
A Comparison of Norepinephrine versus Phenylephrine to Prevent Hypotension after Spinal Anesthesia for Cesarean Section: Systematic Review and Meta-Analysis

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
- Patients (P): all parturient undergoing cesarean section undergoing spinal anesthesia.
- Intervention (I): intravenous (IV) bolus or infusion of norepinephrine.
- Comparison (C): intravenous (IV) bolus or infusion of phenylephrine.
- Outcome measurements (O): The primary outcome of this study was the umbilical artery (UA) or umbilical vein (UV) pH as the neonatal condition at birth, and the secondary outcome was umbilical artery (UA) or umbilical vein (UV) base excess (BE) as an additional prognostic value over the measurement of umbilical pH.
- Study design (SD): The full reports of randomized controlled trials (RCTs) were included. The exclusion criteria were observational studies, conference abstracts, posters, case reports, case series, comments or letters to the editor, reviews, and laboratory or animal studies.
2.2. Information Source and Search Strategy
2.3. Study Selection
2.4. Data Extraction
2.5. Risk of Bias
2.6. Data Analysis
2.7. Quality of the Evidence
3. Results
3.1. Search Selection
3.2. Description of Trials
3.3. Umbilical Artery (UA) or Umbilical Vein (UV) pH
3.4. Base Excess
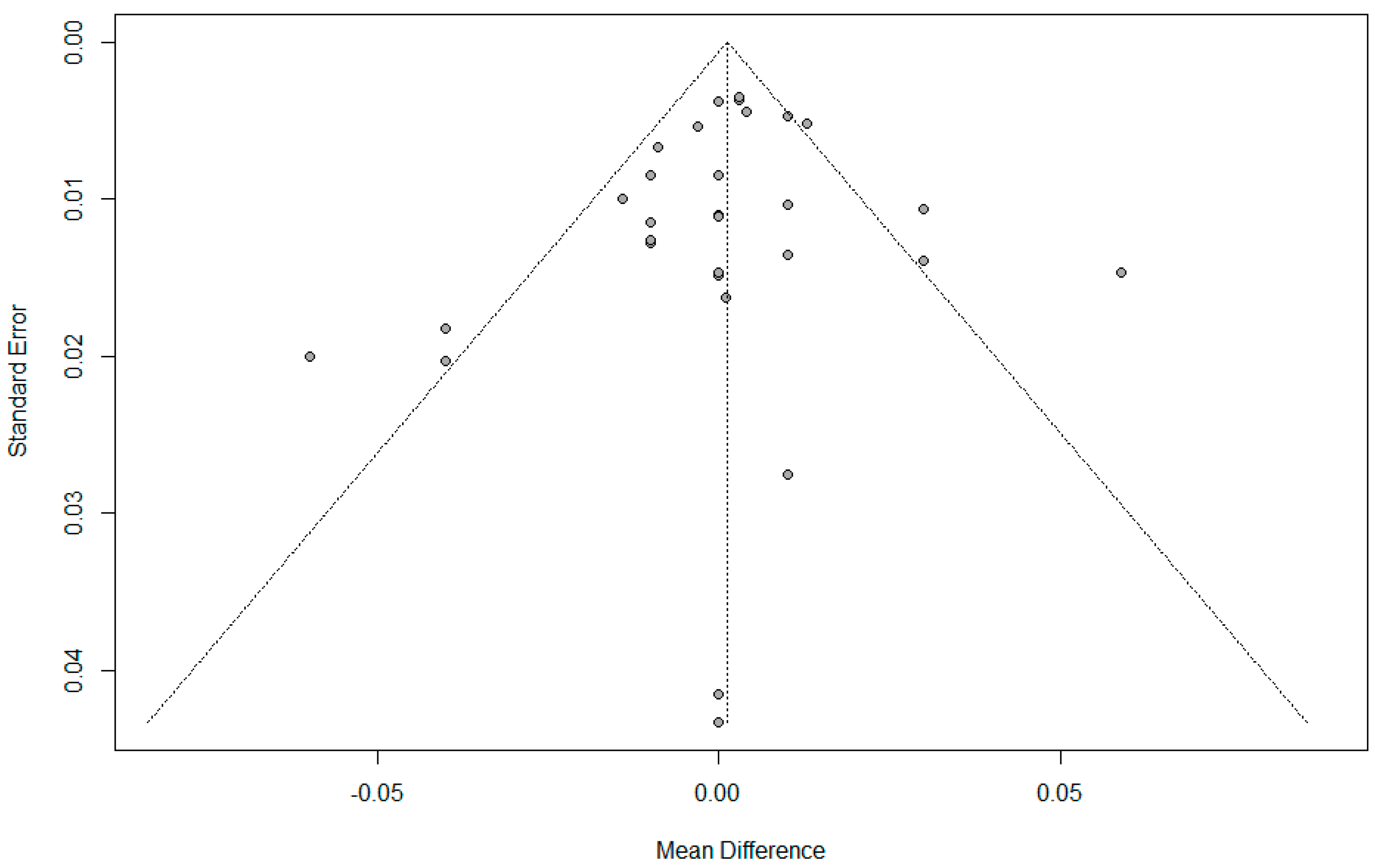
3.5. Risk of Bias
3.6. GRADE
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- James, F.M., 3rd; Greiss, F.C., Jr.; Kemp, R.A. An evaluation of vasopressor therapy for maternal hypotension during spinal anesthesia. Anesthesiology 1970, 33, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Ngan Kee, W.D.; Khaw, K.S.; Tan, P.E.; Ng, F.F.; Karmakar, M.K. Placental transfer and fetal metabolic effects of phenylephrine and ephedrine during spinal anesthesia for cesarean delivery. Anesthesiology 2009, 111, 506–512. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.J.; Cho, H.J.; Lee, I.H.; Jee, Y.S.; Kim, S.M. Comparison of hemodynamic changes between phenylephrine and combined phenylephrine and glycopyrrolate groups after spinal anesthesia for cesarean delivery. Korean J. Anesthesiol. 2012, 62, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Ngan Kee, W.D.; Lee, S.W.; Ng, F.F.; Tan, P.E.; Khaw, K.S. Randomized double-blinded comparison of norepinephrine and phenylephrine for maintenance of blood pressure during spinal anesthesia for cesarean delivery. Anesthesiology 2015, 122, 736–745. [Google Scholar] [CrossRef] [PubMed]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart L., A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef] [PubMed]
- Cochrane Handbook for Systematic Reviews of Interventions; Cochrane: Chichester, UK, 2019.
