
Evaluation of an mHealth Medication Regimen Self-Management Program for African American and Hispanic Uncontrolled Hypertensives

Abstract
:1. Introduction
2. Results and Discussion
2.1. Results

{kind=link}
{kind=link}
| Variable | SMASH | SC | |||||
|---|---|---|---|---|---|---|---|
| All (n = 18) a | African Americans (n = 8) | Hispanics (n = 10) | All (n = 20) a | African Americans (n = 10) | Hispanics (n = 10) | ||
| Age in years (Mean ± Std.) | 47.50 ± 11.80 | 55.63 ± 10.17 | 41.00 ± 8.78 | 48.45 ± 11.32 | 52.9 ± 11.02 | 44.00 ± 10.25 | |
| Gender | Male | 7 (38.9%) | 1 (12.5%) | 6 (60.0%) | 8 (40.0%) | 2 (20.0%) | 6 (60.0%) |
| Female | 11 (61.1%) | 7 (87.5%) | 4 (40.0%) | 12 (60.0%) | 8 (80.0%) | 4 (40.0%) | |
| Single | 3 (16.7%) | 0 (0.0%) | 3 (30.0%) | 10 (50.0%) | 6 (60.0%) | 4 (40.0%) | |
| Marital Status | Married/With significant other | 10 (55.6%) | 3 (37.5%) | 7 (70.0%) | 6 (30.0%) | 2 (20.0%) | 4 (40.0%) |
| Separated/Divorced | 4 (22.2%) | 4 (50.5%) | 0 (0.0%) | 3 (15.0%) | 2 (20.0%) | 1 (10.0%) | |
| Widowed | 1 (5.6%) | 1 (12.5%) | 0 (0.0%) | 1 (5.0%) | 0 (0.00%) | 1 (10.0%) | |
| Education | High School or less | 10 (55.6%) | 3 (37.5%) | 7 (70.0%) | 12 (60.0%) | 5 (50.0%) | 7 (70.0%) |
| Partial/college graduate | 8 (44.4%) | 5 (62.5%) | 3 (30.0%) | 8 (40.0%) | 5 (50.0%) | 3 (30.0%) | |
| $0-25K | 7 (38.9%) | 3 (37.5%) | 4 (40.0%) | 8 (40.0%) | 5 (50.0%) | 3 (30.0%) | |
| Income | $25-50K | 6 (33.3%) | 2 (25.5%) | 4 (40.0%) | 5 (25.0%) | 3 (30.0%) | 2 (20.0%) |
| $ >50K | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1 (5.0%) | 0 (0.0%) | 1 (10.0%) | |
| Not Reported | 5 (27.8%) | 3 (37.5%) | 2 (20.0%) | 6 (30.0%) | 2 (20.0%) | 4 (40.0%) | |
| Employment | Full-/Part-time | 11 (61.1%) | 3 (37.5%) | 8 (80.0%) | 14 (70.0%) | 5 (50.0%) | 9 (90.0%) |
