
Drug Survival, Safety, and Effectiveness of Secukinumab for up to 5 Years in Patients with Psoriasis and Psoriatic Arthritis: A Long-Term Real-Life Experience

 ,
, 
Abstract
1. Introduction
2. Methods
2.1. Objectives
2.2. Patients
2.3. Drug Survival
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cariti, C.; Dapavo, P.; Mastorino, L.; Ortoncelli, M.; Siliquini, N.; Merli, M.; Avallone, G.; Giordano, S.; Fabrizio, R.; Ribero, S.; et al. Comparison of secukinumab and Ixekizumab in psoriasis: A real-life cohort study on the efficacy and drug survival of 445 patients. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e233–e235. [Google Scholar] [CrossRef] [PubMed]
- Bugaut, H.; Aractingi, S. Major Role of the IL17/23 Axis in Psoriasis Supports the Development of New Targeted Therapies. Front. Immunol. 2021, 12, 621956. [Google Scholar] [CrossRef] [PubMed]
- Cheuk, S.; Martini, E.; Bergh, K.; Chang, D.; Rethi, B.; Ståhle, M.; Eidsmo, L. Granzyme A potentiates chemokine production in IL-17-stimulated keratinocytes. Exp. Dermatol. 2017, 26, 824–827. [Google Scholar] [CrossRef] [PubMed]
- Lockshin, B.; Balagula, Y.; Merola, J.F. Interleukin 17, inflammation, and cardiovascular risk in patients with psoriasis. J. Am. Acad. Dermatol. 2018, 79, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Branisteanu, D.E.; Cojocaru, C.; Diaconu, R.; Porumb, E.A.; Alexa, A.I.; Nicolescu, A.C.; Bogdanici, C.M.; Branisteanu, G.; Brihan, I.; Branisteanu, D.C.; et al. Update on the etiopathogenesis of psoriasis (Review). Exp. Ther. Med. 2022, 23, 201. [Google Scholar] [CrossRef] [PubMed]
- Kampylafka, E.; Simon, D.; D’Oliveira, I.; Linz, C.; Lerchen, V.; Englbrecht, M.; Rech, J.; Kleyer, A.; Sticherling, M.; Hueber, A.J.; et al. Disease interception with interleukin-17 inhibition in high-risk psoriasis patients with subclinical joint inflammation-data from the prospective IVEPSA study. Arthritis Res. Ther. 2019, 21, 178. [Google Scholar] [CrossRef]
- Langley, R.G.; Sofen, H.; Dei-Cas, I.; Reich, K.; Sigurgeirsson, B.; Warren, R.B.; Paul, C.; Tsai, T.-F.; Szepietowski, J.C.; Papavassilis, C.; et al. Secukinumab long-term efficacy and safety in psoriasis through to year 5 of treatment: Results of a randomized extension of the phase III ERASURE and FIXTURE trials. Br. J. Dermatol. 2023, 188, 198–207. [Google Scholar] [CrossRef] [PubMed]