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Viera, A.J.; Garrett, J.M. Understanding interobserver agreement: The kappa statistic. Fam. Med. 2005, 37, 360–363. [Google Scholar] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; Emberson, J.R.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Atkins, D.; Best, D.; Briss, P.A.; Eccles, M.; Falck-Ytter, Y.; Flottorp, S.; Guyatt, G.H.; Harbour, R.T.; Haugh, M.C.; Henry, D.; et al. Grading quality of evidence and strength of recommendations. BMJ 2004, 328, 1490. [Google Scholar] [PubMed]
- Wang, X.; Mao, M.; Liu, S.; Xu, S.; Yang, J. A Comparative Study of Bolus Norepinephrine, Phenylephrine, and Ephedrine for the Treatment of Maternal Hypotension in Parturients with Preeclampsia During Cesarean Delivery Under Spinal Anesthesia. Med. Sci. Monit. 2019, 25, 1093–1101. [Google Scholar] [CrossRef] [PubMed]
- Eskandr, A.M.; Ahmed, A.M.; Bahgat, N.M.E. Comparative Study Among Ephedrine, Norepinephrine and Phenylephrine Infusions to Prevent Spinal Hypotension During Cesarean Section. A Randomized Controlled Double-Blind Study. Egypt. J. Anaesth. 2021, 37, 295–301. [Google Scholar] [CrossRef]
- Dong, L.; Dong, Q.; Song, X.; Liu, Y.; Wang, Y. Comparison of prophylactic bolus norepinephrine and phenylephrine on hypotension during spinal anesthesia for cesarean section. Int. J. Clin. Exp. 2017, 10, 12315–12321. [Google Scholar]
- Zhou, Y.; Yu, Y.; Chu, M.; Zhang, Y.; Yu, X.; Chen, G. Comparison of Metaraminol, Phenylephrine, and Norepinephrine Infusion for Prevention of Hypotension During Combined Spinal-Epidural Anaesthesia for Elective Caesarean Section: A Three-Arm, Randomized, Double-Blind, Non-Inferiority Trial. Drug Des. Dev. Ther. 2022, 16, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Vallejo, M.C.; Attaallah, A.F.; Elzamzamy, O.M.; Cifarelli, D.T.; Phelps, A.L.; Hobbs, G.R.; Shapiro, R.; Ranganathan, P. An open-label randomized controlled clinical trial for comparison of continuous phenylephrine versus norepinephrine infusion in prevention of spinal hypotension during cesarean delivery. Int. J. Obstet. Anesth. 2017, 29, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Theodoraki, K.; Hadzilia, S.; Valsamidis, D.; Stamatakis, E. Prevention of hypotension during elective cesarean section with a fixed-rate norepinephrine infusion versus a fixed-rate phenylephrine infusion. A double-blinded randomized controlled trial. Int. J. Surg. 2020, 84, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Jain, K.; Goel, N.; Arora, A.; Kumar, P. Neonatal outcomes following prophylactic administration of phenylephrine or noradrenaline in women undergoing scheduled caesarean delivery: A randomised clinical trial. Eur. J. Anaesthesiol. 2022, 39, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.; Singh, J.; Mitra, S.; Anand, L.K.; Goel, B.; Kaur, M. Comparison of prophylactic phenylephrine and norepinephrine infusion on umbilical arterial pH and maternal blood pressure during spinal anaesthesia for caesarean delivery. Indian J. Anaesth. 2022, 66 (Suppl. 2), S115–S121. [Google Scholar] [CrossRef] [PubMed]
