
Effects of NF-κB Inhibitor on Sepsis Depend on the Severity and Phase of the Animal Sepsis Model

 , ,
, ,  and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
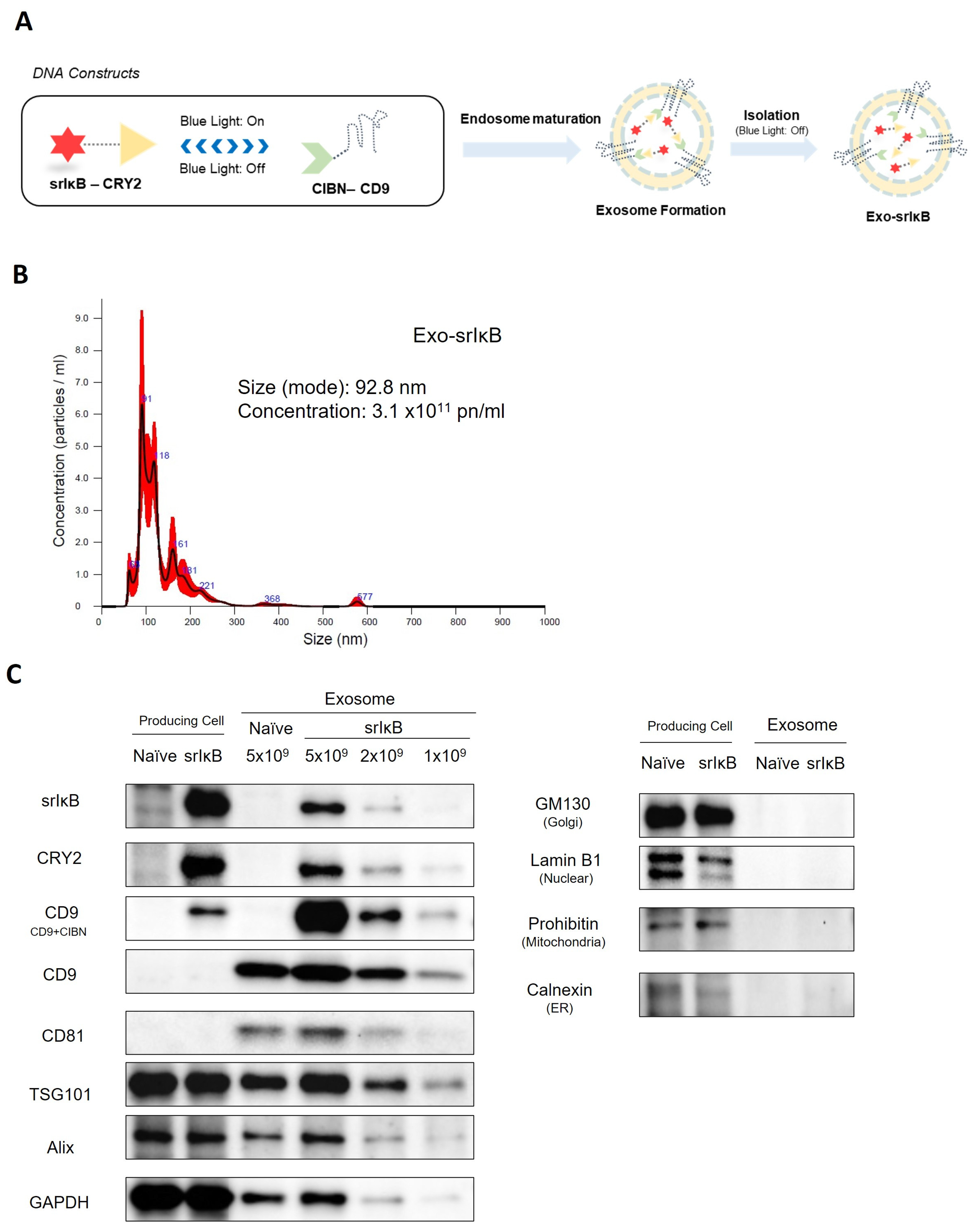
2.1. Exosomes Production
2.2. Nanoparticle Tracking Analysis
2.3. Western Blotting
2.4. In Vivo Sepsis Model Induction
2.5. Kidney Cytokines (Enzyme-Linked Immunosorbent Assays (ELISA))
2.6. Plasma Lactate, Glucose, Arterial Blood Gas Analysis, and Electrolytes
2.7. Statistical Analysis
3. Results
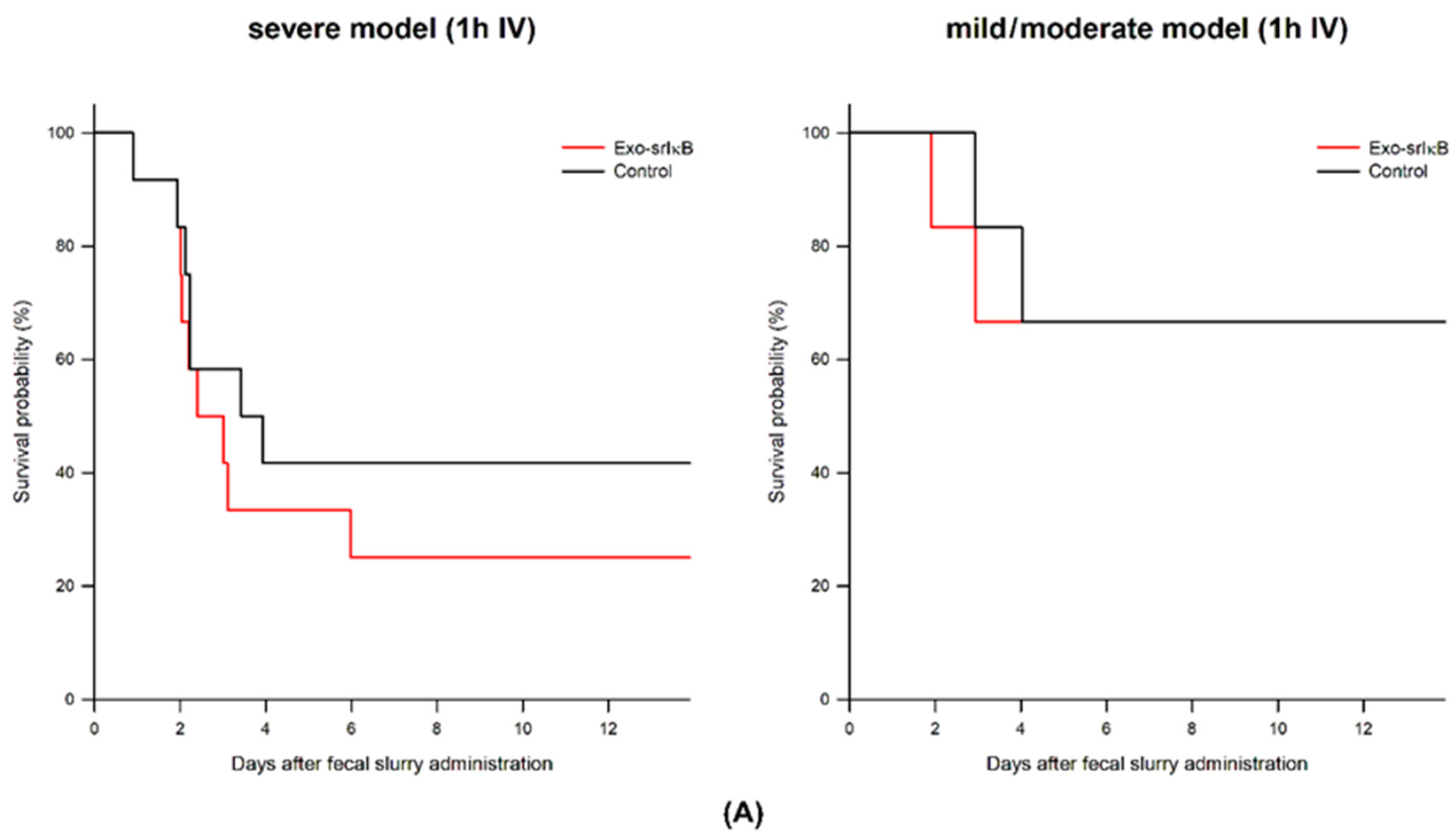
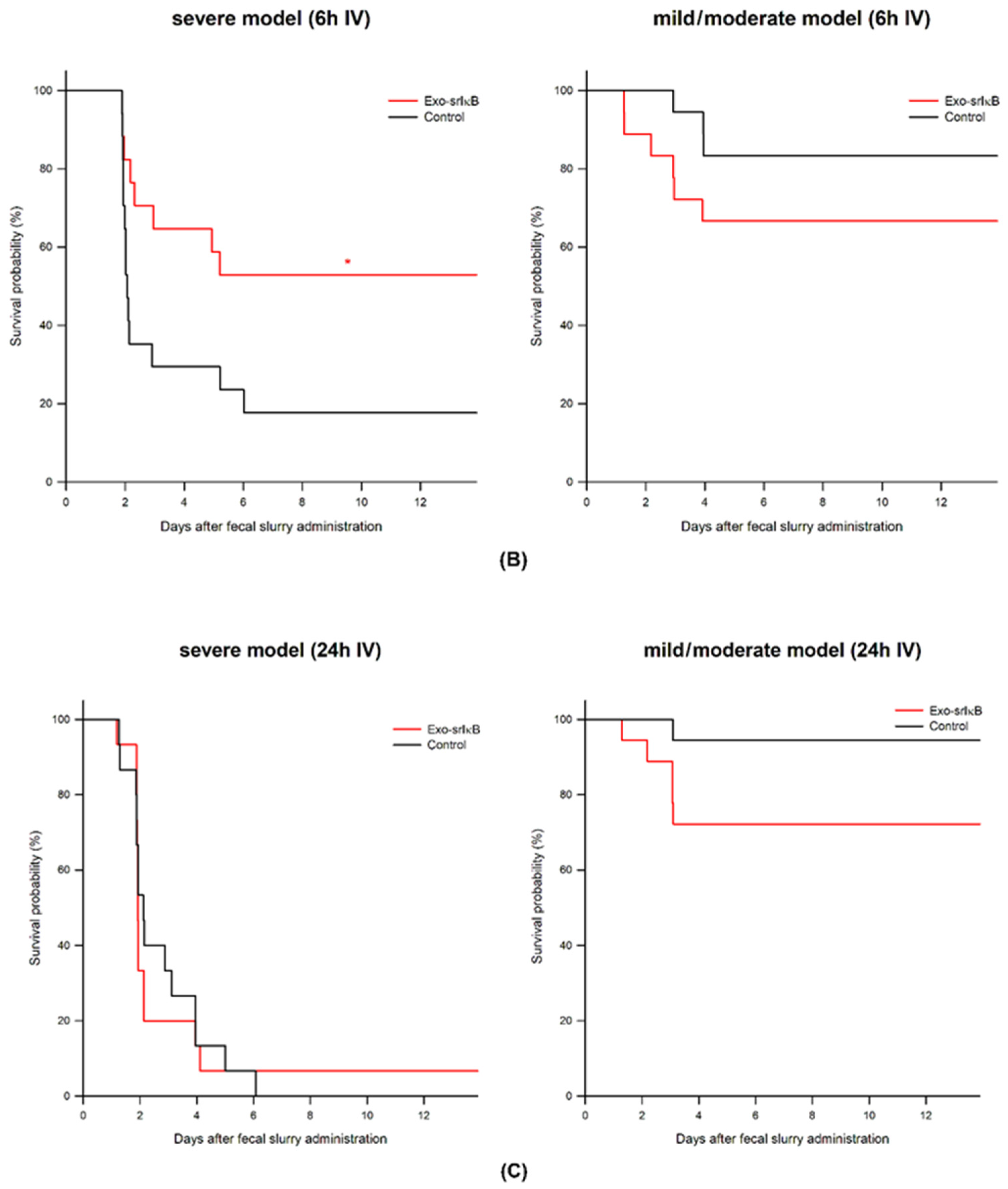
3.1. Survival Study According to the Exo-srIκB Depending on Severity of Sepsis and Phase of Sepsis
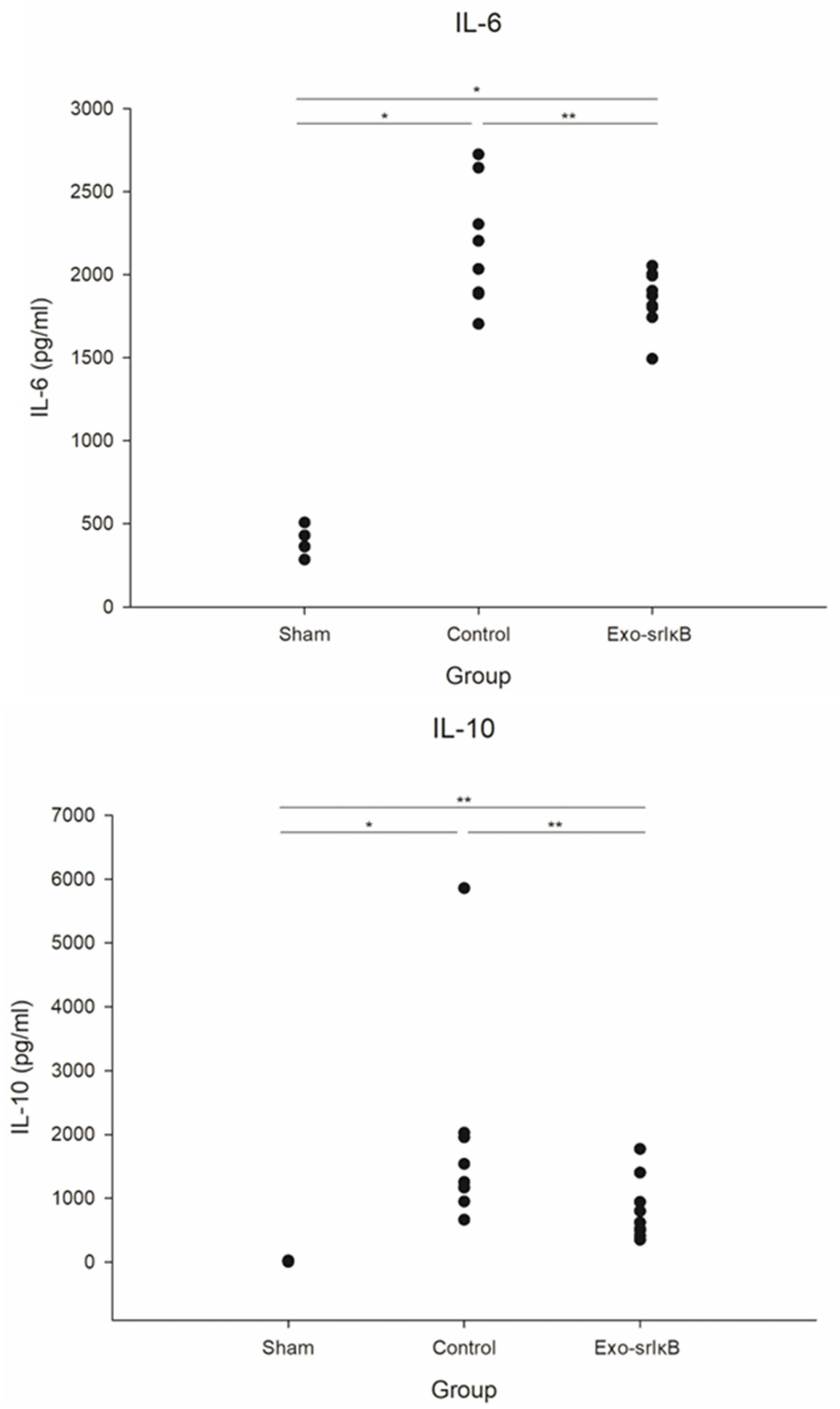
3.2. Kidney Cytokines
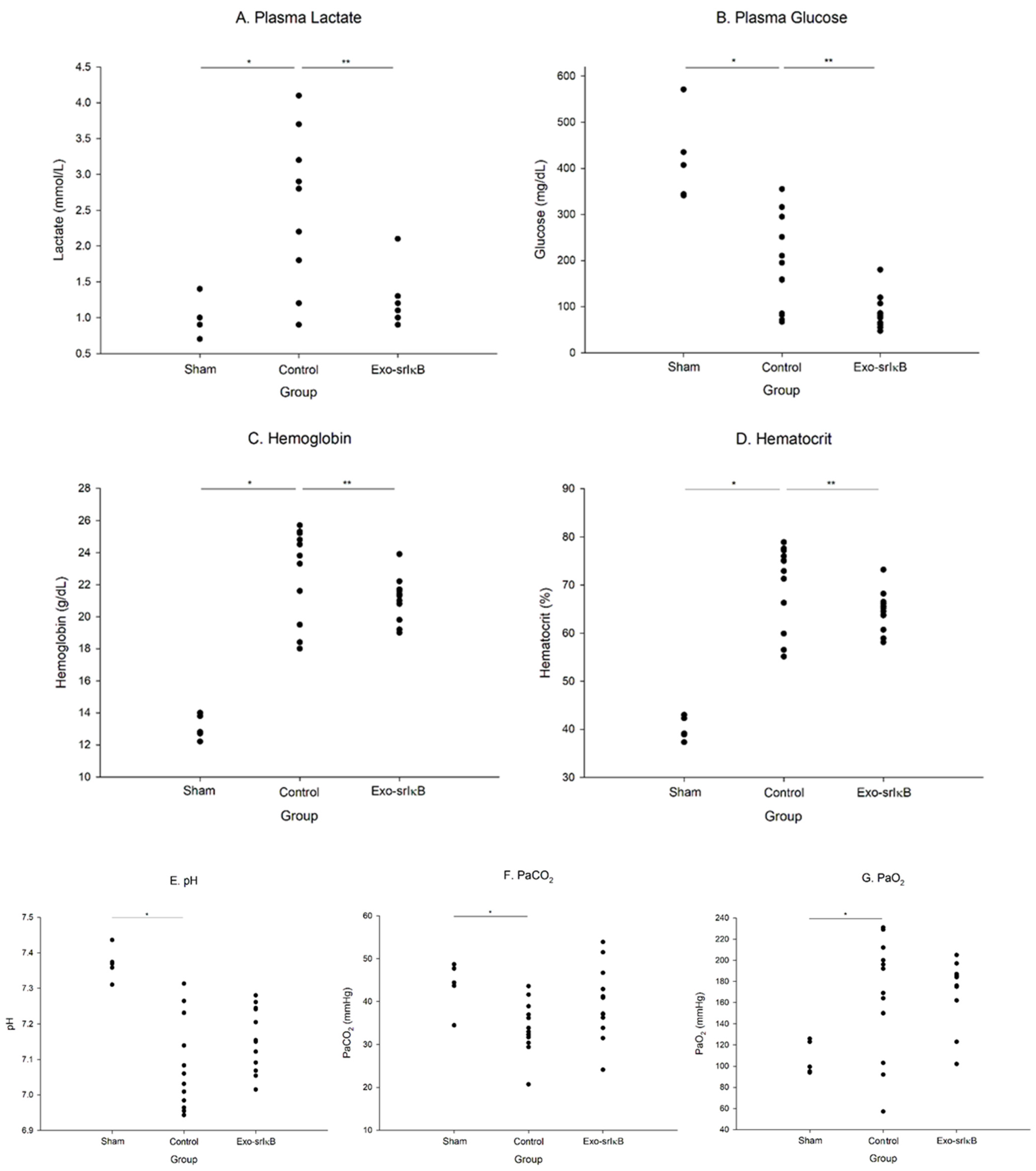
3.3. Plasma Lactate, Glucose, Arterial Blood Gas Analysis, and Electrolytes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fajgenbaum, D.C.; June, C.H. Cytokine Storm. N. Engl. J. Med. 2020, 383, 2255–2273. [Google Scholar] [CrossRef] [PubMed]