- Langley, R.G.; Elewski, B.E.; Lebwohl, M.; Reich, K.; Griffiths, C.E.M.; Papp, K.; Papavassilis, C.; Puig, L.; Nakagawa, H.; Spelman, L.; et al. Secukinumab in plaque psoriasis—Results of two phase 3 trials. N. Engl. J. Med. 2014, 371, 326–338. [Google Scholar] [CrossRef] [PubMed]
- Gialouri, C.G.; Evangelatos, G.; Fragoulis, G.E. Choosing the Appropriate Target for the Treatment of Psoriatic Arthritis: TNFα, IL-17, IL-23 or JAK Inhibitors? Mediterr. J. Rheumatol. 2022, 33 (Suppl. S1), 150–161. [Google Scholar] [CrossRef]
- Avallone, G.; Cariti, C.; Dapavo, P.; Ortoncelli, M.; Conforto, L.; Mastorino, L.; Roccuzzo, G.; Cavallo, F.; Rubatto, M.; Ribero, S.; et al. Real-life comparison of secukinumab and ixekizumab in the treatment of pustular and erythrodermic psoriasis. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e574–e576. [Google Scholar] [CrossRef]
- Avallone, G.; Maronese, C.A.; Murgia, G.; Carrera, C.G.; Mastorino, L.; Roccuzzo, G.; Dapavo, P.; Alberti-Violetti, S.; Quaglino, P.; Ribero, S.; et al. Interleukin-17 vs. Interleukin-23 Inhibitors in Pustular and Erythrodermic Psoriasis: A Retrospective, Multicentre Cohort Study. J. Clin. Med. 2023, 12, 1662. [Google Scholar] [CrossRef]
- Gottlieb, A.B.; Kubanov, A.; Van Doorn, M.; Sullivan, J.; Papp, K.A.; You, R.; Frueh, J.A.; Regnault, P.; Frueh, J.A. Sustained efficacy of secukinumab in patients with moderate-to-severe palmoplantar psoriasis: 2·5-year results from GESTURE, a randomized, double-blind, placebo-controlled trial. Br. J. Dermatol. 2020, 182, 889–899. [Google Scholar] [CrossRef] [PubMed]
- Mendes-Bastos, P.; Morais, P.; Ferreira, P.; Loureiro, M.; Sanganha, J.; Santiago, L.; Basto, A.S.; Henrique, M. Persistence, effectiveness, and real-world outcomes in psoriasis patients treated with secukinumab in Portugal. Dermatol. Ther. 2022, 35, e15510. [Google Scholar] [CrossRef]
- Daudén, E.; de Lima, G.P.G.; Armesto, S.; Herrera-Acosta, E.; Vidal, D.; Villarasa, E.; Rivera, R.; de la Cueva, P.; Martorelli, A.; Llamas-Velasco, M.; et al. Multicenter Retrospective Study of Secukinumab Drug Survival in Psoriasis Patients in a Daily Practice Setting: A Long-Term Experience in Spain. Dermatol. Ther. 2021, 11, 2207–2215. [Google Scholar] [CrossRef] [PubMed]
- Torres, T.; Balato, A.; Conrad, C.; Dapavo, P.; Ferreira, P.; Gaiani, F.; Leite, L.; Malagoli, P.; Mendes-Bastos, P.; Chiricozzi, A.; et al. Secukinumab drug survival in patients with psoriasis: A multicenter, real-world, retrospective study. J. Am. Acad. Dermatol. 2019, 81, 273–275. [Google Scholar] [CrossRef]
