
Managing Fear and Anxiety in Patients Undergoing Dental Hygiene Visits with Guided Biofilm Therapy: Analysis of Psychological and Physiological Differences Between Women and Men—A Conceptual and Multivariate Regression Model

Abstract
1. Introduction
1.1. Background and Significance of the Problem
1.2. Research Objective
2. Materials and Methods
2.1. Study Sample
2.2. Research Procedure
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Study Group
3.2. Psychological Reactions
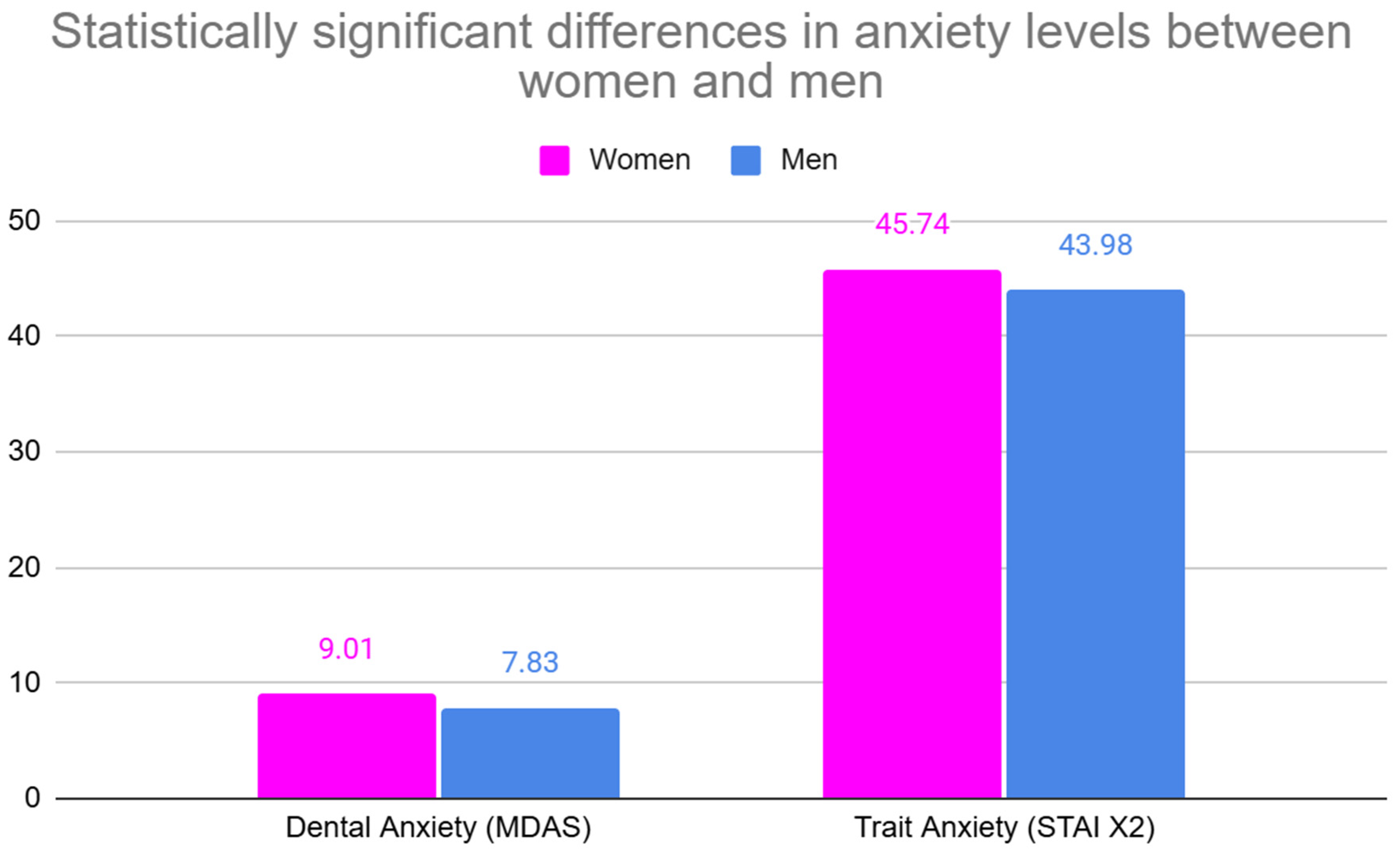
3.2.1. Dental Anxiety (MDAS)
3.2.2. Trait Anxiety (STAI X2)
3.2.3. Variables Without Statistically Significant Differences
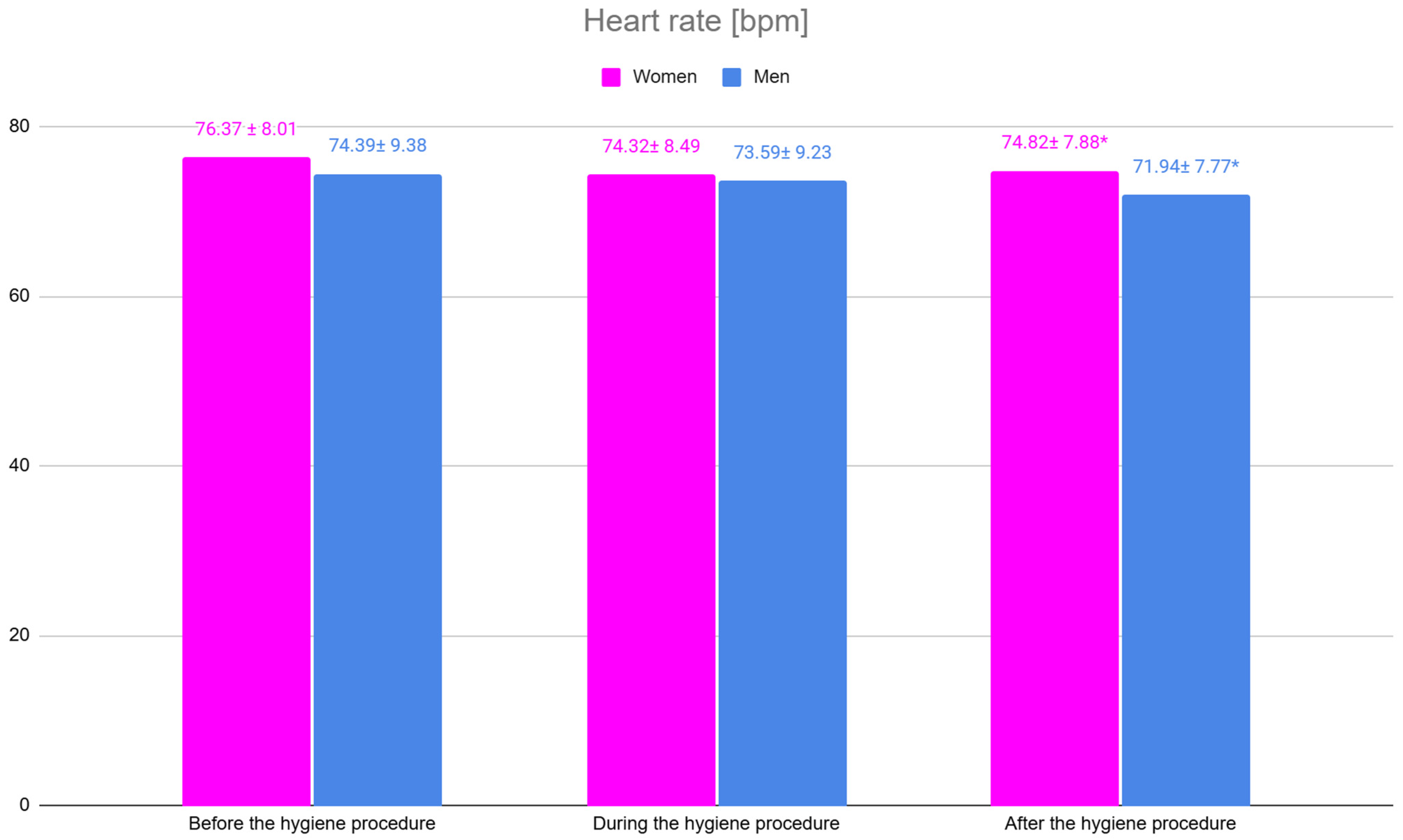
3.3. Physiological Responses–Heart Rate
3.4. Factors Related to Hygiene Visits That, in the Patient’s Opinion, Could Reduce the Experience of Negative Emotions (Fear, Anxiety)
3.5. Health Differences Between Women and Men
3.6. Regression Analysis for Trait Anxiety (STAI X2)
3.7. Regression Analysis for Dental Anxiety (MDAS)
4. Discussion
4.1. Differences in Psychological Reactions Between Women and Men Undergoing Hygiene Visits
The Impact of the COVID-19 Pandemic on Dental Anxiety
4.2. Differences in Physiological Reactions Between Women and Men Undergoing Hygiene Visits
4.3. Differences in the Assessment of Factors That Could Reduce the Experience of Negative Emotions in Women and Men
4.4. Health-Related Factors That May Modify the Experience of Negative Emotions in Women and Men
4.5. The Value of Multivariate Models for Dental Practice
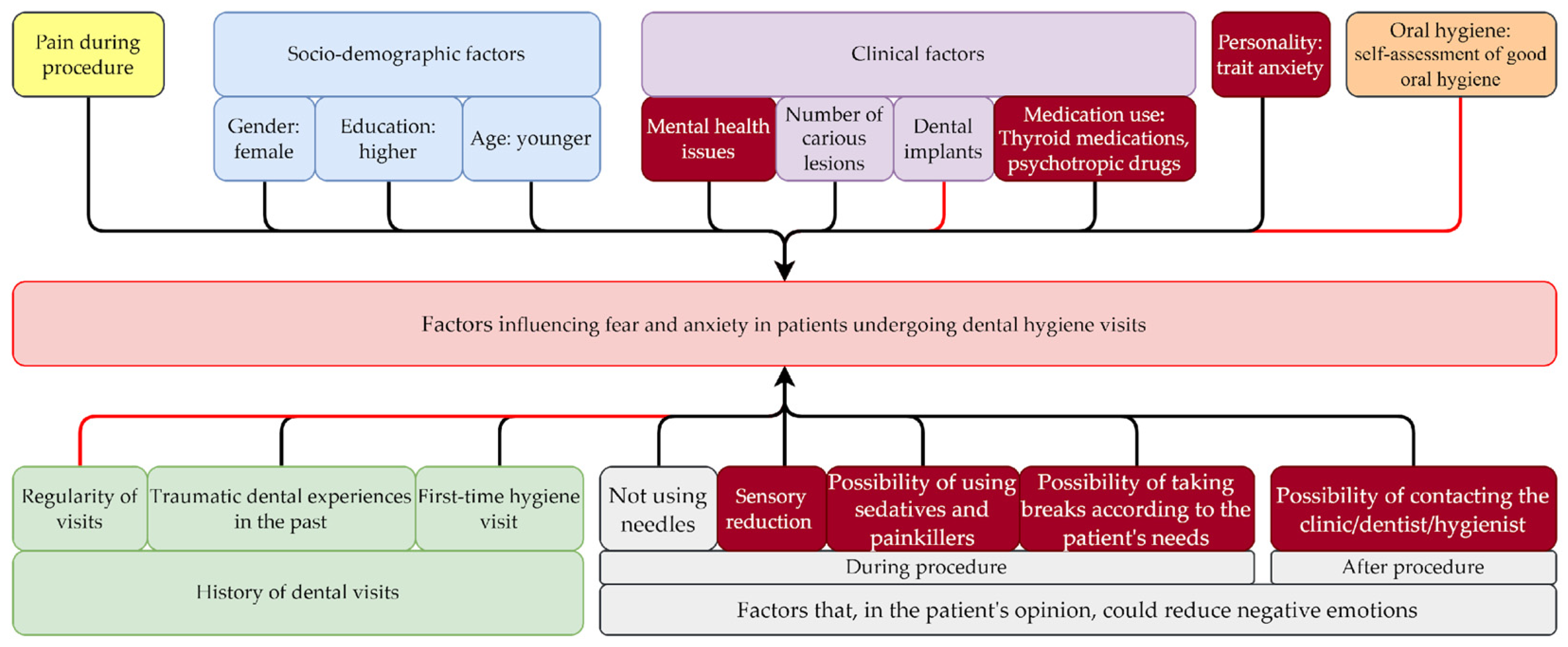
4.6. Conceptual Model and Multivariate Regression Model for Managing Fear and Anxiety in Patients Undergoing Dental Hygiene Visits, Considering Gender Differences
4.7. Limitations of the Conducted Study
4.8. Recommendations for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Economou, G.C. Dental anxiety and personality: Investigating the relationship between dental anxiety and self-consciousness. J. Dent. Educ. 2003, 67, 970–980. [Google Scholar] [PubMed]
- McGrath, C.; Bedi, R. The association between dental anxiety and oral health-related quality of life in Britain. Community Dent. Oral Epidemiol. 2004, 32, 67–72. [Google Scholar] [PubMed]
