
Technical Aspects of Coenzyme Q10 Analysis: Validation of a New HPLC-ED Method

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Samples
2.2. Method
2.3. Validation Procedure
2.4. LC-MS/MS Method
2.5. Statistical Analyses
3. Results
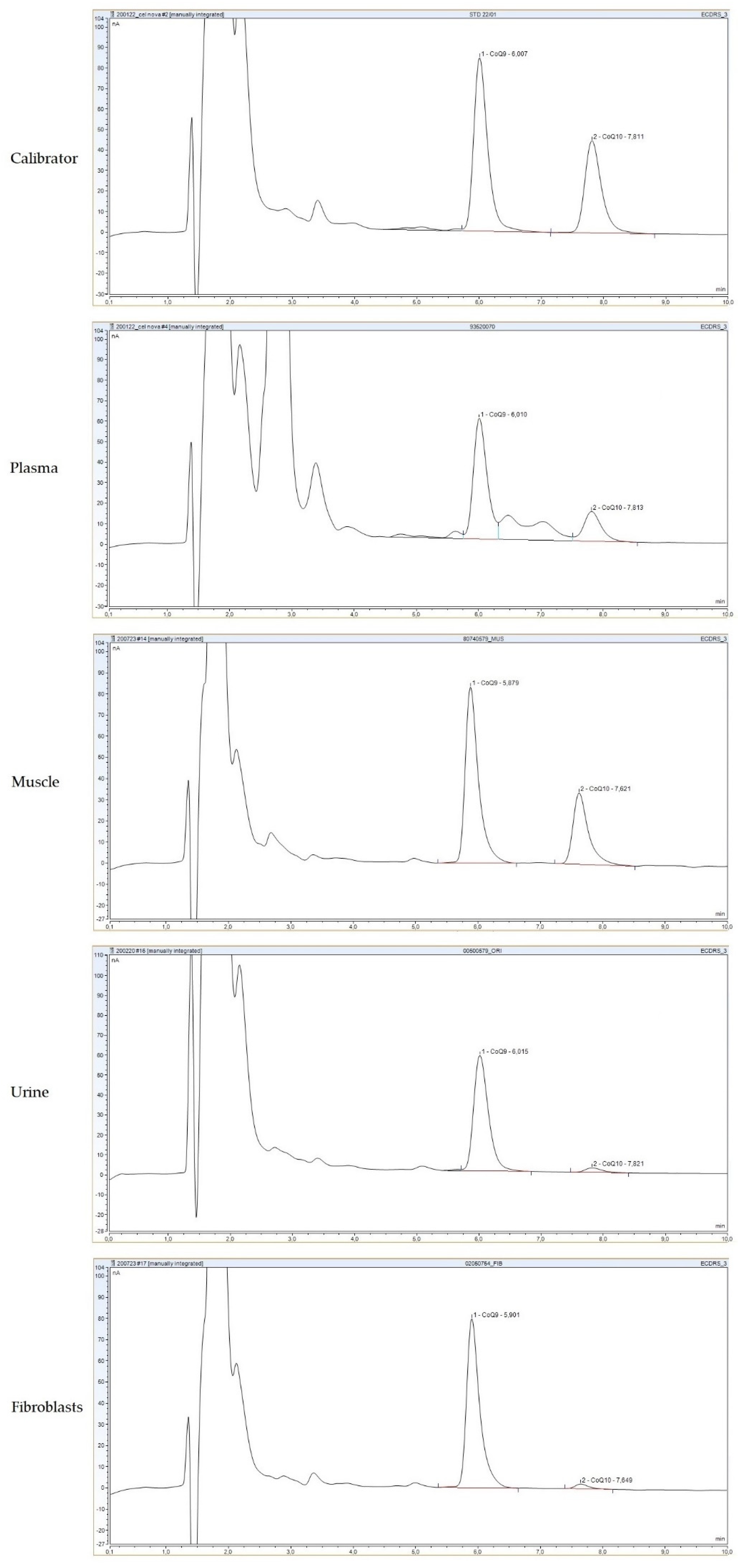
3.1. Optimization of the Method and Performance in Different Biological Samples
3.2. Analytical Validation of the Method and EQC Scheme Results
3.3. Method Comparison
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Turunen, M.; Olsson, J.; Dallner, G. Metabolism and function of coenzyme Q. Biochim. Biophys. Acta 2004, 1660, 171–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trevisson, E.; Dimauro, S.; Navas, P.; Salviati, L. Coenzyme Q deficiency in muscle. Curr. Opin. Neurol. 2011, 24, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Quinzii, C.M.; Hirano, M. Primary and secondary CoQ10 deficiencies in humans. BioFactors 2011, 37, 361–365. [Google Scholar] [CrossRef]
- Emmanuele, V.; López, L.C.; Berardo, A.; Naini, A.; Tadesse, S.; Wen, B.; D’Agostino, E.; Solomon, M.; DiMauro, S.; Quinzii, C.; et al. Heterogeneity of coenzyme Q10 deficiency: Patient study and literature review. Arch. Neurol. 2012, 69, 978–983. [Google Scholar] [CrossRef] [Green Version]
- Alcázar-Fabra, M.; Trevisson, E.; Brea-Calvo, G. Clinical syndromes associated with coenzyme Q10 deficiency. Essays Biochem. 2018, 62, 377–398. [Google Scholar] [CrossRef]
- Desbats, M.A.; Lunardi, G.; Doimo, M.; Trevisson, E.; Salviati, L. Genetic bases and clinical manifestations of coenzyme Q10 (CoQ10) deficiency. J. Inherit. Metab. Dis. 2014, 38, 145–156. [Google Scholar] [CrossRef]
- Hargreaves, I.; Heaton, R.A.; Mantle, D. Disorders of Human Coenzyme Q10 Metabolism: An Overview. Int. J. Mol. Sci. 2020, 21, 6695. [Google Scholar] [CrossRef]
- Abe, K.; Ishibashi, K.; Ohmae, M.; Kawabe, K.; Katsui, G. Determination of ubiquinone in serum and liver by high-speed liquid chromatography. J. Nutr. Sci. Vitaminol. 1978, 24, 555–567. [Google Scholar] [CrossRef] [Green Version]
- Ogasahara, S.; Engel, A.G.; Frens, D.; Mack, D. Muscle coenzyme Q deficiency in familial mitochondrial encephalomyopathy. Proc. Natl. Acad. Sci. USA 1989, 86, 2379–2382. [Google Scholar] [CrossRef] [Green Version]
- Okamoto, T.; Fukunaga, Y.; Ida, Y.; Kishi, T. Determination of reduced and total ubiquinones in biological materials by liquid chromatography with electrochemical detection. J. Chromatogr. 1988, 430, 11–19. [Google Scholar] [CrossRef]
- Grossi, G.; Bargossi, A.M.; Fiorella, P.L.; Piazzi, S.; Battino, M.; Bianchi, G.P. Improved high-performance liquid chromatographic method for the determination of coenzyme Q10 in plasma. J. Chromatogr. 1992, 593, 217–226. [Google Scholar] [CrossRef]