- Ortolan, A.; Lorenzin, M.; Leo, G.; Pampaloni, F.; Messina, F.; Doria, A.; Piaserico, S.; Ramonda, R. Secukinumab Drug Survival in Psoriasis and Psoriatic Arthritis Patients: A24-Month Real-Life Study. Dermatology 2022, 238, 897–903. [Google Scholar] [CrossRef] [PubMed]
- Sotiriou, E.; Bakirtzi, K.; Vakirlis, E.; Papadimitriou, I.; Eftychidou, P.; Trifona, M.; Lallas, A.; Ioannides, D. Long-term drug survival of secukinumab in real life in the era of novel biologics: A 5-year, retrospective study, including difficult-to-treat areas. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e626–e627. [Google Scholar] [CrossRef]
- Nguyen, H.T.; Pham, N.T.U.; Tran, T.N.A.; Pham, N.N.; Bui, Y.T.; Vu, T.T.P. Long-Term Effectiveness and Drug Survival of Secukinumab in Vietnamese Patients with Psoriasis: Results from a Retrospective ENHANCE Study. Dermatol. Ther. 2023, 13, 465–476. [Google Scholar] [CrossRef]
- Foley, P.; Manuelpillai, N.; Dolianitis, C.; Cains, G.D.; Mate, E.; Tronnberg, R.; Baker, C. Secukinumab treatment demonstrated high drug survival and sustained effectiveness in patients with severe chronic plaque psoriasis: 21-month analysis in Australian routine clinical practice (SUSTAIN study). Australas. J. Dermatol. 2022, 63, 303–311. [Google Scholar] [CrossRef]
- Chatzimichail, G.; Günther, J.; Ständer, S.; Thaçi, D. Drug survival of secukinumab, ustekinumab, and certolizumab pegol in psoriasis: A 2-year, monocentric, retrospective study. J. Dermatol. Treat. 2022, 33, 1749–1753. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, X.; Yu, Y.; Yuan, L.; Yu, X.; Yang, B. A retrospective study to assess the efficacy, safety, and drug survival of secukinumab in plaque psoriasis patients in China. Dermatol. Ther. 2021, 34, e15081. [Google Scholar] [CrossRef]
- Alonso, S.; Villa, I.; Fernández, S.; Martín, J.L.; Charca, L.; Pino, M.; Riancho, L.; Morante, I.; Santos, M.; Queiro, R.; et al. Multicenter Study of Secukinumab Survival and Safety in Spondyloarthritis and Psoriatic Arthritis: SEcukinumab in Cantabria and ASTURias Study. Front. Med. 2021, 8, 679009. [Google Scholar] [CrossRef] [PubMed]
