
Long-Term Outcomes of Patients with Biologically Treated Psoriatic Arthritis and Atopic Dermatitis—A Single-Center Experience

 and
and
Abstract
1. Introduction
2. Materials and Methods
3. Results
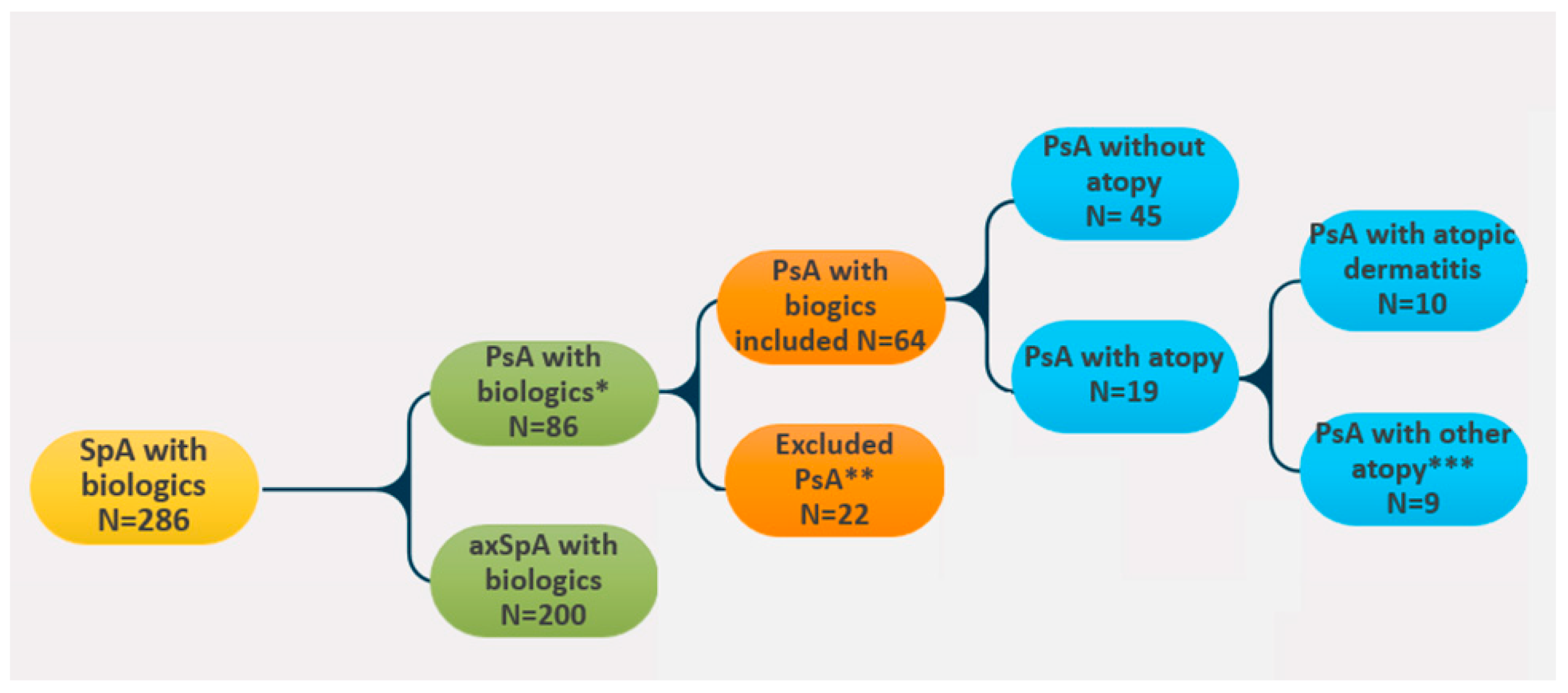
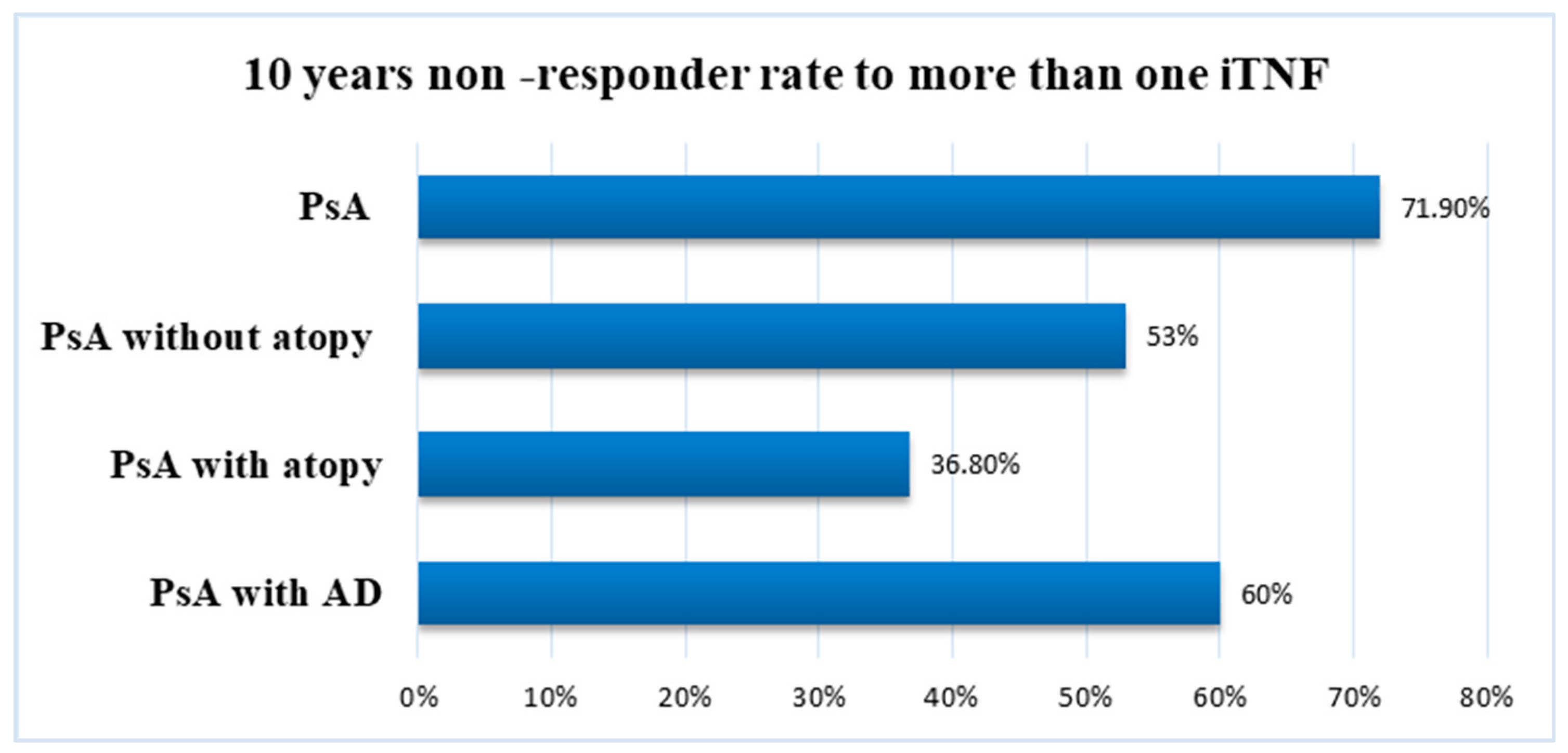
3.1. Psoriatic Arthritis under Biologics: General Findings
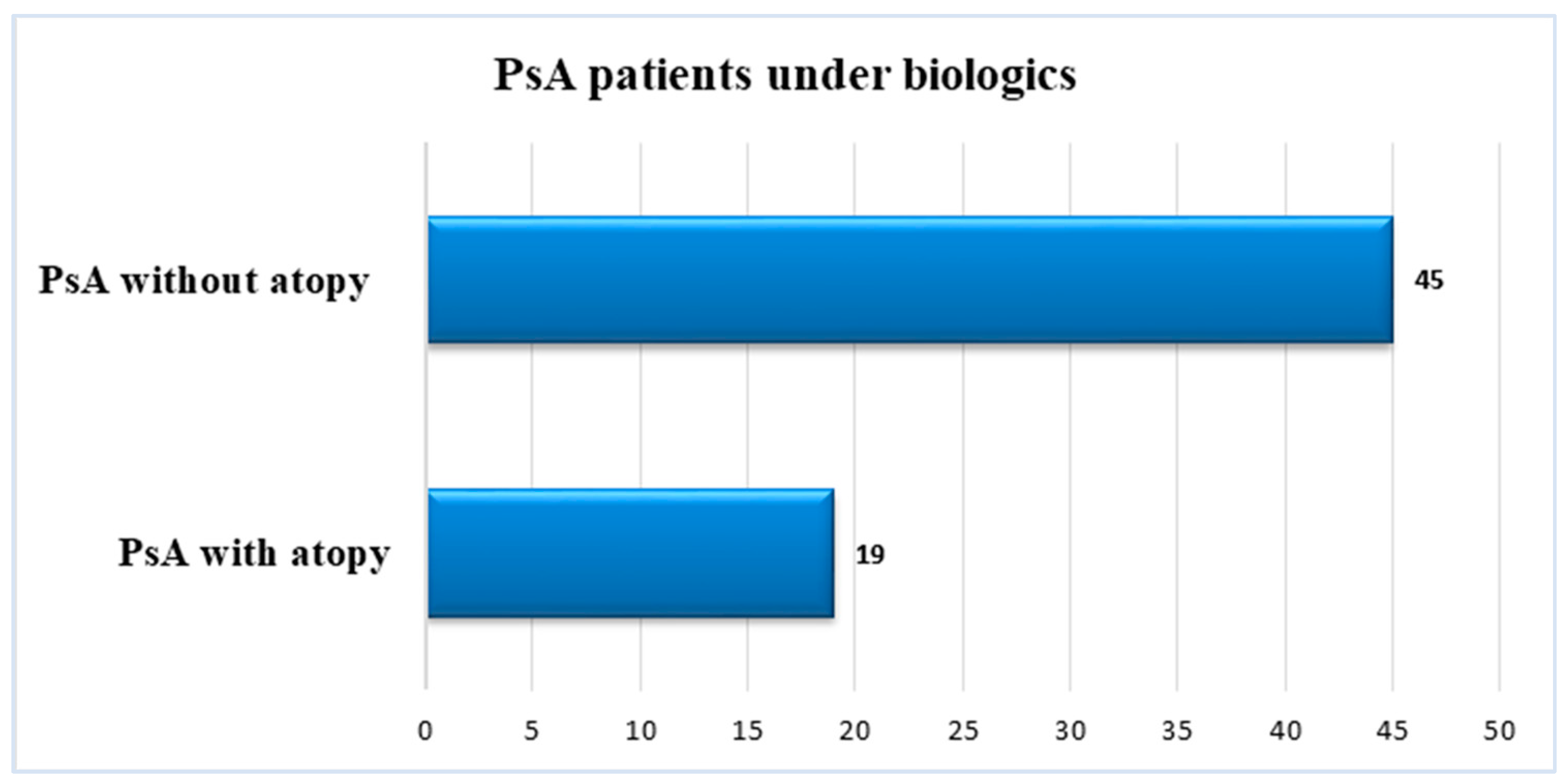
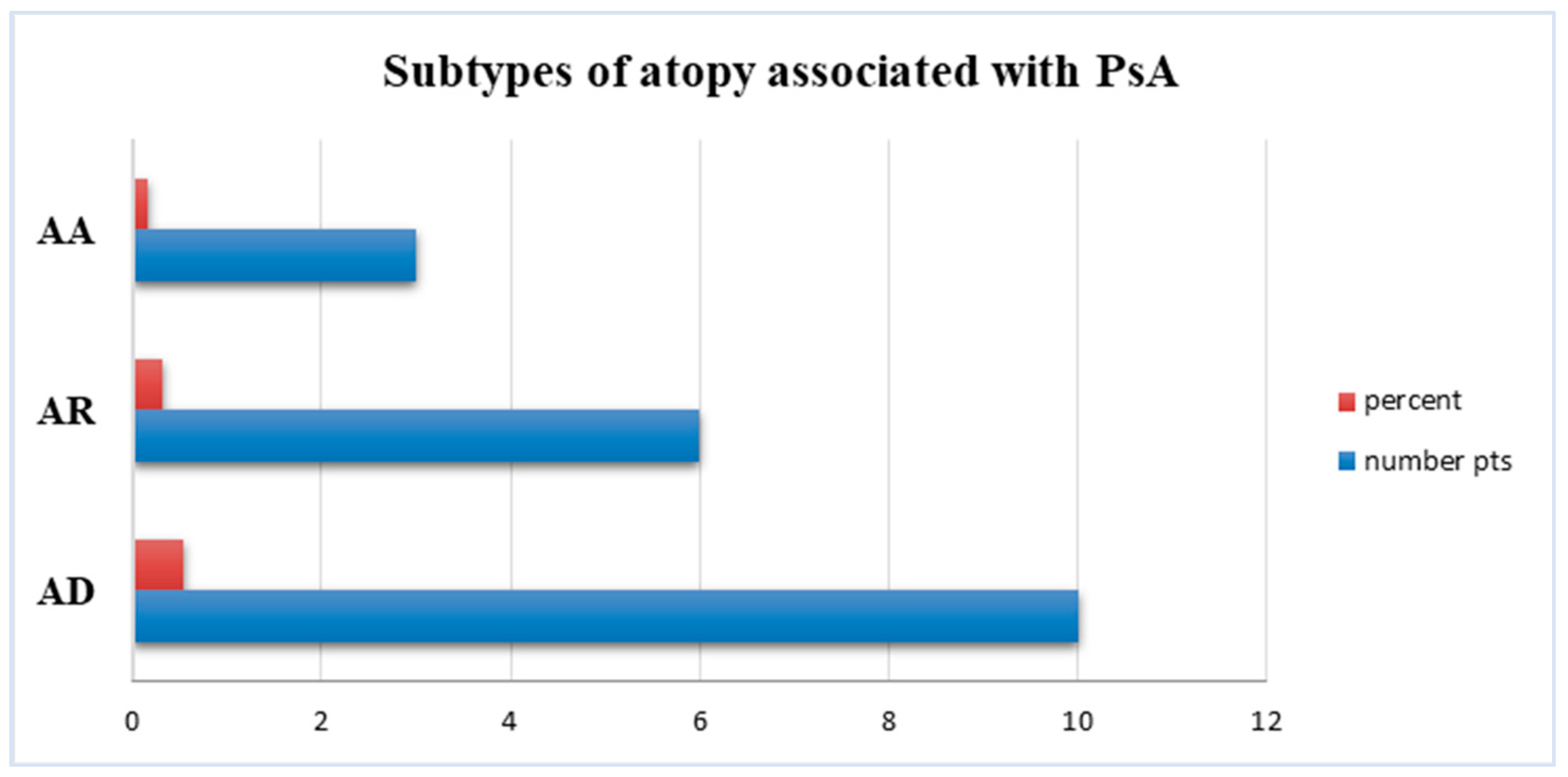
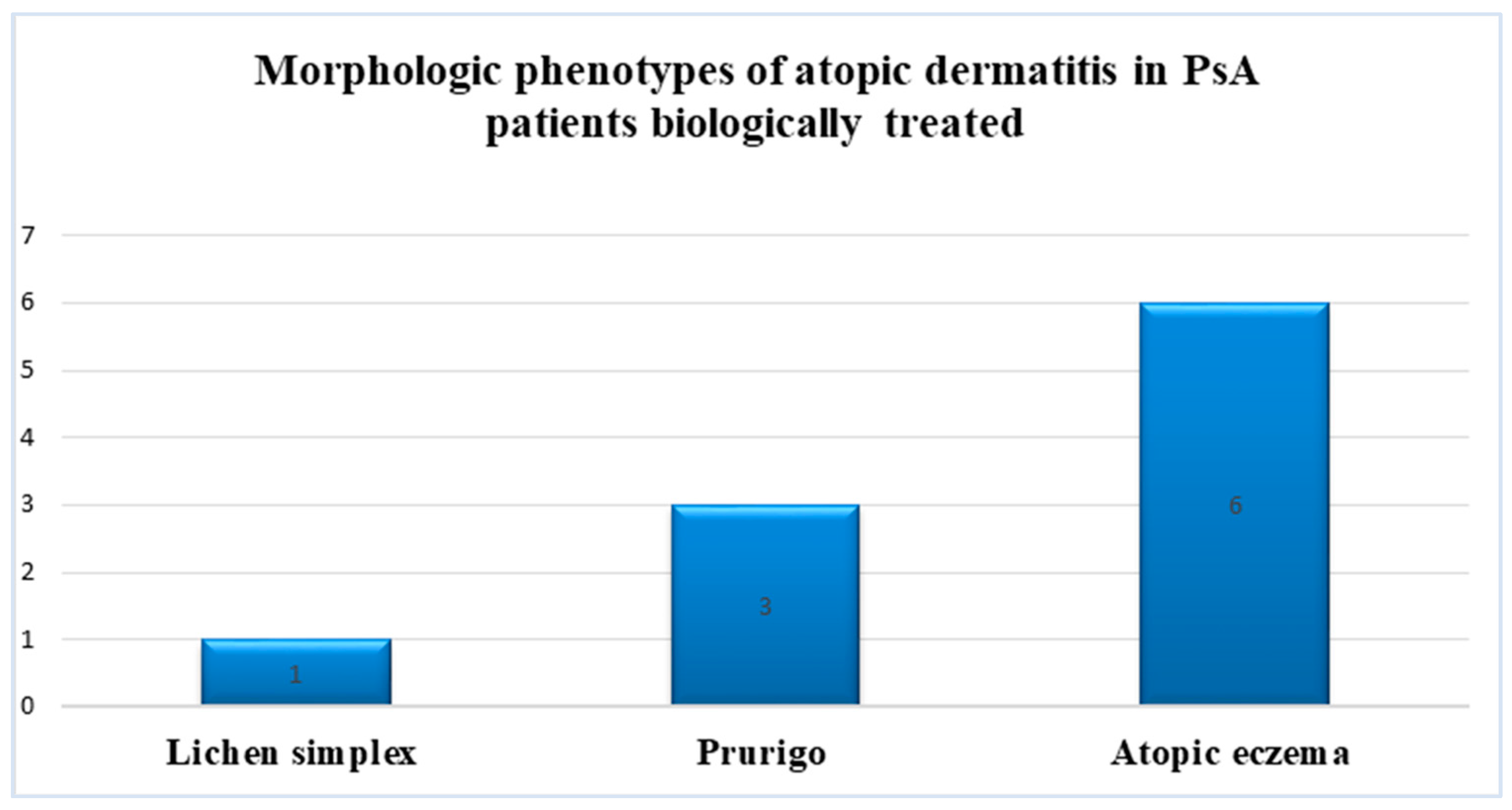
3.2. Psoriatic Arthritis and Concomitant Atopy
3.3. Psoriatic Arthritis with and without Atopy—Comparative Data
3.3.1. Demographics
3.3.2. Disease-Related Parameters
3.3.3. Treatment-Related Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Menegatti, S.; Guillemot, V.; Latis, E.; Yahia-Cherbal, H.; Mittermüller, D.; Rouilly, V.; Mascia, E.; Rosine, N.; Koturan, S.; Millot, G.A.; et al. Immune response profiling of patients with spon-dyloarthritis reveals signalling networks mediating TNF-blocker function in vivo. Ann. Rheum. Dis. 2021, 80, 475–486. [Google Scholar] [CrossRef] [PubMed]
- Stolwijk, C.; Boonen, A.; van Tubergen, A.; Reveille, J.D. Epidemiology of spondyloarthritis. Rheum. Dis. Clin. N. Am. 2012, 38, 441–476. [Google Scholar] [CrossRef]
- Tillett, W.; Costa, L.; Jadon, D.; Wallis, D.; Cavill, C.; McHUGH, J.; Korendowych, E.; McHUGH, N. The ClASsification for Psoriatic ARthritis (CASPAR) Criteria—A Retrospective Feasibility, Sensitivity, and Specificity Study. J. Rheumatol. 2012, 39, 154–156. [Google Scholar] [CrossRef]