- Nicolas, E.; Collado, V.; Faulks, D.; Bullier, B.; Hennequin, M. A national cross-sectional survey of dental anxiety in the French adult population. BMC Oral Health 2007, 7, 12. [Google Scholar]
- Enkling, N.; Marwinski, G.; Johren, P. Dental anxiety in a representative sample of residents of a large German city. Clin. Oral Investig. 2006, 10, 84–91. [Google Scholar] [PubMed]
- Górska, R.; Konopka, T. Periodontologia Współczesna. I; Med Tour Press International: Warszawa, Poland, 2013. [Google Scholar]
- Vassend, O.; Czajkowski, N.O.; Røysamb, E.; Nielsen, C.S. The role of neuroticism and pain in dental anxiety: A twin study. Community Dent. Oral Epidemiol. 2023, 51, 786–793. [Google Scholar]
- Shrivastava, D.; Natoli, V.; Srivastava, K.C.; Alzoubi, I.A.; Nagy, A.I.; Hamza, M.O.; Al-Johani, K.; Alam, M.K.; Khurshid, Z. Novel approach to dental biofilm management through guided biofilm therapy (Gbt): A review. Microorganisms 2021, 9, 1966. [Google Scholar] [CrossRef] [PubMed]
- Furrer, C.; Bättig, R.; Votta, I.; Bastendorf, K.D.; Schmidlin, P.R. Patientenakzeptanz nach Umstellung auf «Guided Biofilm Therapy». SWISS Dent. J. SSO–Sci. Clin. Top. 2021, 131, 229–234. [Google Scholar] [CrossRef]
- Yokota, K.; Yu, S.W.; Tan, T.; Anderson, J.; Stormon, N. The extent and nature of dental anxiety in Australians experiencing homelessness. Health Soc. Care Community 2020, 28, 2352–2361. [Google Scholar]
- Ogawa, M.; Saito, A.; Karukivi, M.; Lahti, S. Associations of sensory sensitivity, pain catastrophizing, and alexithymia with dental anxiety. Eur. J. Oral Sci. 2024, 132, e12973. [Google Scholar]
- Goh, E.Z.; Beech, N.; Johnson, N.R. Dental anxiety in adult patients treated by dental students: A systematic review. J. Dent. Educ. 2020, 84, 805–811. [Google Scholar]
- Dadalti, M.T.; Cunha, A.J.; Souza, T.G.; Silva, B.A.; Luiz, R.R.; Risso, P.A. Anxiety about dental treatment a gender issue. Acta Odontológica Latinoam. 2021, 34, 195–200. [Google Scholar]
- Luna, M.J.; Ameli, R.; Sinaii, N.; Cheringal, J.; Panahi, S.; Berger, A. Gender differences in psycho-social-spiritual healing. J. Womens Health 2019, 28, 1513–1521. [Google Scholar] [CrossRef]
