
Computational Approach for Spatially Fractionated Radiation Therapy (SFRT) and Immunological Response in Precision Radiation Therapy

 ,
, 
 ,
,  and
and
Abstract
:1. Introduction
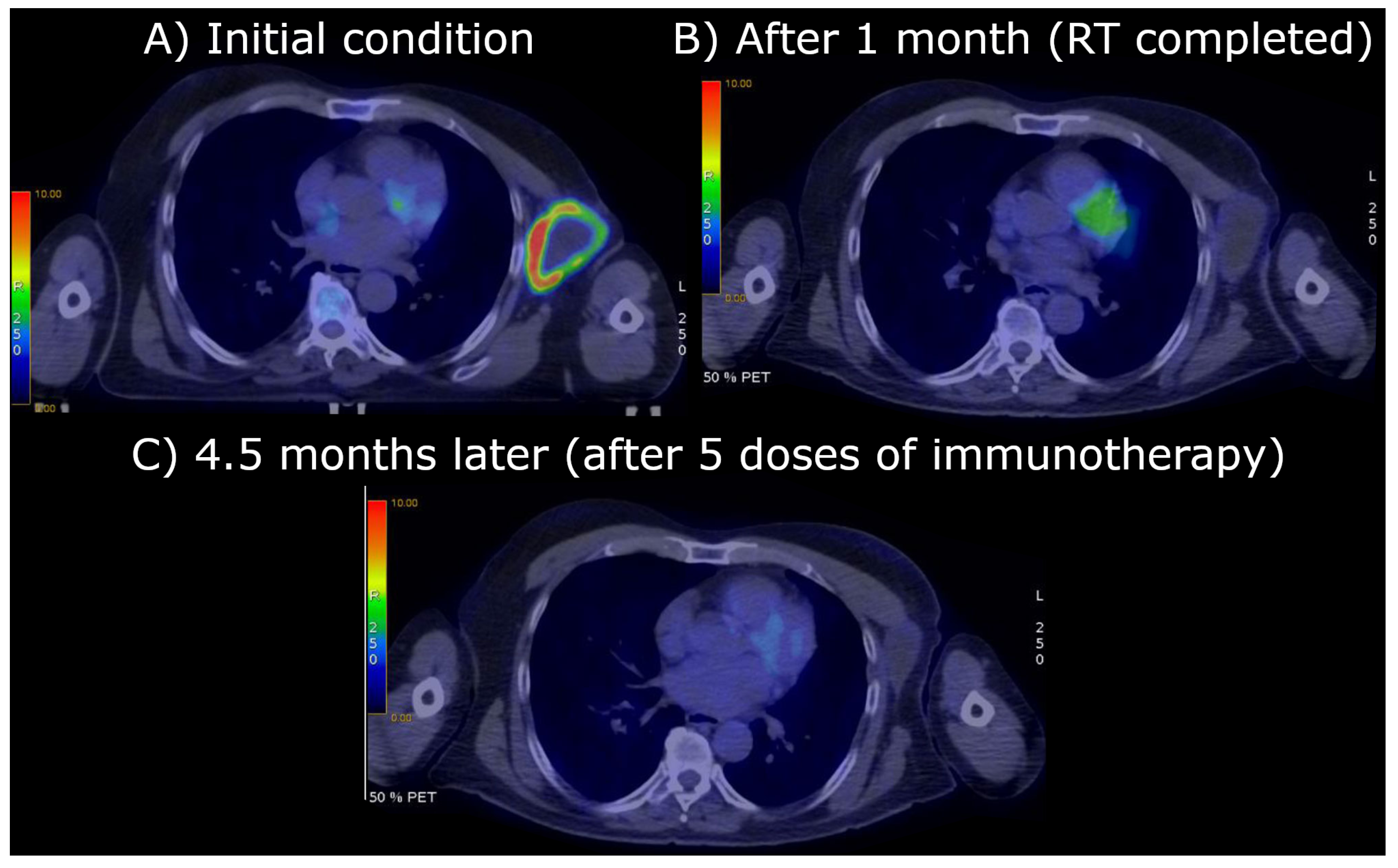
2. The Case Report: Radiotherapy and Clinical Results
3. Methods
- was defined as the tumor volume before the first treatment;
- is the observed volume after n doses (“exp” indicates the experimental value);
- is the volume numerically evaluated starting with by applying the Linear Quadratic Model (LQM) (including OER when necessary) for n doses (“rad” indicates radiotherapy).