- Zabotti, A.; De Lucia, O.; Sakellariou, G.; Batticciotto, A.; Cincinelli, G.; Giovannini, I.; Idolazzi, L.; Maioli, G.; Tinazzi, I.; Aletaha, D.; et al. Predictors, Risk Factors, and Incidence Rates of Psoriatic Arthritis Development in Psoriasis Patients: A Systematic Literature Review and Meta-Analysis. Rheumatol. Ther. 2021, 8, 1519–1534. [Google Scholar] [CrossRef]
- Gill, T.; Asquith, M.; Rosenbaum, J.T.; Colbert, R.A. The intestinal microbiome in spondyloarthritis. Curr. Opin. Rheumatol. 2015, 27, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Sharip, A.; Kunz, J. Understanding the Pathogenesis of Spondyloarthritis. Biomolecules 2020, 10, 1461. [Google Scholar] [CrossRef]
- Makos, A.; Kuiper, J.H.; Kehoe, O.; Amarasena, R. Psoriatic arthritis: Review of potential biomarkers predicting response to TNF inhibitors. Inflammopharmacology 2023, 31, 77–87. [Google Scholar] [CrossRef]
- Chen, W.-Y.; Chen, S.-C.; Hsu, S.-Y.; Lin, Y.-A.; Shih, C.-M.; Huang, C.-Y.; Wang, K.-H.; Lee, A.-W. Annoying psoriasis, and atopic dermatitis: A narrative review. J. Mol. Sci. 2022, 23, 4898. [Google Scholar] [CrossRef] [PubMed]
- Rudwaleit, M.; Andermann, B.; Alten, R.; Sörensen, H.; Listing, J.; Zink, A.; Sieper, J.; Braun, J. Atopic disorders in ankylosing spondylitis and rheumatoid arthritis. Ann. Rheum. Dis. 2002, 61, 968–974. [Google Scholar] [CrossRef]