- Leśna, M.; Górna, K.; Kwiatek, J. Managing Fear and Anxiety in Patients Undergoing Dental Hygiene Visits with Guided Biofilm Therapy: A Conceptual Model. Appl. Sci. 2024, 14, 8159. [Google Scholar] [CrossRef]
- Falk, R.F. A Primer for Soft Modeling; Ohio Univ AkronPress: Akron, OH, USA, 1992. [Google Scholar]
- Muglali, M.; Komerik, N. Factors related to patients’ anxiety before and after oral surgery. J. Oral Maxillofac. Surg. 2008, 66, 870–877. [Google Scholar] [CrossRef]
- Guentsch, A.; Stier, C.; Raschke, G.F.; Peisker, A.; Fahmy, M.D.; Kuepper, H.; Schueler, I. Oral health and dental anxiety in a German practice-based sample. Clin. Oral Investig. 2017, 21, 1675–1680. [Google Scholar] [CrossRef] [PubMed]
- Yakar, B.; Kaygusuz, T.Ö.; Pirinçci, E. Evaluation of Dental Anxiety and Fear in Patients who Admitted to the Faculty of Dentistry: Which Patients are More Risky in terms of Dental Anxiety. Ethiop. J. Health Sci. 2019, 29. [Google Scholar] [CrossRef]
- Wang, T.; Li, M.; Xu, S.; Jiang, C.; Gao, D.; Wu, T.; Lu, F.; Liu, B.; Wang, J. The factorial structure of trait anxiety and its mediating effect between mindfulness and depression. Front. Psychiatry 2018, 9, 514. [Google Scholar] [CrossRef] [PubMed]
- Razavian, H.; Sara, M.S.V.; Zare, H.; Sepahvandi, A.M. State and trait anxiety evaluation in dental patients. Int. J. Depress. Anxiety 2018, 1, 008. [Google Scholar]
- Schneider, C.; Zitzmann, N.U.; Zemp, E. Changes in dental care behaviour between 2002 and 2012 and its association with complete dentition in men and women in Switzerland. medRxiv 2019. [Google Scholar] [CrossRef]
- Sfeatcu, R.; Balgiu, B.A.; Mihai, C.; Petre, A.; Pantea, M.; Tribus, L. Gender differences in oral health: Self-reported attitudes, values, behaviours and literacy among Romanian adults. J. Pers. Med. 2022, 12, 1603. [Google Scholar] [CrossRef]
- Lipsky, M.S.; Su, S.; Crespo, C.J.; Hung, M. Men and oral health: A review of sex and gender differences. Am. J. Men’s Health 2021, 15, 15579883211016361. [Google Scholar] [CrossRef]
- Chrisler, J.C.; McCreary, D.R. Handbook of Gender Research in Psychology; Springer: Berlin/Heidelberg, Germany, 2010; Volume 1. [Google Scholar]
- Pigott, T.A. Gender differences in the epidemiology and treatment of anxiety disorders. J. Clin. Psychiatry 1999, 60, 4–15. [Google Scholar] [PubMed]
