
Evaluating the Utility of Clinical Scores APACHE, CURB, SOFA, and NEWS2 at Admission and 5-Days after Symptom Onset in Predicting Severe COVID-19 in Patients with Diabetes

 , , ,
, , ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection and Variables
2.4. Statistical Analysis
3. Results
4. Discussion
4.1. Analysis of Findings
4.2. Study Limitations and Future Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gavkare, A.M.; Nanaware, N.; Rayate, A.S.; Mumbre, S.; Nagoba, B.S. COVID-19 associated diabetes mellitus: A review. World J. Diabetes 2022, 13, 729–737. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dallavalasa, S.; Tulimilli, S.V.; Prakash, J.; Ramachandra, R.; Madhunapantula, S.V.; Veeranna, R.P. COVID-19: Diabetes Perspective-Pathophysiology and Management. Pathogens 2023, 12, 184. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ssentongo, P.; Zhang, Y.; Witmer, L.; Chinchilli, V.M.; Ba, D.M. Association of COVID-19 with diabetes: A systematic review and meta-analysis. Sci. Rep. 2022, 12, 20191. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Floyd, J.S.; Walker, R.L.; Kuntz, J.L.; Shortreed, S.M.; Fortmann, S.P.; Bayliss, E.A.; Harrington, L.B.; Fuller, S.; Albertson-Junkans, L.H.; Powers, J.D.; et al. Association between Diabetes Severity and Risks of COVID-19 Infection and Outcomes. J. Gen. Intern. Med. 2023, 38, 1484–1492. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Geetha, H.S.; Singh, G.; Sekar, A.; Gogtay, M.; Singh, Y.; Abraham, G.M.; Trivedi, N. Hyperglycemia in COVID-19 infection without diabetes mellitus: Association with inflammatory markers. World J. Clin. Cases 2023, 11, 1287–1298. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Khamidullina, Z.; Avzaletdinova, D.; Gareeva, D.; Morugova, T.; Lakman, I.; Kopp, K.; Fiedler, L.; Motloch, L.J.; Zagidullin, N. Long-Term Outcomes of COVID-19 in Hospitalized Type 2 Diabetes Mellitus Patients. Biomedicines 2024, 12, 467. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fernandes, S.; Sérvio, R.; Patrício, P.; Pereira, C. Validation of the Acute Physiology and Chronic Health Evaluation (APACHE) II Score in COVID-19 Patients Admitted to the Intensive Care Unit in Times of Resource Scarcity. Cureus 2023, 15, e34721. [Google Scholar] [CrossRef] [PubMed]