- Chang, W.P.; Kuo, C.N.; Kuo, L.N.; Wang, Y.T.; Perng, W.T.; Kuo, H.C.; Wei, J.C.C. Increased risk of allergic diseases in patients with ankylosing spondylitis: A 10-year follow-up population-based study in Taiwan. Medicine 2016, 95, e5172. [Google Scholar] [CrossRef]
- Shen, T.-C.; Lin, C.-L.; Wei, C.-C.; Chen, C.-H.; Tu, C.-Y.; Hsia, T.-C.; Shih, C.-M.; Hsu, W.-H.; Sung, F.-C. The Risk of Asthma in Patients with Ankylosing Spondylitis: A Population-Based Cohort Study. PLoS ONE 2015, 10, e0116608. [Google Scholar] [CrossRef][Green Version]
- Strugariu, G.; Pomîrleanu, C.; Bran, C.; Costea, A.; Vicovan, A.; Tatarciuc, D.; Eșanu, I.; Ancuța, E.; Chirieac, R.; Ancuța, C. The Prevalence of Atopy in Biologically Treated Spondyloarthropathies: A Retrospective Study of 200 Patients. J. Clin. Med. 2022, 11, 55. [Google Scholar] [CrossRef] [PubMed]
- Marshall, J.S.; Warrington, R.; Watson, W.; Kim, H.L. An introduction to immunology and immunopathology. Allergy Asthma Clin. Immunol. 2018, 14, 49. [Google Scholar] [CrossRef]
- Barry, K.; Zancanaro, P.; Casseres, R.; Abdat, R.; Dumont, N.; Rosmarin, D. Concomitant atopic dermatitis and psoriasis—A retrospective review. J. Dermatol. Treat. 2021, 32, 716–720. [Google Scholar] [CrossRef]
- Cunliffe, A.; Gran, S.; Ali, U.; Grindlay, D.; Lax, S.J.; Williams, H.C.; Burden-Teh, E. Can atopic eczema and psoriasis coexist? A systematic review and meta-analysis. Skin Health Dis. 2021, 1, e29. [Google Scholar] [CrossRef] [PubMed]