| Retired/Disabled | 2 (11.1%) | 2 (25.5%) | 0 (0.0%) | 3 (15.0%) | 3 (30.0%) | 0 (0.0%) | |
| Unemployed | 5 (27.8%) | 3 (37.5%) | 2 (20.0%) | 3 (15.0%) | 2 (20.0%) | (10.0%) | |
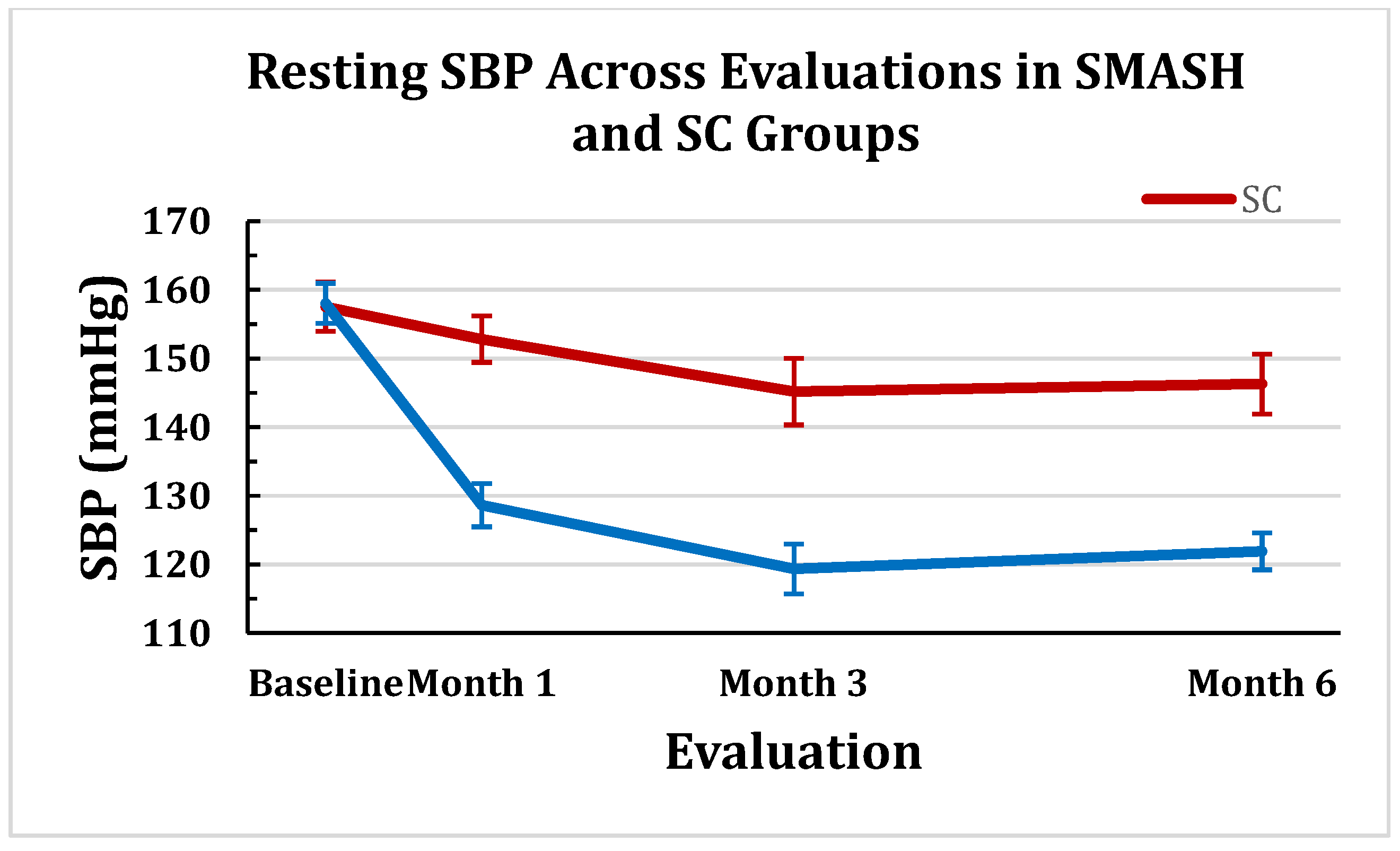
2.1.1. Changes in Clinic Systolic Blood Pressure (SBP)

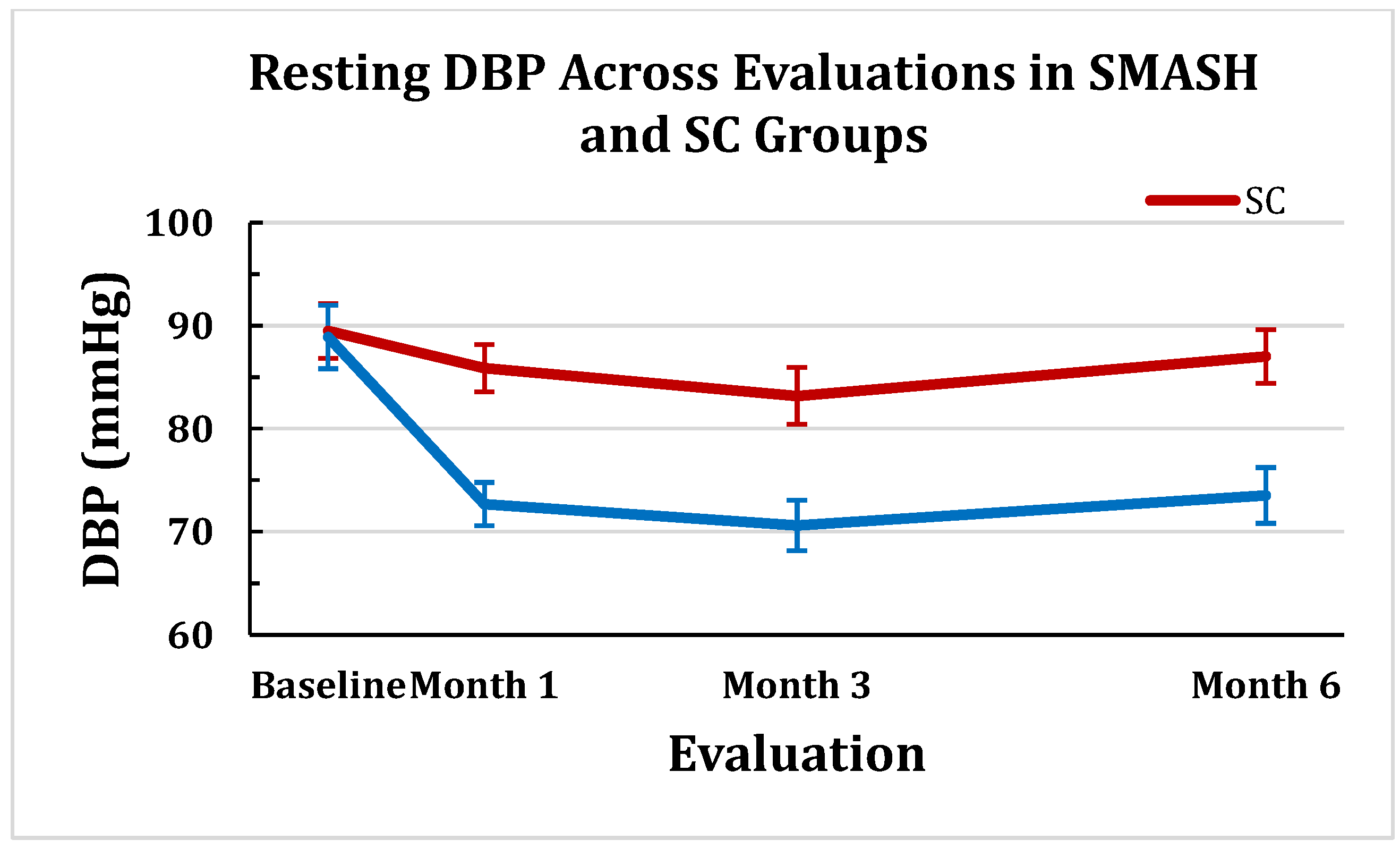
2.1.2. Changes in Clinic Diastolic Blood Pressure (DBP)

2.1.3. Changes in SBP Control
| Controlled SBP | SMASH | Control | p-value |
|---|---|---|---|
| Baseline | 00.0% | 00.0% | 1.000 |
| Month 1 | 70.6% | 15.8% | 0.001 |
| Month 3 | 94.4% | 55.0% | 0.009 |
| Month 6 | 94.4% | 41.2% | 0.003 |
| Sustained from month 1 through month 6 | 70.6% | 6.3% | 0.0004 |
2.1.4. Changes in DBP Control
| Controlled DBP | SMASH | Control | p-value |
|---|---|---|---|
| Baseline | 50.0% | 55.0% | 1.0 |
| Month 1 | 100.0% | 68.4% | 0.02 |
| Month 3 | 100.0% | 65.0% | 0.009 |
| Month 6 | 94.4% | 76.5% | 0.04 |
| Sustained from month 1 through month 6 | 94.1% | 37.5% | 0.0008 |
2.1.5. Feasibility Measures (Recruitment and Retention Rates, MA, BP Adherence)
2.1.6. Cost of SMASH Implementation
2.2. Discussion
3. Experimental Section
3.1. Study Participants
3.2. BP Screening and Randomization
3.3. SMASH Protocol
3.4. Outcome Measures
3.5. Data Analytic Plan
4. Conclusions
Acknowledgements
Author Contributions
Conflicts of Interest
References
- James, P.A.; Oparil, S.; Carter, B.L.; Cushman, W.C.; Dennison-Himmelfarb, C.; Handler, J.; Lackland, D.T.; LeFevre, M.L.; MacKenzie, T.D.; Ogedegbe, O.; et al. 2014 evidence-based guideline for the management of high blood pressure in adults: Report from the panel members appointed to the eighth joint national committee (jnc 8). JAMA 2014, 311, 507–520. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.S.; Ostchega, Y.; Louis, T. Recent trends in the prevalence of high blood pressure and its treatment and control, 1999–2008. NCHS Data Brief 2010, 48, 1–8. [Google Scholar] [PubMed]