- Sharkey, A.M.; Siddiqui, N.; Downey, K.; Ye, X.Y.; Guevara, J.; Carvalho, J.C.A. Comparison of Intermittent Intravenous Boluses of Phenylephrine and Norepinephrine to Prevent and Treat Spinal-Induced Hypotension in Cesarean Deliveries: Randomized Controlled Trial. Anesth. Analg. 2019, 129, 1312–1318. [Google Scholar] [CrossRef] [PubMed]
- Ngan Kee, W.D.; Lee, S.W.Y.; Ng, F.F.; Lee, A. Norepinephrine or phenylephrine during spinal anaesthesia for Caesarean delivery: A randomised double-blind pragmatic non-inferiority study of neonatal outcome. Br. J. Anaesth. 2020, 125, 588–595. [Google Scholar] [CrossRef] [PubMed]
- Mohta, M.; Bambode, N.; Chilkoti, G.T.; Agarwal, R.; Malhotra, R.K.; Batra, P. Neonatal outcomes following phenylephrine or norepinephrine for treatment of spinal anaesthesia-induced hypotension at emergency caesarean section in women with fetal compromise: A randomised controlled study. Int. J. Obstet. Anesth. 2022, 49, 103247. [Google Scholar] [CrossRef] [PubMed]
- Mohta, M.; Lakshmi, R.; Chilkoti, G.T.; Agarwal, R.; Malhotra, R.K. A randomised double-blind comparison of phenylephrine and norepinephrine for the management of postspinal hypotension in pre-eclamptic patients undergoing caesarean section. Eur. J. Anaesthesiol. 2021, 38, 1077–1084. [Google Scholar] [CrossRef] [PubMed]
- Mohta, M.; Garg, A.; Chilkoti, G.T.; Malhotra, R.K. A randomised controlled trial of phenylephrine and noradrenaline boluses for treatment of postspinal hypotension during elective caesarean section. Anaesthesia 2019, 74, 850–855. [Google Scholar] [CrossRef]
- Hasanin, A.; Amin, S.; Refaat, S.; Habib, S.; Zayed, M.; Abdelwahab, Y.; Elsayad, M.; Mostafa, M.; Raafat, H.; Elshall, A.; et al. Norepinephrine versus phenylephrine infusion for prophylaxis against post-spinal anaesthesia hypotension during elective caesarean delivery: A randomised controlled trial. Anaesth. Crit. Care Pain. Med. 2019, 38, 601–607. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.; Qin, R.; Ren, X.; Han, C.; Xue, W.; He, L.; Ma, L.; Pan, H.; Ma, S.; Chen, Y.; et al. Prophylactic norepinephrine or phenylephrine infusion for bradycardia and post-spinal anaesthesia hypotension in patients with preeclampsia during Caesarean delivery: A randomised controlled trial. Br. J. Anaesth. 2022, 128, e305–e307. [Google Scholar] [CrossRef] [PubMed]
- Du, W.; Song, Y.; Li, J.; Zhou, X.; Xu, Z.; Liu, Z. Comparison of Prophylactic Norepinephrine and Phenylephrine Infusions During Spinal Anaesthesia for Primary Caesarean Delivery in Twin Pregnancies: A Randomized Double-Blinded Clinical Study. Drug Des. Dev. Ther. 2022, 16, 789–798. [Google Scholar] [CrossRef] [PubMed]
- Cho, W.J.; Cho, S.Y.; Lee, A.R. Systemic hemodynamic effects of norepinephrine versus phenylephrine in intermittent bolus doses during spinal anesthesia for cesarean delivery. Anesth. Pain. Med. 2020, 15, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Zhou, J.; Wan, L.; Huang, H. Norepinephrine versus phenylephrine infusion for preventing postspinal hypotension during cesarean section for twin pregnancy: A double-blinded randomized controlled clinical trial. BMC Anesthesiol. 2022, 22, 17. [Google Scholar] [CrossRef] [PubMed]