- Eyerich, S.; Onken, A.T.; Weidinger, S.; Franke, A.; Nasorri, F.; Pennino, D.; Grosber, M.; Pfab, F.; Schmidt-Weber, C.B.; Mempel, M.; et al. Mutual antagonism of T cells causing psoriasis and atopic eczema. N. Engl. J. Med. 2011, 365, 231–238. [Google Scholar] [CrossRef]
- Tsoi, L.C.; Rodriguez, E.; Degenhardt, F.; Baurecht, H.; Wehkamp, U.; Volks, N.; Szymczak, S.; Swindell, W.R.; Sarkar, M.K.; Raja, K.; et al. Atopic dermatitis is an IL-13edominant disease with greater molecular heterogeneity compared to psoriasis. J. Investig. Dermatol. 2019, 139, 1480–1489. [Google Scholar] [CrossRef]
- Guttman-Yassky, E.; Krueger, J.G.; Mark, G.; Lebwohl, M.G. Systemic immune mechanisms in atopic dermatitis and psoriasis with implications for treatment. Exp. Dermatol. 2018, 27, 409–417. [Google Scholar] [CrossRef]
- Moy, A.P.; Nurali, M.M.; Kroshinsky, D.; Duncan, L.; Nazarian, R.N. Immunologic overlap of helper T-cell subtypes 17 and 22 in erytrodermic psoriasis and atopic dermatitis. JAMA Dermatol. 2015, 151, 753–760. [Google Scholar] [CrossRef]
- Rudwaleit, M.; van der Heijde, D.; Landewé, R.; Akkoc, N.; Brandt, J.; Chou, C.T.; Dougados, M.; Huang, F.; Gu, J.; Kirazli, Y.; et al. The Assessment of SpondyloArthritis International Society classification criteria for peripheral spondyloarthritis and for spondyloarthritis in general. Ann. Rheum. Dis. 2011, 70, 25–31. [Google Scholar] [CrossRef]
