
Short and Extra Short Dental Implants in Osseous Microvascular Free Flaps: A Retrospective Case Series

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
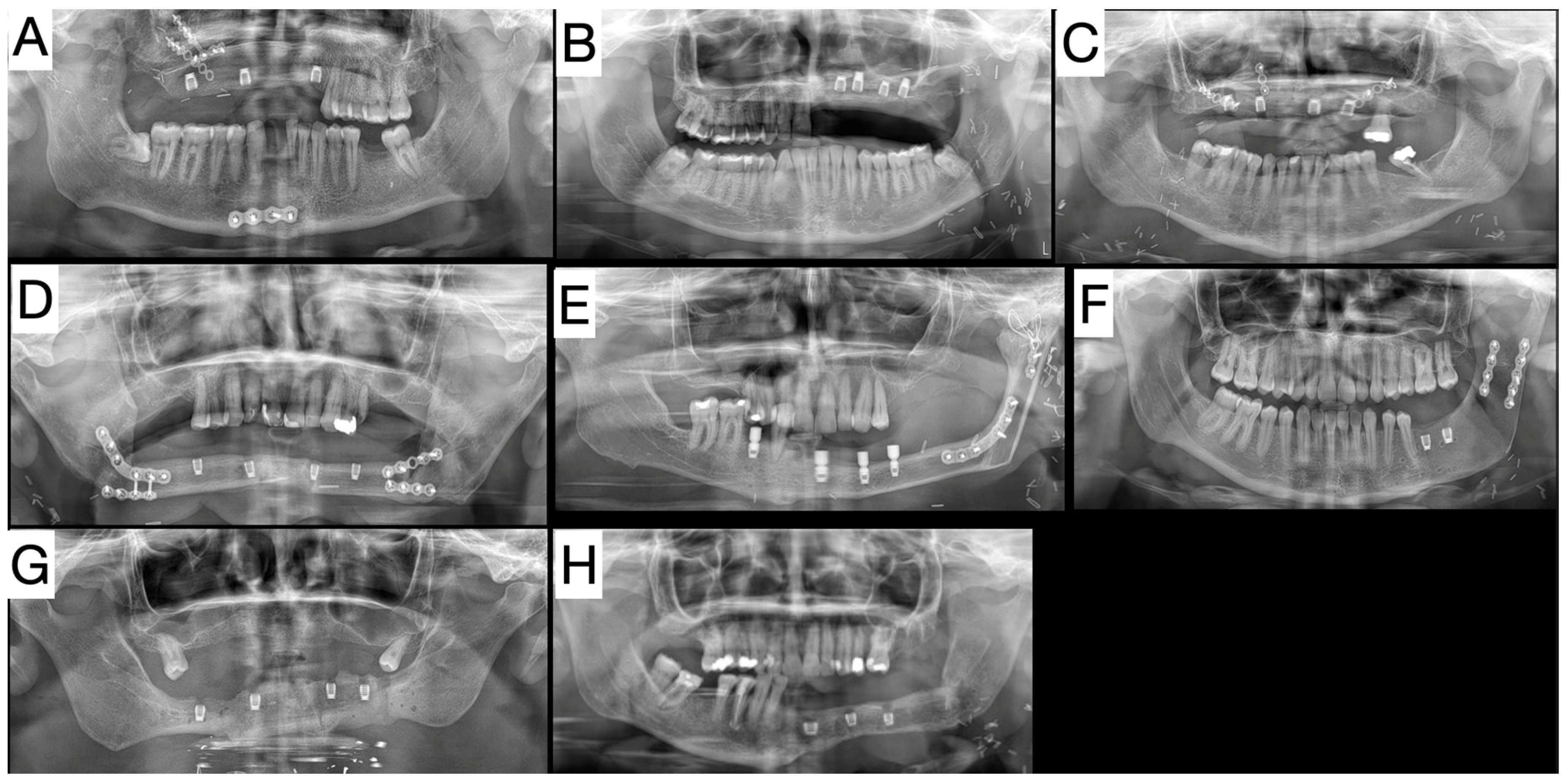
2.1. Patient 1—Case Report of Extra Short Dental Implants in Fibula Free Flap
2.2. Patient 2—Case Report of Extra Short Dental Implants in DCIA
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sahin, B.; Ulusan, M.; Basaran, B.; Gunes, S.; Oymak, E.; Genc, S. Supraclavicular artery island flap for head and neck reconstruction. Acta Chir. Plast. 2021, 63, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.R.; Ganry, L.; Ozturk, C.; Lohman, R.; Al Afif, A.; McSpadden, R.; Frias, V.; Pu, J.J. Fibula Flap Reconstruction for the Mandible: Why It Is Still the Workhorse? Atlas Oral Maxillofac. Surg. Clin. N. Am. 2023, 31, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Cebrian-Carretero, J.L.; Guinales-Diaz de Cevallos, J.; Sobrino, J.A.; Yu, T.; Burgueno-Garcia, M. Predictable dental rehabilitation in maxillomandibular reconstruction with free flaps. The role of implant guided surgery. Med. Oral Patol. Oral Cir. Bucal 2014, 19, e605–e611. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.Y.; Kim, D.D.; Ghali, G.E. Maxillofacial Reconstruction Using Vascularized Fibula Free Flaps and Endosseous Implants. Oral. Maxillofac. Surg. Clin. N. Am. 2019, 31, 259–284. [Google Scholar] [CrossRef] [PubMed]
- Barber, H.D.; Seckinger, R.J.; Hayden, R.E.; Weinstein, G.S. Evaluation of osseointegration of endosseous implants in radiated, vascularized fibula flaps to the mandible: A pilot study. J. Oral Maxillofac. Surg. 1995, 53, 640–644; discussion 644–645. [Google Scholar] [CrossRef]
- Tahmasebi, E.; Keykha, E.; Hajisadeghi, S.; Moslemi, H.; Shafiei, S.; Motamedi, M.H.K.; Torabizadeh, A.; Tabrizi, R.; Alam, M. Outcomes and influential factors in functional and dental rehabilitation following microvascular fibula flap reconstruction in the maxillomandibular region: A systematic review and meta-analysis. Maxillofac. Plast Reconstr. Surg. 2023, 45, 24. [Google Scholar] [CrossRef] [PubMed]
- Resnik, R. Misch’s Contemporary Implant Dentistry e-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Papaspyridakos, P.; Chen, C.J.; Chuang, S.K.; Weber, H.P.; Gallucci, G.O. A systematic review of biologic and technical complications with fixed implant rehabilitations for edentulous patients. Int. J. Oral Maxillofac. Implant. 2012, 27, 102–110. [Google Scholar]