- Keenan, N.L.; Rosendorf, K.A.; Centers for Disease Control and Prevention (CDC). Prevalence of hypertension and controlled hypertension—united states, 2005–2008. MMWR Surveill. Summ. 2011, 60, 94–97. [Google Scholar] [PubMed]
- Egan, B.M.; Zhao, Y.; Axon, R.N. US trends in prevalence, awareness, treatment, and control of hypertension, 1988–2008. JAMA 2010, 303, 2043–2050. [Google Scholar] [CrossRef] [PubMed]
- Bosworth, H.B.; Dudley, T.; Olsen, M.K.; Voils, C.I.; Powers, B.; Goldstein, M.K.; Oddone, E.Z. Racial differences in blood pressure control: Potential explanatory factors. Am. J. Med. 2006, 119, 70.e9–70.e15. [Google Scholar] [CrossRef] [PubMed]
- Holmes, H.M.; Luo, R.; Hanlon, J.T.; Elting, L.S.; Suarez-Almazor, M.; Goodwin, J.S. Ethnic disparities in adherence to antihypertensive medications of medicare part d beneficiaries. J. Am. Geriatr. Soc. 2012, 60, 1298–1303. [Google Scholar] [CrossRef] [PubMed]
- Ishisaka, D.Y.; Jukes, T.; Romanelli, R.J.; Wong, K.S.; Schiro, T.A. Disparities in adherence to and persistence with antihypertensive regimens: An exploratory analysis from a community-based provider network. J. Am. Soc. Hypertens. 2012, 6, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Lemstra, M.; Alsabbagh, M.W. Proportion and risk indicators of nonadherence to antihypertensive therapy: A meta-analysis. Patient Prefer. Adherence 2014, 8, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Olives, C.; Myerson, R.; Mokdad, A.H.; Murray, C.J.; Lim, S.S. Prevalence, awareness, treatment, and control of hypertension in United States counties, 2001–2009. PLoS ONE 2013, 8, e60308. [Google Scholar] [CrossRef] [PubMed]