- Doğanay, F.; Ak, R. Performance of the CURB-65, ISARIC-4C and COVID-GRAM scores in terms of severity for COVID-19 patients. Int. J. Clin. Pract. 2021, 75, e14759. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Trongtrakul, K.; Tajarernmuang, P.; Limsukon, A.; Theerakittikul, T.; Niyatiwatchanchai, N.; Surasit, K.; Glunriangsang, P.; Liwsrisakun, C.; Bumroongkit, C.; Pothirat, C.; et al. The National Early Warning Score 2 with Age and Body Mass Index (NEWS2 Plus) to Determine Patients with Severe COVID-19 Pneumonia. J. Clin. Med. 2024, 13, 298. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Faisal, M.; Mohammed, M.A.; Richardson, D.; Steyerberg, E.W.; Fiori, M.; Beatson, K. Predictive accuracy of enhanced versions of the on-admission National Early Warning Score in estimating the risk of COVID-19 for unplanned admission to hospital: A retrospective development and validation study. BMC Health Serv. Res. 2021, 21, 957. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- City, I.; De Ridder, T.; Bruckers, L.; Geebelen, L.; Gharmaoui, S.; Callebaut, I.; Vandenbrande, J.; Berends, N.; Dubois, J.; Stessel, B. Predictive value of serial evaluation of the Sequential Organ Failure Assessment (SOFA) score for intensive care unit mortality in critically ill patients with COVID-19: A retrospective cohort study. Anaesthesiol. Intensive Ther. 2022, 54, 3–11. [Google Scholar] [CrossRef]
- Citu, C.; Citu, I.M.; Motoc, A.; Forga, M.; Gorun, O.M.; Gorun, F. Predictive Value of SOFA and qSOFA for In-Hospital Mortality in COVID-19 Patients: A Single-Center Study in Romania. J. Pers. Med. 2022, 12, 878. [Google Scholar] [CrossRef] [PubMed]
- Fayed, M.; Patel, N.; Angappan, S.; Nowak, K.; Vasconcelos Torres, F.; Penning, D.H.; Chhina, A.K. Sequential Organ Failure Assessment (SOFA) Score and Mortality Prediction in Patients with Severe Respiratory Distress Secondary to COVID-19. Cureus 2022, 14, e26911. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sciberras, J.; Camilleri, L.M.; Cuschieri, S. The burden of type 2 diabetes pre-and during the COVID-19 pandemic—A review. J. Diabetes Metab. Disord. 2020, 19, 1357–1365. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sen, S.; Chakraborty, R.; Kalita, P.; Pathak, M.P. Diabetes mellitus and COVID-19: Understanding the association in light of current evidence. World J. Clin. Cases 2021, 9, 8327–8339. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hossain, M.J.; Al-Mamun, M.; Islam, M.R. Diabetes mellitus, the fastest growing global public health concern: Early detection should be focused. Health Sci. Rep. 2024, 7, e2004. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Li, R.; Shen, M.; Yang, Q.; Fairley, C.K.; Chai, Z.; McIntyre, R.; Ong, J.J.; Liu, H.; Lu, P.; Hu, W.; et al. Global Diabetes Prevalence in COVID-19 Patients and Contribution to COVID-19-Related Severity and Mortality: A Systematic Review and Meta-analysis. Diabetes Care 2023, 46, 890–897. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Trofin, F.; Nastase, E.V.; Roșu, M.F.; Bădescu, A.C.; Buzilă, E.R.; Miftode, E.G.; Manciuc, D.C.; Dorneanu, O.S. Inflammatory Response in COVID-19 Depending on the Severity of the Disease and the Vaccination Status. Int. J. Mol. Sci. 2023, 24, 8550. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Haroun, R.A.; Osman, W.H.; Amin, R.E.; Eessa, A.M.; Saad, S. Increased serum interleukin-6 and lactate dehydrogenase levels among nonsurvival severe COVID-19 patients when compared to survival ones. Int. Immunopharmacol. 2023, 122, 110626. [Google Scholar] [CrossRef] [PubMed]
- Núñez-Cortés, R.; Malhue-Vidal, C.; Gath, F.; Valdivia-Lobos, G.; Torres-Castro, R.; Cruz-Montecinos, C.; Martinez-Arnau, F.M.; Pérez-Alenda, S.; López-Bueno, R.; Calatayud, J. The Impact of Charlson Comorbidity Index on the Functional Capacity of COVID-19 Survivors: A Prospective Cohort Study with One-Year Follow-Up. Int. J. Environ. Res. Public Health 2022, 19, 7473. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mehryar, H.R.; Yarahmadi, P.; Anzali, B.C. Mortality predictive value of APACHE II Scores in COVID-19 patients in the intensive care unit: A cross-sectional study. Ann. Med. Surg. 2023, 85, 2464–2468. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Plummer, M.P.; Rait, L.; Finnis, M.E.; French, C.J.; Bates, S.; Douglas, J.; Bhurani, M.; Broadley, T.; Trapani, T.; Deane, A.M.; et al. Diabetes mellitus, glycaemic control, and severe COVID-19 in the Australian critical care setting: A nested cohort study. Aust. Crit. Care 2023, 36, 579–585. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Asmarawati, T.P.; Suryantoro, S.D.; Rosyid, A.N.; Marfiani, E.; Windradi, C.; Mahdi, B.A.; Sutanto, H. Predictive Value of Sequential Organ Failure Assessment, Quick Sequential Organ Failure Assessment, Acute Physiology and Chronic Health Evaluation II, and New Early Warning Signs Scores Estimate Mortality of COVID-19 Patients Requiring Intensive Care Unit. Indian J. Crit. Care Med. 2022, 26, 464–471. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Beigmohammadi, M.T.; Amoozadeh, L.; Rezaei Motlagh, F.; Rahimi, M.; Maghsoudloo, M.; Jafarnejad, B.; Eslami, B.; Salehi, M.R.; Zendehdel, K. Mortality Predictive Value of APACHE II and SOFA Scores in COVID-19 Patients in the Intensive Care Unit. Can. Respir. J. 2022, 2022, 5129314. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Esmaeili Tarki, F.; Afaghi, S.; Rahimi, F.S.; Kiani, A.; Varahram, M.; Abedini, A. Serial SOFA-score trends in ICU-admitted COVID-19 patients as predictor of 28-day mortality: A prospective cohort study. Health Sci. Rep. 2023, 6, e1116. [Google Scholar] [CrossRef]