- Ewers, R.; Marincola, M.; Perpetuini, P.; Morina, A.; Bergamo, E.T.P.; Cheng, Y.C.; Bonfante, E.A. Severely Atrophic Mandibles Restored with Fiber-Reinforced Composite Prostheses Supported by 5.0-mm Ultra-Short Implants Present High Survival Rates Up to Eight Years. J. Oral Maxillofac. Surg. 2022, 80, 81–92. [Google Scholar] [CrossRef] [PubMed]
- Wiesli, M.G.; Fankhauser-De Sousa, S.; Metzler, P.; Rohner, D.; Jaquiery, C. Peri-implant Parameters of Dental Implants Inserted in Prefabricated Microvascular Fibular Flaps: A Retrospective Study. Int. J. Oral Maxillofac. Implant. 2023, 38, 1151–1160. [Google Scholar] [CrossRef]
- Papanikolas, M.J.; Clark, J.R. Trends in free flap reconstruction of the head and neck: A single surgeon series of 1027 free tissue transfers. ANZ J. Surg. 2024, 94, 140–147. [Google Scholar] [CrossRef]
- Smeets, R.; Henningsen, A.; Jung, O.; Heiland, M.; Hammacher, C.; Stein, J.M. Definition, etiology, prevention and treatment of peri-implantitis—A review. Head Face Med. 2014, 10, 34. [Google Scholar] [CrossRef] [PubMed]
- Ishii, J.; Yoshida, T.; Yokoo, S.; Komori, T. Use of magnetic abutments for short endosseous implants following a fibula bone graft in an oral cancer patient: A case report. J. Oral Implantol. 2003, 29, 289–292. [Google Scholar] [CrossRef]
- Disa, J.J.; Winters, R.M.; Hidalgo, D.A. Long-term evaluation of bone mass in free fibula flap mandible reconstruction. Am. J. Surg. 1997, 174, 503–506. [Google Scholar] [CrossRef] [PubMed]
- Edher, F.; Nguyen, C.T. Short dental implants: A scoping review of the literature for patients with head and neck cancer. J. Prosthet. Dent. 2018, 119, 736–742. [Google Scholar] [CrossRef] [PubMed]
- Al-Johany, S.S.; Al Amri, M.D.; Alsaeed, S.; Alalola, B. Dental Implant Length and Diameter: A Proposed Classification Scheme. J. Prosthodont. 2017, 26, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Annibali, S.; Cristalli, M.P.; Dell’Aquila, D.; Bignozzi, I.; La Monaca, G.; Pilloni, A. Short dental implants: A systematic review. J. Dent. Res. 2012, 91, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Das Neves, F.D.; Fones, D.; Bernardes, S.R.; do Prado, C.J.; Neto, A.J. Short implants--an analysis of longitudinal studies. Int. J. Oral Maxillofac. Implant. 2006, 21, 86–93. [Google Scholar] [CrossRef]
