri, Sara Antonietti, Tamara Ius, Marco Maria Fontanella, and Pier Paolo Panciani. 2024. "Advancing the Management of Skull Base Chondrosarcomas: A Systematic Review of Targeted Therapies" Journal of Personalized Medicine 14, no. 3: 261. https://doi.org/10.3390/jpm14030261
APA StyleAgosti, E., Zeppieri, M., Antonietti, S., Ius, T., Fontanella, M. M., & Panciani, P. P. (2024). Advancing the Management of Skull Base Chondrosarcomas: A Systematic Review of Targeted Therapies. Journal of Personalized Medicine, 14(3), 261. https://doi.org/10.3390/jpm14030261