- Gossec, L.; Baraliakos, X.; Kerschbaumer, A.; de Wit, M.; McInnes, I.; Dougados, M.; Primdahl, J.; McGonagle, D.G.; Aletaha, D.; Balanescu, A.; et al. EULAR recommendations for the management of psoriatic arthritis with pharmacological therapies: 2019 update. Ann. Rheum. Dis. 2020, 79, 700–712. [Google Scholar] [CrossRef] [PubMed]
- Guttman-Yassky, E.; Krueger, J.G. Atopic dermatitis, and psoriasis: Two different immune diseases or one spectrum? Curr. Opin. Immunol. 2017, 48, 68–73. [Google Scholar] [CrossRef]
- Coates, L.C.; Corp, N.; van der Windt, A.D.; O’Sullivan, D.; Soriano, E.R.; Kavanaugh, A. GRAPPA Treatment Recommendations: 2021 Update. J. Rheumatol. 2022, 49 (Suppl. S1), 52–54. [Google Scholar] [CrossRef]
- Megna, M.; Potestio, L.; Angelo Ruggiero, A.; Cacciapuoti, S.; Maione, F.; Tasso, M.; Caso, C.; Costa, L. JAK Inhibitors in Psoriatic Disease. Clin. Cosmet. Investig. Dermatol. 2023, 16, 3129–3145. [Google Scholar] [CrossRef] [PubMed]
- Nash, P. Janus Kinase Inhibitors: Safety in Patients with Psoriatic Arthritis. J. Rheumatol. 2022, 49, 44–47. [Google Scholar] [CrossRef] [PubMed]
- Kamata, M.; Tada, Y. Optimal Use of Jak Inhibitors and Biologics for Atopic Dermatitis on the Basis of the Current Evidence. JID Innov. 2023, 3, 100195. [Google Scholar] [CrossRef]
- Mikhaylov, D.; Ungar, B.; Renert-Yuval, Y.; Guttman-Yassky, E. Oral Janus kinase inhibitors for atopic dermatitis. Ann. Allergy Asthma Immunol. 2023, 130, 577–592. [Google Scholar] [CrossRef]