- Hagi, D.; Deporter, D.A.; Pilliar, R.M.; Arenovich, T. A targeted review of study outcomes with short (< or = 7 mm) endosseous dental implants placed in partially edentulous patients. J. Periodontol. 2004, 75, 798–804. [Google Scholar] [CrossRef] [PubMed]
- Kotsovilis, S.; Fourmousis, I.; Karoussis, I.K.; Bamia, C. A systematic review and meta-analysis on the effect of implant length on the survival of rough-surface dental implants. J. Periodontol. 2009, 80, 1700–1718. [Google Scholar] [CrossRef]
- Menchero-Cantalejo, E.; Barona-Dorado, C.; Cantero-Alvarez, M.; Fernandez-Caliz, F.; Martinez-Gonzalez, J.M. Meta-analysis on the survival of short implants. Med. Oral Patol. Oral Cir. Bucal 2011, 16, e546–e551. [Google Scholar] [CrossRef]
- Misch, C.E. Short dental implants: A literature review and rationale for use. Dent Today 2005, 24, 64–66, 68. [Google Scholar] [PubMed]
- Jokstad, A. The evidence for endorsing the use of short dental implants remains inconclusive. Evid. Based Dent. 2011, 12, 99–101. [Google Scholar] [CrossRef] [PubMed]
- Thoma, D.S.; Zeltner, M.; Husler, J.; Hammerle, C.H.; Jung, R.E. EAO Supplement Working Group 4—EAO CC 2015 Short implants versus sinus lifting with longer implants to restore the posterior maxilla: A systematic review. Clin. Oral Implant. Res. 2015, 26 (Suppl. S11), 154–169. [Google Scholar] [CrossRef] [PubMed]
- Takushima, A.; Harii, K.; Asato, H.; Momosawa, A.; Okazaki, M.; Nakatsuka, T. Choice of osseous and osteocutaneous flaps for mandibular reconstruction. Int. J. Clin. Oncol. 2005, 10, 234–242. [Google Scholar] [CrossRef] [PubMed]
- Mashrah, M.A.; Aldhohrah, T.; Abdelrehem, A.; Sakran, K.A.; Ahmad, H.; Mahran, H.; Abu-Lohom, F.; Su, H.; Fang, Y.; Wang, L. Survival of vascularized osseous flaps in mandibular reconstruction: A network meta-analysis. PLoS ONE 2021, 16, e0257457. [Google Scholar] [CrossRef] [PubMed]
- Khadembaschi, D.; Russell, P.; Beech, N.; Batstone, M.D. Osseointegrated implant survival, success and prosthodontic outcomes in composite free flaps: A 10-year retrospective cohort study. Clin. Oral Implant. Res. 2021, 32, 1251–1261. [Google Scholar] [CrossRef] [PubMed]
