
Digital versus Manual Tracing in Cephalometric Analysis: A Systematic Review and Meta-Analysis

 , ,
, ,  ,
,  and
and 
Abstract
:1. Introduction
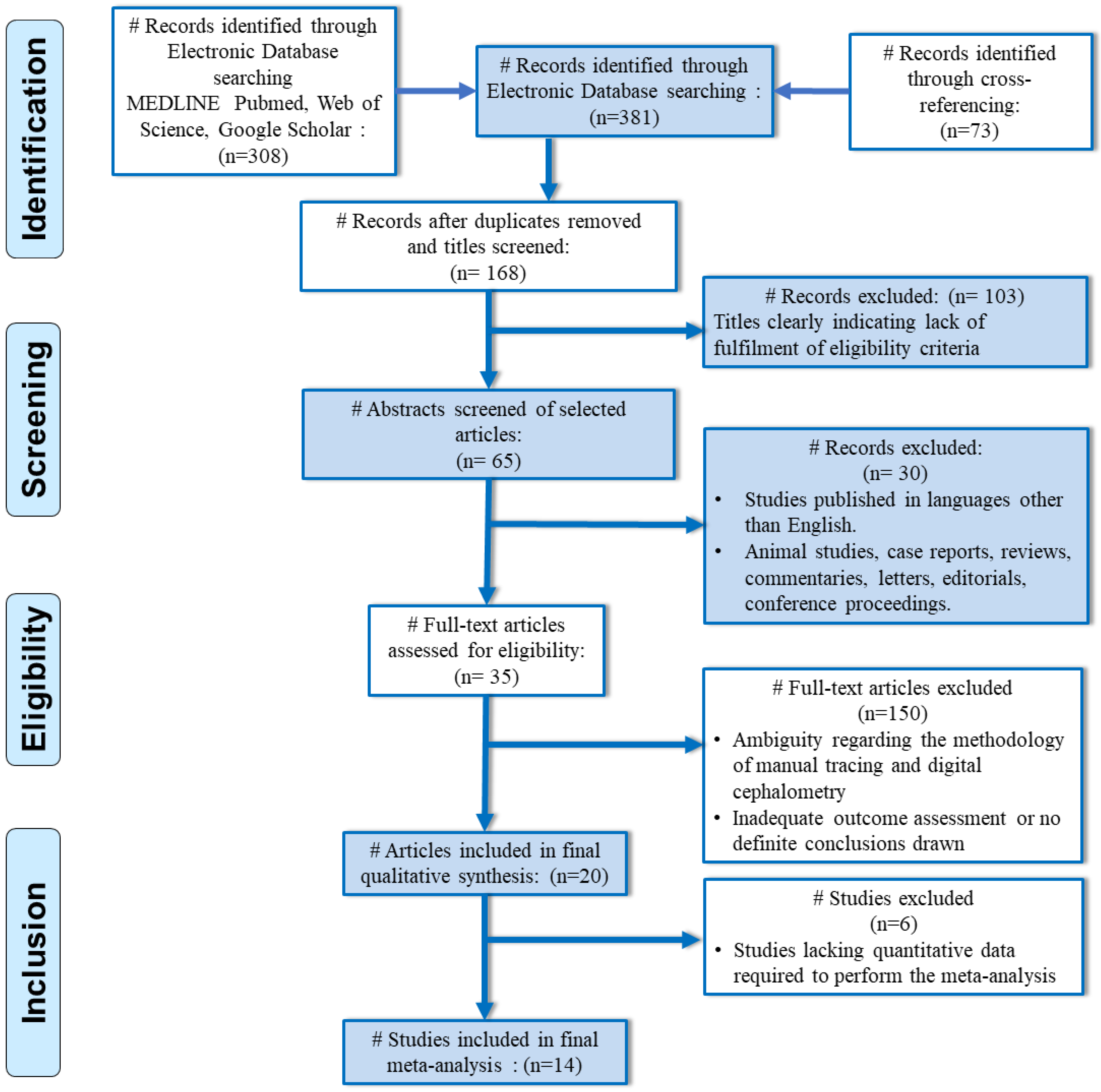
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Data Extraction
- Angular measurements—SNA, SNB, ANB, IMPA, Interincisal angle, SN-MP, SN-PP, MMA, and Gonial angle
- Linear measurements were recorded—anterior cranial base (N-S), mandibular length (Go-Me), maxillary length (ANS to PNS), and LAFH—lower anterior facial height. (ANS to Me)
2.3. Data Reporting
2.4. Assessments of the Risk of Bias and Quality
2.5. Statistical Analysis for Quantitative Synthesis
3. Results
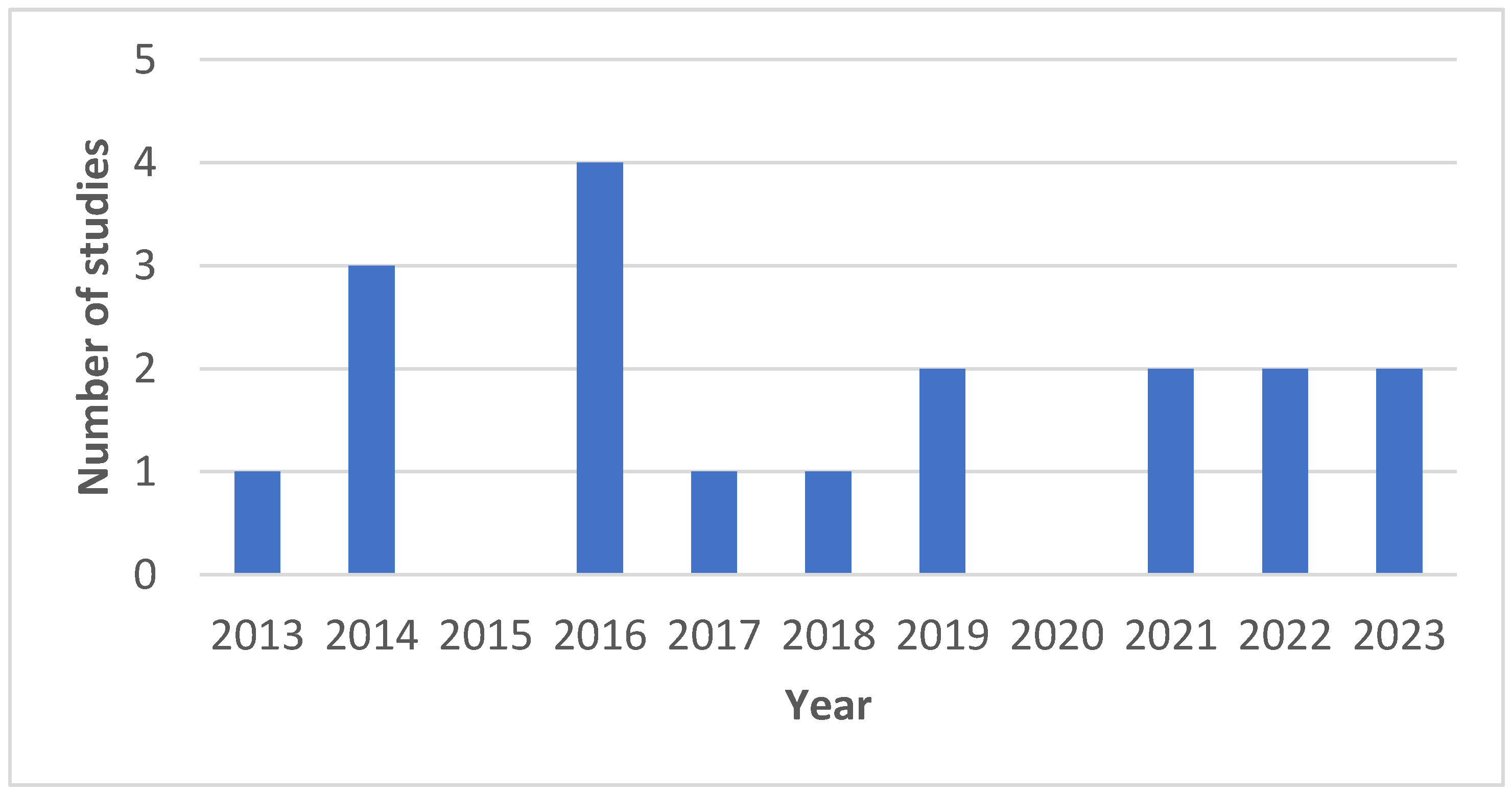
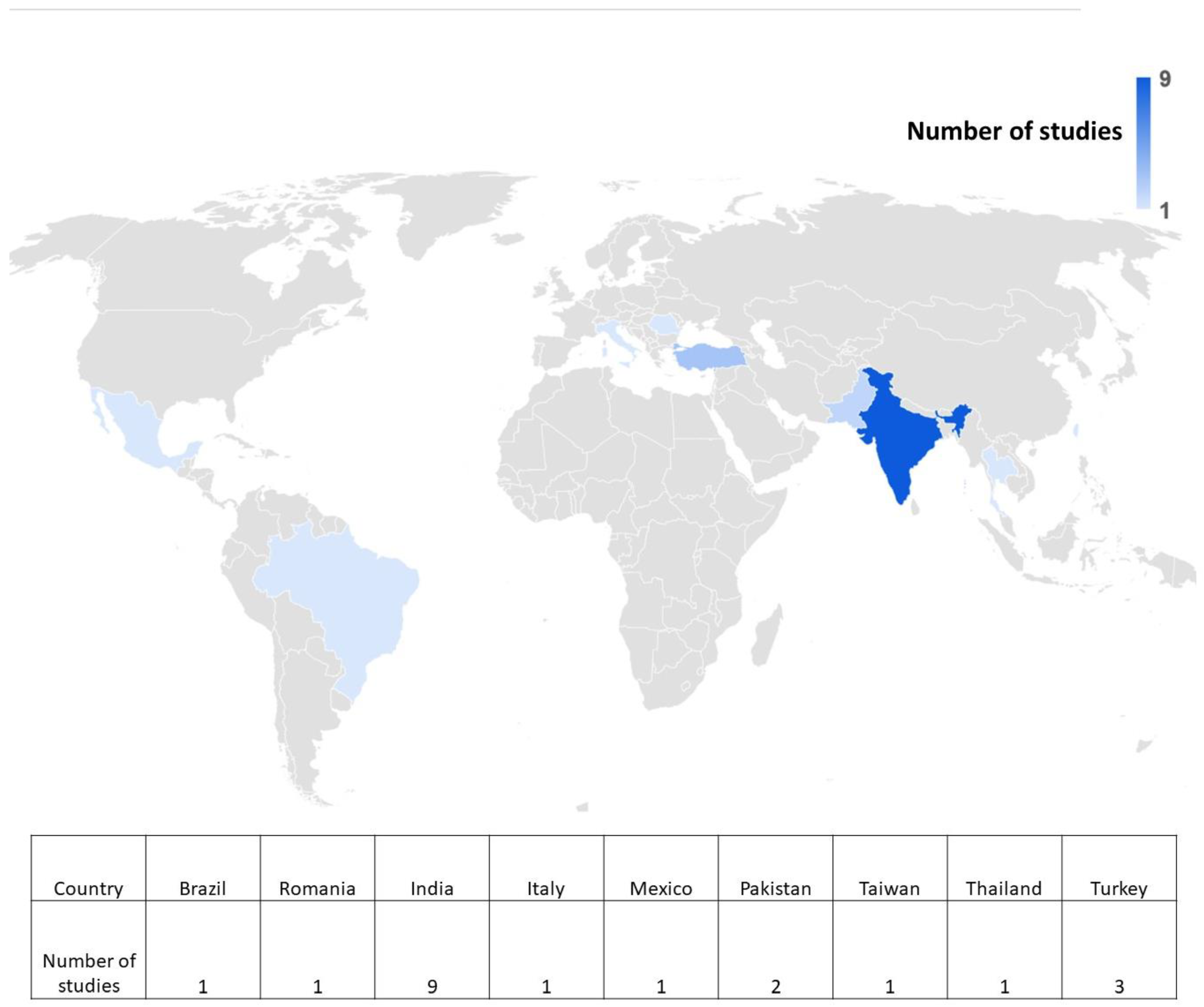
3.1. Narrative Synthesis
3.2. Meta-Analysis
3.2.1. Effect Measures
3.2.2. Study Inclusion
3.2.3. Maxilla
- SNA (Sella-Nasion-A Point): Our meta-analysis included data from twelve studies for the assessment of SNA. The pooled SNA estimate was 0.54 (95% CI: −0.28 to 1.35), suggesting that SNA values were greater with digital tracing compared to manual tracing. However, the overall results were not statistically significant (p > 0.05), and there was substantial heterogeneity (65%), necessitating the use of a random effects model for analysis.
- Co-A (Cephalometric A Point): Our analysis incorporated data from five studies for Co-A measurements, resulting in a pooled value of 0.78 mm (95% CI: −1.37 to 2.94). This indicates that Co-A measurements were greater with digital tracing compared to manual tracing. Similarly, the overall results were not statistically significant (p > 0.05), with a high level of heterogeneity (89%), leading to the application of a random effects model.