- Hajjar, I.; Kotchen, T.A. Trends in prevalence, awareness, treatment, and control of hypertension in the united states, 1988–2000. JAMA 2003, 290, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Dusing, R. Overcoming barriers to effective blood pressure control in patients with hypertension. Curr. Med. Res. Opin. 2006, 22, 1545–1553. [Google Scholar] [CrossRef] [PubMed]
- Osterberg, L.; Blaschke, T. Adherence to medication. N. Engl. J. Med. 2005, 353, 487–497. [Google Scholar] [CrossRef] [PubMed]
- Ho, P.M.; Bryson, C.L.; Rumsfeld, J.S. Medication adherence: Its importance in cardiovascular outcomes. Circulation 2009, 119, 3028–3035. [Google Scholar] [CrossRef] [PubMed]
- Bautista, R.E.; Graham, C.; Mukardamwala, S. Health disparities in medication adherence between african-americans and caucasians with epilepsy. Epilepsy Behav. 2011, 22, 495–498. [Google Scholar] [CrossRef] [PubMed]
- Dickson, V.V.; Knafl, G.J.; Riegel, B. Predictors of medication nonadherence differ among black and white patients with heart failure. Res. Nurs. Health 2015, 38, 289–300. [Google Scholar] [CrossRef] [PubMed]
- Kales, H.C.; Nease, D.E., Jr.; Sirey, J.A.; Zivin, K.; Kim, H.M.; Kavanagh, J.; Lynn, S.; Chiang, C.; Neighbors, H.W.; Valenstein, M.; et al. Racial differences in adherence to antidepressant treatment in later life. Am. J. Geriatr. Psychiatry 2013, 21, 999–1009. [Google Scholar] [CrossRef] [PubMed]
- Lewey, J.; Shrank, W.H.; Bowry, A.D.; Kilabuk, E.; Brennan, T.A.; Choudhry, N.K. Gender and racial disparities in adherence to statin therapy: A meta-analysis. Am. Heart J. 2013, 165, 665–678. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Thumula, V.; Pace, P.F.; Banahan, B.F., 3rd; Wilkin, N.E.; Lobb, W.B. Predictors of medication nonadherence among patients with diabetes in Medicare Part D programs: A retrospective cohort study. Clin. Ther. 2009, 31, 2178–2188. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.; Bills, J.E.; Hecht, T.J.; Light, R.P. Role of home blood pressure monitoring in overcoming therapeutic inertia and improving hypertension control: A systematic review and meta-analysis. Hypertension 2011, 57, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Cappuccio, F.P.; Kerry, S.M.; Forbes, L.; Donald, A. Blood pressure control by home monitoring: Meta-analysis of randomised trials. Br. Med. J. 2004, 329. [Google Scholar] [CrossRef] [PubMed]
- Glynn, L.G.; Murphy, A.W.; Smith, S.M.; Schroeder, K.; Fahey, T. Interventions used to improve control of blood pressure in patients with hypertension. Cochrane Database Syst. Rev. 2010. [Google Scholar] [CrossRef]
- Militello, L.K.; Kelly, S.A.; Melnyk, B.M. Systematic review of text-messaging interventions to promote healthy behaviors in pediatric and adolescent populations: Implications for clinical practice and research. Worldviews Evid. Based Nurs. 2012, 9, 66–77. [Google Scholar] [CrossRef] [PubMed]
- Free, C.; Phillips, G.; Galli, L.; Watson, L.; Felix, L.; Edwards, P.; Patel, V.; Haines, A. The effectiveness of mobile-health technology-based health behaviour change or disease management interventions for health care consumers: A systematic review. PLoS Med. 2013, 10, e1001362. [Google Scholar] [CrossRef] [PubMed]
- de Jongh, T.; Gurol-Urganci, I.; Vodopivec-Jamsek, V.; Car, J.; Atun, R. Mobile phone messaging for facilitating self-management of long-term illnesses. Cochrane Database Syst. Rev. 2012, 12. [Google Scholar] [CrossRef]
- Mobile technology fact sheet: Data from pew internet and American life project survey in January 2014. Available online: http://www.pewinternet.org/fact-sheets/mobile-technology-fact-sheet/ (accessed on 10 May 2014).
- Smith, A. U.S. smartphone use in 2015. Available online: http://www.pewinternet.org/2015/04/01/us-smartphone-use-in-2015/ (accessed on 3 April 2015).