- Barshop, B.A.; Gangoiti, J.A. Analysis of coenzyme Q in human blood and tissues. Mitochondrion 2007, 7, S89–S93. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.F.; Franke, A.A. Analysis of circulating lipid-phase micronutrients in humans by HPLC: Review and overview of new developments. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2013, 931, 23–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, G.; Christensen, P.; Tüchsen, E.; Lund, T. Sensitive and selective analysis of coenzyme Q10 in human serum by negative APCI LC-MS. Analyst 2004, 129, 45–50. [Google Scholar] [CrossRef]
- Ruiz-Jiménez, J.; Priego-Capote, F.; Mata-Granados, J.M.; Quesada, J.M.; Luque de Castro, M.D. Determination of the ubiquinol-10 and ubiquinone-10 (coenzyme Q10) in human serum by liquid chromatography tandem mass spectrometry to evaluate the oxidative stress. J. Chromatogr. A 2007, 1175, 242–248. [Google Scholar] [CrossRef]
- Turkowicz, M.J.; Karpińska, J. Analytical problems with the determination of coenzyme Q10 in biological samples. Biofactors 2013, 39, 176–185. [Google Scholar] [CrossRef]
- Kishikawa, N.; Kuroda, N. Analytical techniques for the determination of biologically active quinones in biological and environmental samples. J. Pharm. Biomed. Anal. 2014, 87, 261–270. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Aguilera, J.; Cortés, A.; Fernández-Ayala, D.; Navas, P. Biochemical assessment of coenzyme Q10 deficiency. J. Clin. Med. 2017, 6, 27. [Google Scholar] [CrossRef] [Green Version]
- Yubero, D.; Montero, R.; Ramos, M.; Neergheen, V.; Navas, P.; Artuch, R.; Hargreaves, I. Determination of urinary coenzyme Q10 by HPLC with electrochemical detection: Reference values for a paediatric population. BioFactors 2015, 41, 424–430. [Google Scholar] [CrossRef]
- Montero, R.; Sánchez-Alcázar, J.A.; Briones, P.; Hernández, Á.R.; Cordero, M.D.; Trevisson, E.; Salviati, L.; Pineda, M.; García-Cazorla, A.; Navas, P.; et al. Analysis of coenzyme Q10 in muscle and fibroblasts for the diagnosis of CoQ10 deficiency syndromes. Clin. Biochem. 2008, 41, 697–700. [Google Scholar] [CrossRef]
- Lowry, O.H.; Rosebrough, N.J.; Farr, A.L.; Randall, R.J. Protein measurement with the Folin phenol reagent. J. Biol. Chem. 1951, 193, 265–275. [Google Scholar] [CrossRef]
- Fowler, B.; Burlina, A.; Kozich, V.; Vianey-Saban, C. Quality of analytical performance in inherited metabolic disorders: The role of ERNDIM. J. Inherit. Metab. Dis. 2008, 31, 680–689. [Google Scholar] [CrossRef] [PubMed]
- Bravo-Alonso, I.; Navarrete, R.; Vega, A.I.; Ruíz-Sala, P.; Silva, M.T.G.; Martín-Hernández, E.; Quijada-Fraile, P.; Belanger-Quintana, A.; Stanescu, S.; Bueno, M.; et al. Genes and Variants Underlying Human Congenital Lactic Acidosis-From Genetics to Personalized Treatment. J. Clin. Med. 2019, 8, 1811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paredes-Fuentes, A.J.; Montero, R.; Codina, A.; Jou, C.; Fernández, G.; Maynou, J.; Santos-Ocaña, C.; Riera, J.; Navas, P.; Drobnic, F.; et al. Coenzyme Q 10 Treatment Monitoring in Different Human Biological Samples. Antioxidants 2020, 9, 979. [Google Scholar] [CrossRef] [PubMed]