- Yang, Z.; Hu, Q.; Huang, F.; Xiong, S.; Sun, Y. The prognostic value of the SOFA score in patients with COVID-19: A retrospective, observational study. Medicine 2021, 100, e26900. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Belikina, D.V.; Malysheva, E.S.; Petrov, A.V.; Nekrasova, T.A.; Nekaeva, E.S.; Lavrova, A.E.; Zarubina, D.G.; Atduev, K.A.; Magomedova, D.M.; Strongin, L.G. COVID-19 in Patients with Diabetes: Clinical Course, Metabolic Status, Inflammation, and Coagulation Disorder. Sovrem. Tekhnologii Med. 2021, 12, 6–16. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Guo, J.; Zhou, B.; Zhu, M.; Yuan, Y.; Wang, Q.; Zhou, H.; Wang, X.; Lv, T.; Li, S.; Liu, P.; et al. CURB-65 may serve as a useful prognostic marker in COVID-19 patients within Wuhan, China: A retrospective cohort study. Epidemiol. Infect. 2020, 148, e241. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Eldaboosy, S.; Almoosa, Z.; Saad, M.; Al Abdullah, M.; Farouk, A.; Awad, A.; Mahdy, W.; Abdelsalam, E.; Nour, S.O.; Makled, S.; et al. Comparison Between Physiological Scores SIPF, CURB-65, and APACHE II as Predictors of Prognosis and Mortality in Hospitalized Patients with COVID-19 Pneumonia: A Multicenter Study, Saudi Arabia. Infect. Drug Resist. 2022, 15, 7619–7630. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nikniaz, Z.; Somi, M.H.; Dinevari, M.F.; Taghizadieh, A.; Mokhtari, L. Diabesity Associates with Poor COVID-19 Outcomes among Hospitalized Patients. J. Obes. Metab. Syndr. 2021, 30, 149–154. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

{kind=link}
| Variables | With Diabetes (n = 141) | Without Diabetes (n = 316) | p-Value |
|---|---|---|---|
| Age, years (mean ± SD) | 58.7 ± 13.4 | 56.2 ± 14.1 | 0.076 |
| Gender, men | 82 (58.16%) | 153 (48.42%) | 0.068 |
| BMI (mean ± SD) | 29.7 ± 4.7 | 27.4 ± 5.3 | <0.001 |
| Smoking | 28 (19.86%) | 63 (19.94%) | 0.986 |
| Alcohol use | 13 (9.22%) | 36 (11.39%) | 0.596 |
| Diabetes type | - | - | - |
| T1DM | 22 (15.61%) | - | - |
| T2DM | 119 (84.39%) | - | - |
| Duration of diabetes, years (mean ± SD) | 8.1 ± 6.6 | - | - |
| HbA1C (mean ± SD) | 8.4 ± 2.9 | - | - |
| COVID-19 vaccinated | 77 (54.61%) | 159 (50.32%) | 0.455 |
| CCI > 2 | 68 (48.23%) | 97 (30.70%) | <0.001 |
| COVID-19 severity | - | - | 0.109 |
| Mild | 63 (44.68%) | 167 (52.85%) | - |
| Moderate | 51 (36.17%) | 84 (26.58%) | - |
| Severe | 27 (19.15%) | 65 (20.57%) | - |
| ICU admissions | 19 (13.48%) | 16 (5.06%) | 0.003 |