- Fujita, H.; Ohtsuki, M.; Morita, A.; Nagao, R.; Seko, N.; Matsumoto, K.; Tani, Y.; Terui, T. Safety and effectiveness of secukinumab in psoriasis vulgaris and psoriatic arthritis: Real-world evidence in Japan. J. Dermatol. 2021, 48, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Notario, J.; Deza, G.; Vilarrasa, E.; Valentí, F.; Muñoz, C.; Mollet, J.; Carrascosa, J.-M.; del Alcázar, E.; Alsina, M.; Ferran, M.; et al. Treatment of patients with plaque psoriasis with secukinumab in a real-life setting: A 52-week, multicenter, retrospective study in Spain. J. Dermatol. Treat. 2019, 30, 424–429. [Google Scholar] [CrossRef]
- Ruiz-Villaverde, R.; Rodríguez Fernández-Freire, L.; Galán-Gutiérrez, M.; Armario-Hita, J.C.; Martinez-Pilar, L. Secukinumab: Drug Survival in Clinical Practice Settings. Secukinumab: Supervivencia en práctica clínica real. Actas Dermosifiliogr. 2021, 112, 361–364. [Google Scholar] [CrossRef] [PubMed]
- Augustin, M.; Sator, P.G.; von Kiedrowski, R.; Conrad, C.; Rigopoulos, D.; Romanelli, M.; Ghislain, P.-D.; Torres, T.; Ioannides, D.; Aassi, M.; et al. Secukinumab demonstrated sustained retention, effectiveness and safety in a real-world setting in patients with moderate-to-severe plaque psoriasis: Long-term results from an interim analysis of the SERENA study. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 1796–1804. [Google Scholar] [CrossRef] [PubMed]
- Tada, Y.; Morita, A.; Yamanaka, K.; Kono, M.; Imafuku, S.; Okubo, Y.; Yamazaki, F.; Kawamura, T.; Itakura, A.; Ohtsuki, M.; et al. Real-world retention rates and effectiveness of secukinumab in psoriasis: Results from a multicenter cohort study (RAILWAY). J. Dermatol. 2023, 50, 1415–1426. [Google Scholar] [CrossRef]
- Zhou, H.; Wu, R.; Kong, Y.; Zhao, M.; Su, Y. Impact of smoking on psoriasis risk and treatment efficacy: A meta-analysis. J. Int. Med. Res. 2020, 48, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, C.W.; Loft, N.; Rasmussen, M.K.; Nissen, C.V.; Dam, T.N.; Ajgeiy, K.K.; Egeberg, A.; Lone, S.K.O.V. Predictors of Response to Biologics in Patients with Moderate-to-severe Psoriasis: A Danish Nationwide Cohort Study. Acta Derm.-Venereol. 2021, 101, adv00579. [Google Scholar] [CrossRef]
- Mourad, A.; Straube, S.; Armijo-Olivo, S.; Gniadecki, R. Factors predicting persistence of biologic drugs in psoriasis: A systematic review and meta-analysis. Br. J. Dermatol. 2019, 181, 450–458. [Google Scholar] [CrossRef]