- McGillicuddy, J.W.; Weiland, A.K.; Frenzel, R.M.; Mueller, M.; Brunner-Jackson, B.M.; Taber, D.J.; Baliga, P.K.; Treiber, F.A. Patient attitudes toward mobile phone-based health monitoring: Questionnaire study among kidney transplant recipients. J. Med. Internet Res. 2013, 15, e6. [Google Scholar] [CrossRef] [PubMed]
- Price, M.; Williamson, D.; McCandless, R.; Mueller, M.; Gregoski, M.; Brunner-Jackson, B.; Treiber, E.; Davidson, L.; Treiber, F. Hispanic migrant farm workers’ attitudes toward mobile phone-based telehealth for management of chronic health conditions. J. Med. Internet. Res. 2013, 15, e76. [Google Scholar] [CrossRef] [PubMed]
- Figge, H.L. Electronic tools to measure and enhance medication adherence. US Pharm. 2010, 36, 6–10. [Google Scholar]
- Demonceau, J.; Ruppar, T.; Kristanto, P.; Hughes, D.A.; Fargher, E.; Kardas, P.; De Geest, S.; Dobbels, F.; Lewek, P.; Urquhart, J.; et al. Identification and assessment of adherence-enhancing interventions in studies assessing medication adherence through electronically compiled drug dosing histories: A systematic literature review and meta-analysis. Drugs 2013, 73, 545–562. [Google Scholar] [CrossRef] [PubMed]
- Checchi, K.D.; Huybrechts, K.F.; Avorn, J.; Kesselheim, A.S. Electronic medication packaging devices and medication adherence: A systematic review. JAMA 2014, 312, 1237–1247. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.R.; Corley, D.J.; Lennie, T.A.; Moser, D.K. Effect of a medication-taking behavior feedback theory-based intervention on outcomes in patients with heart failure. J. Card. Fail. 2012, 18, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Eisenberger, U.; Wuthrich, R.P.; Bock, A.; Ambuhl, P.; Steiger, J.; Intondi, A.; Kuranoff, S.; Maier, T.; Green, D.; DiCarlo, L.; et al. Medication adherence assessment: High accuracy of the new ingestible sensor system in kidney transplants. Transplantation 2013, 96, 245–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Markland, D.; Ryan, R.M.; Tobin, V.J.; Rollnick, S. Motivational interviewing and self-determination theory. J. Soc. Clin. Psychol. 2005, 24, 811–831. [Google Scholar] [CrossRef]
- Ryan, R.; Patrick, H.; Deci, E.; Williams, G. Facilitating health behaviour change and its maintenance: Interventions based on self-determination theory. Eur. Health Psychol. 2008, 10, 2–5. [Google Scholar]
- Deci, E.L.; Koestner, R.; Ryan, R.M. A meta-analytic review of experiments examining the effects of extrinsic rewards on intrinsic motivation. Psychol. Bull. 1999, 125, 627–668. [Google Scholar] [CrossRef] [PubMed]
- Ng, J.; Chiu, Y.L.; Awni, W.; Bernstein, B.; Causemaker, S.J.; Klein, C.E. Pharmacokinetics and safety of the lopinavir/ritonavir tablet 500/125 mg twice daily coadministered with efavirenz in healthy adult participants. J. Clin. Pharmacol. 2012, 52, 1248–1254. [Google Scholar] [CrossRef] [PubMed]
- Resnicow, K.; Davis, R.E.; Zhang, G.; Konkel, J.; Strecher, V.J.; Shaikh, A.R.; Tolsma, D.; Calvi, J.; Alexander, G.; Anderson, J.P.; et al. Tailoring a fruit and vegetable intervention on novel motivational constructs: Results of a randomized study. Ann. Behav. Med. 2008, 35, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.M.; Kuhl, J.; Deci, E.L. Nature and autonomy: An organizational view of social and neurobiological aspects of self-regulation in behavior and development. Dev. Psychopathol. 1997, 9, 701–728. [Google Scholar] [CrossRef] [PubMed]
