
Dietary Antioxidant Vitamins and Minerals and Breast Cancer Risk: Prospective Results from the SUN Cohort

 , ,
, ,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
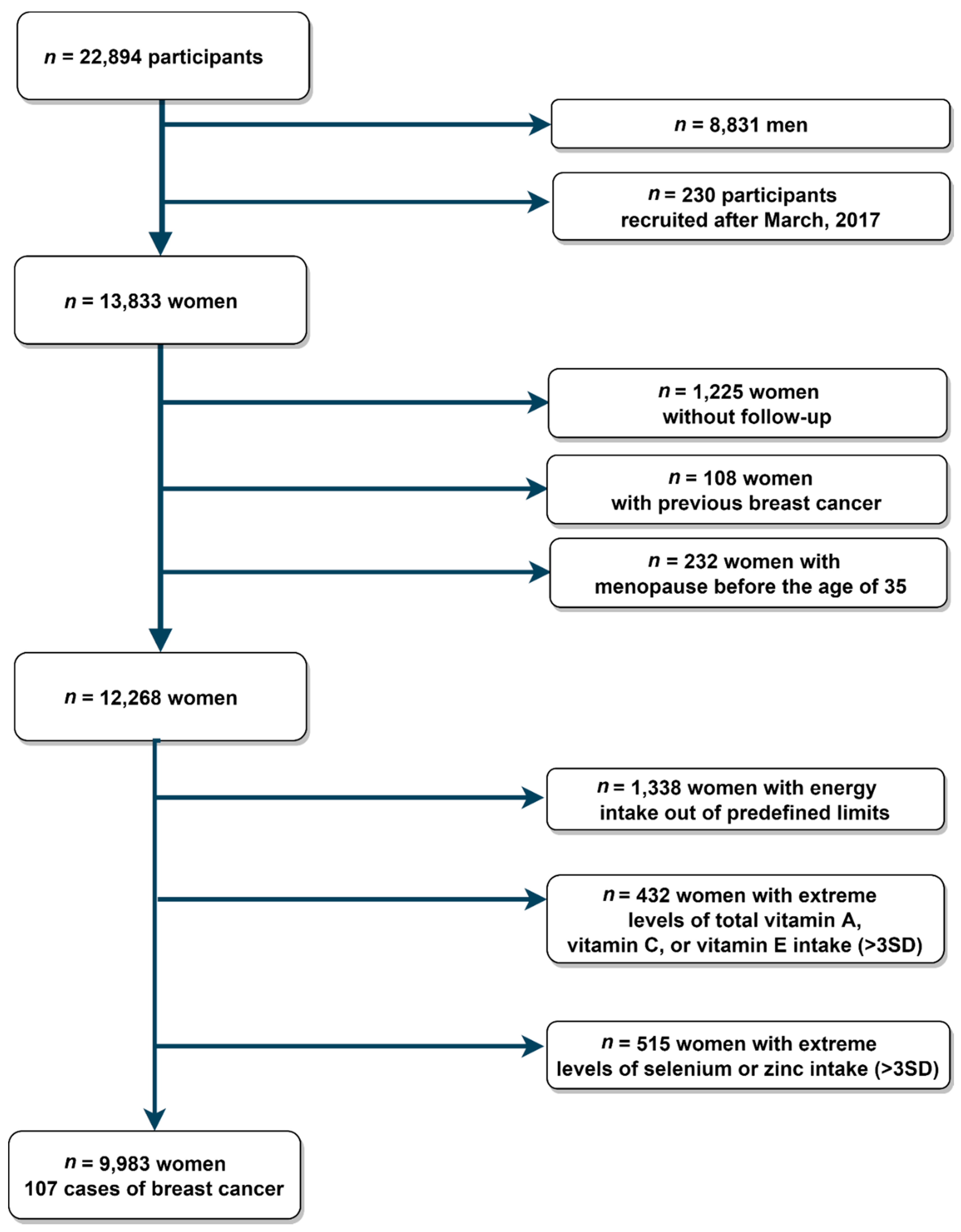
2.1. Study Population
2.2. Exposure Assessment
2.3. Incident Breast Cancer Ascertainment
2.4. Covariates
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wild, C.P.; Weiderpass, E.; Stewart, B.W. (Eds.) World Cancer Report: Cancer Research for Cancer Prevention; International Agency for Research on Cancer: Lyon, France, 2020. Available online: http://publications.iarc.fr/586 (accessed on 22 December 2020).
- Naghavi, M.; Abajobir, A.A.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abera, S.F.; Aboyans, V.; Adetokunboh, O.; Ärnlöv, J.; Afshin, A.; et al. Global, regional, and national age-sex specifc mortality for 264 causes of death, 1980–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar] [CrossRef]
- Smittenaar, C.R.; Petersen, K.A.; Stewart, K.; Moitt, N. Cancer incidence and mortality projections in the UK until 2035. Br. J. Cancer 2016, 115, 1147–1155. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Statistics. Deaths According to Cause of Death. 2018. Available online: https://www.ine.es/en/prensa/edcm_2018_en.pdf (accessed on 30 November 2020).
