

Systemic Health Effects of Oleuropein and Hydroxytyrosol Supplementation: A Systematic Review of Randomized Controlled Trials
 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Quality Assessment
3. Results
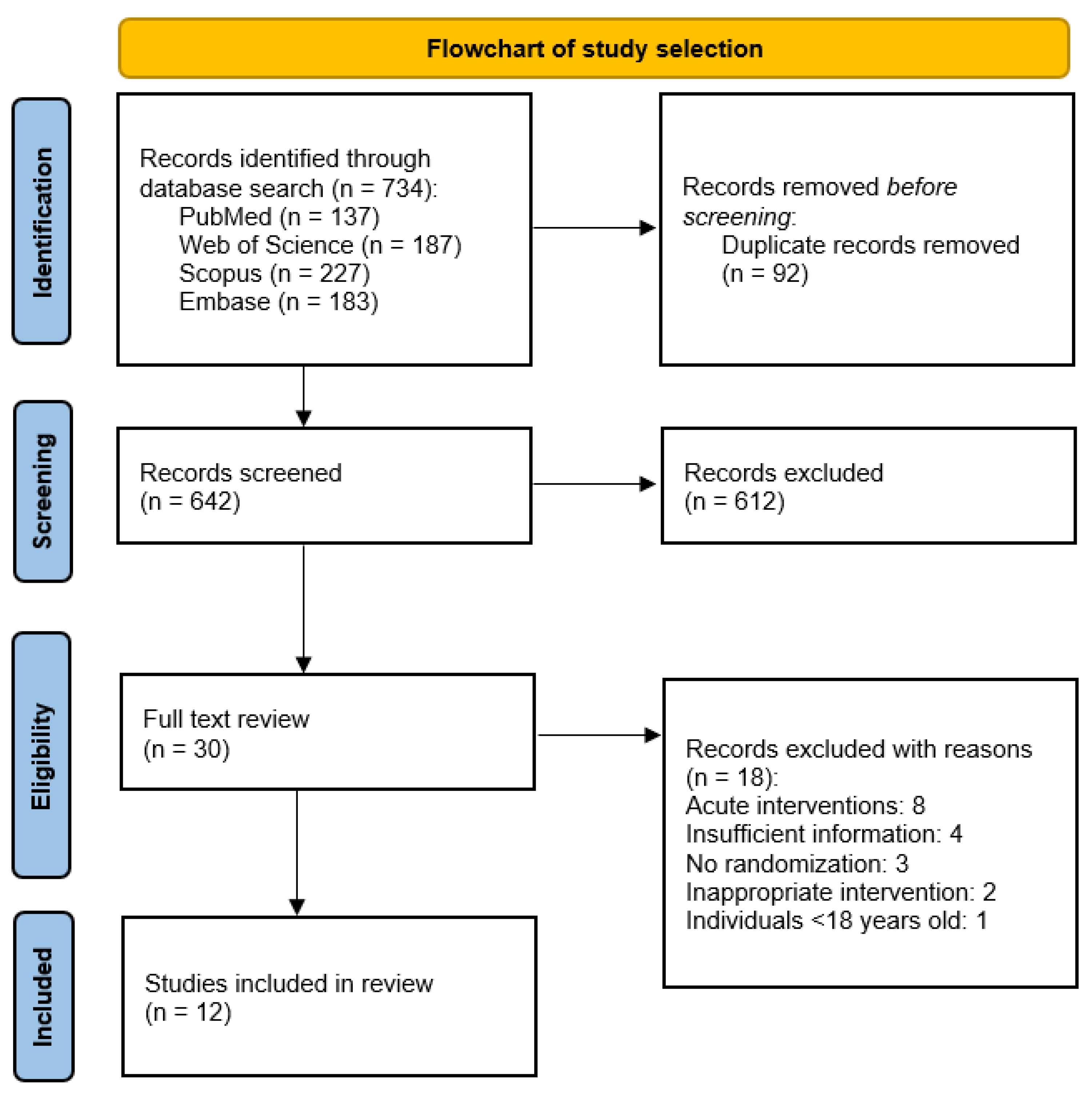
3.1. Literature Search and Data Extraction
3.2. Outcomes
3.3. Risk of Bias Assessment
4. Discussion
4.1. Cardiovascular Disease Risk Factors
4.1.1. Effects of OLE and HT Supplementation on Anthropometric Parameters
4.1.2. Effects of OLE and HT Supplementation on Lipid Levels
4.1.3. Effects of OLE and HT Supplementation on Glycemic Parameters
4.1.4. Effects of OLE and HT Supplementation on Blood Pressure
4.1.5. Effects of OLE and HT Supplementation on Inflammatory and Oxidative Markers
4.2. Liver Function
4.3. Bone and Joint Health
4.4. Cognitive Health
5. Limitations and Future Perspectives
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Noncommunicable Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 28 May 2024).