- Nperp-A (Nasion Perpendicular A): Our analysis included data from two studies for Nperp-A measurements, resulting in a pooled value of −2.30 mm (95% CI: −4.11 to −0.50), indicating that Nperp-A measurements were smaller with digital tracing compared to manual tracing. Notably, the overall results were not statistically significant (p > 0.05), and heterogeneity was minimal (0%).
3.2.4. Mandible
- SNB (Sella-Nasion-B Point): Eleven studies were incorporated into the assessment of SNB. The pooled SNB estimate was 0.26 (95% CI: −0.43 to 0.95), suggesting that SNB values were greater with digital tracing compared to manual tracing. Nevertheless, the overall results were not statistically significant (p > 0.05), and there was a moderate level of heterogeneity (39%), leading to the use of a random effects model for analysis.
- Co-Gn (Cephalometric Gnathion): Our analysis included data from five studies for the evaluation of Co-Gn measurements. The pooled Co-Gn estimate was −0.39 (95% CI: −1.69 to 0.90), indicating that Co-Gn measurements were smaller with digital tracing compared to manual tracing. The overall results were not statistically significant (p > 0.05), with a low level of heterogeneity (8%).
- Pog-NB: Two studies were included in the assessment of Pog-NB. The pooled value obtained was 2.91 [−3.58, 9.40], which was greater with digital tracing as compared to manual tracing. Overall results were not statistically significant (p > 0.05) with 100% heterogeneity. As a result, the random effects model was used for analysis.
- FMPA: Eight studies were included in the assessment of FMPA. The pooled value obtained was 0.62 [−0.54, 1.78], which was greater with digital tracing as compared to manual tracing. Overall results were not statistically significant (p > 0.05) with 50% heterogeneity. As a result, the random effects model was used for analysis.