- Molyneux, S.L.; Florkowski, C.M.; Lever, M.; George, P.M. Biological variation of coenzyme Q10. Clin. Chem. 2005, 51, 455–457. [Google Scholar] [CrossRef] [Green Version]
- Miles, L.; Miles, M.V.; Tang, P.H.; Horn, P.S.; Wong, B.L.; DeGrauw, T.J.; Morehart, P.J.; Bove, K.E. Muscle coenzyme Q: A potential test for mitochondrial activity and redox status. Pediatr. Neurol. 2005, 32, 318–324. [Google Scholar] [CrossRef]
- Duncan, A.J.; Bitner-Glindzicz, M.; Meunier, B.; Costello, H.; Hargreaves, I.P.; López, L.C.; Hirano, M.; Quinzii, C.M.; Sadowski, M.I.; Hardy, J.; et al. A Nonsense Mutation in COQ9 Causes Autosomal-Recessive Neonatal-Onset Primary Coenzyme Q10 Deficiency: A Potentially Treatable Form of Mitochondrial Disease. Am. J. Hum. Genet. 2009, 84, 558. [Google Scholar] [CrossRef] [Green Version]
- Barca, E.; Musumeci, O.; Montagnese, F.; Marino, S.; Granata, F.; Nunnari, D.; Peverelli, L.; DiMauro, S.; Quinzii, C.M.; Toscano, A. Cerebellar ataxia and severe muscle CoQ10 deficiency in a patient with a novel mutation in ADCK3. Clin. Genet. 2016, 90, 156–160. [Google Scholar] [CrossRef] [Green Version]
- Arias, A.; García-Villoria, J.; Rojo, A.; Buján, N.; Briones, P.; Ribes, A. Analysis of coenzyme Q10 in lymphocytes by HPLC-MS/MS. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2012, 908, 23–26. [Google Scholar] [CrossRef]
- Colomé, C.; Artuch, R.; Vilaseca, M.A.; Sierra, C.; Brandi, N.; Lambruschini, N.; Cambra, F.J.; Campistol, J. Lipophilic antioxidants in patients with phenylketonuria. Am. J. Clin. Nutr. 2003, 77, 185–188. [Google Scholar] [CrossRef] [Green Version]
- Lee, B.L.; Ong, C.N. Comprehensive high-performance liquid chromatographic method for the measurements of lipophilic antioxidants in human plasma. J. Chromatogr. A 2009, 1216, 3131–3137. [Google Scholar] [CrossRef] [PubMed]
- Schou-Pedersen, A.M.V.; Schemeth, D.; Lykkesfeldt, J. Determination of Reduced and Oxidized Coenzyme Q 10 in Canine Plasma and Heart Tissue by HPLC-ECD: Comparison with LC-MS/MS Quantification. Antioxidants 2019, 8, 253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, J.; Bi, J.; Johnson, D.; Sun, Y.; Song, M.; Qiu, P.; Dong, P.; Decker, E.; Xiao, H. Analysis of 10 metabolites of polymethoxyflavones with high sensitivity by electrochemical detection in high-performance liquid chromatography. J. Agric. Food Chem. 2015, 63, 509–516. [Google Scholar] [CrossRef] [PubMed]
- García, M.C. The effect of the mobile phase additives on sensitivity in the analysis of peptides and proteins by high-performance liquid chromatography-electrospray mass spectrometry. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2005, 825, 111–123. [Google Scholar] [CrossRef] [PubMed]
- Kotani, A.; Yuan, Y.; Yang, B.; Hayashi, Y.; Matsuda, R.; Kusu, F. Selection of the optimal solvent grade for the mobile phase in HPLC with electrochemical detection based on FUMI theory. Anal. Sci. Int. J. Jpn. Soc. Anal. Chem. 2009, 25, 925–929. [Google Scholar] [CrossRef] [Green Version]