- WHO. Cardiovascular Diseases (CVDs). Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 28 May 2024).
- Bays, H.E.; Taub, P.R.; Epstein, E.; Michos, E.D.; Ferraro, R.A.; Bailey, A.L.; Kelli, H.M.; Ferdinand, K.C.; Echols, M.R.; Weintraub, H.; et al. Ten things to know about ten cardiovascular disease risk factors. Am. J. Prev. Cardiol. 2021, 5, 100149. [Google Scholar] [CrossRef] [PubMed]
- Cespedes, E.M.; Hu, F.B. Dietary patterns: From nutritional epidemiologic analysis to national guidelines. Am. J. Clin. Nutr. 2015, 101, 899–900. [Google Scholar] [CrossRef]
- Widmer, R.J.; Flammer, A.J.; Lerman, L.O.; Lerman, A. The Mediterranean diet, its components, and cardiovascular disease. Am. J. Med. 2015, 128, 229–238. [Google Scholar] [CrossRef]
- Grosso, G.; Marventano, S.; Yang, J.; Micek, A.; Pajak, A.; Scalfi, L.; Galvano, F.; Kales, S.N. A comprehensive meta-analysis on evidence of Mediterranean diet and cardiovascular disease: Are individual components equal? Crit. Rev. Food Sci. Nutr. 2017, 57, 3218–3232. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; Gea, A.; Ruiz-Canela, M. The Mediterranean diet and cardiovascular health: A critical review. Circ. Res. 2019, 124, 779–798. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; Dominguez, L.J.; Delgado-Rodríguez, M. Olive oil consumption and risk of CHD and/or stroke: A meta-analysis of case-control, cohort and intervention studies. Br. J. Nutr. 2014, 112, 248–259. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; Sayón-Orea, C.; Bullón-Vela, V.; Bes-Rastrollo, M.; Rodríguez-Artalejo, F.; Yusta-Boyo, M.J.; García-Solano, M. Effect of olive oil consumption on cardiovascular disease, cancer, type 2 diabetes, and all-cause mortality: A systematic review and meta-analysis. Clin. Nutr. 2022, 41, 2659–2682. [Google Scholar] [CrossRef]
- Tuck, K.L.; Hayball, P.J. Major phenolic compounds in olive oil: Metabolism and health effects. J. Nutr. Biochem. 2002, 13, 636–644. [Google Scholar] [CrossRef]
- Romani, A.; Ieri, F.; Urciuoli, S.; Noce, A.; Marrone, G.; Nediani, C.; Bernini, R. Health effects of phenolic compounds found in extra-virgin olive oil, by-products, and leaf of Olea europaea L. Nutrients 2019, 11, 1776. [Google Scholar] [CrossRef]
- Markhali, F.S.; Teixeira, J.A. Extractability of oleuropein, hydroxytyrosol, tyrosol, verbascoside and flavonoid-derivatives from olive leaves using ohmic heating (a green process for value addition). Sustain. Food Technol. 2024, 2, 461–469. [Google Scholar] [CrossRef]
- Termentzi, A.; Halabalaki, M.; Skaltsounis, A.L. From drupes to olive oil: An exploration of olive key metabolites. In Olive and Olive Oil Bioactive Constituents; AOCS Press: Urbana, IL, USA, 2015; pp. 147–177. ISBN 9781630670429. [Google Scholar]
- CBI. The European Market Potential for Table Olives. Available online: https://www.cbi.eu/market-information/processed-fruit-vegetables-edible-nuts/table-olives/market-potential (accessed on 2 June 2024).