- Biricik, E.; Karacaer, F.; Ünal, İ.; Sucu, M.; Ünlügenç, H. The effect of epinephrine for the treatment of spinal-hypotension: Comparison with norepinephrine and phenylephrine, clinical trial. Braz. J. Anesthesiol. 2020, 70, 500–507. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Mao, M.; Zhang, S.S.; Wang, Z.H.; Xu, S.Q.; Shen, X.F. Bolus norepinephrine and phenylephrine for maternal hypotension during elective cesarean section with spinal anesthesia: A randomized, double-blinded study. Chin. Med. J. 2020, 133, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Puolakka, J.; Kauppila, A.; Tuimala, R.; Jouppila, R.; Vuori, J. The effect of parturition on umbilical blood plasma levels of norepinephrine. Obstet. Gynecol. 1983, 61, 19–21. [Google Scholar] [CrossRef] [PubMed]
- Kinsella, S.M.; Carvalho, B.; Dyer, R.A.; Fernando, R.; McDonnell, N.; Mercier, F.J.; Palanisamy, A.; Sia, A.T.H.; Van de Velde, M.; Vercueil, A.; et al. International consensus statement on the management of hypotension with vasopressors during caesarean section under spinal anaesthesia. Anaesthesia 2018, 73, 71–92. [Google Scholar] [CrossRef] [PubMed]
- Ngan Kee, W.D.; Lee, S.W.Y.; Ng, F.F.; Khaw, K.S. Prophylactic Norepinephrine Infusion for Preventing Hypotension During Spinal Anesthesia for Cesarean Delivery. Anesth. Analg. 2018, 126, 1989–1994. [Google Scholar] [CrossRef] [PubMed]
- Norepinephrine Bitartrate Injection, USP Package Insert. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/007513s038lbl.pdf (accessed on 23 November 2023).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Year, Country | Participants | Anesthesia | Mode of Administration | Intervention | Outcome |
|---|---|---|---|---|---|
| Zhou, 2022, China [14] | 50 healthy women | CSEA with hyperbaric 0.5% bupivacaine 12.5 mg | bolus + continuous infusion | Bolus of NE 4 ug vs. PE 50 ug + continuous infusion of (NE 8 μg/mL vs. PE 100 ug/mL) at a rate of 30 mL/h. | primary outcome: neonatal UA/ UV BGA, APGAR score (1, 5 min); secondary outcome: maternal SBP, HR, IONV |
| Singh, 2022, India [17] | 100 healthy women | SA with 0.5% hyperbaric bupivacaine 10 mg + fentanyl 25 μg | continuous infusion | PE 100 ug/min vs. NE 5 μg/min to maintain SBP 90–110% baseline. | primary outcome: neonatal UA/ UV BGA, APGAR score (1, 5 min); secondary outcome: maternal SBP, HR, IONV |
| Singh, 2022, India [18] | 60 healthy women | SA with 0.5% bupivacaine 11 mg | Continuous infusion of PE 50 μg/min vs. NE 2.5 μg/min. | ||
| Mohta, 2022, India [21] | 100 healthy women | SA with 0.5% hyperbaric bupivacaine 10–11 mg | intermittent bolus | Bolus of PE 100 μg or NE 8 μg when SBP <100 mmHg. | primary outcome: neonatal UA/UV BGA, APGAR score; secondary outcome: rescues of vasopressor, episodes of hypotension, incidence of bradycardia/tachycardia/arrhythmias, IONV |