| Supplemental oxygen | 39 (27.66%) | 42 (13.29%) | <0.001 |
| Mechanical ventilation | 11 (7.80%) | 7 (2.22%) | 0.010 |
| Mortality | 7 (4.96%) | 5 (1.58%) | 0.076 |
| Variables (Mean ± SD) | With Diabetes (n = 141) | Without Diabetes (n = 316) | p-Value |
|---|---|---|---|
| Oxygen saturation | 92.34 ± 3.21 | 94.56 ± 2.62 | <0.001 |
| WBC (×109/L) | 9.38 ± 2.82 | 7.21 ± 3.14 | <0.001 |
| Temperature | 38.32 ± 0.72 | 37.98 ± 0.52 | <0.001 |
| Heart rate | 88.42 ± 11.24 | 81.37 ± 13.19 | <0.001 |
| Glasgow coma scale | 14.22 ± 1.63 | 14.95 ± 0.42 | <0.001 |
| Bilirubin levels | 1.34 ± 0.56 | 0.92 ± 0.31 | <0.001 |
| Creatinine (mg/dL) | 1.64 ± 0.61 | 0.95 ± 0.42 | <0.001 |
| PaO2/FiO2 ratio | 285.43 ± 65.23 | 320.47 ± 50.35 | <0.001 |
| Platelets | 220.39 ± 50.67 | 250.28 ± 70.43 | <0.001 |
| Respiratory rate | 22.15 ± 3.97 | 19.06 ± 3.09 | <0.001 |
| Systolic blood pressure | 130.87 ± 15.32 | 125.48 ± 19.76 | 0.004 |
| BUN | 29.42 ± 10.38 | 18.65 ± 8.24 | <0.001 |
| Clinical scores | |||
| APACHE II | 18.47 ± 6.32 | 15.13 ± 4.98 | <0.001 |
| CURB-65 | 2.14 ± 0.83 | 1.56 ± 0.69 | <0.001 |
| SOFA | 4.03 ± 2.09 | 2.04 ± 1.22 | <0.001 |
| NEWS2 | 5.27 ± 1.98 | 3.29 ± 1.13 | <0.001 |
| Variables (Mean ± SD) | With Diabetes (n = 141) | Without Diabetes (n = 316) | p-Value |
|---|---|---|---|
| Oxygen saturation | 90.78 ± 4.32 | 93.64 ± 3.58 | <0.001 |
| WBC (×109/L) | 11.22 ± 3.76 | 8.34 ± 2.99 | <0.001 |
| Temperature | 37.96 ± 0.82 | 37.12 ± 0.61 | <0.001 |
| Heart rate | 92.38 ± 12.78 | 84.56 ± 11.29 | <0.001 |
| Glasgow coma scale | 13.87 ± 1.94 | 14.89 ± 0.83 | <0.001 |
| Bilirubin levels | 1.52 ± 0.67 | 0.89 ± 0.36 | <0.001 |
| Creatinine (mg/dL) | 1.82 ± 0.73 | 0.98 ± 0.47 | <0.001 |
| PaO2/FiO2 ratio | 268.94 ± 73.48 | 315.72 ± 51.23 | <0.001 |
| Platelets | 205.14 ± 55.23 | 244.38 ± 69.47 | <0.001 |
| Respiratory rate | 24.21 ± 5.18 | 20.84 ± 4.21 | <0.001 |
| Systolic blood pressure | 128.65 ± 16.42 | 122.94 ± 18.34 | 0.002 |
| BUN | 31.78 ± 11.25 | 20.39 ± 9.28 | <0.001 |
| Clinical scores | |||
| APACHE II | 19.52 ± 7.23 | 16.49 ± 6.17 | <0.001 |
| CURB-65 | 2.38 ± 0.92 | 1.62 ± 0.76 | <0.001 |
| SOFA | 4.56 ± 2.31 | 2.38 ± 1.32 | <0.001 |
| NEWS2 | 5.92 ± 2.16 | 3.84 ± 1.47 | <0.001 |
| Parameters | Time Frame | Best Cutoff Value | Sensitivity | Specificity | AUC | p-Value |
|---|---|---|---|---|---|---|
| APACHE II | At admission | 17.34 | 87.21% | 84.62% | 0.698 | <0.001 |
| CURB-65 | At admission | 2.18 | 81.14% | 79.48% | 0.883 | <0.001 |
| SOFA | At admission | 3.43 | 89.67% | 90.43% | 0.771 | <0.001 |
| NEWS2 | At admission | 4.22 | 82.67% | 80.29% | 0.892 | <0.001 |