- Silvestrini, A.; Giordani, C.; Bonacci, S.; Giuliani, A.; Ramini, D.; Matacchione, G.; Sabbatinelli, J.; Di Valerio, S.; Pacetti, D.; Procopio, A.D.; et al. Anti-inflammatory effects of olive leaf extract and its bioactive compounds oleacin and oleuropein-aglycone on senescent endothelial and small airway epithelial cells. Antioxidants 2023, 12, 1509. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, F.; Pimentel, F.B.; Oliveira, M.B.P.P. Olive by-products: Challenge application in cosmetic industry. Ind. Crops Prod. 2015, 70, 116–124. [Google Scholar] [CrossRef]
- Tarabanis, C.; Long, C.; Scolaro, B.; Heffron, S.P. Reviewing the cardiovascular and other health effects of olive oil: Limitations and future directions of current supplement formulations. Nutr. Metab. Cardiovasc. Dis. 2023, 33, 2326–2333. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Wang, N.; Ma, Y.; Wen, D. Hydroxytyrosol improves obesity and insulin resistance by modulating gut microbiota in high-fat diet-induced obese mice. Front. Microbiol. 2019, 10, 433543. [Google Scholar] [CrossRef] [PubMed]
- Cao, K.; Xu, J.; Zou, X.; Li, Y.; Chen, C.; Zheng, A.; Li, H.; Li, H.; Szeto, I.M.Y.; Shi, Y.; et al. Hydroxytyrosol prevents diet-induced metabolic syndrome and attenuates mitochondrial abnormalities in obese mice. Free Radic. Biol. Med. 2014, 67, 396–407. [Google Scholar] [CrossRef]
- Pastor, R.; Bouzas, C.; Tur, J.A. Beneficial effects of dietary supplementation with olive oil, oleic acid, or hydroxytyrosol in metabolic syndrome: Systematic review and meta-analysis. Free Radic. Biol. Med. 2021, 172, 372–385. [Google Scholar] [CrossRef]
- Saibandith, B.; Spencer, J.P.E.; Rowland, I.R.; Commane, D.M. Olive polyphenols and the metabolic syndrome. Molecules 2017, 22, 1082. [Google Scholar] [CrossRef]
- De La Torre, R.; Corella, D.; Castañer, O.; Martínez-González, M.A.; Salas-Salvador, J.; Vila, J.; Estruch, R.; Sorli, J.V.; Arós, F.; Fiol, M.; et al. Protective effect of homovanillyl alcohol on cardiovascular disease and total mortality: Virgin olive oil, wine, and catechol-methylathion. Am. J. Clin. Nutr. 2017, 105, 1297–1304. [Google Scholar] [CrossRef]
- Janahmadi, Z.; Nekooeian, A.A.; Moaref, A.R.; Emamghoreishi, M. Oleuropein attenuates the progression of heart failure in rats by antioxidant and antiinflammatory effects. Naunyn. Schmiedebergs. Arch. Pharmacol. 2017, 390, 245–252. [Google Scholar] [CrossRef]
- Esmailidehaj, M.; Rasulian, B.; Rezvani, M.E.; Delfan, B.; Mosaddeghmehrjardi, M.H.; Pourkhalili, K. The anti-infarct, antistunning and antiarrhythmic effects of oleuropein in isolated rat heart. EXCLI J. 2012, 11, 150–162. [Google Scholar]
- Del Ben, M.; Nocella, C.; Loffredo, L.; Bartimoccia, S.; Cammisotto, V.; Mancinella, M.; Angelico, F.; Valenti, V.; Cavarretta, E.; Carnevale, R.; et al. Oleuropein-enriched chocolate by extra virgin olive oil blunts hyperglycaemia in diabetic patients: Results from a one-time 2-hour post-prandial cross over study. Clin. Nutr. 2020, 39, 2187–2191. [Google Scholar] [CrossRef] [PubMed]
- Larussa, T.; Oliverio, M.; Suraci, E.; Greco, M.; Placida, R.; Gervasi, S.; Marasco, R.; Imeneo, M.; Paolino, D.; Tucci, L.; et al. Oleuropein decreases cyclooxygenase-2 and interleukin-17 expression and attenuates inflammatory damage in colonic samples from ulcerative colitis patients. Nutrients 2017, 9, 391. [Google Scholar] [CrossRef] [PubMed]