| Guo, 2022, China [25] | 138 pre-eclampsia women | SA with 0.5% hyperbaric bupivacaine 12.5 mg | continuous infusion | Continuous infusions of PE 0.625 μg /kg/min vs. NE 0.05 μg/kg/min. | primary outcome: incidence of bradycardia; secondary outcome: incidence of hypotension, hypertension, IONV, stability of HR, sbp, UA BGA, APGAR score |
| Du, 2022, China [26] | 62 twin pregnancies | SA with 0.5% isobaric ropivacaine 12 mg + sufentanil 5 μg | continuous infusion | Continuous infusion of NE 6 μg/min vs. phenylepinephrine 75 μg/min. | primary outcome: maternal episodes of hypotension, bradycardia, reactive hypertension, N/V; secondary outcome: neonatal APGAR (1, 5 min), UV BGA |
| Chen, 2022, China [28] | 100 healthy women | SA with of 0.5% isobaric bupivacaine 12.5 mg | continuous infusion | Continuous infusion of NE 3.2 μg/min or PE infusion 40 μg/min. Bolus of NE 8 μg vs. PE 100 μg for parturients with PE when SBP < 90 mmHg or 80% baseline. | primary outcome: maternal SBP, HR; secondary outcome: neonatal APGAR score, UA UV BGA. |
| Mohta, 2021, India [22] | 86 pre-eclampsia, singleton | SA with hyperbaric 0.5% bupivacaine 11 mg | intermittent bolus | Bolus of PE 50 μg or NE 4 μg when SBP <100 mmHg, SBP fall 20% from the baseline. | primary outcome: umbilical artery pH; secondary outcomes: APGAR scores (1 and 5 min), the number of hypotensive episodes, vasopressor boluses, tachycardia, bradycardia, arrhythmias or hypertension and maternal complications. |
| Wang, 2020, China [30] | 102 healthy women | SA with 0.5% ropivacaine 15 mg | intermittent bolus | Bolus of NE 8 µg vs. PE 100 µg when SBP <80%. | primary outcome: maternal SBP, HR, CO, SV, TPR; secondary outcomes: neonatal APGAR, UA/UV BGA |
| Theodoraki, 2020, Greece [16] | 82 healthy women | CSEA with 0.75% ropivacaine 13.5 mg + fentanyl 10 μg. | continuous infusion | Continuous infusion rate of PE 50 μg/min vs. NE 4 μg/min. | primary outcome: maternal bradycardia episodes, incidences of hypotension, hypertension; secondary outcome: neonatal UV BGA, APGAR score < 7 |
| Ngan Kee, 2020, China [20] | 668 women elective/non-elective CS under spinal or CSE anesthesia | SA or CSEA with hyperbaric bupivacaine 0.5% + fentanyl with no restriction on dose. | intravenous infusion or intermittent boluses, or both according to individual preference. | NE 6 μg/mL or PE 100 μg/mL either prophylactically or therapeutically, as an infusion or bolus. | primary outcome: neonatal APGAR score < 7, UA/UV BGA |
| Cho, 2020, South Korea [27] | 44 healthy women | SA with hyperbaric bupivacaine 8 mg with fentanyl 15 μg | intermittent bolus | Bolus of study drug whenever hypotension occurred. Hypotension was defined as < 80% baseline SBP or < 90 mmHg. | primary outcome: maternal outcome (SBP, HR, CO, SV, SVR); secondary outcome: neonatal outcomes (APGAR scores 1, 5 min; UA BGA) |
| Biricik, 2020, Turkey [29] | 80/160 healthy women | SA with hyperbaric bupivacaine 10 mg + fentanyl 20 μg | continuous infusion | 5 μg/mL NE, 100 μg/mL infused at a 30 mL/h. | primary outcome: APGAR, UA pH (IQR); secondary outcome: maternal hypotension incidence, number of patients receiving ephedrine rescue, mean ephedrine consumption |