- Goubet, K.E.; Chrysikou, E.G. Emotion regulation flexibility: Gender differences in context sensitivity and repertoire. Front. Psychol. 2019, 10, 935. [Google Scholar]
- Łazarz-Półkoszek, M.J.; Orczykowska, M.; Gala Pihut, M. Impact of the COVID-19 pandemic on patients’ anxiety levels related to dental appointments in Poland. Dent. Med. Probl. 2023, 60, 367–373. [Google Scholar] [PubMed]
- Tolin, D.F.; Foa, E.B. Sex differences in trauma and posttraumatic stress disorder: A quantitative review of 25 years of research. Psychol. Bull. 2006, 132, 959–992. [Google Scholar] [CrossRef] [PubMed]
- Broche-Pérez, Y.; Fernández-Fleites, Z.; Jiménez-Puig, E.; FernándezCastillo, E.; Rodríguez-Martin, B.C. Gender and fear of COVID-19 in a Cuban population sample. Int. J. Ment. Health Addict. 2022, 20, 83–91. [Google Scholar] [CrossRef]
- Bangasser, D.A. Sex Differences in Stress-Related Receptors:“Micro” Differences with “Macro” Implications for Mood and Anxiety Disorders. Biol. Sex Differ. 2013, 4, 2. [Google Scholar]
- Ghaffar, R.S.A.; Sheikh, M.; Kidwai, M.; Sanaullah, A.; Salman, M.; Ilyas, A.; Ahmed, N.; Lal, A. Impact of high-speed handpiece noise-induced dental anxiety on heart rate: Analyzing experienced and non-experienced patients-a comparative study. BMC Oral Health 2024, 24, 265. [Google Scholar] [CrossRef] [PubMed]
- Settineri, S.; Tati, F.; Fanara, G. Gender differences in dental anxiety: Is the chair position important. J. Contemp. Dent. Pract. 2005, 6, 115–122. [Google Scholar]
- Liddell, A.; Locker, D. Gender and age differences in attitudes to dental pain and dental control. Community Dent. Oral Epidemiol. 1997, 25, 314–318. [Google Scholar] [CrossRef]
- Marca-Frances, G.; Frigola-Reig, J.; Menéndez-Signorini, J.A.; Compte-Pujol, M.; Massana-Morera, E. Defining patient communication needs during hospitalization to improve patient experience and health literacy. BMC Health Serv. Res. 2020, 20, 131. [Google Scholar] [CrossRef] [PubMed]