- Anand, P.; Kunnumakara, A.B.; Sundaram, C.; Harikumar, K.B.; Tharakan, S.T.; Lai, O.S.; Sung, B.; Aggarwal, B.B. Cancer is a preventable disease that requires major lifestyle changes. Pharm. Res. 2008, 25, 2097–2116. [Google Scholar] [CrossRef]
- Vera-Ramirez, L.; Sanchez-Rovira, P.; Ramirez-Tortosa, M.C.; Ramirez-Tortosa, C.L.; Granados-Principal, S.; Lorente, J.A.; Quiles, J.L. Free radicals in breast carcinogenesis, breast cancer progression and cancer stem cells. Biological bases to develop oxidative-based therapies. Crit. Rev. Oncol. Hematol. 2011, 80, 347–368. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Peterson, L.L. The impact of diet on breast cancer outcomes. Curr. Nutr. Rep. 2019, 8, 212–221. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.F.; Rumgay, H.; Dunlop, C.; Ryan, M.; Quartly, F.; Cox, A.; Deas, A.; Elliss-Brookes, L.; Gavin, A.; Hounsome, L.; et al. The fraction of cancer attributable to modifiable risk factors in England, Wales, Scotland, Northern Ireland, and the United Kingdom in 2015. Br. J. Cancer 2018, 118, 1130–1141. [Google Scholar] [CrossRef]
- Key, T.J.; Bradbury, K.E.; Perez-Cornago, A.; Sinha, R.; Tsilidis, K.K.; Tsugane, S. Diet, nutrition, and cancer risk: What do we know and what is the way forward? BMJ 2020, 368, m511. [Google Scholar] [CrossRef] [PubMed]
- Kapil, U.; Bhadoria, A.S.; Sareen, N.; Singh, P.; Dwivedi, S.N. Role of Micronutrients in Breast Cancer: A Review. Int. J. Basic Appl. Med. Sci. 2013, 3, 190–200. [Google Scholar]
- Chen, Q.; Espey, M.G.; Sun, A.Y.; Pooput, C.; Kirk, K.L.; Krishna, M.C.; Khosh, D.B.; Drisko, J.; Levine, M. Pharmacologic doses of ascorbate act as a prooxidant and decrease growth of aggressive tumor xenografts in mice. Proc. Natl. Acad. Sci. USA 2008, 105, 11105–11109. [Google Scholar] [CrossRef]
- Kang, D.H. Oxidative stress, DNA damage, and breast cancer. AACN Clin. Issues 2002, 13, 540–549. [Google Scholar] [CrossRef] [PubMed]
- Moloney, J.N.; Cotter, T.G. ROS signalling in the biology of cancer. Semin. Cell Dev. Biol. 2018, 80, 50–64. [Google Scholar] [CrossRef] [PubMed]
- George, S.; Abrahamse, H. Redox potential of antioxidants in cancer progression and prevention. Antioxidants 2020, 9, 1156. [Google Scholar] [CrossRef] [PubMed]
- Michels, K.B.; Mohllajee, A.P.; Roset-Bahmanyar, E.; Beehler, G.P.; Moysich, K.B. Diet and breast cancer: A review of the prospective observational studies. Cancer 2007, 109, 2712–2749. [Google Scholar] [CrossRef]
- Fulan, H.; Changxing, J.; Yi Baina, W.; Wencui, Z.; Chunqing, L.; Fan, W.; Dandan, L.; Dianjun, S.; Tong, W.; Da, P.; et al. Retinol, vitamins A, C, and e and breast cancer risk: A meta-analysis and meta-regression. Cancer Causes Control 2011, 22, 1383–1396. [Google Scholar] [CrossRef]
- Zeng, J.; Gu, Y.; Fu, H.; Liu, C.; Zou, Y.; Chang, H. Association between one-carbon metabolism-related vitamins and risk of breast cancer: A systematic review and meta-analysis of prospective studies. Clin. Breast Cancer 2020, 20, e469–e480. [Google Scholar] [CrossRef]
- Kuria, A.; Fang, X.; Li, M.; Han, H.; He, J.; Aaseth, J.O.; Cao, Y. Does dietary intake of selenium protect against cancer? A systematic review and meta-analysis of population-based prospective studies. Crit. Rev. Food Sci. Nutr. 2020, 60, 684–694. [Google Scholar] [CrossRef]
- Zhang, D.; Xu, P.; Li, Y.; Wei, B.; Yang, S.; Zheng, Y.; Lyu, L.; Deng, Y.; Zhai, Z.; Li, N.; et al. Association of vitamin C intake with breast cancer risk and mortality: A meta-analysis of observational studies. Aging 2020, 12, 18415–18435. [Google Scholar] [CrossRef] [PubMed]
- SUN Project Coordinators. The SUN Project [Proyecto SUN]. Available online: www.proyectosun.es (accessed on 23 February 2021).