- Constantin, M.M.; Bucur, S.; Mutu, C.C.; Poenaru, E.; Olteanu, R.; Ionescu, R.A.; Nicolescu, A.C.; Furtunescu, F.; Constantin, T. The Impact of Smoking on Psoriasis Patients with Biological Therapies in a Bucharest Hospital. J. Pers. Med. 2021, 11, 752. [Google Scholar] [CrossRef] [PubMed]
- Klavdianou, K.; Lazarini, A.; Grivas, A.; Tseronis, D.; Tsalapaki, C.; Rapsomaniki, P.; Antonatou, K.; Thomas, K.; Boumpas, D.; Vassilopoulos, D.; et al. Real Life Efficacy and Safety of Secukinumab in Biologic-Experienced Patients With Psoriatic Arthritis. Front. Med. 2020, 7, 288. [Google Scholar] [CrossRef]
- Orzan, O.A.; Țieranu, C.G.; Olteanu, A.O.; Dorobanțu, A.M.; Cojocaru, A.; Mihai, M.M.; Popa, L.G.; Gheorghiu, A.M.; Giurcăneanu, C.; Ion, A.; et al. An Insight on the Possible Association between Inflammatory Bowel Disease and Biologic Therapy with IL-17 Inhibitors in Psoriasis Patients. Pharmaceutics 2023, 15, 2171. [Google Scholar] [CrossRef] [PubMed]
- Krikelis, M.; Papathanasiou, E.; Leonidakis, G.; Pardalis, P.; Michopoulos, S.; Zampeli, E. New-Onset, Treatment-Resistant Inflammatory Bowel Disease after Administration of Secukinumab for Plaque Psoriasis: A Case Report and Review of the Existing Literature. Mediterr. J. Rheumatol. 2024, 35, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Tada, Y.; Soliman, A.M.; Ishii, K.; Sakuma, R.; Pinter, A.; Davis, M.; Nunag, D.; Buessing, M.; Puig, L.; Imafuku, S.; et al. Dose escalation of biologic treatment in patients with moderate-to-severe psoriasis in Japan. Exp. Dermatol. 2024, 33, e15067. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (a) General Characteristics of the Patients | ||||
|---|---|---|---|---|
| Patients (n = 255) | ||||
| Sex (M) % | 64.3% | |||
| Mean age (years) | 58 (SD 15) | |||
| Mean age of onset (years) | 36 (SD 18.2) | |||
| BMI (kg/m2) (mean) | 27.6 (SD 5.4) | |||
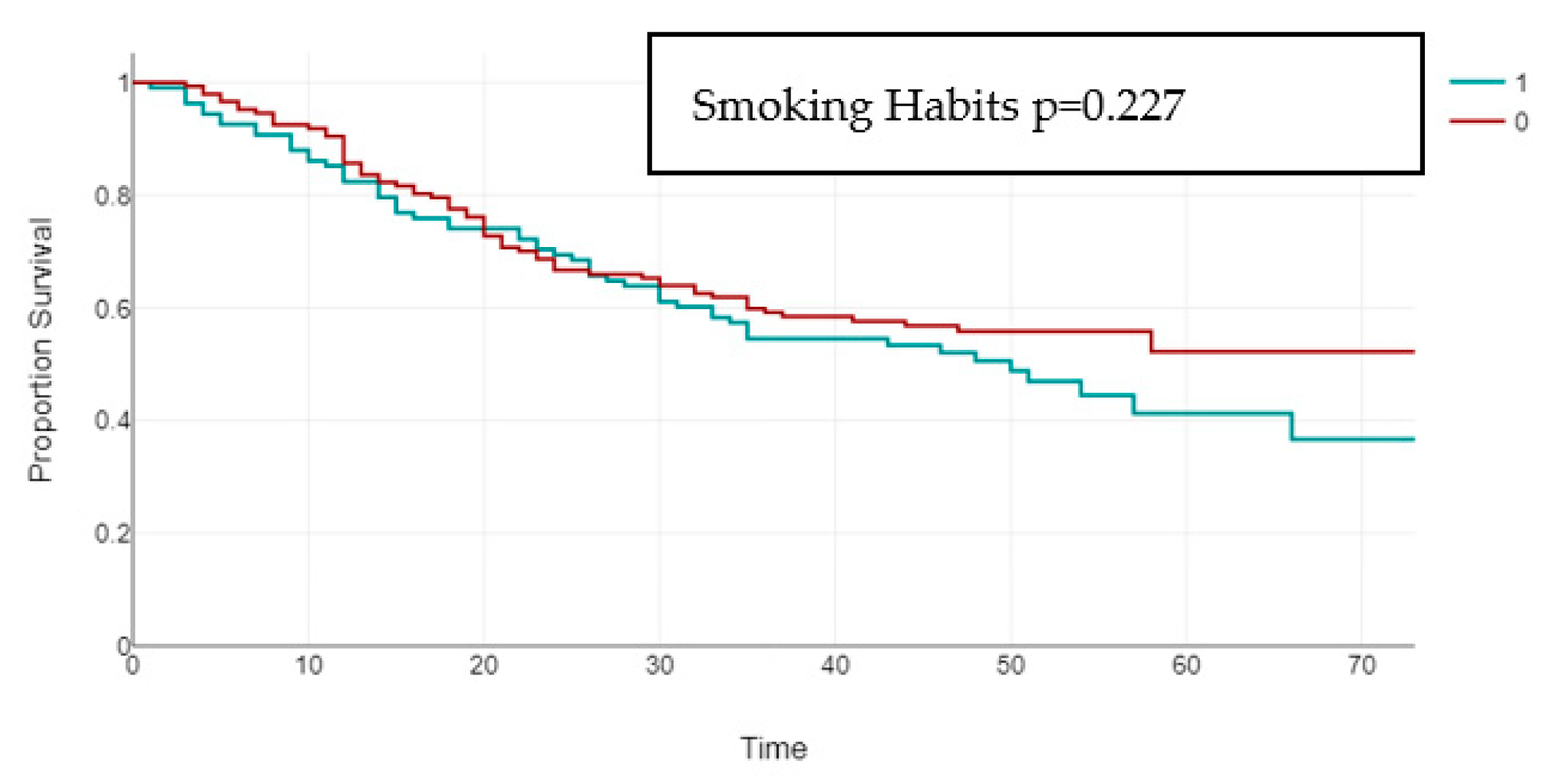
| Smoking Habits (yes) | 42.35% | |||
| PsA % | 35.7% | |||
| Obesity (BMI ≥ 30)% | 27.1% | |||
| CV comorbidities % | 45.6% | |||
| T2D | 13.4% | |||
| Bio-Naive | 37.7% | |||
| Difficult-site Involvement | 24% | |||
| PASI baseline (mean) | 15.8 (SD 5.7) | |||
| (b) Predictors of Secukinumab Interruption | ||||
| p | HR | Lower 95% CI | Upper 95% CI | |
| Age (years) | 0.19 | 1.01 | 0.99 | 1.03 |
| Sex (male) | 0.605 | 0.91 | 0.62 | 1.32 |
| Smoking Habits (yes) | 0.043 | 1.48 | 1.01 | 2.17 |
| Age of onset (years) | 0.078 | 0.99 | 0.97 | 1 |
| Difficult-site involvement | 0.365 | 0.82 | 0.54 | 1.26 |