- Williams, G.C.; Gagne, M.; Ryan, R.M.; Deci, E.L. Facilitating autonomous motivation for smoking cessation. Health Psychol. 2002, 21, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Williams, G.C.; Rodin, G.C.; Ryan, R.M.; Grolnick, W.S.; Deci, E.L. Autonomous regulation and long-term medication adherence in adult outpatients. Health Psychol. 1998, 17, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Mcgillicuddy, J.; Anderson, A.; Favela, A.; Sox, L.; Wilder, S.; Brunner-Jackson, B.; Mueller, M.; Treiber, F. Impact of a patient and provider centered health technology enabled medical regimen self management program among african american uncontrolled hypertensives. Psychosom. Med. 2015, in press. [Google Scholar]
- Sieverdes, J.; Gregoski, M.; Patel, S.; Williamson, D.; Brunner-Jackson, B.; Rundbaken, J.; Treiber, E.; Davidson, L.; Treiber, F. Medication and blood pressure mhealth self-management program with hispanic hypertensives: A proof of concept trial. Smart Homecare Technol. Telehealth. 2013, 1, 1–10. [Google Scholar] [CrossRef]
- McGillicuddy, J.W.; Gregoski, M.J.; Weiland, A.K.; Rock, R.A.; Brunner-Jackson, B.M.; Patel, S.K.; Thomas, B.S.; Taber, D.J.; Chavin, K.D.; Baliga, P.K.; et al. Mobile health medication adherence and blood pressure control in renal transplant recipients: A proof-of-concept randomized controlled trial. JMIR Res. Protoc. 2013, 2, e32. [Google Scholar] [CrossRef] [PubMed]
- McGillicuddy, J.; Gregoski, M.; Brunner-Jackson, B.; Weiland, A.; Patel, S.; Rock, R.; Treiber, E.; Davidson, L.; Treiber, F. Facilitating medication adherence and eliminating therapeutic inertia using wireless technology: Proof-of-concept findings with uncontrolled hypertensives and kidney transplant recipients. In Proceedings of the Conference on Wireless Health, New York, NY, USA, 2012. [CrossRef]
- Russell, C.; Conn, V.; Ashbaugh, C.; Madsen, R.; Wakefield, M.; Webb, A.; Coffey, D.; Peace, L. Taking immunosuppressive medications effectively (timelink): A pilot randomized controlled trial in adult kidney transplant recipients. Clin. Transplant. 2010, 25, 864–870. [Google Scholar] [CrossRef] [PubMed]
- McGillicuddy, J.; Taber, D.; Mueller, M.; Patel, S.; Baliga, P.; Chavin, K.; Sox, L.; Favela, A.; Brunner-Jackson, B.; Treiber, F. Sustainability of mobile health medication adherence and blood pressure control program among kidney transplant patients: A one year follow-up pilot study. Prog. Transplant. 2015, in press. [Google Scholar]
- Cauce, A.M.; Domenech-Rodriguez, M.; Paradise, M.; Cochran, B.N.; Shea, J.M.; Srebnik, D.; Baydar, N. Cultural and contextual influences in mental health help seeking: A focus on ethnic minority youth. J. Consult. Clin. Psychol. 2002, 70, 44–55. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.B.; Rodriguez, M.D.; Bernal, G. Culture. J. Clin. Psychol. 2011, 67, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Gregoski, M.; Williamson, D.; Rundbaken, M.; Davidson, L.; Treiber, E.; McCandless, R.; Treiber, F. Smartphone medication adherence stops hypertension (smash) among hispanics. Ann. Behav. Med. 2013, 45, S24. [Google Scholar]
- Gregoski, M.J.; Barnes, V.A.; Tingen, M.S.; Dong, Y.; Zhu, H.; Treiber, F.A. Differential impact of stress reduction programs upon ambulatory blood pressure among African American adolescents: Influences of endothelin-1 gene and chronic stress exposure. Int. J. Hypertens. 2012, 2012. [Google Scholar] [CrossRef] [PubMed]
- Wagner, E.H.; Austin, B.T.; Davis, C.; Hindmarsh, M.; Schaefer, J.; Bonomi, A. Improving chronic illness care: Translating evidence into action. Health Aff. 2001, 20, 64–78. [Google Scholar] [CrossRef]
- Glasgow, R.E.; Orleans, C.T.; Wagner, E.H. Does the chronic care model serve also as a template for improving prevention? Milbank. Q. 2001, 79, 579–612. [Google Scholar] [CrossRef] [PubMed]