- Bone, R.C. Toward a theory regarding the pathogenesis of the systemic inflammatory response syndrome: What we do and do not know about cytokine regulation. Crit. Care Med. 1996, 24, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Hotchkiss, R.S.; Moldawer, L.L.; Opal, S.M.; Reinhart, K.; Turnbull, I.R.; Vincent, J.L. Sepsis and septic shock. Nat. Rev. Dis. Primers 2016, 2, 16045. [Google Scholar] [CrossRef] [PubMed]
- Oczkowski, S.; Alshamsi, F.; Belley-Cote, E.; Centofanti, J.E.; Hylander Møller, M.; Nunnaly, M.E.; Alhazzani, W. Surviving Sepsis Campaign Guidelines 2021: Highlights for the practicing clinician. Pol. Arch. Intern. Med. 2022, 132, 16290. [Google Scholar] [CrossRef] [PubMed]
- Cavaillon, J.M.; Singer, M.; Skirecki, T. Sepsis therapies: Learning from 30 years of failure of translational research to propose new leads. EMBO Mol. Med. 2020, 12, e10128. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.; Park, J.E.; Kim, A.; Hwang, S.; Bae, J.; Shin, T.G.; Kim, K. The DEXA-SEPSIS study protocol: A phase II randomized double-blinded controlled trial of the effect of early dexamethasone in high-risk sepsis patients. Clin. Exp. Emerg. Med. 2022, 9, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.J.; Lee, M.J.; Bae, J.; Lee, J.H.; Lee, H.A.R.; Mun, S.; Kim, Y.S.; Yune, C.J.; Chung, T.N.; Kim, K. Effects of Glucocorticoid Therapy on Sepsis Depend Both on the Dose of Steroids and on the Severity and Phase of the Animal Sepsis Model. Life 2022, 12, 421. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.; Kim, Y.; Mirzaaghasi, A.; Heo, J.; Kim, Y.N.; Shin, J.H.; Kim, S.; Kim, N.H.; Cho, E.S.; In Yook, J.; et al. Exosome-based delivery of super-repressor IκBα relieves sepsis-associated organ damage and mortality. Sci. Adv. 2020, 6, eaaz6980. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.H.; Ryu, S.W.; Choi, H.; You, S.; Park, J.; Choi, C. Manufacturing Therapeutic Exosomes: From Bench to Industry. Mol. Cells 2022, 45, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.J.; Kim, K.; Jo, Y.H.; Lee, J.H.; Hwang, J.E. Dose-dependent mortality and organ injury in a cecal slurry peritonitis model. J. Surg. Res. 2016, 206, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.W.; Lee, M.J.; Chung, T.N.; Lee, H.A.R.; Lee, J.H.; Choi, S.Y.; Park, Y.J.; Kim, C.H.; Jin, I.; Kim, S.H.; et al. The immune modulatory effects of mitochondrial transplantation on cecal slurry model in rat. Crit. Care 2021, 25, 20. [Google Scholar] [CrossRef] [PubMed]
- Murando, F.; Peloso, A.; Cobianchi, L. Experimental Abdominal Sepsis: Sticking to an Awkward but Still Useful Translational Model. Mediat. Inflamm. 2019, 2019, 8971036. [Google Scholar] [CrossRef] [PubMed]
- Nemzek, J.A.; Hugunin, K.M.; Opp, M.R. Modeling sepsis in the laboratory: Merging sound science with animal well-being. Comp. Med. 2008, 58, 120–128. [Google Scholar] [PubMed]