- MIA: Two studies were included in the assessment of FMIA. The pooled mean difference value obtained was −0.28 [−2.92, 2.37], which was less with digital tracing as compared to manual tracing. Overall results were not statistically significant (p > 0.05) with 0% heterogeneity.
- Nperp-Pog: Two studies were included in the assessment of Nperp-Pog. The pooled value obtained was −4.41 [−9.07, 0.26], indicating that Nperp-Pog was less with digital tracing as compared to manual tracing. Overall results were not statistically significant (p > 0.05), with 24% heterogeneity.
3.2.5. Intermaxillary Relationships
- ANB: Ten studies were included in the assessment of the ANB angle. The pooled value obtained was −2.29 [−4.66, 0.06], indicating that ANB was lower with digital tracing as compared to manual tracing. Overall results were not statistically significant (p > 0.05), with 97% heterogeneity. As a result, a random effects model was used for analysis.
- Wits appraisal: Four studies were included in the assessment of Wits appraisal. The pooled value obtained was −0.28 [−1.08, 0.51]. This implies that the value of the Wits appraisal obtained with digital tracing was less than manual tracing. Overall results were not statistically significant (p > 0.05) with 0% heterogeneity.
- ANS-Me: Five studies were included in the assessment of ANS-Me landmark. The pooled value obtained was 0.85 [−0.28, 2.28]. This implies that the value of ANS-Me obtained with digital tracing was greater than that obtained with manual tracing. Overall results were not statistically significant (p > 0.05) with 55% heterogeneity. A random effects model was used for analysis.
- Jarabak ratio: Two studies were included in the assessment of the Jarabak ratio. The pooled value obtained was −0.11 [−1.39, 1.18]. This implies that the value of the Jarabak ratio obtained with digital tracing was less than that obtained with manual tracing. Overall results were not statistically significant (p > 0.05) with 0% heterogeneity.