- Micheli, L.; Bertini, L.; Bonato, A.; Villanova, N.; Caruso, C.; Caruso, M.; Bernini, R.; Tirone, F. Role of hydroxytyrosol and oleuropein in the prevention of aging and related disorders: Focus on neurodegeneration, skeletal muscle dysfunction, and gut microbiota. Nutrients 2023, 15, 1767. [Google Scholar] [CrossRef] [PubMed]
- Fki, I.; Sayadi, S.; Mahmoudi, A.; Daoued, I.; Marrekchi, R.; Ghorbel, H. Comparative study on beneficial effects of hydroxytyrosol- and oleuropein-rich olive leaf extracts on high-fat diet-induced lipid metabolism disturbance and liver injury in rats. Biomed Res. Int. 2020, 2020, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Mahmoudi, A.; Hadrich, F.; Feki, I.; Ghorbel, H.; Bouallagui, Z.; Marrekchi, R.; Fourati, H.; Sayadi, S. Oleuropein and hydroxytyrosol rich extracts from olive leaves attenuate liver injury and lipid metabolism disturbance in bisphenol A-treated rats. Food Funct. 2018, 9, 3220–3234. [Google Scholar] [CrossRef]
- Bender, C.; Strassmann, S.; Golz, C. Oral bioavailability and metabolism of hydroxytyrosol from food supplements. Nutrients 2023, 15, 325. [Google Scholar] [CrossRef]
- Menezes, R.C.R.; Peres, K.K.; Costa-Valle, M.T.; Faccioli, L.S.; Dallegrave, E.; Garavaglia, J.; Dal Bosco, S.M. Oral administration of oleuropein and olive leaf extract has cardioprotective effects in rodents: A systematic review. Rev. Port. Cardiol. 2022, 41, 167–175. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Clark, H.D.; Wells, G.A.; Huët, C.; McAlister, F.A.; Salmi, L.R.; Fergusson, D.; Laupacis, A. Assessing the quality of randomized trials: Reliability of the Jadad scale. Control. Clin. Trials 1999, 20, 448–452. [Google Scholar] [CrossRef]
- Chen, Q.; Zhang, Y.; Wang, Z.; Wang, S.; Zhang, H.; Wang, Y.; Lu, C.; Xuan, H.; Wang, C.; Li, D.; et al. Efficacy and safety of low dose ticagrelor in patients with acute coronary syndrome: A systematic review and meta-analysis. Postgrad. Med. J. 2020, 96, 693–702. [Google Scholar] [CrossRef]
- Vázquez-Velasco, M.; Esperanza Daz, L.; Lucas, R.; Gómez-Martínez, S.; Bastida, S.; Marcos, A.; Sánchez-Muniz, F.J. Effects of hydroxytyrosol-enriched sunflower oil consumption on CVD risk factors. Br. J. Nutr. 2011, 105, 1448–1452. [Google Scholar] [CrossRef] [PubMed]
- Colica, C.; Di Renzo, L.; Trombetta, D.; Smeriglio, A.; Bernardini, S.; Cioccoloni, G.; Costa De Miranda, R.; Gualtieri, P.; Sinibaldi Salimei, P.; De Lorenzo, A. Antioxidant effects of a hydroxytyrosol-based pharmaceutical formulation on body composition, metabolic state, and gene expression: A randomized double-blinded, placebo-controlled crossover trial. Oxid. Med. Cell. Longev. 2017, 2017, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Fytili, C.; Nikou, T.; Tentolouris, N.; Tseti, I.K.; Dimosthenopoulos, C.; Sfikakis, P.P.; Simos, D.; Kokkinos, A.; Skaltsounis, A.L.; Katsilambros, N.; et al. Effect of long-term hydroxytyrosol administration on body weight, fat mass, and urine metabolomics: A randomized double-blind prospective human study. Nutrients 2022, 14, 1525. [Google Scholar] [CrossRef] [PubMed]