- Laverty, D.P.; Addison, O.; Wubie, B.A.; Heo, G.; Parmar, S.; Martin, T.; Praveen, P.; Pearson, D.; Newsum, D.; Murphy, M.; et al. Outcomes of implant-based oral rehabilitation in head and neck oncology patients-a retrospective evaluation of a large, single regional service cohort. Int. J. Implant Dent. 2019, 5, 8. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.C.; Perpetuini, P.; Marincola, M.; Speratti, D.; Murcko, L.; Hirayama, M.; Benalcazar-Jalkh, E.B.; Bonfante, E.A. Prefabricated shouldered abutments enable successful restoration of molar crowns on implants. Clin. Implant Dent. Relat. Res. 2024; online ahead of print. [Google Scholar] [CrossRef]
- Pjetursson, B.E.; Thoma, D.; Jung, R.; Zwahlen, M.; Zembic, A. A systematic review of the survival and complication rates of implant-supported fixed dental prostheses (FDPs) after a mean observation period of at least 5 years. Clin. Oral Implant. Res. 2012, 23 (Suppl. S6), 22–38. [Google Scholar] [CrossRef]
- Ten Bruggenkate, C.M.; van der Kwast, W.A.; Oosterbeek, H.S. Success criteria in oral implantology. A review of the literature. Int. J. Oral Implantol. 1990, 7, 45–51. [Google Scholar]
- Pjetursson, B.E.; Sailer, I.; Merino-Higuera, E.; Spies, B.C.; Burkhardt, F.; Karasan, D. Systematic review evaluating the influence of the prosthetic material and prosthetic design on the clinical outcomes of implant-supported multi-unit fixed dental prosthesis in the posterior area. Clin. Oral Implant. Res. 2023, 34 (Suppl. S26), 86–103. [Google Scholar] [CrossRef]
- Attia, S.; Wiltfang, J.; Pons-Kuhnemann, J.; Wilbrand, J.F.; Streckbein, P.; Kahling, C.; Howaldt, H.P.; Schaaf, H. Survival of dental implants placed in vascularised fibula free flaps after jaw reconstruction. J. Craniomaxillofac. Surg. 2018, 46, 1205–1210. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.C.; Perpetuini, P.; Murcko, L.; Hirayama, M.; Morgan, K.; Marincola, M.; Bonfante, E.A.; Bergamo, E.T.P.; Ewers, R. Fiber-reinforced composite full-arch prosthetic reconstructions supported by three standard, short or extra-short implants: A two-center retrospective study. Clin. Oral Investig. 2023, 27, 4191–4203. [Google Scholar] [CrossRef] [PubMed]
- Thoma, D.S.; Haas, R.; Sporniak-Tutak, K.; Garcia, A.; Taylor, T.D.; Tutak, M.; Pohl, V.; Hammerle, C.H.F. Randomized controlled multi-centre study comparing shorter dental implants (6 mm) to longer dental implants (11–15 mm) in combination with sinus floor elevation procedures: 10-year data. J. Clin. Periodontol. 2024, 51, 499–509. [Google Scholar] [CrossRef] [PubMed]