- Carlos, S.; De La Fuente-Arrillaga, C.; Bes-Rastrollo, M.; Razquin, C.; Rico-Campà, A.; Martínez-González, M.A.; Ruiz-Canela, M. Mediterranean diet and health outcomes in the SUN cohort. Nutrients 2018, 10, 439. [Google Scholar] [CrossRef] [PubMed]
- Willett, W. Nutritional Epidemiology, 3rd ed.; Oxford University Press: New York, NY, USA, 2013. [Google Scholar]
- de la Fuente-Arrillaga, C.; Vázquez Ruiz, Z.; Bes-Rastrollo, M.; Sampson, L.; Martinez-González, M.A. Reproducibility of an FFQ validated in Spain. Public Health Nutr. 2010, 13, 1364–1372. [Google Scholar] [CrossRef]
- Martin-Moreno, J.M.; Boyle, P.; Gorgojo, L.; Maisonneuve, P.; Fernandez-Rodriguez, J.C.; Salvini, S.; Willet, W. Development and validation of a food frequency questionnaire in Spain. Int. J. Epidemiol. 1993, 22, 512e9. [Google Scholar] [CrossRef]
- Fernández-Ballart, J.D.; Piñol, J.L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Perez-Bauer, M.; Martínez-González, M.Á.; Salas-Salvadó, J.; Martn-Moreno, J.M.; et al. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef]
- Moreiras, O.; Carbajal, A.; Cabrera, L.; Cuadrado, C. Tablas de Composición de Alimentos (Food Composition Tables), 15th ed.; Piraámide: Madrid, Spain, 2011. [Google Scholar]
- Mataix-Verdú, J.; García-Diaz, L.; Manas, M.; Martinez-Victoria, E.; Sanchez, J.; Borregon, A. Tabla de Composición de Alimentos (Spanish Food Composition Tables), 4th ed.; Universidad de Granada Press: Granada, Spain, 2003. [Google Scholar]
- Bes-Rastrollo, M.; Valdivieso-Pérez, J.; Sánchez-Villegas, A.; Alonso, Á.; Martínez-González, M.Á. Validación del peso e índice de masa corporal auto-declarados de los participantes de una cohorte de graduados universitarios [validation of self-reported weight and body mass index of participants from a cohort of college graduates]. Rev. Esp. Obes. 2005, 3, 352–358. [Google Scholar]
- Martínez-González, M.A.; López-Fontana, C.; Varo, J.J.; Sánchez-Villegas, A.; Martinez, J.A. Validation of the Spanish version of the physical activity questionnaire used in the Nurses’ Health Study and the Health Professionals’ Follow-up Study. Public Health Nutr. 2005, 8, 920–927. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef]
- Sánchez-Quesada, C.; Romanos-Nanclares, A.; Navarro, A.M.; Gea, A.; Cervantes, S.; Martínez-González, M.Á.; Toledo, E. Coffee consumption and breast cancer risk in the SUN project. Eur. J. Nutr. 2020, 59, 3461–3471. [Google Scholar] [CrossRef] [PubMed]
- Romanos-Nanclares, A.; Toledo, E.; Gardeazabal, I.; Jiménez-Moleón, J.J.; Martínez-González, M.A.; Gea, A. Sugar-sweetened beverage consumption and incidence of breast cancer: The Seguimiento Universidad de Navarra (SUN) Project. Eur. J. Nutr. 2019, 58, 2875–2886. [Google Scholar] [CrossRef]
- Romanos-Nanclares, A.; Gea, A.; Martínez-González, M.Á.; Zazpe, I.; Gardeazabal, I.; Fernandez-Lazaro, C.I.; Toledo, E. Carbohydrate quality index and breast cancer risk in a Mediterranean cohort: The SUN project. Clin. Nutr. 2020, 40, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Romanos-Nanclares, A.; Sánchez-Quesada, C.; Gardeazábal, I.; Martínez-González, M.Á.; Gea, A.; Toledo, E. phenolic acid subclasses, individual compounds, and breast cancer risk in a Mediterranean cohort: The SUN Project. J. Acad. Nutr. Diet. 2020, 120, 1002–1015.e5. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Sandin, S.; Löf, M.; Hébert, J.R.; Adami, H.O.; Weiderpass, E. Prospective study of dietary inflammatory index and risk of breast cancer in Swedish women. Br. J. Cancer 2015, 113, 1099–1103. [Google Scholar] [CrossRef]