- Measurement of the initial tumor volume , since the initial size of the untreated tumor includes the effect of the host immune response.
- Numerical evaluation of the final volume according to the scheduled radio-treatment and the LQM (including OER if necessary). For example, for the normoxic cell volume, one getsafter n treatments of dose d, with time interval day, and assuming the regrowth is negligible between daily subsequent doses (the regrowth is however included in the mathematical formulation, see Equations (A5) and (A6) of Appendix A. is the theoretical, expected, tumor shrinkage by radiotherapy only.
- Measurement of the final tumor volume , after n doses, which gives the effective tumor volume reduction.
- Comparison of the effective tumor size at the end of therapy with the theoretical value. If , definewhich describes the difference between the observed volume and the expected one by LQM, at the end of radiotherapy.
- According to the computational model, is due to the immune response activated by radiotherapy, A (see Equations (A5) and (A6) in Appendix A), which at the end of the n treatments turns out to beA (0, nt) quantitatively defines the induced immune response. In other words, the activation of the immune response due to radiotherapy (to note, this is not a “passive or exogenous” immunotherapy, but a consequence of the immune response to the cell debris resulting from apoptotic cells due to radiation) determines, at the clinical level, the difference between the “theoretical value” calculated by the LQM and the observed tumor size reduction.
- To estimate the specific regrowth rate at the end of radiotherapy (see Equations (A8) and (A9) in Appendix A) one needs to evaluate the constantwhere is the lethal maximum tumor volume supported by the environmental condition (oxygen, nutrient supplies, …), generally corresponding to cells, i.e., about a diameter of 12 cm [12].
- Compare the previous constant with the calculated in Equation (3). Ifthen the disease evolves towards complete recovery, due to the immune response activated by radiotherapy, because the specific rate turns out to be negative. In general, this is not the case, since the first term is large.
- More precisely, immediately after the end of radiotherapy, according to the reasonable assumption that in this limited timeframe the induced immune response remains almost constant, the progression depends on the conditionA few days, m, after the end of radiotherapy (in such a way ), the previous condition can be written asthat can be calculated since the GL parameter k is experimentally known [13], and , previously evaluated, can be considered a reliable estimate of the activated immune response, due to the short time interval.
- If the previous condition is verified, the tumor volume initially decreases after the end of therapy, but the progression can restart. Indeed, for , the time evolution without further immunotherapy follows the law in Equation (A7) of Appendix A (see also Figure 4).By assuming a constant effect of the radiotherapy-activated immune response following radiotherapy, the time for the beginning of the regrowth can be evaluated and it turns out to be (see Equation (A9) in Appendix A, for )On the other hand, for a more realistic, time-dependent immune response, the critical time is defined by the implicit relationIn general, since the stronger constraint in Equation (5) is not satisfied, the patient needs immunotherapy to increase the possibility of a complete recovery or a late tumor regrowth. The effects of the immunotherapy, for , are described by the function , reported in Equations (A12) and (A13) in Appendix A. The condition of the previous Equation (6) for complete recovery now becomes
4. Application to the Case Report
5. Discussion and Conclusions
- The evaluation of the cell killing fraction or volume shrinkage due to the immune response activated by radiotherapy, as a difference to the standard LQM results;
- An estimate of the complete recovery condition or of the regrowth time, by considering a constant immune-activated response at the end of radiotherapy;
- A possible prediction of the immunotherapy effects after the final radiation dose, by patient-oriented monitoring observations, which permits a phenomenological determination of the function B in Equations (10) and (A14).