3.2.6. Dentoalveolar
- U1-A point: Two studies were included in the assessment of the U1-A point landmark. The pooled value obtained was −0.24 [−0.73, 0.24], indicating that the value of this landmark obtained with digital tracing was less as compared to manual tracing. Overall results were not statistically significant (p > 0.05), with 32% heterogeneity. As a result, a random effects model was used for analysis.
- LI-A Pog: Four studies were included in the assessment of the LI-A Pog landmark. The pooled value obtained was −0.15 [−0.38–0.07], indicating that the value of this landmark obtained with digital tracing was less as compared to manual tracing. Overall results were not statistically significant (p > 0.05), with 21% heterogeneity.
- IMPA: Five studies were included in the assessment of the IMPA angle. The pooled value obtained was −0.67 [−2.69, 1.34]. The value of this landmark obtained with digital tracing was less as compared to manual tracing. Overall results were not statistically significant (p > 0.05) with 85% heterogeneity. As a result, a random effects model was used for analysis.
- UI-NA angle: Eight studies were included in the assessment of the UI-NA angle. The pooled value obtained was −0.17 [−0.51–0.17] degrees, indicating that the value of this landmark obtained with digital tracing was less as compared to manual tracing. Overall results were not statistically significant (p > 0.05), with 21% heterogeneity.
- UI-NA (mm): Ten studies were included in the assessment of UI-NA distance. The pooled value obtained was −0.09 [−0.52, 0.34] mm indicating that the value of this landmark obtained with digital tracing was less as compared to manual tracing. Overall results were not statistically significant (p > 0.05) with 92% heterogeneity. As a result, a random effects model was used for analysis.
- LI-NB angle: Nine studies were included in the assessment of the LI-NB angle. The pooled value obtained was −0.09 [−0.27, 0.08] degrees, indicating that the value of this landmark obtained with digital tracing was less as compared to manual tracing. Overall results were not statistically significant (p > 0.05), with 43% heterogeneity. As a result, a random effects model was used for analysis.
- LI-NB (mm): Ten studies were included in the assessment of LI-NB distance. The pooled value obtained was 0.10 [−0.12, 0.31] mm indicating that the value of this landmark obtained with digital tracing was greater as compared to manual tracing. Overall results were not statistically significant (p > 0.05) with 70% heterogeneity. As a result, a random effects model was used for analysis.
- Go Gn to SN: Four studies were included in the assessment of the Go Gn to SN landmark. The pooled value obtained was 0.11 [−0.04, 0.27], indicating that the value of this landmark obtained with digital tracing was greater as compared to manual tracing. Overall results were not statistically significant (p > 0.05) with 0% heterogeneity.
- Nasolabial angle: Six studies were included in the assessment of the Nasolabial angle. The pooled value obtained was 0.24 [−0.05, 0.53] degrees, indicating that the value of this landmark obtained with digital tracing was greater as compared to manual tracing. Overall results were not statistically significant (p > 0.05), with 59% heterogeneity. As a result, a random effects model was used for analysis.
- Interincisal angle: Three studies were included in the assessment of the interincisal angle. The pooled value obtained was −0.03 [−0.27, 0.21] degrees, indicating that the value of this landmark obtained with digital tracing was less as compared to manual tracing. Overall results were not statistically significant (p > 0.05) with 0% heterogeneity.
- LAFH: Two studies were included in the assessment of the LAFH landmark. The pooled value obtained was −0.51 [−1.36, 0.35], indicating that the value of this landmark obtained with digital tracing was less as compared to manual tracing. Overall results were not statistically significant (p > 0.05), with 73% heterogeneity. As a result, a random effects model was used for analysis.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dinesh, A.; Mutalik, S.; Feldman, J.; Tadinada, A. Value-addition of lateral cephalometric radiographs in orthodontic diagnosis and treatment planning. Angle Orthod. 2020, 90, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Kotuła, J.; Kuc, A.E.; Lis, J.; Kawala, B.; Sarul, M. New sagittal and vertical cephalometric analysis methods: A systematic review. Diagnostics 2022, 12, 1723. [Google Scholar] [CrossRef] [PubMed]
- Gholinia, F.; Pourgholi, M. The reliability of cephalometric measurements in orthodontics: Cone beam computed tomography versus two-dimensional cephalograms. J. Dentomaxillofac. Radiol. Pathol. Surg. 2020, 9, 38–44. [Google Scholar]