- Bacigalupe, A.; Martín, U. Gender inequalities in depression/anxiety and the consumption of psychotropic drugs: Are we medicalising women’s mental health? Scand. J. Public Health 2021, 49, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Maestre-Miquel, C.; López-de-Andrés, A.; Ji, Z.; de Miguel-Diez, J.; Brocate, A.; Sanz-Rojo, S.; López-Farre, A.; Carabantes-Alarcon, D.; Jiménez-García, R.; Zamorano-León, J.J. Gender differences in the prevalence of mental health, psychological distress and psychotropic medication consumption in Spain: A nationwide population-based study. Int. J. Environ. Res. Public Health 2021, 18, 6350. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value | |
|---|---|---|
| Women | Men | |
| Mean ± SD | ||
| Age [years] | 41.70 ± 17.06 | 45.49 ± 16.32 |
| n (%) | ||
| Number of participants | 147 (59.51) | 100 (40.49) |
| Age [years] | ||
| 18–34 | 45 (30.60) | 34 (34.00) |
| 35–54 | 49 (33.30) | 36 (36.00) |
| 55–76 | 53 (36.10) | 30 (30.00) |
| Education | ||
| primary/middle school/secondary | 36 (24.00) | 34 (34.00) |
| Higher | 111 (76.00) | 66 (66.00) |
| First-time hygiene visit | ||
| Yes | 14 (9.52) | 12 (12.00) |
| No | 133 (90.47) | 88 (88.00) |
| Orthodontic treatment in the past | ||
| Yes | 62 (42.18) | 33 (33.00) |
| No | 85 (57.82) | 67 (67.00) |
| Dental visits in childhood | ||
| Yes | 137 (93.20) | 86 (86.00) |
| No | 10 (6.80) | 14 (14.00) |
| Physical health problems | ||
| Yes | 48 (32.65) | 20 (20.00) |
| No | 99 (67.35) | 80 (80.00) |
| Mental health problems | ||
| Yes | 16 (10.88) | 2 (2.00) |
| No | 131 (89.12) | 98 (98.00) |
| Diagnosis of dentophobia | ||
| Yes | 0 (0.00%) | 0 (0.00%) |
| No | 147 (100.00%) | 100 (100.00%) |
| Variable | Before Procedure (Mean ± SD) | Test Result | p-Value | After Procedure (Mean ± SD) | Test Result | p-Value | ||
|---|---|---|---|---|---|---|---|---|
| Women | Men | Women | Men | |||||
| Dental anxiety (MDAS) | 9.01 ± 3.86 | 7.83 ± 2.92 | Z= −2.43 | 0.015 | - | - | - | - |
| Trait anxiety (STAI X2) | 45.74 ± 3.95 | 43.98 ± 4.16 | Z = −3.13 | 0.002 | - | - | - | - |
| State anxiety (STAI X1) | 45.77 ± 4.17 | 45.81 ± 4.33 | Z = 0.39 | NS | 44.20 ± 4.10 | 43.16 ± 4.10 | Z = −1.96 | NS |
| Dental fear (Gatchel’s scale) | 3.86 ± 2.50 | 3.35 ± 2.12 | Z = −1.32 | NS | 3.21 ± 2.31 | 2.77 ± 2.00 | Z = −1.32 | NS |
| Fear related to the hygiene procedure (author-developed question) | 2.67 ± 2.19 | 2.27 ± 1.65 | Z = −0.81 | NS | 2.12 ± 1.69 | 1.91 ± 1.28 | Z = −0.06 | NS |