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix A.1. General Formalism
Appendix A.2. Including Immunotherapy
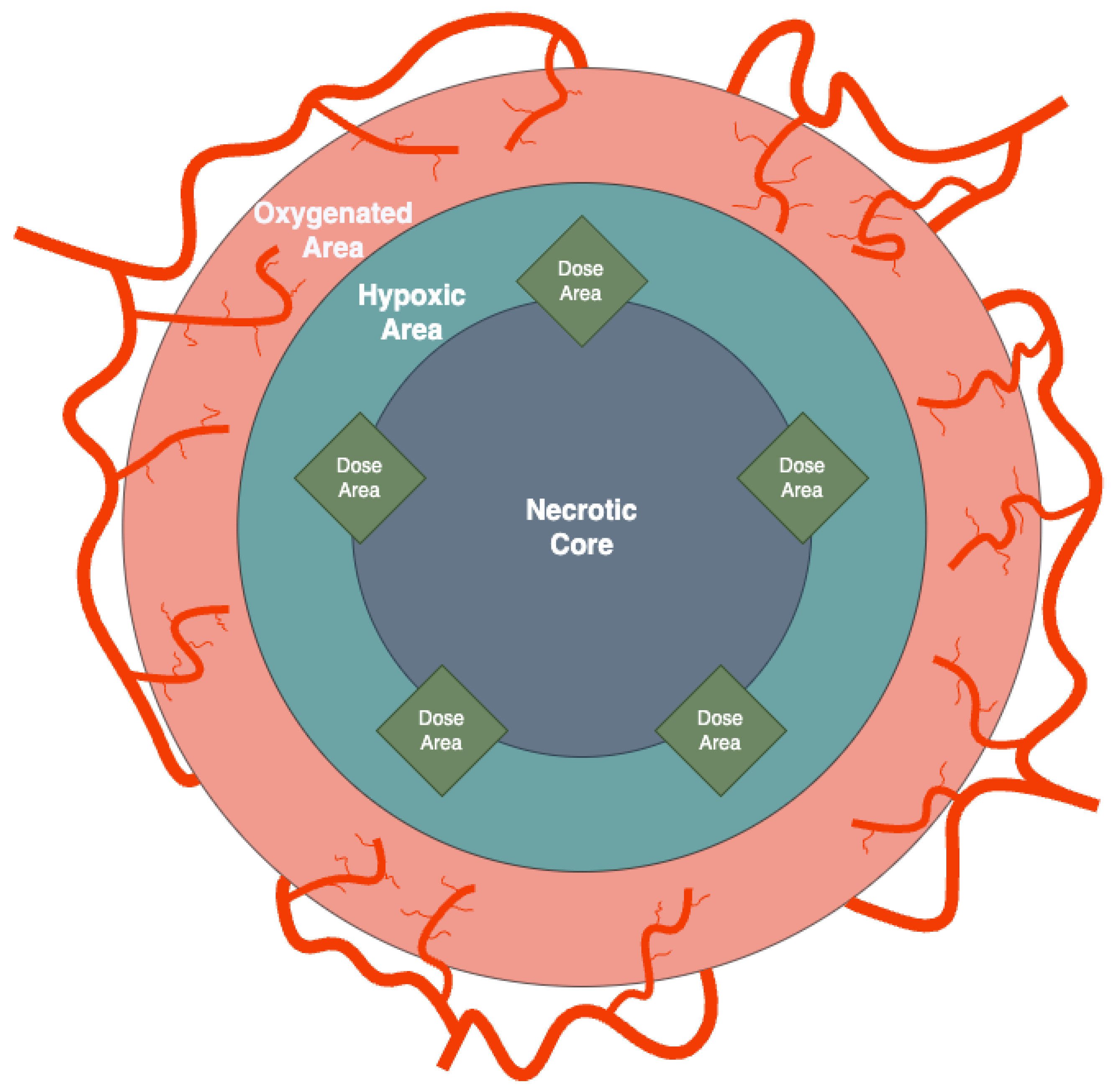
Appendix A.3. Geometrical Setting and Radiotherapy Treatment of the Case Report

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Day | Reduction Factor |
|---|---|
| 0 | |
| 1 | |
| 2 | |
| 3 | |
| 4 | |
| 5 | |
| 6 | |
| 7 | |
| 8 | |
| 9 | |
| 10 |
References
- Tubin, S.; Vozenin, M.; Prezado, Y.; Durante, M.; Prise, K.; Lara, P.; Greco, C.; Massaccesi, M.; Guha, C.; Wu, X.; et al. Novel unconventional radiotherapy techniques: Current status and future perspectives—Report from the 2nd international radiation oncology online seminar. Clin. Transl. Radiat. Oncol. 2023, 40, 100605. [Google Scholar] [CrossRef] [PubMed]
- Ferini, G.; Parisi, S.; Lillo, S.; Viola, A.; Minutoli, F.; Critelli, P.; Valenti, V.; Illari, S.I.; Brogna, A.; Umana, G.E.; et al. Impressive results after “metabolism-guided” lattice irradiation in patients submitted to palliative radiation therapy: Preliminary results of LATTICE_01 Multicenter Study. Cancers 2022, 14, 3909. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Lin, Y.; Wang, F.; Badkul, R.; Chen, R.C.; Gao, H. Lattice position optimization for LATTICE therapy. Med. Phys. 2023, 50, 7359–7367. [Google Scholar] [CrossRef] [PubMed]
- Ferini, G.; Zagardo, V.; Pergolizzi, S. To answer Spałek’s question: Lattice radiotherapy is more hope than hype. Ann. Palliat. Med. 2023, 12, 1106108. [Google Scholar] [CrossRef] [PubMed]
- Ferini, G.; Valenti, V.; Viola, A.; Umana, G.E.; Illari, S.I.; Parisi, S.; Pontoriero, A.; Pergolizzi, S. First-ever Clinical Experience with Magnetic Resonance-based Lattice Radiotherapy for Treating Bulky Gynecological Tumors. Anticancer Res. 2022, 42, 4641–4646. [Google Scholar] [CrossRef] [PubMed]
- Tubin, S.; Khan, M.K.; Salerno, G.; Mourad, W.F.; Yan, W.; Jeremic, B. Mono-institutional phase 2 study of innovative Stereotactic Body RadioTherapy targeting PArtial Tumor HYpoxic (SBRT-PATHY) clonogenic cells in unresectable bulky non-small cell lung cancer: Profound non-targeted effects by sparing peri-tumoral immune microenvironment. Radiat. Oncol. 2019, 14, 212. [Google Scholar] [PubMed]