- Pinheiro, M.; Ma, X.; Fagan, M.J.; McIntyre, G.T.; Lin, P.; Sivamurthy, G.; Mossey, P.A. A 3D cephalometric protocol for the accurate quantification of the craniofacial symmetry and facial growth. J. Biol. Eng. 2019, 13, 42. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.I.; Lagravère Vich, M.; Mayoral, P.; Miguez, M. Three-dimensional changes in skeletal/dental landmarks with use of mandibular advancement devices. J. Dent. Sleep Med. 2020, 7, 1–8. [Google Scholar] [CrossRef]
- Azad, M.; Elaiwat, S.; Alam, M.K. A Computational Tool for Detection of Soft Tissue Landmarks and Cephalometric Analysis. Electronics 2022, 11, 2408. [Google Scholar] [CrossRef]
- Graf, C.C.; Dritsas, K.; Ghamri, M.; Gkantidis, N. Reliability of cephalometric superimposition for the assessment of craniofacial changes: A systematic review. Eur. J. Orthod. 2022, 44, 477–490. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, C.; Liu, C.Y.J.; Shrimpton, S.; Greenway, E. Craniofacial identification standards: A review of reliability, reproducibility, and implementation. Forensic Sci. Int. 2024, 359, 111993. [Google Scholar] [CrossRef] [PubMed]
- Kunnath, J.T.; Subrahmanya, R.M.; Dhillon, H. Assessment of facial soft tissue thickness in individuals having skeletal class II malocclusion. World J. Dent. 2020, 11, 179–184. [Google Scholar]
- Hlongwa, P. Cephalometric analysis: Manual tracing of a lateral cephalogram. S. Afr. Dent. J. 2019, 74, 389–393. [Google Scholar] [CrossRef]
- Elnagar, M.H.; Gajendrareddy, P.; Lee, M.K.; Allareddy, V. Artificial Intelligence and Orthodontic Practice: The Future Unveiled. In Integrated Clinical Orthodontics; John Wiley & Sons Ltd.: Hoboken, NJ, USA, 2023; pp. 565–575. [Google Scholar]
- Harrell, W.E., Jr. Limitations of Two-Dimensional Cephalometric Analysis in Orthodontic Diagnosis and Treatment Planning: The Future of Three-Dimensional Analysis; SAO Newsletter: Zurich, Switzerland, 2005. [Google Scholar]
- Durão, A.R.; Pittayapat, P.; Rockenbach, M.I.; Olszewski, R.; Ng, S.; Ferreira, A.P.; Jacobs, R. Validity of 2D lateral cephalometry in orthodontics: A systematic review. Prog. Orthod. 2013, 14, 31. [Google Scholar] [CrossRef] [PubMed]
- Lo Giudice, A.; Ronsivalle, V.; Zappalà, G.; Leonardi, R.; Campagna, P.; Isola, G.; Palazzo, G. The evolution of the cephalometric superimposition techniques from the beginning to the digital era: A brief descriptive review. Int. J. Dent. 2021, 2021, 6677133. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, A.K.; Chen, Y.; Almalki, A.; Sivamurthy, G.; Kafle, D. Cephalometric Analysis in Orthodontics Using Artificial Intelligence—A Comprehensive Review. Biomed. Res. Int. 2022, 2022, 1880113. [Google Scholar] [CrossRef] [PubMed]
- Bulatova, G.; Kusnoto, B.; Grace, V.; Tsay, T.P.; Avenetti, D.M.; Sanchez, F.J. Assessment of automatic cephalometric landmark identification using artificial intelligence. Orthod. Craniofac. Res. 2021, 24, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Duran, G.S.; Gökmen, Ş.; Topsakal, K.G.; Görgülü, S. Evaluation of the accuracy of fully automatic cephalometric analysis software with artificial intelligence algorithm. Orthod. Craniofac. Res. 2023, 26, 481–490. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- PROSPERO. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42023452625 (accessed on 25 April 2024).
- Cochrane Handbook for Systematic Reviews of Interventions. Available online: https://training.cochrane.org/handbook (accessed on 10 January 2024).
- National Heart, Lung, and Blood Institute. Study Quality Assessment Tools; National Heart, Lung, and Blood Institute: Bethesda, MD, USA. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 4 April 2024).
- Navarro, R.D.; Oltramari-Navarro, P.V.; Fernandes, T.M.; Oliveira, G.F.; Conti, A.C.; Almeida, M.R.; de Almeida, R.R. Comparison of manual, digital and lateral CBCT cephalometric analyses. J. Appl. Oral Sci. 2013, 21, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Goracci, C.; Ferrari, M. Reproducibility of measurements in tablet-assisted, PC-aided, and manual cephalometric analysis. Angle Orthod. 2014, 84, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Iacob, M.; Roşu, S.; Zetu, I. Accuracy of computer-assisted cephalometric measurements: A comparative study. Int. J. Med. Dent. 2014, 4, 35–39. [Google Scholar]
- Tanwani, H.B.; Potnis, S.S.; Baralay, S.S.; Patil, S.S. Comparison of conventional and digital cephalometric analysis: A pilot study. J. Dent. Allied Sci. 2014, 3, 80. [Google Scholar]
- Farooq, M.U.; Khan, M.A.; Imran, S.; Sameera, A.; Qureshi, A.; Ahmed, S.A.; Kumar, S.; Rahman, M.A.U. Assessing the reliability of digitalized cephalometric analysis in comparison with manual cephalometric analysis. J. Clin. Diagn. Res. 2016, 10, ZC20. [Google Scholar] [CrossRef]
- Kamath, M.; Arun, A. Comparison of cephalometric readings between manual tracing and digital software tracing: A pilot study. Int. J. Orthod. Rehabil. 2016, 7, 135. [Google Scholar] [CrossRef]