- Suzuki, E.; Umezawa, K. Inhibition of macrophage activation and phagocytosis by a novel NF-kappaB inhibitor, dehydroxymethylepoxyquinomicin. Biomed. Pharmacother. 2006, 60, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; Elmahi, E.; et al. Dexamethasone in Hospitalized Patients with Covid-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef] [PubMed]
- Kocks, J.; Kerkhof, M.; Scherpenisse, J.; van de Maat, A.; van Geer-Postmus, I.; le Rütte, T.; Schaart, J.; Gans, R.O.B.; Kerstjens, H.A.M. A potential harmful effect of dexamethasone in non-severe COVID-19: Results from the COPPER-pilot study. ERJ Open Res. 2022, 8, 00129. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, Y.J.; Bae, J.; Yoo, J.-K.; Ahn, S.-H.; Park, S.Y.; Kim, Y.-S.; Lee, M.J.; Moon, S.Y.; Chung, T.N.; Choi, C.; et al. Effects of NF-κB Inhibitor on Sepsis Depend on the Severity and Phase of the Animal Sepsis Model. J. Pers. Med. 2024, 14, 645. https://doi.org/10.3390/jpm14060645
Park YJ, Bae J, Yoo J-K, Ahn S-H, Park SY, Kim Y-S, Lee MJ, Moon SY, Chung TN, Choi C, et al. Effects of NF-κB Inhibitor on Sepsis Depend on the Severity and Phase of the Animal Sepsis Model. Journal of Personalized Medicine. 2024; 14(6):645. https://doi.org/10.3390/jpm14060645
Chicago/Turabian StylePark, Ye Jin, Jinkun Bae, Jae-Kwang Yoo, So-Hee Ahn, Seon Young Park, Yun-Seok Kim, Min Ji Lee, Seon Young Moon, Tae Nyoung Chung, Chulhee Choi, and et al. 2024. "Effects of NF-κB Inhibitor on Sepsis Depend on the Severity and Phase of the Animal Sepsis Model" Journal of Personalized Medicine 14, no. 6: 645. https://doi.org/10.3390/jpm14060645
APA StylePark, Y. J., Bae, J., Yoo, J.-K., Ahn, S.-H., Park, S. Y., Kim, Y.-S., Lee, M. J., Moon, S. Y., Chung, T. N., Choi, C., & Kim, K. (2024). Effects of NF-κB Inhibitor on Sepsis Depend on the Severity and Phase of the Animal Sepsis Model. Journal of Personalized Medicine, 14(6), 645. https://doi.org/10.3390/jpm14060645