- Ferini, G.; Castorina, P.; Valenti, V.; Illari, S.I.; Sachpazidis, I.; Castorina, L.; Marrale, M.; Pergolizzi, S. A novel radiotherapeutic approach to treat bulky metastases even from cutaneous squamous cell carcinoma: Its rationale and a look at the reliability of the linear-quadratic model to explain its radiobiological effects. Front. Oncol. 2022, 12, 809279. [Google Scholar] [CrossRef]
- Parisi, S.; Napoli, I.; Lillo, S.; Cacciola, A.; Ferini, G.; Iatì, G.; Pontoriero, A.; Tamburella, C.; Davì, V.; Pergolizzi, S. Spine eburnation in a metastatic lung cancer patient treated with immunotherapy and radiotherapy. The first case report of bystander effect on bone. J. Oncol. Pharm. Pract. 2022, 28, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Tubin, S.; Gupta, S.; Grusch, M.; Popper, H.H.; Brcic, L.; Ashdown, M.L.; Khleif, S.N.; Peter-Vörösmarty, B.; Hyden, M.; Negrini, S.; et al. Shifting the immune-suppressive to predominant immune-stimulatory radiation effects by SBRT-PArtial tumor irradiation targeting HYpoxic segment (SBRT-PATHY). Cancers 2020, 13, 50. [Google Scholar] [CrossRef] [PubMed]
- Bertho, A.; Iturri, L.; Prezado, Y. Radiation-induced immune response in novel radiotherapy approaches FLASH and spatially fractionated radiotherapies. Int. Rev. Cell Mol. Biol. 2023, 376, 37–68. [Google Scholar] [PubMed]
- Cytlak, U.M.; Dyer, D.P.; Honeychurch, J.; Williams, K.J.; Travis, M.A.; Illidge, T.M. Immunomodulation by radiotherapy in tumour control and normal tissue toxicity. Nat. Rev. Immunol. 2022, 22, 124–138. [Google Scholar] [CrossRef] [PubMed]
- Norton, L. A Gompertzian model of human breast cancer growth. Cancer Res. 1988, 48, 7067–7071. [Google Scholar] [PubMed]
- Vaghi, C.; Rodallec, A.; Fanciullino, R.; Ciccolini, J.; Mochel, J.P.; Mastri, M.; Poignard, C.; Ebos, J.M.; Benzekry, S. Population modeling of tumor growth curves and the reduced Gompertz model improve prediction of the age of experimental tumors. PLoS Comput. Biol. 2020, 16, e1007178. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Shao, C. Radiotherapy-Mediated Immunomodulation and Anti-Tumor Abscopal Effect Combining Immune Checkpoint Blockade. Cancers 2020, 12, 2762. [Google Scholar] [CrossRef] [PubMed]
- Puglisi, C.; Giuffrida, R.; Borzì, G.; Di Mattia, P.; Costa, A.; Colarossi, C.; Deiana, E.; Picardo, M.; Colarossi, L.; Mare, M.; et al. Radiosensitivity of Cancer Stem Cells Has Potential Predictive Value for Individual Responses to Radiotherapy in Locally Advanced Rectal Cancer. Cancers 2020, 12, 3672. [Google Scholar] [CrossRef] [PubMed]