| Heart rate [bpm] * | 76.37 ± 8.01 | 74.39 ± 9.38 | Z = −1.33 | NS | 74.82 ± 7.88 | 71.94 ± 7.77 | Z = −2.55 | 0.0108 |
| Gender | Mild Anxiety | Moderate Anxiety | High Anxiety | Severe Anxiety |
|---|---|---|---|---|
| Women n (%) | 60 (40.82%) | 37 (25.17%) | 20 (13.61%) | 30 (20.41%) |
| Men n (%) | 55 (55.00%) | 19 (19.00%) | 15 (15.00%) | 11 (11.00%) |
| Gender | No Anxiety | Mild Anxiety | Moderate Anxiety | Severe Anxiety |
|---|---|---|---|---|
| Women n (%) | 0 (0.00) | 30 (20.41%) | 112 (76.19%) | 5 (3.40%) |
| Men n (%) | 0 (0.00) | 37 (37.00%) | 61 (61.00%) | 2 (2.00%) |
| Factors That, in the Patient’s Opinion, Could Reduce Negative Emotions | (Mean ± SD) | Test Result | p-Value | |
|---|---|---|---|---|
| Women | Men | |||
| Absence of tools in the field of view | 1.64 ± 0.91 | 1.21 ± 0.98 | Z = −3.46 | 0.001 |
| Absence of sounds from working tools | 1.60 ± 0.90 | 1.28 ± 0.92 | Z = −2.53 | 0.012 |
| Absence of characteristic dental office smells | 1.61 ± 0.92 | 1.29 ± 1.01 | Z = −2.46 | 0.014 |
| Possibility of using sedatives and painkillers | 1.97 ± 0.88 | 1.69 ± 0.93 | Z = −2.20 | 0.028 |
| Possibility of taking breaks according to the patient’s needs | 2.33 ± 0.78 | 2.04 ± 0.72 | Z = −3.00 | 0.003 |
| Possibility of contacting the clinic/dentist/hygienist | 2.69 ± 0.57 | 2.48 ± 0.61 | Z = −2.62 | 0.009 |
| Variable | Women n (%) | Men n (%) | Test Result | p-Value |
|---|---|---|---|---|
| Physical health problems | 48 (32.65) | 20 (20.00) | Chi2 = 4.78 | 0.029 |
| Mental health problems | 16 (10.88) | 2 (2.00) | Chi2 = 6.95 | 0.009 |
| Taking medication | 67 (45.58) | 26 (26.00) | Chi2 = 9.72 | 0.002 |
| Thyroid medications | 25 (17.01) | 2 (2.00) | Chi2 = 13.77 | 0.000 |
| Medications for depression, insomnia, and other mental disorders (psychotropic drugs) | 14 (9.52) | 2 (2.00) | Chi2 = 5.56 | 0.018 |
| “Other” medications | 19 (12.93) | 3 (3.00) | Chi2 = 7.23 | 0.007 |
| Variable | Thyroid Medications | Medications for Depression, Insomnia, and Other Mental Disorders (Psychotropic Drugs) | “Other” Medications | |||
|---|---|---|---|---|---|---|
| Test Result | p-Value | Test Result | p-Value | Test Result | p-Value | |
| Dental Anxiety (MDAS) | Chi2 = 1.16 | NS | Chi2 = 26.13 | <0.0001 | Chi2 = 5.65 | NS |