| PsA | 0.81 | 1.05 | 0.71 | 1.56 |
| Bio-naive | 0.199 | 0.77 | 0.53 | 1.14 |
| Mean baseline PASI | 0.8 | 1 | 0.96 | 1.03 |
| Obesity (BMI ≥ 30) | 0.028 | 1.61 | 0.05 | 2.45 |
| CV comorbidities | 0.993 | 1 | 0.64 | 1.56 |
| T2D | 0.957 | 00.98 | 0.54 | 1.79 |
| BMI ≥ 30 | BMI < 30 | p | PSA | NON PSA | p | Bio-Exp | Bio-Naive | p | Difficult-Site | Non-Difficult-Site | p | Smokers | Non-Smokers | p | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PASI 100 16 W N°, % | 25/68, 36.8% | 81/186, 43.5% | 0.332 | 33/91, 36.3% | 73/163, 44.8% | 0.187 | 35/95, 36.8% | 71/159, 44.7% | 0.222 | 79/193, 40.9% | 26/60, 43.3% | 0.742 | 45/108, 41.7% | 61/146, 41.8% | 0.985 |
| PASI 90 16 W N°, % | 28/68, 41.1% | 90/186, 48.4% | 0.308 | 36/91, 39.6% | 82/163, 50.3% | 0.1 | 38/95, 40% | 80/159, 50.3% | 0.111 | 88/193, 45.6% | 29/60. 48.3% | 0.71 | 52/108, 48.1% | 66/146, 45.2% | 0.642 |
| PASI ≤ 3 16 W N°, % | 37/68, 54.4% | 115/186, 61.8% | 0.286 | 48/91, 52.7% | 104/163, 63.8% | 0.085 | 53/95, 55.8% | 99/159, 62.3% | 0.308 | 116/193, 60.1% | 35/60, 58.3% | 0.807 | 64/108, 59.3% | 88/146, 60.3% | 0.87 |
| PASI 100 28 W N°, % | 25/63, 39.7% | 100/181, 55.2% | 0.033 | 39/89, 43.8% | 86/155, 55.5% | 0.079 | 40/87, 46% | 85/157, 54% | 0.222 | 99/188, 52.7% | 25/55, 45.5% | 0.347 | 53/104, 51% | 72/140, 51.4% | 0.942 |
| PASI 90 28 W N°, % | 31/63, 49.2% | 116/181, 64.1% | 0.038 | 45/89, 50.6% | 102/155, 65.8% | 0.019 | 44/87, 50.6% | 103/157, 65.6% | 0.022 | 117/188, 62.2% | 29/55, 52.7% | 0.205 | 63/104, 60.6% | 84/140, 60% | 0.927 |
| PASI ≤ 3 28 W N°, % | 39/63, 61.9% | 137/181, 75.5% | 0.036 | 55/89, 61.8% | 121/155, 78.1% | 0.006 | 56/87, 64.4% | 120/157, 76.4% | 0.044 | 136/188, 72.3% | 39/55, 70.9% | 0.835 | 74/104, 71.2% | 102/140, 72.9% | 0.769 |
| PASI 100 52 W N°, % | 26/55, 47.3% | 108/172, 62.8% | 0.042 | 48/83, 57.8% | 86/144, 59.7% | 0.78 | 45/79, 57% | 89/148, 60.1% | 0.643 | 106/175, 60.6% | 27/51, 52.9% | 0.33 | 57/96, 59.4% | 77/131, 58.8% | 0.928 |
| PASI 90 52 N°, % W | 33/55, 60% | 122/172, 70.9% | 0.129 | 53/83, 63.9% | 102/144, 70.8% | 0.277 | 50/79, 63.3% | 105/148, 70.9% | 0.238 | 124/175, 70.9% | 30/51, 58.8% | 0.105 | 66/96, 71% | 89/131, 67.9% | 0.897 |
| PASI ≤ 3 52 W N°, % | 39/55, 70.9% | 142/172, 82.6% | 0.061 | 62/83, 74.7% | 119/144, 82.6% | 0.152 | 61/79, 77.2% | 120/148, 81.1% | 0.49 | 144/175, 82.3% | 36/51, 70.6% | 0.068 | 78/96, 81.3% | 103/131, 78.6% | 0.627 |