- Puglisi, C.; Giuffrida, R.; Borzì, G.; Illari, S.; Caronia, F.; Di Mattia, P.; Colarossi, C.; Ferini, G.; Martorana, E.; Sette, G.; et al. Ex Vivo Irradiation of Lung Cancer Stem Cells Identifies the Lowest Therapeutic Dose Needed for Tumor Growth Arrest and Mass Reduction In Vivo. Front. Oncol. 2022, 12, 837400. [Google Scholar] [CrossRef] [PubMed]
- Ngwa, W.; Irabor, O.; Schoenfeld, J.; Hesser, J.; Demaria, S.; Formenti, S. Using immunotherapy to boost the abscopal effect. Nat. Rev. Cancer 2018, 18, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Mole, R. Whole body irradiation; radiobiology or medicine? Br. J. Radiol. 1953, 26, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Demaria, S.; Ng, B.; Devitt, M.; Babb, J.; Kawashima, N.; Liebes, L.; Formenti, S. Ionizing radiation inhibition of distant untreated tumors (abscopal effect) is immune mediated. Int. J. Radiat. Oncol. Biol. Phys. 2004, 58, 862–870. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castorina, P.; Castiglione, F.; Ferini, G.; Forte, S.; Martorana, E. Computational Approach for Spatially Fractionated Radiation Therapy (SFRT) and Immunological Response in Precision Radiation Therapy. J. Pers. Med. 2024, 14, 436. https://doi.org/10.3390/jpm14040436
Castorina P, Castiglione F, Ferini G, Forte S, Martorana E. Computational Approach for Spatially Fractionated Radiation Therapy (SFRT) and Immunological Response in Precision Radiation Therapy. Journal of Personalized Medicine. 2024; 14(4):436. https://doi.org/10.3390/jpm14040436
Chicago/Turabian StyleCastorina, Paolo, Filippo Castiglione, Gianluca Ferini, Stefano Forte, and Emanuele Martorana. 2024. "Computational Approach for Spatially Fractionated Radiation Therapy (SFRT) and Immunological Response in Precision Radiation Therapy" Journal of Personalized Medicine 14, no. 4: 436. https://doi.org/10.3390/jpm14040436
APA StyleCastorina, P., Castiglione, F., Ferini, G., Forte, S., & Martorana, E. (2024). Computational Approach for Spatially Fractionated Radiation Therapy (SFRT) and Immunological Response in Precision Radiation Therapy. Journal of Personalized Medicine, 14(4), 436. https://doi.org/10.3390/jpm14040436