- Georas, S.N.; Donohue, P.; Connolly, M.; Wechsler, M.E. JAK inhibitors for asthma. J. Allergy Clin. Immunol. 2021, 148, 953–963. [Google Scholar] [CrossRef] [PubMed]
- Ziade, N.; El Khoury, B.; Zoghbi, M.; Merheb, G.; Abi Karam, G.; Kamel Mroue, K.; Messaykeh, J. Prevalence and pattern of comorbidities in chronic rheumatic and musculoskeletal diseases: The COMORD study. Nat. Res. Sci. Rep. 2020, 10, 7683. [Google Scholar] [CrossRef] [PubMed]
- Haugeberg, G.; Mari Hoff, M.; Kavanaugh, A.; Michelsen, B. Psoriatic arthritis: Exploring the occurrence of sleep disturbances, fatigue, and depression and their correlates. Arthritis Res. Ther. 2020, 22, 198. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | PsA lot 64 pts n (%) | Atopic PsA 1 19 pts (29.6%) n (%) | Non-AD PsA 2 9 pts (14%) n (%) | PsA-AD 3 10 pts (15.6%) n (%) | p * < 0.05 (Chi-Square) |
|---|---|---|---|---|---|
| Gender, n (%) | |||||
| Expected total/chi-square. | |||||
| Male | 37 (57.8) | 9 (10.25) [0.15] | 4 (4.85) [0.15] | 5 (5.39) [0.03] | |
| Female | 27 (42.2) | 10 (8.75) [0.18] | 5 (4.15) [0.18] | 5 (4.61) [0.03] | 0.77 (1.1056) |
| Living style, n (%) | |||||
| Expected total/chi-square. | |||||
| Urban | 38 (59.4) | 15 (12.67) [0.43] | 8 (6.00) [0.67] | 7 (6.67) [0.02] | |
| Rural | 26 (40.6) | 4 (6.33) [0.86] | 1 (3.00) [1.33] | 3 (3.33) [0.03] | 0.18 (4.8707) |
| Age (years), n (%) | |||||
| Expected total/chi-square. | |||||