| PASI 100 78 W N°, % | 13/27, 48.1% | 57/100, 57% | 0.412 | 21/47, 44.7% | 49/80, 61.3% | 0.07 | 22/47, 46.8% | 48/80, 60% | 0.149 | 57/101, 56.4% | 13/26, 50% | 0.556 | 25/49, 51% | 45/78, 57.7% | 0.462 |
| PASI 90 78 W N°, % | 17/27, 63% | 65/100, 65% | 0.359 | 26/47, 55.3% | 56/80, 70% | 0.095 | 25/47, 53.2% | 57/80, 71.3% | 0.04 | 66/101, 65.3% | 16/26, 61.5% | 0.717 | 30/49, 61.2% | 52/78, 66.7% | 0.533 |
| PASI ≤ 3 78 W N°, % | 21/27, 77.8% | 84/100, 84% | 0.448 | 37/47, 78.7% | 68/80, 85% | 0.367 | 35/47, 74.5% | 70/80, 87.5% | 0.061 | 84/101, 83.2% | 21/26, 80.8% | 0.773 | 41/49, 83.7% | 64/78, 82.1% | 0.814 |
| PASI 100 104 W N°, % | 8/23, 34.8% | 52/91, 57.1% | 0.055 | 16/38, 42.1% | 44/76, 57.9% | 0.111 | 21/42, 50% | 39/72, 54.2% | 0.667 | 52/90, 57.8% | 8/24, 33.3% | 0.033 | 24/44, 54.5% | 36/70, 51.4% | 0.746 |
| PASI 90 104 W N°, % | 12/23, 52.2% | 57/91, 62.6% | 0.359 | 20/38, 52.6% | 49/76, 64.5% | 0.223 | 24/42, 57.1% | 45/72, 62.5% | 0.572 | 58/90, 64.4% | 11/24, 45.8% | 0.097 | 26/44, 59.1% | 43/70, 61.4% | 0.804 |
| PASI <3 104 W N°, % | 14/23, 60.9% | 75/91, 82.4% | 0.026 | 30/38, 78.9% | 59/76, 77.6% | 0.873 | 32/42, 83.3% | 57/72, 79.2% | 0.711 | 76/90, 84.4% | 13/24, 54.2% | 0.001 | 34/44, 77.3% | 55/70, 78.6% | 0.87 |
| PASI 100 156 W N°, % | 7/18, 38.9% | 45/77, 58.4% | 0.134 | 19/36, 52.7% | 33/59, 55.9% | 0.764 | 22/35, 62.9% | 30/60, 50% | 0.225 | 45/76, 59.2% | 7/19, 36.8% | 0.08 | 20/34, 58.8% | 32/61, 52.5% | 0.55 |
| PASI 90 156 W N°, % | 11/18, 61.1% | 56/77, 72.7% | 0.33 | 25/36, 69.4% | 42/59, 71.1% | 0.857 | 26/35, 74.3% | 41/60, 68.3% | 0.539 | 57/76, 75% | 10/19, 52.6% | 0.056 | 25/34, 73.5% | 42/61, 68.9% | 0.632 |
| PASI <3 156 W N°, % | 14/18, 77.8% | 65/77, 84.4% | 0.498 | 28/36, 77.8% | 51/59, 86.4% | 0.274 | 30/35, 85.7% | 49/60, 81.7% | 0.611 | 65/76, 85.5% | 14/19, 73.7% | 0.217 | 28/34, 82.4% | 51/61, 83.6% | 0.876 |
| PASI 100 208 W N°, % | 2/8, 25% | 29/50, 58% | 0.082 | 10/22, 45.5% | 21/36, 58.3% | 0.34 | 8/19, 42.1% | 23/39, 59% | 0.227 | 27/48, 56.3% | 4/10, 40% | 0.349 | 12/21, 57.1% | 19/37, 51.4% | 0.671 |
| PASI 90 208 W N°, % | 5/8, 62.5% | 35/50, 70% | 0.67 | 12/22, 54.5% | 28/36, 77.8% | 0.064 | 10/19, 52.6% | 30/39, 76.9% | 0.061 | 33/48, 68.8% | 7/10, 70% | 0.938 | 15/21, 71.4% | 25/37, 67.6% | 0.76 |