- Lindner, C.; Wang, C.W.; Huang, C.T.; Li, C.H.; Chang, S.W.; Cootes, T.F. Fully automatic system for accurate localisation and analysis of cephalometric landmarks in lateral cephalograms. Sci. Rep. 2016, 6, 33581. [Google Scholar] [CrossRef]
- Mahto, R.K.; Kharbanda, O.P.; Duggal, R.; Sardana, H.K. A comparison of cephalometric measurements obtained from two computerized cephalometric softwares with manual tracings. J. Indian Orthod. Soc. 2016, 50, 162–170. [Google Scholar] [CrossRef]
- Kasinathan, G.; Kumar, S.; Kommi, P.B.; Sankar, H.; Sabapathy, S.; Arani, N. Reliability in landmark plotting between manual and computerized method—A cephalometric study. Int. J. Sci. Study 2017, 4, 73–78. [Google Scholar]
- Anuwongnukroh, N.; Dechkunakorn, S.; Damrongsri, S.; Nilwarat, C.; Pudpong, N.; Radomsutthisarn, W.; Kangern, S. Assessment of the reliability of automatic cephalometric analysis software. Int. J. Mech. Eng. Robot. Res. 2018, 7, 61–65. [Google Scholar] [CrossRef]
- Hassan, N.; Mushtaq, N.; Khan, M.A.; Shamal, S.; Umer, M. Comparison between linear cephalometric measurements tracing on manual and digitized lateral cephalogram. Pak. Oral Dent. J. 2019, 39, 325–329. [Google Scholar]
- İzgi, E.; Pekiner, F.N. Comparative evaluation of conventional and OnyxCeph dental software measurements on cephalometric radiography. Turk. J. Orthod. 2019, 32, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Mohan, A.; Sivakumar, A.; Nalabothu, P. Evaluation of accuracy and reliability of OneCeph digital cephalometric analysis in comparison with manual cephalometric analysis—A cross-sectional study. BDJ Open 2021, 7, 94–97. [Google Scholar] [CrossRef]
- Zamrik, O.M.; Iseri, H. The reliability and reproducibility of an Android cephalometric smartphone application in comparison with the conventional method. Angle Orthod. 2021, 91, 236–242. [Google Scholar] [CrossRef]
- Katyal, D.; Balakrishnan, N. Evaluation of the accuracy and reliability of WebCeph—An artificial intelligence-based online software. APOS Trends Orthod. 2022, 12, 271–276. [Google Scholar] [CrossRef]
- Kılınç, D.D.; Kırcelli, B.H.; Sadry, S.; Karaman, A. Evaluation and comparison of smartphone application tracing, web-based artificial intelligence tracing and conventional hand tracing methods. J. Stomatol. Oral Maxillofac. Surg. 2022, 123, e906–e915. [Google Scholar] [CrossRef] [PubMed]
- Reyes Salgado, J.J. Design of open code software to Downs and Steiner lateral cephalometric analysis with tracing landmarks. Digital 2022, 2, 120–142. [Google Scholar] [CrossRef]
- Khan, R.N.; Tariq, A.; Jan, A.; Pasha, H.; Ansari, F. Hand-traced versus digitally traced cephalometric analysis: A comparative study. Life Sci. 2023, 4, 5. [Google Scholar] [CrossRef]
- Khattri, N.; Nagar, N.; Agarwal, S.; Mehta, V.; Niharika, T.K.; Joshi, N. To compare the reliability and accuracy of artificial intelligence-based fully automated cephalometric tracing software with computer-aided semi-automatic cephalometric software. J. Dent. Med. Sci. 2023, 22, 26–33. [Google Scholar]
- Prince, S.T.T.; Srinivasan, D.; Duraisamy, S.; Kannan, R.; Rajaram, K. Reproducibility of linear and angular cephalometric measurements obtained by an artificial-intelligence-assisted software (WebCeph) in comparison with digital software (AutoCEPH) and manual tracing method. Dent. Press J. Orthod. 2023, 28, e2321214. [Google Scholar] [CrossRef] [PubMed]
- Serdar, C.C.; Cihan, M.; Yücel, D.; Serdar, M.A. Sample size, power and effect size revisited: Simplified and practical approaches in pre-clinical, clinical and laboratory studies. Biochem. Med. 2021, 31, 27–53. [Google Scholar] [CrossRef] [PubMed]
- Murali, K.; Nirmal, R.M.; Balakrishnan, S.; Shanmugam, S.; Altaf, S.K.; Nandhini, D. Age estimation using cephalometrics—A cross-sectional study among teenagers of Salem District, Tamil Nadu. J. Pharm. Bioallied Sci. 2023, 15 (Suppl. S1), S725–S728. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.S.; Hsiao, S.Y.; Lee, K.T. Analysis of facial skeletal morphology: Nasal bone, maxilla, and mandible. Biomed. Res. Int. 2021, 2021, 5599949. [Google Scholar] [CrossRef] [PubMed]
- Campos, L.A.; Campos, J.A.; Marôco, J.; Peltomäki, T. Aesthetic dental treatment, orofacial appearance, and life satisfaction of Finnish and Brazilian adults. PLoS ONE 2023, 18, e0287235. [Google Scholar] [CrossRef]
- Prado, L.H.; Previato, K.; Delgado, R.Z.; Nelson Filho, P.; Segato, R.A.; Matsumoto, M.A.; Feres, M.F. Adolescents’ perception of malocclusion, their motivations, and expectations concerning the orthodontic treatment. Is it all about attractiveness? A qualitative study. Am. J. Orthod. Dentofac. Orthop. 2022, 161, e345–e352. [Google Scholar] [CrossRef] [PubMed]
- Zaidi, A.B.; Karim, A.A.; Mohiuddin, S.; Rehman, K. Effects of dental aesthetics on psycho-social wellbeing among students of health sciences. J. Pak. Med. Assoc. 2020, 70, 1002–1005. [Google Scholar] [PubMed]
- Zhang, M.J.; Sang, Y.H.; Tang, Z.H. Psychological impact and perceptions of orthodontic treatment of adult patients with different motivations. Am. J. Orthod. Dentofac. Orthop. 2023, 164, e64–e71. [Google Scholar] [CrossRef] [PubMed]