- Pauletto, P.; Ruales-Carrera, E.; Mezzomo, L.A.; Stefani, C.M.; Taba, M., Jr.; Goncalves, R.B.; Flores-Mir, C.; De Luca Canto, G. Clinical performance of short versus standard dental implants in vertically augmented bone: An overview of systematic reviews. Clin. Oral Investig. 2021, 25, 6045–6068. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, G.; D’Agostino, A.; Nocini, P.F.; Signoriello, A.; Zangani, A.; Pardo, A.; Lonardi, F.; Trevisiol, L. Clinical outcomes and periodontal conditions of dental implants placed in free fibula flaps (FFF): A retrospective study with a mean follow-up of 6 years. Clin. Oral Investig. 2023, 27, 7737–7751. [Google Scholar] [CrossRef] [PubMed]
- Fathi, A.; Rismanchian, M.; Khodadadi, R.; Dezaki, S.N. Does the crown-implant ratio affect the survival and complications of implant-supported prostheses? A systematic review. J. Prosthet. Dent. 2022; in press. [Google Scholar] [CrossRef] [PubMed]
- Bonfante, E.A.; Jimbo, R.; Witek, L.; Tovar, N.; Neiva, R.; Torroni, A.; Coelho, P.G. Biomaterial and biomechanical considerations to prevent risks in implant therapy. Periodontology 2000 2019, 81, 139–151. [Google Scholar] [CrossRef]
- Coelho, P.G.; Suzuki, M.; Marin, C.; Granato, R.; Gil, L.F.; Tovar, N.; Jimbo, R.; Neiva, R.; Bonfante, E.A. Osseointegration of Plateau Root Form Implants: Unique Healing Pathway Leading to Haversian-Like Long-Term Morphology. Adv. Exp. Med. Biol. 2015, 881, 111–128. [Google Scholar] [CrossRef]
- Coelho, P.G.; Granato, R.; Marin, C.; Bonfante, E.A.; Janal, M.N.; Suzuki, M. Biomechanical and bone histomorphologic evaluation of four surfaces on plateau root form implants: An experimental study in dogs. Oral Surg. Oral Med. Oral Pathol. Oral Radiol Endod 2010, 109, e39–e45. [Google Scholar] [CrossRef]
- Coelho, P.G.; Jimbo, R. Osseointegration of metallic devices: Current trends based on implant hardware design. Arch. Biochem. Biophys. 2014, 561, 99–108. [Google Scholar] [CrossRef]
- Coelho, P.G.; Jimbo, R.; Tovar, N.; Bonfante, E.A. Osseointegration: Hierarchical designing encompassing the macrometer, micrometer, and nanometer length scales. Dent. Mater. 2015, 31, 37–52. [Google Scholar] [CrossRef]