- Temple, N.J.; Gladwin, K.K. Fruit, vegetables, and the prevention of cancer: Research challenges. Nutrition 2003, 19, 467–470. [Google Scholar] [CrossRef]
- Hernán, M.A.; Hernández-Díaz, S.; Robins, J.M. A structural approach to selection bias. Epidemiology 2004, 15, 615–625. [Google Scholar] [CrossRef] [PubMed]
- Cadeau, C.; Fournier, A.; Mesrine, S.; Clavel-Chapelon, F.; Fagherazzi, G.; Boutron-Ruault, M.C. Vitamin C supplement intake and postmenopausal breast cancer risk: Interaction with dietary vitamin C. Am. J. Clin. Nutr. 2016, 104, 228–234. [Google Scholar] [CrossRef]
- Dorjgochoo, T.; Shrubsole, M.J.; Shu, X.O.; Lu, W.; Ruan, Z.; Zheng, Y.; Cai, H.; Dai, Q.; Gu, K.; Gao, Y.T.; et al. Vitamin supplement use and risk for breast cancer: The Shanghai breast cancer study. Breast Cancer Res. Treat. 2008, 111, 269–278. [Google Scholar] [CrossRef]
- Nagel, G.; Linseisen, J.; Van Gils, C.H.; Peeters, P.H.; Boutron-Ruault, M.C.; Clavel-Chapelon, F.; Romieu, I.; Tjønneland, A.; Olsen, A.; Roswall, N.; et al. Dietary β-carotene, vitamin C and e intake and breast cancer risk in the European Prospective Investigation into Cancer and Nutrition (EPIC). Breast Cancer Res. Treat. 2010, 119, 753–765. [Google Scholar] [CrossRef]
- Michels, K.B.; Holmberg, L.; Bergkvist, L.; Ljung, H.; Bruce, K.; Wolk, A. Dietary antioxidant vitamins, retinol, and breast cancer incidence in a cohort of Swedish women. Int. J. Cancer 2001, 91, 563–567. [Google Scholar] [CrossRef]
- Pantavos, A.; Ruiter, R.; Feskens, E.F.; De Keyser, C.E.; Hofman, A.; Stricker, B.H.; Franco, O.H.; Kiefte-De Jong, J.C. Total dietary antioxidant capacity, individual antioxidant intake and breast cancer risk: The Rotterdam study. Int. J. Cancer 2015, 136, 2178–2186. [Google Scholar] [CrossRef]
- Pan, S.Y.; Zhou, J.; Gibbons, L.; Morrison, H.; Wen, S.W. Antioxidants and breast cancer risk- a population-based case-control study in Canada. BMC Cancer 2011, 11, 1–12. [Google Scholar] [CrossRef]
- Spanish Federation of Nutrition, Food and Dietetetic Associations (FESNAD). Ingestas dietéticas de referen-cia (IDR) para la población española [recommended dietary allowances for spanish population]. Act Diet. 2010, 14, 196–197. [Google Scholar]
- Olza, J.; Aranceta-Bartrina, J.; González-Gross, M.; Ortega, R.; Serra-Majem, L.; Varela-Moreiras, G.; Gil, Á. Reported dietary intake and food sources of zinc, selenium, and vitamins a, e and c in the spanish population: Findings from the ANIBES study. Nutrients 2017, 9, 697. [Google Scholar] [CrossRef]
- Baratta, M.; Miretti, S.; Macchi, E.; Accornero, P.; Martignani, E. Mammary stem cells in domestic animals: The role of ROS. Antioxidants 2018, 8, 6. [Google Scholar] [CrossRef] [PubMed]
- Nimse, S.B.; Pal, D. Free radicals, natural antioxidants, and their reaction mechanisms. RSC Adv. 2015, 5, 27986–28006. [Google Scholar] [CrossRef]
- Altucci, L.; Gronemeyer, H. The promise of retinoids to fight against cancer. Nat. Rev. Cancer 2001, 1, 181–193. [Google Scholar] [CrossRef] [PubMed]
- Ho, E. Zinc deficiency, DNA damage and cancer risk. J. Nutr. Biochem. 2004, 15, 572–578. [Google Scholar] [CrossRef]
- Jackson, M.I.; Combs, G.F. Selenium and anticarcinogenesis: Underlying mechanisms. Curr. Opin. Clin. Nutr. Metab. Care 2008, 11, 718–726. [Google Scholar] [CrossRef] [PubMed]
- Ullah, M.F.; Khan, H.Y.; Zubair, H.; Shamim, U.; Hadi, S.M. The antioxidant ascorbic acid mobilizes nuclear copper leading to a prooxidant breakage of cellular DNA: Implications for chemotherapeutic action against cancer. Cancer Chemother. Pharmacol. 2011, 67, 103–110. [Google Scholar] [CrossRef]