- Jain, M.; Patel, D. Lateral cephalogram from CBCT reliable approach for orthodontic diagnosis: A comparative study. Iran J. Orthod. 2022, 17, 1–7. [Google Scholar]
- Meriç, P.; Naoumova, J. Web-based fully automated cephalometric analysis: Comparisons between app-aided, computerized, and manual tracings. Turk. J. Orthod. 2020, 33, 142. [Google Scholar] [CrossRef] [PubMed]
- Sırlı Yılmazturk, S.; Bozdemir, E.; Orhan, K.; Orhan, H. Evaluation of morphological and morphometric characteristics of the temporomandibular joint in children with different skeletal models in the sagittal and vertical direction. Oral Radiol. 2024, 40, 178–187. [Google Scholar] [CrossRef]
- Kim, I.H.; Kim, Y.G.; Kim, S.; Park, J.W.; Kim, N. Comparing intra-observer variation and external variations of a fully automated cephalometric analysis with a cascade convolutional neural net. Sci. Rep. 2021, 11, 7925. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sr. No. | Author and Year of Study | Country | Sample Size | Age Range (in Years) | Gender (M/F) | Software Used for Digital Cephalometry | Comparator Technique Short Description | Conclusive Findings |
|---|---|---|---|---|---|---|---|---|
| 1. | Navarro 2013 [22] | Brazil | 50 | NP | NP | Dolphin Imaging 11 program i-Cat tomography | Conventional manual tracing | Digital cephalometry: Reliable, similar to manual tracing |
| 2. | Goracci 2014 [23] | Italy | 20 | NP | NP | NemoCeph NX 2009 SmileCeph | Images rescaled to 1:1 using Adobe Photoshop CS and printed on semi-gloss paper on a clear acetate sheet placed over printed images by lead pencil | Tablet-assisted cephalometry: Comparable to manual and PC-aided methods; preferred when user-friendliness and portability are prioritized |
| 3. | Iacob 2014 [24] | Romania | 60 | 8 to 23 | 22/38 | Orthalis cephalometric software | Manual tracing using a 0.5 mm pen on a 0.003-inch acetate paper on a light box, in a dark room | Digital cephalometry: Accuracy akin to manual technique |
| 4. | Tanwani 2014 [25] | India | 20 | NP | NP | Dolphin imaging v 11.7.5.55 | A sheet of lead acetate tracing paper measuring 8 × 10-in and 0.003-in thickness on a view box with the tracing paper positioned over the radiograph with masking tape | Manual vs. digital tracings: Statistically significant differences in Burstone and McNamara’s analyses |
| 5. | Farooq 2016 [26] | India | 44 | 17 to 30 | NP | FACAD 3.6 software | Images resized to 1:1 scale using Adobe Photoshop CS and printed on semi-gloss paper. Traced using a lead pencil on a clear acetate sheet placed over printed images | Most of the commonly used measurements made by digital cephalometry were accurate |
| 6. | Kamath 2016 [27] | India | 20 | NP | NP | FACAD software Ilexis AB, Linköping, | Traced on a view box with acetate tracing paper securely positioned over the radiograph with masking tape. | Manual and digital cephalometry showed statistically significant differences in the measurements obtained on performing Steiner’s analysis |
| 7. | Lindner 2016 [28] | Taiwan | 400 | 7 to 76 mean: 27 | 165/235 | FALA system | Manual tracing | Digital cephalometry: Enhances clinical workflow efficiency by rapidly and accurately analyzing cephalometric landmarks |
| 8. | Mahto 2016 [29] | India | 50 | NP | NP | AutoCEPH© version 1.0 Dolphin® imaging software 11.7 | Using a millimeter ruler and protractor | Digital cephalometry: Agreement with manual tracing, suitable for routine analysis |
| 9. | Kasinathan 2017 [30] | India | 50 | NP | NP | Dolphin Imaging v 11.8 | 0.5 mm lead pencil on a 0.003 thickness acetate sheet in a dark room over an X-ray view box | Digital cephalometry: Similar results to manual, with advantages in archiving and transmission |
| 10. | Anuwongnukroh 2018 [31] | Thailand | 108 | NP | NP | Carestream Dental V6.14 | Manual tracing by overlaying acetate papers on lateral cephalograms | Digital cephalometry: Not as reliable as manual, best used to support diagnosis |
| 11. | Hassan 2019 [32] | Pakistan | 110 | 18 to 38 mean: 23.43 | 44/66 | TrophyDicom software | Lead pencil in a dark room on an illuminator. | Digital cephalometry: User-friendly, time-saving alternative to manual tracing |
| 12. | Izgi 2019 [33] | Turkey | 150 | 12 to 34 | 75/75 | OnyxCeph V3.1.54 | 0.3 mm 2H lead pencil, a ruler, and a protractor on an A4 paper placed over the printed image | Digital cephalometry: Preferred over manual method |
| 13. | Mohan 2021 [34] | India | 20 | 18 to 32 mean: 22.4 | 20/20 | OneCeph | 0.3 mm lead pencil on a sheet of fine grade 36 μm matte acetate tracing paper taped over the X-ray printout | Digital cephalometry: Reliable, fast, and practical for clinical use OneCeph is a simple, reliable, accurate alternative to manual tracing that saves clinical time and armamentarium. |