- Wagner, E.H.; Glasgow, R.E.; Davis, C.; Bonomi, A.E.; Provost, L.; McCulloch, D.; Carver, P.; Sixta, C. Quality improvement in chronic illness care: A collaborative approach. Jt. Comm. J. Qual. Improv. 2001, 27, 63–80. [Google Scholar] [PubMed]
- O’Donnell, R.R. Stepped care and e-health in behavioral managed care. In Stepped Care and e-Health: Practical Applications to Behavioral Disorders; O’Donohue, W.T., Draper, C., Eds.; Springer: New York, NY, USA, 2011; Volume 1, Chapter 14; pp. 263–282. [Google Scholar]
- Khaylis, A.; Yiaslas, T.; Bergstrom, J.; Gore-Felton, C. A review of efficacious technology-based weight-loss interventions: Five key components. Telemed. J. E Health 2010, 16, 931–938. [Google Scholar] [CrossRef] [PubMed]
- Reinders, A.; Reggiori, F.; Shennan, A.H. Validation of the dinamap procare blood pressure device according to the international protocol in an adult population. Blood Press. Monit. 2006, 11, 293–296. [Google Scholar] [CrossRef] [PubMed]
- Appel, L.J.; Champagne, C.M.; Harsha, D.W.; Cooper, L.S.; Obarzanek, E.; Elmer, P.J.; Stevens, V.J.; Vollmer, W.M.; Lin, P.H.; Svetkey, L.P.; et al. Effects of comprehensive lifestyle modification on blood pressure control: Main results of the premier clinical trial. Jama 2003, 289, 2083–2093. [Google Scholar] [PubMed]
- Julius, S.; Nesbitt, S.D.; Egan, B.M.; Weber, M.A.; Michelson, E.L.; Kaciroti, N.; Black, H.R.; Grimm, R.H., Jr.; Messerli, F.H.; Oparil, S.; et al. Feasibility of treating prehypertension with an angiotensin-receptor blocker. N. Engl. J. Med. 2006, 354, 1685–1697. [Google Scholar] [CrossRef] [PubMed]
- Verdecchia, P.; Angeli, F.; Poeta, F.; Reboldi, G.P.; Borgioni, C.; Pittavini, L.; Porcellati, C. Validation of the A&D UA-774 (UA-767Plus) device for self-measurement of blood pressure. Blood Press. Monit. 2004, 9, 225–229. [Google Scholar] [PubMed]
- Fitzmaurice, G.M.; Laird, N.M.; Ware, J.H. Applied Longitudinal Analysis; John Wiley & Sons: Hoboken, NJ, USA, 2012; Chapter 5.6; pp. 124–127. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Davidson, T.M.; McGillicuddy, J.; Mueller, M.; Brunner-Jackson, B.; Favella, A.; Anderson, A.; Torres, M.; Ruggiero, K.J.; Treiber, F.A. Evaluation of an mHealth Medication Regimen Self-Management Program for African American and Hispanic Uncontrolled Hypertensives. J. Pers. Med. 2015, 5, 389-405. https://doi.org/10.3390/jpm5040389
Davidson TM, McGillicuddy J, Mueller M, Brunner-Jackson B, Favella A, Anderson A, Torres M, Ruggiero KJ, Treiber FA. Evaluation of an mHealth Medication Regimen Self-Management Program for African American and Hispanic Uncontrolled Hypertensives. Journal of Personalized Medicine. 2015; 5(4):389-405. https://doi.org/10.3390/jpm5040389
Chicago/Turabian StyleDavidson, Tatiana M., John McGillicuddy, Martina Mueller, Brenda Brunner-Jackson, April Favella, Ashley Anderson, Magaly Torres, Kenneth J. Ruggiero, and Frank A. Treiber. 2015. "Evaluation of an mHealth Medication Regimen Self-Management Program for African American and Hispanic Uncontrolled Hypertensives" Journal of Personalized Medicine 5, no. 4: 389-405. https://doi.org/10.3390/jpm5040389
APA StyleDavidson, T. M., McGillicuddy, J., Mueller, M., Brunner-Jackson, B., Favella, A., Anderson, A., Torres, M., Ruggiero, K. J., & Treiber, F. A. (2015). Evaluation of an mHealth Medication Regimen Self-Management Program for African American and Hispanic Uncontrolled Hypertensives. Journal of Personalized Medicine, 5(4), 389-405. https://doi.org/10.3390/jpm5040389