| APACHE II | At 5 days | 19.26 | 90.31% | 91.57% | 0.806 | <0.001 |
| CURB-65 | At 5 days | 2.44 | 84.19% | 83.24% | 0.780 | <0.001 |
| SOFA | At 5 days | 3.72 | 92.47% | 93.12% | 0.873 | <0.001 |
| NEWS2 | At 5 days | 5.16 | 85.83% | 86.37% | 0.729 | <0.001 |
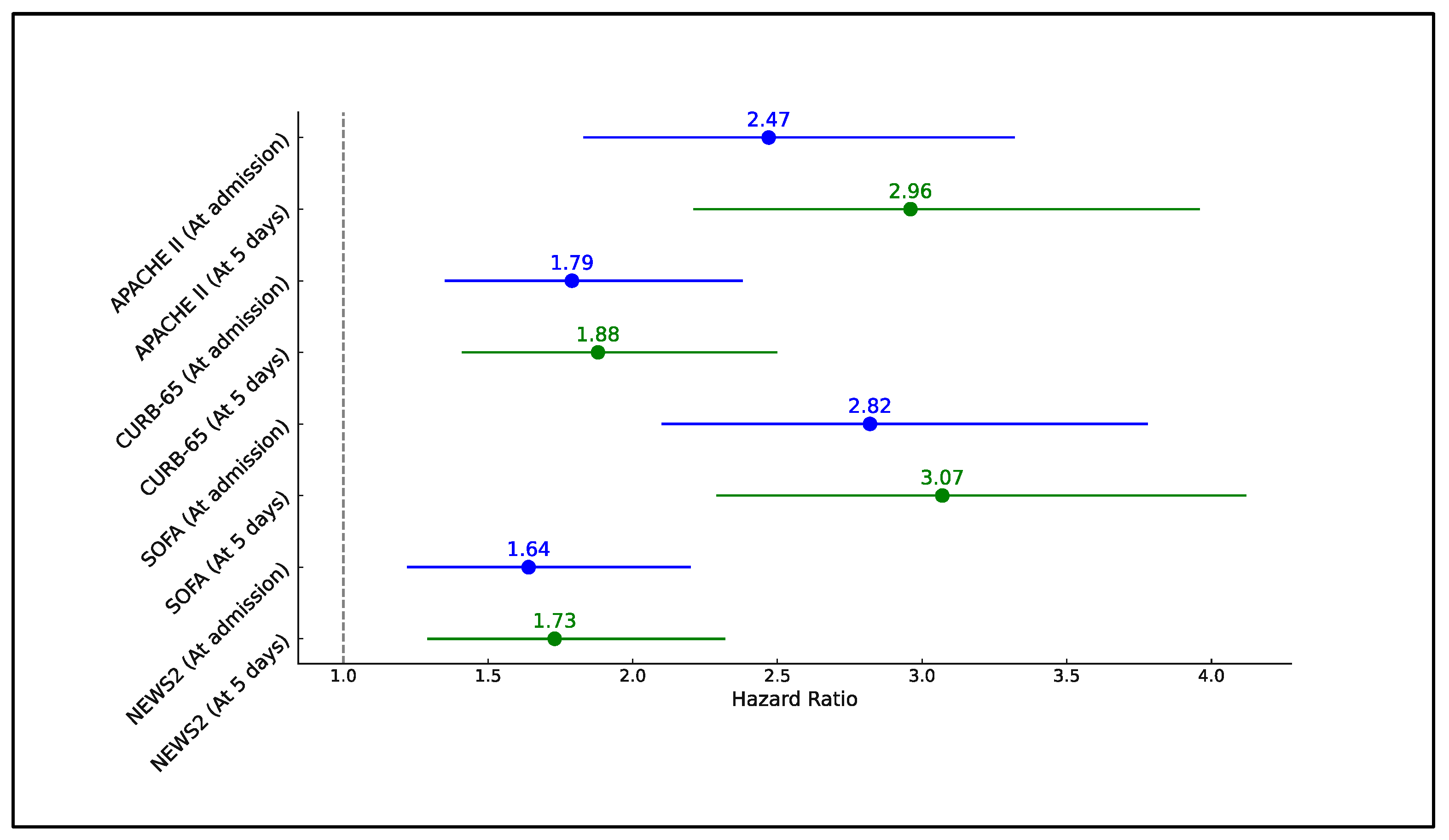
| Factors above the Best Cutoff | Time Frame | Hazard Ratio | 95% CI | p-Value |
|---|---|---|---|---|
| APACHE II | At admission | 2.47 | 1.83–3.32 | <0.001 |
| CURB-65 | At admission | 1.79 | 1.35–2.38 | <0.001 |
| SOFA | At admission | 2.82 | 2.10–3.78 | <0.001 |
| NEWS2 | At admission | 1.64 | 1.22–2.20 | <0.001 |
| APACHE II | At 5 days | 2.96 | 2.21–3.96 | <0.001 |
| CURB-65 | At 5 days | 1.88 | 1.41–2.50 | <0.001 |
| SOFA | At 5 days | 3.07 | 2.29–4.12 | <0.001 |
| NEWS2 | At 5 days | 1.73 | 1.29–2.32 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ion, R.; Kimidi, J.S.S.K.; Kalapala, C.; FNU, O.; Chandrababu, V.R.; Desireddygari, O.R.; Grigras, M.L.; Rosca, O.; Bratosin, F.; Cioca, F.; et al. Evaluating the Utility of Clinical Scores APACHE, CURB, SOFA, and NEWS2 at Admission and 5-Days after Symptom Onset in Predicting Severe COVID-19 in Patients with Diabetes. J. Pers. Med. 2024, 14, 868. https://doi.org/10.3390/jpm14080868
Ion R, Kimidi JSSK, Kalapala C, FNU O, Chandrababu VR, Desireddygari OR, Grigras ML, Rosca O, Bratosin F, Cioca F, et al. Evaluating the Utility of Clinical Scores APACHE, CURB, SOFA, and NEWS2 at Admission and 5-Days after Symptom Onset in Predicting Severe COVID-19 in Patients with Diabetes. Journal of Personalized Medicine. 2024; 14(8):868. https://doi.org/10.3390/jpm14080868
Chicago/Turabian StyleIon, Radu, Jaya Shankar Sai Kumar Kimidi, Chaitanya Kalapala, Oktrian FNU, Varshika Ramakrishnan Chandrababu, Omprakash Reddy Desireddygari, Mirela Loredana Grigras, Ovidiu Rosca, Felix Bratosin, Flavius Cioca, and et al. 2024. "Evaluating the Utility of Clinical Scores APACHE, CURB, SOFA, and NEWS2 at Admission and 5-Days after Symptom Onset in Predicting Severe COVID-19 in Patients with Diabetes" Journal of Personalized Medicine 14, no. 8: 868. https://doi.org/10.3390/jpm14080868
APA StyleIon, R., Kimidi, J. S. S. K., Kalapala, C., FNU, O., Chandrababu, V. R., Desireddygari, O. R., Grigras, M. L., Rosca, O., Bratosin, F., Cioca, F., Timar, R., & Negrean, R. A. (2024). Evaluating the Utility of Clinical Scores APACHE, CURB, SOFA, and NEWS2 at Admission and 5-Days after Symptom Onset in Predicting Severe COVID-19 in Patients with Diabetes. Journal of Personalized Medicine, 14(8), 868. https://doi.org/10.3390/jpm14080868