| Sharkey, 2019, Canada [19] | 112 healthy women | SA with 0.75% hyperbaric bupivacaine 13.5 mg + fentanyl 10 μg + morphine 100 μg | intermittent bolus | Bolus of 100 μg/mL PE vs. 6 μg/mL NE if SBP lower baseline 80% + HR <60 bpm or if SBP < 80% of baseline. | primary outcome: maternal bradycardia (HR <50 bpm); secondary outcomes: incidences of maternal bradycardia; hypotension, hypertension, tachycardia, IONV; block level; UC and UV BGs; APGAR scores |
| Mohta, 2019, India [23] | 90 healthy women | SA with hyperbaric 0.5% bupivacaine 10–11 mg, | intermittent bolus | Bolus of PE 100 μg/mL vs. NE 5 μg/mL when SBP < 100 mmHg or below 20% of baseline. | primary outcome measure: maternal bradycardia; secondary outcome measures included changes in maternal systolic arterial pressure after vasopressor administration; number of episodes of hypotension and reactive hypertension; number of vasopressor doses used to treat first hypotensive episode and the total number required until delivery of baby; incidence of maternal complications, for example, nausea, vomiting, dizziness; APGAR scores at 1 min and 5 min; umbilical artery pH; and incidence of fetal acidosis, defined as umbilical artery pH < 7.20. |
| Hasanin, 2019, Egypt [24] | 123 healthy women | SA with hyperbaric bupivacaine 10 mg + fentanyl 20 μg | continuous infusion | NE infusion rate 0.05 μg/kg/min diluted 4 μg/mL; PE infusion ratem0.75 μg/kg/min diluted 50 μg/mL. | primary outcome: maternal hemodynamic parameter; secondary outcome: neonatal UA blood gas, APGAR |
| Vallejo, 2017, USA [15] | 81 healthy women | SA with hyperbaric bupivacaine 12–15 mg + morphine 0.2 mg + fentanyl 20 μg | continuous infusion | Continuous infusion of PE 0.1 μg/kg/min vs. NE 0.05 μg/kg/min for SBP within 100–120% of baseline. | maternal outcome: SBP, DBP, HR, CO, CI, SV, SVR, vasopressor rescues; neonatal outcome: APGAR score, UV BGA |
| Ngan Kee, 2015, China [4] | 101 healthy women | SA with 0.5% hyperbaric bupivacaine 11 mg + fentanyl 15 μg | continuous infusion | Computer-controlled infusion of NE 5 μg/mL vs. PE 100 μg/mL. | primary outcome: maternal SBP, HR, SVR, SV, CO; secondary outcome: neonatal APGAR, UA/UV BGA |
| Dong, 2017, China [13] | 126 healthy women | SA with 0.5% ropivacaine 15 mg | intermittent bolus | Bolus of NE 10 μg (10 μg/mL) vs. PE 50 μg (50 μg/mL). | primary outcome: neonatal APGAR, UA/UV blood gas; secondary outcome: incidence of maternal hypertension, bradycardia, no. of vasopressor rescues |
| Wang, 2019, China [11] | 111/166 pre-eclampsia parturients | SA with 0.5% bupivacaine 10–11 mg | intermittent bolus | Bolus of NE 4 μg vs. PE 50 μg. | primary outcome: maternal SBP, HR; secondary outcome: incidence of tachycardia, bradycardia, hypertension, no. of vasopressor rescues, APGAR, UA blood gas, pH |