| Trait Anxiety (STAI X2) | Chi2 = 5.96 | 0.0507 (MS) | Chi2 = 0.57 | NS | Chi2 = 11.59 | 0.003 |
| Variable | R2 | β | F | p-Value |
|---|---|---|---|---|
| Step 1 | 0.07 | 19.12 | <0.0001 | |
| Taking medication | −0.27 | <0.0001 | ||
| Step 2 | 0.10 | 13.26 | <0.0001 | |
| Taking medication | −0.24 | 0.000 | ||
| Gender | −0.16 | 0.009 | ||
| Step 3 | 0.11 | 10.19 | <0.0001 | |
| Taking medication (1-yes, 2-no) | −0.23 | 0.000 | ||
| Gender (1-woman, 2-man) | −0.14 | 0.031 | ||
| Absence of tools in the field of view | 0.12 | MS |
| Variable | R2 | β | F | p-Value |
|---|---|---|---|---|
| Step 1 | 0.10 | 28.64 | <0.0001 | |
| Pain experienced during hygiene procedures | 0.32 | <0.0001 | ||
| Step 2 | 0.17 | 25.69 | <0.0001 | |
| Pain experienced during hygiene procedures | 0.30 | <0.0001 | ||
| Traumatic dental experiences in the past | −0.26 | <0.0001 | ||
| Step 3 | 0.21 | 21.56 | <0.0001 | |
| Pain experienced during hygiene procedures | 0.30 | <0.0001 | ||
| Traumatic dental experiences in the past | −0.25 | <0.0001 | ||
| Absence of sounds from working tools | 0.19 | 0.001 | ||
| Step 4 | 0.25 | 20.46 | <0.0001 | |
| Pain experienced during hygiene procedures | 0.27 | <0.0001 | ||
| Traumatic dental experiences in the past | −0.25 | <0.0001 | ||
| Absence of sounds from working tools | 0.22 | 0.000 | ||
| Frequency of dental visits | −0.21 | 0.000 | ||
| Step 5 | 0.28 | 18.30 | <0.0001 | |
| Pain experienced during hygiene procedures | 0.26 | <0.0001 | ||
| Traumatic dental experiences in the past | −0.26 | <0.0001 | ||
| Absence of sounds from working tools | 0.22 | 0.000 | ||
| Frequency of dental visits | −0.19 | 0.001 | ||
| Number of carious lesions | 0.15 | 0.007 | ||
| Step 6 | 0.29 | 16.47 | <0.0001 | |
| Pain experienced during hygiene procedures | 0.27 | <0.0001 | ||
| Traumatic dental experiences in the past | −0.26 | <0.0001 | ||
| Absence of sounds from working tools | 0.21 | 0.000 | ||
| Frequency of dental visits | −0.19 | 0.001 | ||
| Number of carious lesions | 0.14 | 0.009 | ||
| Taking medication | −0.13 | 0.019 | ||
| Step 7 | 0.30 | 14.77 | <0.0001 | |
| Pain experienced during hygiene procedures | 0.24 | <0.0001 | ||
| Traumatic dental experiences in the past | −0.25 | <0.0001 | ||
| Absence of sounds from working tools | 0.20 | 0.000 | ||