- Ikonomidis, I.; Katogiannis, K.; Chania, C.; Iakovis, N.; Tsoumani, M.; Christodoulou, A.; Brinia, E.; Pavlidis, G.; Thymis, J.; Tsilivarakis, D.; et al. Association of hydroxytyrosol enriched olive oil with vascular function in chronic coronary disease. Eur. J. Clin. Investig. 2023, 53, e13983. [Google Scholar] [CrossRef] [PubMed]
- Binou, P.; Stergiou, A.; Kosta, O.; Tentolouris, N.; Karathanos, V.T. Positive contribution of hydroxytyrosol-enriched wheat bread to HbA1c levels, lipid profile, markers of inflammation and body weight in subjects with overweight/obesity and type 2 diabetes mellitus. Eur. J. Nutr. 2023, 62, 2165–2176. [Google Scholar] [CrossRef]
- Yoon, J.; Sasaki, K.; Nishimura, I.; Hashimoto, H.; Okura, T.; Isoda, H. Effects of desert olive tree pearls containing high hydroxytyrosol concentrations on the cognitive functions of middle-aged and older adults. Nutrients 2023, 15, 3234. [Google Scholar] [CrossRef]
- Filip, R.; Possemiers, S.; Heyerick, A.; Pinheiro, I.; Raszewski, G.; Davicco, M.J.; Coxam, V. Twelve-month consumption of a polyphenol extract from olive (Olea europaea) in a double blind, randomized trial increases serum total osteocalcin levels and improves serum lipid profiles in postmenopausal women with osteopenia. J. Nutr. Health Aging 2015, 19, 77–86. [Google Scholar] [CrossRef]
- Stevens, Y.; Winkens, B.; Jonkers, D.; Masclee, A. The effect of olive leaf extract on cardiovascular health markers: A randomized placebo-controlled clinical trial. Eur. J. Nutr. 2021, 60, 2111–2120. [Google Scholar] [CrossRef]
- Horcajada, M.N.; Beaumont, M.; Sauvageot, N.; Poquet, L.; Saboundjian, M.; Costes, B.; Verdonk, P.; Brands, G.; Brasseur, J.; Urbin-Choffray, D.; et al. An oleuropein-based dietary supplement may improve joint functional capacity in older people with high knee joint pain: Findings from a multicentre-RCT and post hoc analysis. Ther. Adv. Musculoskelet. Dis. 2022, 14, 1–15. [Google Scholar] [CrossRef]
- de Bock, M.; Derraik, J.G.B.; Brennan, C.M.; Biggs, J.B.; Morgan, P.E.; Hodgkinson, S.C.; Hofman, P.L.; Cutfield, W.S. Olive (Olea europaea L.) leaf polyphenols improve insulin sensitivity in middle-aged overweight men: A randomized, placebo-controlled, crossover trial. PLoS ONE 2013, 8, e57622. [Google Scholar] [CrossRef]
- Lockyer, S.; Rowland, I.; Spencer, J.P.E.; Yaqoob, P.; Stonehouse, W. Impact of phenolic-rich olive leaf extract on blood pressure, plasma lipids and inflammatory markers: A randomised controlled trial. Eur. J. Nutr. 2017, 56, 1421–1432. [Google Scholar] [CrossRef] [PubMed]
- Araki, R.; Fujie, K.; Yuine, N.; Watabe, Y.; Nakata, Y.; Suzuki, H.; Isoda, H.; Hashimoto, K. Olive leaf tea is beneficial for lipid metabolism in adults with prediabetes: An exploratory randomized controlled trial. Nutr. Res. 2019, 67, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Gong, Y.; Han, Y.; Yu, H.; Zeng, X.; Chen, Z.; An, R.; Sun, N.; Chen, Z.; Yin, X. Body weight, weight change and the risk of cardiovascular disease in patients with hypertension: A primary-care cohort study. Int. J. Obes. 2023, 47, 848–854. [Google Scholar] [CrossRef] [PubMed]