| Eskandr, 2021, Egypt [12] | 50/75 healthy women | SA with 0.5% hyperbaric bupivacaine 9–13 mg + fentanyl 25 μg | intermittent bolus | Bolus of PE 0.2 μg/kg vs. NE 0.1 μg/kg. | APGAR, umbilical blood pH, acidosis |
| pH | BE | |||
|---|---|---|---|---|
| p-Value | p-Value | |||
| UA or UV | 0.3921 | UApH −0.0006 (−0.0072 to 0.0061) | ||
| UVpH 0.0042 (−0.0044 to 0.0127) | ||||
| Infusion method | 0.9291 | Infusion 0.0016 (−0.0066; 0.0098) | 0.3293 | Infusion 0.3444 [−0.2158; 0.9045] |
| bolus −0.0004 (−0.0102; 0.0094) | Bolus −0.2956 [−0.9356; 0.3443] | |||
| Infusion or bolus 0.0030 [−0.0145; 0.0205] | Infusion or bolus 0.2000 [−0.9450; 1.3450] | |||
| Single or twin | 0.7037 | Single 0.0016 [−0.0045; 0.0077] | 0.3105 | Single 0.1887 [−0.1965; 0.5739] |
| Twin −0.0013 [−0.0153; 0.0126] | Twin −0.2570 [−1.0273; 0.5134] | |||
| Number of parturients | 0.700 | Number of patients 0.000 (−0.000 to 0.000) | 0.881 | Number of patients 0.000 (−0.002 to 0.002) |
| Outcomes | Number of Studies | Quality Assessment | Heterogeneity | MD (95% CI) | Quality | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| ROB | Inconsistency | Indirectness | Imprecision | Publication Bias | Tau(τ)2 | I2 | ||||
| pH overall | 24 | not serious | serious | not serious | not serious | not serious | 0.0001 | I2 = 58% | −0.001 (−0.004 to 0.007) | ⨁⨁⨁○ Moderate |
| pH UA | 17 | not serious | not serious | not serious | not serious | not serious | < 0.0001 | 27% | 0.000 (−0.004 to 0.004) | ⨁⨁⨁⨁ High |
| pH UV | 13 | not serious | serious | not serious | not serious | not serious | 0.0005 | 71% | 0.002 (−0.013 to 0.017) | ⨁⨁⨁○ Moderate |
| BE overall | 17 | not serious | serious | not serious | not serious | not serious | 0.4736 | 62% | 0.096 (−0.258 to 0.451) | ⨁⨁⨁○ Moderate |
| pH BE | 41 | not serious | not serious | not serious | not serious | not serious | 0.0001 | 37% | 0.076 (−0.141 to 0.294) | ⨁⨁⨁⨁ High |
| pH U BE | not serious | serious | not serious | not serious | not serious | 1.1557 | 74% | 0.121 (−0.569 to 0.811) | ⨁⨁⨁○ Moderate | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, H.; Sung, T.-Y.; Jee, Y.S.; Kwon, W.; Cho, S.-A.; Ahn, S.; Cho, C.-K. A Comparison of Norepinephrine versus Phenylephrine to Prevent Hypotension after Spinal Anesthesia for Cesarean Section: Systematic Review and Meta-Analysis. J. Pers. Med. 2024, 14, 803. https://doi.org/10.3390/jpm14080803
Kang H, Sung T-Y, Jee YS, Kwon W, Cho S-A, Ahn S, Cho C-K. A Comparison of Norepinephrine versus Phenylephrine to Prevent Hypotension after Spinal Anesthesia for Cesarean Section: Systematic Review and Meta-Analysis. Journal of Personalized Medicine. 2024; 14(8):803. https://doi.org/10.3390/jpm14080803
Chicago/Turabian StyleKang, Hyun, Tae-Yun Sung, Young Seok Jee, Woojin Kwon, Sung-Ae Cho, Somin Ahn, and Choon-Kyu Cho. 2024. "A Comparison of Norepinephrine versus Phenylephrine to Prevent Hypotension after Spinal Anesthesia for Cesarean Section: Systematic Review and Meta-Analysis" Journal of Personalized Medicine 14, no. 8: 803. https://doi.org/10.3390/jpm14080803