- Aggarwal, B.B.; Sundaram, C.; Prasad, S.; Kannappan, R. Tocotrienols, the vitamin E of the 21st century: Its potential against cancer and other chronic diseases. Biochem. Pharmacol. 2010, 80, 1613–1631. [Google Scholar] [CrossRef]
- Yang, C.S.; Luo, P.; Zeng, Z.; Wang, H.; Malafa, M.; Suh, N. Vitamin E and cancer prevention: Studies with different forms of tocopherols and tocotrienols. Mol. Carcinog. 2020, 59, 365–389. [Google Scholar] [CrossRef] [PubMed]
- Miquel, J.; Ramírez-Boscá, A.; Ramírez-Bosca, J.V.; Alperi, J.D. Menopause: A review on the role of oxygen stress and favorable effects of dietary antioxidants. Arch. Gerontol. Geriatr. 2006, 42, 289–306. [Google Scholar] [CrossRef]
- Wang, Z.; Chandrasena, E.R.; Yuan, Y.; Peng, K.W.; Van Breemen, R.B.; Thatcher, G.R.J.; Bolton, J.L. Redox cycling of catechol estrogens generating apurinic/apyrimidinic sites and 8-oxo-deoxyguanosine via reactive oxygen species differentiates equine and human estrogens. Chem. Res. Toxicol. 2010, 23, 1365–1373. [Google Scholar] [CrossRef]
- Agarwal, A.; Doshi, S. The role of oxidative stress in menopause. J. Midlife Health 2013, 4, 140. [Google Scholar] [CrossRef]
- Cilla, A.; Bosch, L.; Barberá, R.; Alegría, A. Effect of processing on the bioaccessibility of bioactive compounds–A review focusing on carotenoids, minerals, ascorbic acid, tocopherols and polyphenols. J. Food Compos. Anal. 2018, 68, 3–15. [Google Scholar] [CrossRef]
- Guillén, S.; Mir-Bel, J.; Oria, R.; Salvador, M.L. Influence of cooking conditions on organoleptic and health-related properties of artichokes, green beans, broccoli and carrots. Food Chem. 2017, 217, 209–216. [Google Scholar] [CrossRef]
- Kalt, W. Effects of production and processing factors on major fruit and vegetable antioxidants. J. Food Sci. 2005, 70, R11–R19. [Google Scholar] [CrossRef]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Ruiz, Á.; García-Villanova, B.; Guerra-Hernández, E.; Amiano, P.; Ruiz-Canela, M.; Molina-Montes, E. A review of a priori defined oxidative balance scores relative to their components and impact on health outcomes. Nutrients 2019, 11, 774. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Total Cohort |
|---|---|
| N (frequency) | 9983 |
| Age, years | 35.1 (10.5) |
| Height, cm | 163.6 (6.0) |
| BMI, kg/m2 | 22.2 (3.0) |
| Marital status, married, n(%) | 4287 (42.9%) |
| Years of university studies | 4.8 (1.3) |
| Smoking status at baseline, n(%) | |
| Never smokers | 5153 (51.6%) |
| Current smokers | 2304 (23.1%) |
| Former smokers | 2526 (25.3%) |
| Cumulative smoking habit, packs-years | 3.4 (7.0) |
| Alcohol intake, g/d | 4.1 (5.9) |
| Coffee consumption, >1 cup/d | 4601 (46.1%) |
| Physical activity at baseline, METs-h/week | 18.4 (19.1) |
| TV-watching, h/d | 1.6 (1.2) |
| Oral contraceptive use, n(%) | 237 (2.4%) |
| Multivitamin and/or mineral users at baseline, n(%) | 2229 (22.3%) |
| Self-reported diabetes at baseline, n(%) | 102 (1.0%) |
| Diet, energy, and nutrients | |
| a Adherence to the Mediterranean diet a | 3.8 (1.7) |
| Sugar-sweetened beverage consumption, n(%) | |
| Never/seldom | 3516 (35.2%) |
| 1/month to ≤1 serving/week | 4459 (44.7%) |
| >1 servings/week | 2008 (20.1%) |
| Total energy intake, kcal/d | 2279 (571) |
| Carbohydrate intake, % E | 43.2 (7.2) |
| Protein intake, % E | 18.3 (3.2) |
| Fat intake, % E | 37.2 (6.4) |
| Saturated fatty acids, % E | 12.6 (3.1) |
| Monounsaturated fatty acids, % E | 16.1 (3.8) |
| Polyunsaturated fatty acids, % E | 5.1 (1.4) |
| Family history of breast cancer (first degree), n(%) | 1063 (10.6%) |
| Reproductive history | |
| Obstetric history | |
| Nulliparous & <25 years | 1789 (17.9%) |