- Coelho, P.G.; Suzuki, M.; Guimaraes, M.V.; Marin, C.; Granato, R.; Gil, J.N.; Miller, R.J. Early bone healing around different implant bulk designs and surgical techniques: A study in dogs. Clin. Implant Dent. Relat. Res. 2010, 12, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Ardisson, A.; Senna, P.; Granato, R.; Bergamo, E.; Bonfante, E.; Marin, C. Success Rate of Mandible Implants Placed in Vascularized Fibula Bone Graft: A Systematic Review. J. Oral Implantol. 2023, 49, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Dibart, S.; Warbington, M.; Su, M.F.; Skobe, Z. In vitro evaluation of the implant-abutment bacterial seal: The locking taper system. Int. J. Oral Maxillofac. Implant. 2005, 20, 732–737. [Google Scholar]
- Iezzi, G.; Perrotti, V.; Felice, P.; Barausse, C.; Piattelli, A.; Del Fabbro, M. Are <7-mm long implants in native bone as effective as longer implants in augmented bone for the rehabilitation of posterior atrophic jaws? A systematic review and meta-analysis. Clin. Implant. Dent. Relat. Res. 2020, 22, 552–566. [Google Scholar] [CrossRef] [PubMed]
- Saenz-Ravello, G.; Ossandon-Zuniga, B.; Munoz-Meza, V.; Mora-Ferraro, D.; Baeza, M.; Fan, S.; Sagheb, K.; Schiegnitz, E.; Diaz, L. Short implants compared to regular dental implants after bone augmentation in the atrophic posterior mandible: Umbrella review and meta-analysis of success outcomes. Int. J. Implant. Dent. 2023, 9, 18. [Google Scholar] [CrossRef] [PubMed]
- Barausse, C.; Pistilli, R.; Canullo, L.; Bonifazi, L.; Ferri, A.; Felice, P. A 5-year randomized controlled clinical trial comparing 4-mm ultrashort to longer implants placed in regenerated bone in the posterior atrophic jaw. Clin. Implant. Dent. Relat. Res. 2022, 24, 4–12. [Google Scholar] [CrossRef]
- Malet, J.; Mora, F.; Bouchard, P. Implant Dentistry at a Glance; John Wiley & Sons: Hoboken, NJ, USA, 2018. [Google Scholar]
- Giro, G.; Marin, C.; Granato, R.; Bonfante, E.A.; Suzuki, M.; Janal, M.N.; Coelho, P.G. Effect of drilling technique on the early integration of plateau root form endosteal implants: An experimental study in dogs. J. Oral Maxillofac. Surg. 2011, 69, 2158–2163. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex | Age at Time of Placing Dental Implants | Reconstructed Jaw | Type of Free Flap * | Number of Dental Implants in Free Flap | Implant Size (Bicon, Bicon LLC) | Status | |
|---|---|---|---|---|---|---|---|
| Patient No. 1 | Male | 67 | Mandible | FFF | 4 | 4.0 × 6.0 Integra CP | Prosthetic work in function |