- Paredes-Fuentes, A.J.; Julià-Palacios, N.A.; Montero, R.; Yubero, D.; Cascajo-Almenara, M.V.; García-Cazorla, À.; Santos-Ocaña, C.; Artuch, R. Laboratory Diagnosis of a Case with Coenzyme Q10 Deficiency. Clin. Chem. 2020, 66, 1465–1467. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Validation Parameters | |
|---|---|
| Intra-assay precision (%) | |
| 0.3 µmol/L | 6.48 |
| 1 µmol/L | 6.10 |
| Inter-assay precision (%) | |
| 0.74 µmol/L | 8.85 |
| Linearity (µmol/L) | 0.06–7.07 |
| r2 | 0.999 |
| AMR (µmol/L) | 0.12–5.60 |
| LOQ (µmol/L) | 0.06 |
| LOD (µmol/L) | 0.02 |
| Accuracy | 100.6 (6.62) |
| 2020 (n = 11) | 2021 (n = 13) | |
|---|---|---|
| Mean values detected (µmol/L) | 0.757 | 0.901 |
| Precision (CV of the duplicates, %) | 52.7 | 50.5 |
| Linearity (r) | 0.782 | 0.664 |
| Recovery (% of added CoQ) | 27 | 26 |
| Interlaboratory CV (%) | 141 | 82.2 |
| Duplicate | Lab 1 (HPLC-ED) | Lab 2 (LC-MS/MS) | All Participants | |
|---|---|---|---|---|
| SAS2020.01 | 1 | 1.4 | 0.41 | 1.2 |
| SAS2020.02 | 2 | 0.41 | 0.43 | 0.43 |
| SAS2020.03 | 3 | 0.22 | 0.36 | 0.34 |
| SAS2020.04 | 4 | 1.1 | 1.9 | 1.1 |
| SAS2020.05 | 4 | 1.9 | 2.2 | 2.0 |
| SAS2020.06 | 3 | 0.18 | 0.33 | 0.32 |
| SAS2020.07 | 1 | 1.2 | 1.5 | 1.2 |
| SAS2020.08 | 2 | 0.49 | 0.61 | 0.54 |
| SAS2021.01 | 1 | 0.21 | 0.32 | 0.27 |
| SAS2021.02 | 2 | 0.69 | 0.62 | 0.69 |
| SAS2021.03 | 3 | 0.59 | 0.94 | 0.92 |
| SAS2021.04 | 4 | 0.60 | 0.67 | 0.57 |
| SAS2021.05 | 1 | 0.14 | 0.30 | 0.27 |
| SAS2021.06 | 3 | NR | 0.97 | 1.2 |
| SAS2021.07 | 2 | 1.7 | 1.9 | 1.5 |
| SAS2021.08 | 4 | 0.51 | 0.53 | 0.53 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paredes-Fuentes, A.J.; Oliva, C.; Montero, R.; Alcaide, P.; Ruijter, G.J.G.; García-Villoria, J.; Ruiz-Sala, P.; Artuch, R. Technical Aspects of Coenzyme Q10 Analysis: Validation of a New HPLC-ED Method. Antioxidants 2022, 11, 528. https://doi.org/10.3390/antiox11030528
Paredes-Fuentes AJ, Oliva C, Montero R, Alcaide P, Ruijter GJG, García-Villoria J, Ruiz-Sala P, Artuch R. Technical Aspects of Coenzyme Q10 Analysis: Validation of a New HPLC-ED Method. Antioxidants. 2022; 11(3):528. https://doi.org/10.3390/antiox11030528
Chicago/Turabian StyleParedes-Fuentes, Abraham J., Clara Oliva, Raquel Montero, Patricia Alcaide, George J. G. Ruijter, Judit García-Villoria, Pedro Ruiz-Sala, and Rafael Artuch. 2022. "Technical Aspects of Coenzyme Q10 Analysis: Validation of a New HPLC-ED Method" Antioxidants 11, no. 3: 528. https://doi.org/10.3390/antiox11030528
APA StyleParedes-Fuentes, A. J., Oliva, C., Montero, R., Alcaide, P., Ruijter, G. J. G., García-Villoria, J., Ruiz-Sala, P., & Artuch, R. (2022). Technical Aspects of Coenzyme Q10 Analysis: Validation of a New HPLC-ED Method. Antioxidants, 11(3), 528. https://doi.org/10.3390/antiox11030528