| Nulliparous & ≥25 years | 4881 (48.9%) |
| First pregnancy before 25 years | 450 (4.5%) |
| First pregnancy between 25–29 years | 1461 (14.6%) |
| First pregnancy being 30 years or older | 1402 (14.0%) |
| Lifetime breastfeeding, months | 2.3 (4.9) |
| Age of menarche, n (%) | |
| ≤11 years | 2001 (20.0%) |
| 12–13 years | 5474 (54.8%) |
| 13–14 years | 1703 (17.1%) |
| ≥15 years | 805 (8.1%) |
| Menopausal status at baseline, n (%) | |
| Premenopausal | 9239 (92.5%) |
| Postmenopausal | 744 (7.5%) |
| b Age at menopause, n (%) b | |
| Postmenopausal < 50 years | 318 (42.7%) |
| Postmenopausal ≥ 50 years | 426 (57.3%) |
| b Cause of menopause, n (%) b | |
| Natural | 643 (86.4%) |
| c Induced c | 101 (13.6%) |
| b Hormone replacement therapy, n (%) b | |
| Ever-use | 446 (4.5%) |
| Duration of use, years | 1.4 (2.5) |
| Tertiles of Energy-Adjusted of Dietary Vitamin A Intake | ||||
|---|---|---|---|---|
| T1 | T2 | T3 | P for Trend | |
| Overall | ||||
| Intake range, (mcg⁄d) | <1387 | 1387–2282 | >2282 | |
| Median intake, (mcg⁄d) | 1033 | 1747 | 2984 | |
| No of participants | 3328 | 3328 | 3327 | |
| Person-years | 38,540 | 37,718 | 36,740 | |
| Cases | 36 | 31 | 40 | |
| Incidence rate/10,000 person-years | 9.34 | 821 | 10.88 | |
| Age-adjusted | 1.00 (reference) | 0.80 (0.49–1.29) | 0.96 (0.61–1.50) | 0.998 |
| Model 1 | 1.00 (reference) | 0.77 (0.48–1.26) | 0.94 (0.59–1.50) | 0.975 |
| Model 2 | 1.00 (reference) | 0.85 (0.51–1.41) | 1.07 (0.64–1.77) | 0.673 |
| Premenopausal | ||||
| Intake range, (mcg⁄d) | <1366 | 1366–2250 | >2250 | |
| Median intake, (mcg⁄d) | 1017 | 1719 | 2944 | |
| No of participants | 3077 | 3077 | 3076 | |
| Person-years | 33,149 | 32,113 | 30,580 | |
| Cases | 22 | 20 | 18 | |
| Incidence rate/10,000 person-years | 6.64 | 6.23 | 5.89 | |
| Age-adjusted | 1.00 (reference) | 0.88 (0.48–1.61) | 0.78 (0.42–1.45) | 0.434 |
| Model 1 | 1.00 (reference) | 0.88 (0.48–1.63) | 0.77 (0.40–1.46) | 0.423 |
| Model 2 | 1.00 (reference) | 0.95 (0.50–1.80) | 0.81 (0.40–1.62) | 0.537 |
| Postmenopausal | ||||
| Intake range, (mcg⁄d) | <1513 | 1513–2499 | >2499 | |
| Median intake, (mcg⁄d) | 1153 | 1924 | 3249 | |
| No of participants | 987 | 987 | 987 | |
| Person-years | 6307 | 6860 | 6844 | |
| Cases | 12 | 10 | 17 | |
| Incidence rate/10,000 person-years | 19.02 | 14.58 | 24.84 | |
| Age-adjusted | 1.00 (reference) | 0.80 (0.35–1.86) | 1.35 (0.65–2.84) | 0.311 |
| Model 1 | 1.00 (reference) | 0.72 (0.31–1.70) | 1.51 (0.70–3.23) | 0.178 |
| Model 2 | 1.00 (reference) | 0.78 (0.32–1.90) | 1.72 (0.73–4.01) | 0.127 |
| Tertiles of Energy-Adjusted of Dietary Vitamin C Intake | ||||
|---|---|---|---|---|
| T1 | T2 | T3 | P for Trend | |
| Overall | ||||
| Intake range, (mg⁄d) | <219 | 219–322 | >322 | |
| Median intake, (mg⁄d) | 168 | 265 | 406 | |
| No of participants | 3328 | 3328 | 3327 | |
| Person-years | 38,458 | 37,754 | 36,878 | |
| Cases | 39 | 28 | 40 | |
| Incidence rate/10,000 person-years | 10.14 | 7.41 | 10.87 | |
| Age-adjusted | 1.00 (reference) | 0.68 (0.42–1.10) | 0.89 (0.57–1.39) | 0.756 |
| Model 1 | 1.00 (reference) | 0.70 (0.43–1.15) | 0.92 (0.58–1.46) | 0.866 |
| Model 2 | 1.00 (reference) | 0.73 (0.43–1.22) | 1.00 (0.58–1.71) | 0.846 |
| Premenopausal | ||||
| Intake range, (mg⁄d) | <216 | 216–317 | >317 | |
| Median intake, (mg⁄d) | 167 | 262 | 401 | |
| No of participants | 3077 | 3077 | 3076 | |
| Person-years | 33,385 | 31,971 | 30,485 | |
| Cases | 23 | 18 | 19 | |
| Incidence rate/10,000 person-years | 6.89 | 5.63 | 6.23 | |
| Age-adjusted | 1.00 (reference) | 0.73 (0.44–1.22) | 0.82 (0.50–1.33) | 0.485 |