- Santos, A.C.N.A.; Duarte de Souza, M.L.; Machado, A.M.; Kümmel Duarte, C. Olive oil and body fat: A systematic review with meta-analysis. Food Funct. 2023, 14, 5516–5536. [Google Scholar] [CrossRef]
- Peyrol, J.; Riva, C.; Amiot, M.J. Hydroxytyrosol in the prevention of the metabolic syndrome and related disorders. Nutrients 2017, 9, 306. [Google Scholar] [CrossRef]
- Wang, N.; Ma, Y.; Liu, Z.; Liu, L.; Yang, K.; Wei, Y.; Liu, Y.; Chen, X.; Sun, X.; Wen, D. Hydroxytyrosol prevents PM2.5-induced adiposity and insulin resistance by restraining oxidative stress related NF-κB pathway and modulation of gut microbiota in a murine model. Free Radic. Biol. Med. 2019, 141, 393–407. [Google Scholar] [CrossRef]
- Hao, J.; Shen, W.; Yu, G.; Jia, H.; Li, X.; Feng, Z.; Wang, Y.; Weber, P.; Wertz, K.; Sharman, E.; et al. Hydroxytyrosol promotes mitochondrial biogenesis and mitochondrial function in 3T3-L1 adipocytes. J. Nutr. Biochem. 2010, 21, 634–644. [Google Scholar] [CrossRef]
- Vlavcheski, F.; Young, M.; Tsiani, E. Antidiabetic effects of hydroxytyrosol: In vitro and in vivo evidence. Antioxidants 2019, 8, 188. [Google Scholar] [CrossRef]
- de Carvalho Faria, R.V.; Duarte, M.S.; de Souza Nogueira, J.; Gregório, B.M.; Romana-Souza, B. Nrf2 activation by hydroxytyrosol and dimethyl fumarate ameliorates skin tissue repair in high-fat diet-fed mice by promoting M2 macrophage polarization and normalizing inflammatory response and oxidative damage. J. Biochem. Mol. Toxicol. 2024, 38, e23652. [Google Scholar] [CrossRef]
- Zhu, L.; Liu, Z.; Feng, Z.; Hao, J.; Shen, W.; Li, X.; Sun, L.; Sharman, E.; Wang, Y.; Wertz, K.; et al. Hydroxytyrosol protects against oxidative damage by simultaneous activation of mitochondrial biogenesis and phase II detoxifying enzyme systems in retinal pigment epithelial cells. J. Nutr. Biochem. 2010, 21, 1089–1098. [Google Scholar] [CrossRef]
- van der Stelt, I.; Hoek-van den Hil, E.F.; Swarts, H.J.M.; Vervoort, J.J.M.; Hoving, L.; Skaltsounis, L.; Lemonakis, N.; Andreadou, I.; van Schothorst, E.M.; Keijer, J. Nutraceutical oleuropein supplementation prevents high fat diet-induced adiposity in mice. J. Funct. Foods 2015, 14, 702–715. [Google Scholar] [CrossRef]
- Mikami, T.; Kim, J.; Park, J.; Lee, H.; Yaicharoen, P.; Suidasari, S.; Yokozawa, M.; Yamauchi, K. Olive leaf extract prevents obesity, cognitive decline, and depression and improves exercise capacity in mice. Sci. Rep. 2021, 11, 12495. [Google Scholar] [CrossRef] [PubMed]
- Mortensen, M.B.; Dzaye, O.; Bøtker, H.E.; Jensen, J.M.; Maeng, M.; Bentzon, J.F.; Kanstrup, H.; Sørensen, H.T.; Leipsic, J.; Blankstein, R.; et al. Low-density lipoprotein cholesterol is predominantly associated with atherosclerotic cardiovascular disease events in patients with evidence of coronary atherosclerosis: The Western Denmark Heart Registry. Circulation 2023, 147, 1053–1063. [Google Scholar] [CrossRef]
- Jabbarzadeh-Ganjeh, B.; Jayedi, A.; Shab-Bidar, S. The effects of olive oil consumption on blood lipids: A systematic review and dose–response meta-analysis of randomised controlled trials. Br. J. Nutr. 2023, 130, 728–736. [Google Scholar] [CrossRef] [PubMed]
- EFSA. Polyphenols in Olive Related Health Claims. Available online: https://www.efsa.europa.eu/en/efsajournal/pub/2033 (accessed on 28 May 2024).