| 14. | Zamrik 2021 [35] | Turkey | 30 | NP | NP | OneCeph | Manual tracing using a 0.3 mm hard black (HB) lead pencil | Digital vs. manual cephalometry: Clinically insignificant differences. Both tracing methods reliable for daily clinical practice. |
| 15. | Katyal 2022 [36] | India | 25 | mean 18 | 14/11 | WebCeph FACAD | Digital images were imported to Adobe Photoshop 7.0 and rescaled to 1:1, then printed Manually traced using a 0.35 mm lead pencil | Digital cephalometry: Reliable, with advantages of online AI-based software (WebCeph) including cloud-based storage, online archiving, quick analysis, no need for specific installation or software, and compatibility with any operating system. |
| 16. | Klinic 2022 [37] | Turkey | 110 | 10 to 24 mean: 15.83 | 44/66 | SATM CephNinja V4.20 WebCeph | Manual tracing using a 0.3 mm hard black lead pencil | Digital vs. manual cephalometry: Statistically and clinically significant differences Digital cephalometry on smartphones: Clearer image perception, improved comfort AI-based cephalometry: Promises enhanced comfort, practicality, speed |
| 17. | Salgado 2022 [38] | Mexico | 42 | 7 to 19 mean: 13 | 18/24 | Cephalopoint | 4H pencil, adhesive tape, protractor, ruler, erasers, tracing paper, and negatoscope, | Digital cephalometry: One-third time of manual tracing, efficient analysis |
| 18. | Khan 2023 [39] | Pakistan | 120 | 12 to 24 mean: 17.37 | 56/64 | View Box V4.0 | 0.5 mm lead pencil and protractors on 0.003-inch matte acetate paper under a standard view box | No significant difference: Manual vs. digital cephalometry for selected angular and linear measurements |
| 19. | Khattri 2023 [40] | India | 100 | NP | NP | WebCeph V15.0 FACAD | Manual tracing | AI-based tracing: Not yet ready to replace semi-automated computer-aided methods |
| 20. | Prince 2023 [41] | India | 50 | NP | NP | AutoCEPH© | The cephalograms were printed on 8 × 10-in size radiographic film using a compatible X-ray printer. | WebCeph™ AI software: High agreement with validated methods—AutoCEPH© and manual tracing. |
| Study ID | Objective Clearly Stated? | Study Population Clearly Defined? | Participation Rate at Least 50%? | Subjects Comparable? | Justification of Sample Size? | Reliability of Outcome Measures? | Assessors Blinding? | Adjustment for Confounders? | Quality of Studies |
|---|---|---|---|---|---|---|---|---|---|
| Navarro 2013 [22] | Yes | Yes | Yes | Yes | Yes | Yes | No | No | Good |
| Goracci 2014 [23] | Yes | Yes | Yes | Yes | No | Yes | No | No | Good |
| Iacob 2014 [24] | Yes | Yes | Yes | Yes | No | Yes | No | No | Good |
| Tanwani 2014 [25] | Yes | Yes | Unclear | Yes | No | Yes | Unclear | No | Fair |
| Farooq 2016 [26] | Yes | Yes | Yes | Yes | No | Yes | No | No | Good |
| Kamath 2016 [27] | Yes | Yes | Unclear | Yes | No | Yes | No | No | Fair |
| Lindner 2016 [28] | Yes | Yes | Yes | Yes | No | Yes | No | No | Good |
| Mahto 2016 [29] | Yes | Yes | Yes | Yes | No | Yes | No | No | Good |
| Kasinathan 2017 [30] | Yes | Yes | Unclear | Yes | No | Yes | No | No | Fair |
| Anuwongnukro 2018 [31] | Yes | Yes | Yes | Yes | No | Yes | No | Yes | Good |
| Hassan 2019 [32] | Yes | Yes | Yes | Yes | No | Yes | No | No | Good |
| Izgi 2019 [33] | Yes | Yes | Yes | Yes | No | Yes | No | No | Good |
| Mohan 2021 [34] | Yes | Yes | Yes | Yes | No | Yes | No | No | Good |
| Zamrik 2021 [35] | Yes | Yes | Yes | Yes | No | Yes | No | No | Good |
| Katyal 2022 [36] | Yes | Yes | Yes | Yes | No | Yes | No | No | Good |
| Klinic 2022 [37] | Yes | Yes | Yes | Yes | No | Yes | No | No | Good |
| Salgado 2022 [38] | No | Unclear | Yes | Unclear | No | Yes | No | No | Poor |
| Khan 2023 [39] | Yes | Yes | Yes | Yes | Yes | Yes | Unclear | No | Good |
| Khattri 2023 [40] | Yes | Yes | Yes | Yes | No | Yes | Unclear | No | Good |
| Prince 2023 [41] | Yes | Yes | Yes | Yes | No | Yes | No | No | Good |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Narkhede, S.; Rao, P.; Sawant, V.; Sachdev, S.S.; Arora, S.; Pawar, A.M.; Reda, R.; Testarelli, L. Digital versus Manual Tracing in Cephalometric Analysis: A Systematic Review and Meta-Analysis. J. Pers. Med. 2024, 14, 566. https://doi.org/10.3390/jpm14060566
Narkhede S, Rao P, Sawant V, Sachdev SS, Arora S, Pawar AM, Reda R, Testarelli L. Digital versus Manual Tracing in Cephalometric Analysis: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine. 2024; 14(6):566. https://doi.org/10.3390/jpm14060566
Chicago/Turabian StyleNarkhede, Sameer, Paritosh Rao, Veera Sawant, Sanpreet Singh Sachdev, Suraj Arora, Ajinkya M. Pawar, Rodolfo Reda, and Luca Testarelli. 2024. "Digital versus Manual Tracing in Cephalometric Analysis: A Systematic Review and Meta-Analysis" Journal of Personalized Medicine 14, no. 6: 566. https://doi.org/10.3390/jpm14060566
APA StyleNarkhede, S., Rao, P., Sawant, V., Sachdev, S. S., Arora, S., Pawar, A. M., Reda, R., & Testarelli, L. (2024). Digital versus Manual Tracing in Cephalometric Analysis: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine, 14(6), 566. https://doi.org/10.3390/jpm14060566