| PASI <3 208 W N°, % | 5/8, 62.5% | 43/50, 86% | 0.102 | 17/22, 77.3% | 31/36, 86.1% | 0.387 | 13/19, 68.4% | 35/39, 89.7% | 0.044 | 39/48, 81.3% | 9/10, 90% | 0.505 | 18/21, 85.7% | 30/37, 81.1% | 0.227 |
| PASI 100 260 W N°, % | 2/3, 66.6% | 10/14, 71.4% | 0.87 | 5/7, 71.4% | 7/10, 70% | 0.1 | 7/10, 70% | 5/7, 71.4% | 0.949 | 11/16, 68.8% | 1/1, 100% | 0.506 | 5/6, 83.3% | 7/11, 63.6 | 0.6 |
| PASI 90 260 W N°, % | 2/3, 66.6% | 13/14, 92.9% | 0.201 | 5/7, 71.4% | 10/10, 100% | 0.072 | 8/10, 80% | 7/7, 100% | 0.208 | 14/16, 87.5% | 1/1, 100% | 0.707 | 5/6, 83.3% | 10/11, 90.9% | 1 |
| PASI <3 260 W N°, % | 3/3, 100% | 14/14, 100% | 1 | 7/7, 100% | 10/10, 100% | 1 | 10/10, 100% | 7/7, 100% | 1 | 16/16, 100% | 1/1, 100% | 1 | 6/6 100% | 11/11 100% | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mastorino, L.; Dapavo, P.; Cariti, C.; Susca, S.; Siliquini, N.; Ortoncelli, M.; Stroppiana, E.; Verrone, A.; Giunipero di Corteranzo, I.; Leo, F.; et al. Drug Survival, Safety, and Effectiveness of Secukinumab for up to 5 Years in Patients with Psoriasis and Psoriatic Arthritis: A Long-Term Real-Life Experience. J. Pers. Med. 2024, 14, 718. https://doi.org/10.3390/jpm14070718
Mastorino L, Dapavo P, Cariti C, Susca S, Siliquini N, Ortoncelli M, Stroppiana E, Verrone A, Giunipero di Corteranzo I, Leo F, et al. Drug Survival, Safety, and Effectiveness of Secukinumab for up to 5 Years in Patients with Psoriasis and Psoriatic Arthritis: A Long-Term Real-Life Experience. Journal of Personalized Medicine. 2024; 14(7):718. https://doi.org/10.3390/jpm14070718
Chicago/Turabian StyleMastorino, Luca, Paolo Dapavo, Caterina Cariti, Sara Susca, Niccolò Siliquini, Michela Ortoncelli, Elena Stroppiana, Anna Verrone, Isotta Giunipero di Corteranzo, Francesco Leo, and et al. 2024. "Drug Survival, Safety, and Effectiveness of Secukinumab for up to 5 Years in Patients with Psoriasis and Psoriatic Arthritis: A Long-Term Real-Life Experience" Journal of Personalized Medicine 14, no. 7: 718. https://doi.org/10.3390/jpm14070718
APA StyleMastorino, L., Dapavo, P., Cariti, C., Susca, S., Siliquini, N., Ortoncelli, M., Stroppiana, E., Verrone, A., Giunipero di Corteranzo, I., Leo, F., Quaglino, P., & Ribero, S. (2024). Drug Survival, Safety, and Effectiveness of Secukinumab for up to 5 Years in Patients with Psoriasis and Psoriatic Arthritis: A Long-Term Real-Life Experience. Journal of Personalized Medicine, 14(7), 718. https://doi.org/10.3390/jpm14070718