- de Bock, M.; Thorstensen, E.B.; Derraik, J.G.B.; Henderson, H.V.; Hofman, P.L.; Cutfield, W.S. Human absorption and metabolism of oleuropein and hydroxytyrosol ingested as olive (Olea europaea L.) leaf extract. Mol. Nutr. Food Res. 2013, 57, 2079–2085. [Google Scholar] [CrossRef] [PubMed]
- López de las Hazas, M.C.; Piñol, C.; Macià, A.; Romero, M.P.; Pedret, A.; Solà, R.; Rubió, L.; Motilva, M.J. Differential absorption and metabolism of hydroxytyrosol and its precursors oleuropein and secoiridoids. J. Funct. Foods 2016, 22, 52–63. [Google Scholar] [CrossRef]
- Pongkitwitoon, B.; Putalun, W.; Triwitayakorn, K.; Kitisripanya, T.; Kanchanapoom, T.; Boonsnongcheep, P. Anti-inflammatory activity of verbascoside- and isoverbascoside-rich Lamiales medicinal plants. Heliyon 2024, 10, e23644. [Google Scholar] [CrossRef]
- Pierre Luhata, L.; Usuki, T. Free radical scavenging activities of verbascoside and isoverbascoside from the leaves of Odontonema strictum (Acanthaceae). Bioorganic Med. Chem. Lett. 2022, 59, 128528. [Google Scholar] [CrossRef]
- Zhao, Y.; Wang, S.; Pan, J.; Ma, K. Verbascoside: A neuroprotective phenylethanoid glycosides with anti-depressive properties. Phytomedicine 2023, 120, 155027. [Google Scholar] [CrossRef]
- Covas, M.I.; Nyyssönen, K.; Poulsen, H.E.; Kaikkonen, J.; Zunft, H.J.F.; Kiesewetter, H.; Gaddi, A.; De La Torre, R.; Mursu, J.; Bäumler, H.; et al. The effect of polyphenols in olive oil on heart disease risk factors: A randomized trial. Ann. Intern. Med. 2006, 145, 333–341. [Google Scholar] [CrossRef]
- Jemai, H.; Fki, I.; Bouaziz, M.; Bouallagui, Z.; El Feki, A.; Isoda, H.; Sayadi, S. Lipid-lowering and antioxidant effects of hydroxytyrosol and its triacetylated derivative recovered from olive tree leaves in cholesterol-fed rats. J. Agric. Food Chem. 2008, 56, 2630–2636. [Google Scholar] [CrossRef]
- Tabernero, M.; Sarriá, B.; Largo, C.; Martínez-López, S.; Madrona, A.; Espartero, J.L.; Bravo, L.; Mateos, R. Comparative evaluation of the metabolic effects of hydroxytyrosol and its lipophilic derivatives (hydroxytyrosyl acetate and ethyl hydroxytyrosyl ether) in hypercholesterolemic rats. Food Funct. 2014, 5, 1556–1563. [Google Scholar] [CrossRef]
- Park, S.; Choi, Y.; Um, S.J.; Yoon, S.K.; Park, T. Oleuropein attenuates hepatic steatosis induced by high-fat diet in mice. J. Hepatol. 2011, 54, 984–993. [Google Scholar] [CrossRef] [PubMed]
- Olmez, E.; Vural, K.; Gok, S.; Ozturk, Z.; Kayalar, H.; Ayhan, S.; Var, A. Olive leaf extract improves the atherogenic lipid profile in rats fed a high cholesterol diet. Phyther. Res. 2015, 29, 1652–1657. [Google Scholar] [CrossRef] [PubMed]
- Riise, H.K.R.; Igland, J.; Sulo, G.; Graue, M.; Haltbakk, J.; Tell, G.S.; Iversen, M.M. Casual blood glucose and subsequent cardiovascular disease and all-cause mortality among 159 731 participants in Cohort of Norway (CONOR). BMJ Open Diabetes Res. Care 2021, 9, e001928. [Google Scholar] [CrossRef] [PubMed]
- Violi, F.; Loffredo, L.; Pignatelli, P.; Angelico, F.; Bartimoccia, S.; Nocella, C.; Cangemi, R.; Petruccioli, A.; Monticolo, R.; Pastori, D.; et al. Extra virgin olive oil use is associated with improved post-prandial blood glucose and LDL cholesterol in healthy subjects. Nutr. Diabetes 2015, 5, e172. [Google Scholar] [CrossRef]