| Frequency of dental visits | −0.17 | 0.0029 | ||
| Number of carious lesions | 0.13 | 0.0162 | ||
| Taking medication | −0.12 | 0.0317 | ||
| Oral hygiene self-assessment | −0.11 | NS (0.0617) | ||
| Step 8 | 0.31 | 13.37 | <0.0001 | |
| Pain experienced during hygiene procedures | 0.24 | <0.0001 | ||
| Traumatic dental experiences in the past (1-yes, 2-no) | −0.25 | <0.0001 | ||
| Absence of sounds from working tools | 0.19 | 0.0010 | ||
| Frequency of dental visits (1–rare, 2–normal, 3–frequent | −0.17 | 0.0030 | ||
| Number of carious lesions | 0.13 | 0.0171 | ||
| Taking medication (1-yes, 2-no) | −0.10 | NS (0.0744) | ||
| Oral hygiene self-assessment (scale 0–4, 0–very poor, 4–very good) | −0.12 | 0.0448 | ||
| Gender (1-woman, 2-man) | −0.09 | NS (0.0960) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leśna, M.; Górna, K.; Kwiatek, J. Managing Fear and Anxiety in Patients Undergoing Dental Hygiene Visits with Guided Biofilm Therapy: Analysis of Psychological and Physiological Differences Between Women and Men—A Conceptual and Multivariate Regression Model. J. Pers. Med. 2025, 15, 147. https://doi.org/10.3390/jpm15040147
Leśna M, Górna K, Kwiatek J. Managing Fear and Anxiety in Patients Undergoing Dental Hygiene Visits with Guided Biofilm Therapy: Analysis of Psychological and Physiological Differences Between Women and Men—A Conceptual and Multivariate Regression Model. Journal of Personalized Medicine. 2025; 15(4):147. https://doi.org/10.3390/jpm15040147
Chicago/Turabian StyleLeśna, Marta, Krystyna Górna, and Jakub Kwiatek. 2025. "Managing Fear and Anxiety in Patients Undergoing Dental Hygiene Visits with Guided Biofilm Therapy: Analysis of Psychological and Physiological Differences Between Women and Men—A Conceptual and Multivariate Regression Model" Journal of Personalized Medicine 15, no. 4: 147. https://doi.org/10.3390/jpm15040147
APA StyleLeśna, M., Górna, K., & Kwiatek, J. (2025). Managing Fear and Anxiety in Patients Undergoing Dental Hygiene Visits with Guided Biofilm Therapy: Analysis of Psychological and Physiological Differences Between Women and Men—A Conceptual and Multivariate Regression Model. Journal of Personalized Medicine, 15(4), 147. https://doi.org/10.3390/jpm15040147