| Patient No. 2 | Male | 51 | Mandible | FFF | 3 | 4.0 × 6.0 Integra CP | Adjusting prosthetic work |
| Patient No. 3 | Female | 55 | Maxilla | FFF | 4 | 4.0 × 6.5 Integra CP | Prosthetic work in function |
| Patient No. 4 | Male | 24 | Maxilla | FFF | 4 | 4.5 × 6.0 Integra CP (2×) 4.5 × 8.0 Integra CP (2×) | Prosthetic work in function |
| Patient No. 5 | Male | 26 | Maxilla | DCIA | 3 | 4.5 × 6.0 Integra CP (1×) 5.0 × 6.0 Integra CP (2×) | Prosthetic work in function |
| Patient No. 6 | Female | 21 | Mandible | DCIA | 2 | 4.5 × 6.0 Integra CP (1×) 5.0 × 6.0 Integra CP (1×) | Prosthetic work in function |
| Patient No. 7 | Male | 46 | Mandible | FFF | 4 | 5.0 × 6.0 Integra CP (4×) | Adjusting prosthetic work |
| Patient No. 8 | Female | 55 | Mandible | FFF | 3 | 4.5 × 5.0 mm Integra-CP (3×) | Loaded interim fixed prostheses |
| Implants at Risk | Time (Months) | ||||
|---|---|---|---|---|---|
| 0 | 10 | 20 | 30 | 40 | |
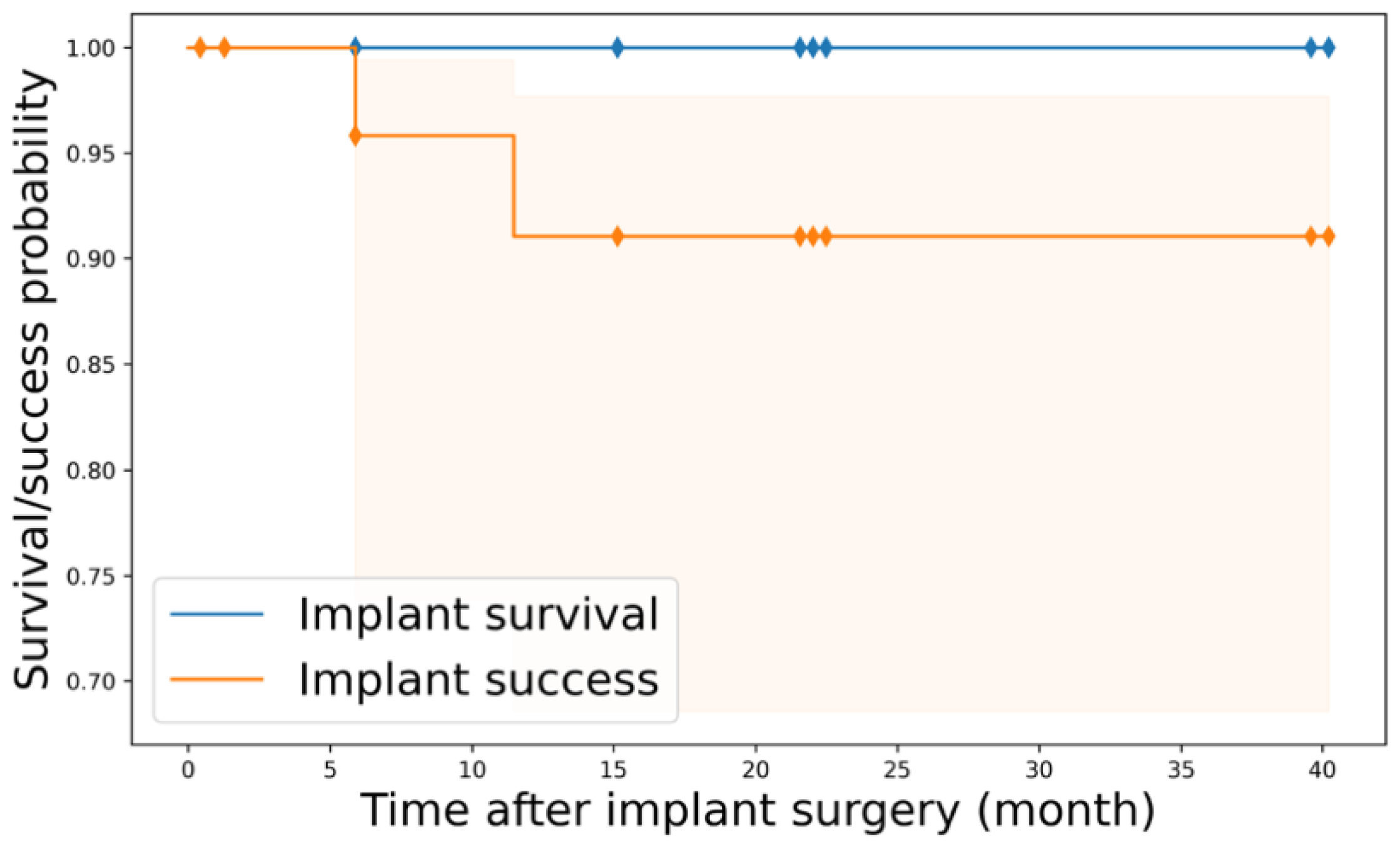
| At risk | 27 | 27 | 24 | 20 | 7 |
| Censored | 0 | 3 | 4 | 13 | 0 |
| Implant failure | 0 | 0 | 0 | 0 | 0 |
| Implant survival probability | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Implants at Risk | Time (Months) | ||||
|---|---|---|---|---|---|
| 0 | 10 | 20 | 30 | 40 | |
| At risk | 27 | 27 | 24 | 19 | 6 |
| Censored | 0 | 3 | 3 | 13 | 0 |
| Implant complication | 0 | 0 | 2 | 0 | 0 |
| Implant success probability | 1.00 | 1.00 | 0.917 | 0.917 | 0.917 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hocková, B.; Slávik, R.; Azar, B.; Stebel, J.; Poruban, D.; Bonfante, E.A.; Ewers, R.; Cheng, Y.-C.; Stebel, A. Short and Extra Short Dental Implants in Osseous Microvascular Free Flaps: A Retrospective Case Series. J. Pers. Med. 2024, 14, 384. https://doi.org/10.3390/jpm14040384
Hocková B, Slávik R, Azar B, Stebel J, Poruban D, Bonfante EA, Ewers R, Cheng Y-C, Stebel A. Short and Extra Short Dental Implants in Osseous Microvascular Free Flaps: A Retrospective Case Series. Journal of Personalized Medicine. 2024; 14(4):384. https://doi.org/10.3390/jpm14040384
Chicago/Turabian StyleHocková, Barbora, Rastislav Slávik, Basel Azar, Jakub Stebel, Dušan Poruban, Estevam A. Bonfante, Rolf Ewers, Yu-Chi Cheng, and Adam Stebel. 2024. "Short and Extra Short Dental Implants in Osseous Microvascular Free Flaps: A Retrospective Case Series" Journal of Personalized Medicine 14, no. 4: 384. https://doi.org/10.3390/jpm14040384