| Model 1 | 1.00 (reference) | 0.76 (0.46–1.28) | 0.87 (0.53–1.44) | 0.652 |
| Model 2 | 1.00 (reference) | 0.76 (0.44–1.31) | 0.88 (0.49–1.59) | 0.758 |
| Postmenopausal | ||||
| Intake range, (mg⁄d) | <235 | 235–348 | >348 | |
| Median intake, (mg⁄d) | 181 | 289 | 432 | |
| No of participants | 987 | 987 | 987 | |
| Person-years | 6016 | 6914 | 7081 | |
| Cases | 11 | 12 | 16 | |
| Incidence rate/10,000 person-years | 18.29 | 17.36 | 22.60 | |
| Age-adjusted | 1.00 (reference) | 0.98 (0.43–2.23) | 1.28 (0.59–2.77) | 0.485 |
| Model 1 | 1.00 (reference) | 1.00 (0.43–2.31) | 1.40 (0.63–3.12) | 0.368 |
| Model 2 | 1.00 (reference) | 1.13 (0.46–2.74) | 1.72 (0.66–4.45) | 0.234 |
| Tertiles of Energy-Adjusted of Dietary Vitamin E Intake | ||||
|---|---|---|---|---|
| T1 | T2 | T3 | P for Trend | |
| Overall | ||||
| Intake range, (mg⁄d) | <5.56 | 5.56–7.15 | >7.15 | |
| Median intake, (mg⁄d) | 4.68 | 6.30 | 8.87 | |
| No of participants | 3328 | 3328 | 3327 | |
| Person-years | 38,036 | 37,475 | 37,4788 | |
| Cases | 38 | 36 | 33 | |
| Incidence rate/10,000 person-years | 9.99 | 9.61 | 8.80 | |
| Age-adjusted | 1.00 (reference) | 0.94 (0.60–1.48) | 0.86 (0.54–1.37) | 0.525 |
| Model 1 | 1.00 (reference) | 0.94 (0.59–1.48) | 0.86 (0.54–1.38) | 0.533 |
| Model 2 | 1.00 (reference) | 1.00 (0.62–1.63) | 0.92 (0.55–1.54) | 0.728 |
| Premenopausal | ||||
| Intake range, (mg⁄d) | <5.53 | 5.53–7.13 | >7.13 | |
| Median intake, (mg⁄d) | 4.66 | 6.27 | 8.79 | |
| No of participants | 3077 | 3077 | 3076 | |
| Person-years | 32,260 | 31,894 | 31,687 | |
| Cases | 17 | 26 | 17 | |
| Incidence rate/10,000 person-years | 5.27 | 8.15 | 5.37 | |
| Age-adjusted | 1.00 (reference) | 1.00 (0.61–1.64) | 0.93 (0.56–1.55) | 0.779 |
| Model 1 | 1.00 (reference) | 0.99 (0.60–1.62) | 0.95 (0.57–1.58) | 0.832 |
| Model 2 | 1.00 (reference) | 1.05 (0.62–1.79) | 1.03 (0.59–1.81) | 0.924 |
| Postmenopausal | ||||
| Intake range, (mg⁄d) | <5.63 | 5.63–7.27 | >7.27 | |
| Median intake, (mg⁄d) | 4.74 | 6.41 | 9.10 | |
| No of participants | 987 | 987 | 987 | |
| Person-years | 6592 | 6568 | 6850 | |
| Cases | 20 | 10 | 9 | |
| Incidence rate/10,000 person-years | 30.33 | 15.22 | 13.14 | |
| Age-adjusted | 1.00 (reference) | 0.50 (0.24–1.08) | 0.44 (0.20–0.96) | 0.042 |
| Model 1 | 1.00 (reference) | 0.47 (0.22–1.01) | 0.40 (0.18–0.90) | 0.028 |
| Model 2 | 1.00 (reference) | 0.45 (0.20–1.04) | 0.35 (0.14–0.86) | 0.027 |
| Tertiles of Energy-Adjusted of Dietary Selenium Intake | ||||
|---|---|---|---|---|
| T1 | T2 | T3 | P for Trend | |
| Overall | ||||
| Intake range, (mcg⁄d) | <80.9 | 80.9–101.1 | >101.1 | |
| Median intake, (mcg⁄d) | 69.0 | 90.5 | 114.5 | |
| No of participants | 3328 | 3328 | 3327 | |
| Person-years | 37,884 | 37,563 | 37,553 | |
| Cases | 32 | 26 | 49 | |
| Incidence rate/10,000 person-years | 8.44 | 6.92 | 13.05 | |
| Age-adjusted | 1.00 (reference) | 0.74 (0.44–1.25) | 1.26 (0.81–1.97) | 0.215 |
| Model 1 | 1.00 (reference) | 0.73 (0.43–1.23) | 1.27 (0.81–1.99) | 0.209 |
| Model 2 | 1.00 (reference) | 0.76 (0.45–1.29) | 1.37 (0.85–2.20) | 0.135 |
| Premenopausal | ||||
| Intake range, (mcg⁄d) | <80.4 | 80.4–100.3 | >100.3 | |
| Median intake, (mcg⁄d) | 68.6 | 90.1 | 113.8 | |
| No of participants | 3077 | 3077 | 3076 | |
| Person-years | 32,766 | 31,929 | 31,147 | |
| Cases | 19 | 17 | 24 | |
| Incidence rate/10,000 person-years | 5.80 | 5.32 | 7.71 | |
| Age-adjusted | 1.00 (reference) | 0.67 (0.38–1.17) | 1.18 (0.73–1.90) | 0.379 |
| Model 1 | 1.00 (reference) | 0.64 (0.36–1.13) | 1.24 (0.77–2.01) | 0.268 |
| Model 2 | 1.00 (reference) | 0.65 (0.37–1.16) | 1.29 (0.78–2.14) | 0.226 |