| <40 | 7 (11) | 6 (3.54) [1.71] | 3 (1.68) [1.04] | 3 (1.86) [0.69] | |
| 41–60 | 28 (44) | 7 (7.82) [0.09] | 2 (3.71) [0.79] | 5 (4.12) [0.19] | |
| >60 | 29 (45) | 6 (7.64) [0.35] | 4 (3.62) [0.04] | 2(4.02) [1.01] | |
| Mean age (years) | 57 ± 6.8 | 51 ± 6.5 | 40 ± 3.4 | 50 ± 3.7 | 0.20 (8.4688). |
| Skeletal involvement, n (%) | |||||
| Expected total/chi-square. | |||||
| Axial | 17 (26.5) | 7 (4.99) [0.81] | 4 (2.36) [1.13] | 4 (2.36) [1.13] | 0.33 (3.3982) |
| Peripheral | 60 (94) | 12(14.01) [0.29] | 5 (6.64) [0.40] | 5 (6.64) [0.40] | |
| Duration of PsA ** | |||||
| Mean ±SD | 16.22 ± 9.18 | 13.5 ± 9.3 | 13.4 ± 8.7 | 13.85 ± 9.9 | |
| Median (IQR) | 14 (40) 0.95 | 14 (37) 0.93 | 13 (37) 0.97 | 10 (35) 0.98 | 0.98 |
| Years from onset to diagnosis ** | |||||
| Mean ± SD | 3.11 ± 6.15 | 3.12 ± 6.13 | 3.11 ± 6.2 | 3.8 ± 6.12 | |
| Median (range) | 0 (33) 0.98 | 0 (27) 0.96 | 0 (27) 0.97 | 0 (33) 0.94 | 0.96 |
| Years of PsA diagnosis ** | |||||
| Mean ± SD | 13.46 ± 8.97 | 10.4 ± 6.9 | 10 ± 5.6 | 10.5 ± 7.5 | |
| Median (range) | 0 (40) 0.8 | 0 (37) 0.98 | 0 (33) 0.97 | 7 (40) 0.88 | 0.97 |
| Years on iTNF ** | 1 | ||||
| Mean ± SD | 8.28 ± 4.61 | 8.15 ± 3.88 | 8.1 ± 3.6 | 7.25 ± 3.25 | |
| Median (range) | 8 (17) 1 | 8 (17) 1 | 8 (16) 1 | 7 (15) 1 | |
| Years on iIL-17 ** | |||||
| Mean ± SD | 0.56 ± 0.56 | 0.55 ± 0.53 | 0.54 ± 0.47 | 0.58 ± 0.49 | |
| Median (range) | 0 (5) 1 | 0 (5) 1 | 0 (5) 1 | 0 (4) 1 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Strugariu, G.; Pomîrleanu, C.; Russu, M.; Popescu, A.; Petrariu, L.A.; Ancuta, E.; Chirieac, R.; Temelie-Olinici, D.; Ancuța, C. Long-Term Outcomes of Patients with Biologically Treated Psoriatic Arthritis and Atopic Dermatitis—A Single-Center Experience. J. Pers. Med. 2024, 14, 427. https://doi.org/10.3390/jpm14040427
Strugariu G, Pomîrleanu C, Russu M, Popescu A, Petrariu LA, Ancuta E, Chirieac R, Temelie-Olinici D, Ancuța C. Long-Term Outcomes of Patients with Biologically Treated Psoriatic Arthritis and Atopic Dermatitis—A Single-Center Experience. Journal of Personalized Medicine. 2024; 14(4):427. https://doi.org/10.3390/jpm14040427
Chicago/Turabian StyleStrugariu, Georgiana, Cristina Pomîrleanu, Mara Russu, Alexandra Popescu, Luiza Andreea Petrariu, Eugen Ancuta, Rodica Chirieac, Doinița Temelie-Olinici, and Codrina Ancuța. 2024. "Long-Term Outcomes of Patients with Biologically Treated Psoriatic Arthritis and Atopic Dermatitis—A Single-Center Experience" Journal of Personalized Medicine 14, no. 4: 427. https://doi.org/10.3390/jpm14040427
APA StyleStrugariu, G., Pomîrleanu, C., Russu, M., Popescu, A., Petrariu, L. A., Ancuta, E., Chirieac, R., Temelie-Olinici, D., & Ancuța, C. (2024). Long-Term Outcomes of Patients with Biologically Treated Psoriatic Arthritis and Atopic Dermatitis—A Single-Center Experience. Journal of Personalized Medicine, 14(4), 427. https://doi.org/10.3390/jpm14040427