| Postmenopausal | ||||
| Intake range, (mcg⁄d) | < 84.5 | 84.5–105.2 | > 105.2 | |
| Median intake, (mcg⁄d) | 72.7 | 93.8 | 118.2 | |
| No of participants | 987 | 987 | 987 | |
| Person-years | 6360 | 6663 | 6988 | |
| Cases | 11 | 8 | 20 | |
| Incidence rate/10,000 person-years | 17.30 | 12.01 | 28.62 | |
| Age-adjusted | 1.00 (reference) | 0.69 (0.28–1.71) | 1.68 (0.80–3.51) | 0.106 |
| Model 1 | 1.00 (reference) | 0.64 (0.25–1.61) | 1.65 (0.78–3.48) | 0.115 |
| Model 2 | 1.00 (reference) | 0.68 (0.27–1.75) | 1.70 (0.77–3.75) | 0.118 |
| Tertiles of Energy-Adjusted of Dietary Zinc Intake | ||||
|---|---|---|---|---|
| T1 | T2 | T3 | P for Trend | |
| Overall | ||||
| Intake range, (mg⁄d) | <12.8 | 12.8–17.2 | >17.2 | |
| Median intake, (mg⁄d) | 11.5 | 14.2 | 22.9 | |
| No of participants | 3328 | 3328 | 3327 | |
| Person-years | 39,115 | 37,831 | 36,053 | |
| Cases | 38 | 35 | 34 | |
| Incidence rate/10,000 person-years | 9.72 | 9.25 | 9.43 | |
| Age-adjusted | 1.00 (reference) | 0.92 (0.58–1.45) | 0.92 (0.58–1.46) | 0.770 |
| Model 1 | 1.00 (reference) | 0.93 (0.59–1.48) | 0.93 (0.58–1.50) | 0.815 |
| Model 2 | 1.00 (reference) | 0.98 (0.61–1.58) | 1.01 (0.61–1.69) | 0.939 |
| Premenopausal | ||||
| Intake range, (mg⁄d) | <12.8 | 12.8–17.0 | >17.0 | |
| Median intake, (mg⁄d) | 11.5 | 14.1 | 22.6 | |
| No of participants | 3077 | 3077 | 3076 | |
| Person-years | 33,391 | 31,851 | 30,600 | |
| Cases | 19 | 21 | 20 | |
| Incidence rate/10,000 person-years | 5.69 | 6.59 | 6.54 | |
| Age-adjusted | 1.00 (reference) | 0.95 (0.57–1.57) | 1.06 (0.65–1.75) | 0.729 |
| Model 1 | 1.00 (reference) | 0.99 (0.59–1.65) | 1.16 (0.69–1.93) | 0.521 |
| Model 2 | 1.00 (reference) | 1.04 (0.62–1.76) | 1.26 (0.73–2.19) | 0.367 |
| Postmenopausal | ||||
| Intake range, (mg⁄d) | <12.9 | 12.9–17.6 | >17.6 | |
| Median intake, (mg⁄d) | 11.6 | 14.3 | 24.7 | |
| No of participants | 987 | 987 | 987 | |
| Person-years | 6406 | 6618 | 6987 | |
| Cases | 14 | 12 | 13 | |
| Incidence rate/10,000 person-years | 21.85 | 18.13 | 18.61 | |
| Age-adjusted | 1.00 (reference) | 0.84 (0.39–1.83) | 0.85 (0.40–1.82) | 0.761 |
| Model 1 | 1.00 (reference) | 0.84 (0.39–1.84) | 0.82 (0.37–1.78) | 0.680 |
| Model 2 | 1.00 (reference) | 0.89 (0.40–1.99) | 0.89 (0.38–2.07) | 0.840 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernandez-Lazaro, C.I.; Martínez-González, M.Á.; Aguilera-Buenosvinos, I.; Gea, A.; Ruiz-Canela, M.; Romanos-Nanclares, A.; Toledo, E. Dietary Antioxidant Vitamins and Minerals and Breast Cancer Risk: Prospective Results from the SUN Cohort. Antioxidants 2021, 10, 340. https://doi.org/10.3390/antiox10030340
Fernandez-Lazaro CI, Martínez-González MÁ, Aguilera-Buenosvinos I, Gea A, Ruiz-Canela M, Romanos-Nanclares A, Toledo E. Dietary Antioxidant Vitamins and Minerals and Breast Cancer Risk: Prospective Results from the SUN Cohort. Antioxidants. 2021; 10(3):340. https://doi.org/10.3390/antiox10030340
Chicago/Turabian StyleFernandez-Lazaro, Cesar I., Miguel Ángel Martínez-González, Inmaculada Aguilera-Buenosvinos, Alfredo Gea, Miguel Ruiz-Canela, Andrea Romanos-Nanclares, and Estefanía Toledo. 2021. "Dietary Antioxidant Vitamins and Minerals and Breast Cancer Risk: Prospective Results from the SUN Cohort" Antioxidants 10, no. 3: 340. https://doi.org/10.3390/antiox10030340
APA StyleFernandez-Lazaro, C. I., Martínez-González, M. Á., Aguilera-Buenosvinos, I., Gea, A., Ruiz-Canela, M., Romanos-Nanclares, A., & Toledo, E. (2021). Dietary Antioxidant Vitamins and Minerals and Breast Cancer Risk: Prospective Results from the SUN Cohort. Antioxidants, 10(3), 340. https://doi.org/10.3390/antiox10030340