- Dehghani, F.; Morvaridzadeh, M.; Pizarro, A.B.; Rouzitalab, T.; Khorshidi, M.; Izadi, A.; Shidfar, F.; Omidi, A.; Heshmati, J. Effect of extra virgin olive oil consumption on glycemic control: A systematic review and meta-analysis. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 1953–1961. [Google Scholar] [CrossRef]
- Jemai, H.; Feki, A.E.L.; Sayadi, S. Antidiabetic and antioxidant effects of hydroxytyrosol and oleuropein from olive leaves in alloxan-diabetic rats. J. Agric. Food Chem. 2009, 57, 8798–8804. [Google Scholar] [CrossRef]
- Pirozzi, C.; Lama, A.; Simeoli, R.; Paciello, O.; Pagano, T.B.; Mollica, M.P.; Di Guida, F.; Russo, R.; Magliocca, S.; Canani, R.B.; et al. Hydroxytyrosol prevents metabolic impairment reducing hepatic inflammation and restoring duodenal integrity in a rat model of NAFLD. J. Nutr. Biochem. 2016, 30, 108–115. [Google Scholar] [CrossRef]
- López-Villodres, J.A.; Abdel-Karim, M.; De La Cruz, J.P.; Rodríguez-Pérez, M.D.; Reyes, J.J.; Guzmán-Moscoso, R.; Rodriguez-Gutierrez, G.; Fernández-Bolaños, J.; González-Correa, J.A. Effects of hydroxytyrosol on cardiovascular biomarkers in experimental diabetes mellitus. J. Nutr. Biochem. 2016, 37, 94–100. [Google Scholar] [CrossRef]
- Qadir, N.M.; Ali, K.A.; Qader, S.W. Antidiabetic effect of oleuropein from Olea europaea leaf against alloxan induced type 1 diabetic in rats. Brazilian Arch. Biol. Technol. 2016, 59, 1–10. [Google Scholar] [CrossRef]
- Nediani, C.; Ruzzolini, J.; Romani, A.; Calorini, L. Oleuropein, a bioactive compound from Olea europaea L., as a potential preventive and therapeutic agent in non-communicable diseases. Antioxidants 2019, 8, 578. [Google Scholar] [CrossRef] [PubMed]
- Hadrich, F.; Bouallagui, Z.; Junkyu, H.; Isoda, H.; Sayadi, S. The α-glucosidase and α-amylase enzyme inhibitory of hydroxytyrosol and oleuropein. J. Oleo Sci. 2015, 64, 835–843. [Google Scholar] [CrossRef]
- Kerimi, A.; Nyambe-Silavwe, H.; Pyner, A.; Oladele, E.; Gauer, J.S.; Stevens, Y.; Williamson, G. Nutritional implications of olives and sugar: Attenuation of post-prandial glucose spikes in healthy volunteers by inhibition of sucrose hydrolysis and glucose transport by oleuropein. Eur. J. Nutr. 2019, 58, 1315–1330. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, F.D.; Whelton, P.K. High blood pressure and cardiovascular disease. Hypertension 2020, 75, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Zamora-Zamora, F.; Martínez-Galiano, J.M.; Gaforio, J.J.; Delgado-Rodríguez, M. Effects of olive oil on blood pressure: A systematic review and meta-analysis. Grasas y Aceites 2018, 69, e272. [Google Scholar] [CrossRef]
- Morvaridzadeh, M.; Cohen, A.A.; Heshmati, J.; Alami, M.; Berrougui, H.; Zoubdane, N.; Pizarro, A.B.; Khalil, A. Effect of extra virgin olive oil on anthropometric indices, inflammatory and cardiometabolic markers: A systematic review and meta-analysis of randomized clinical trials. J. Nutr. 2024, 154, 95–120. [Google Scholar] [CrossRef]
- Hermans, M.P.; Lempereur, P.; Salembier, J.P.; Maes, N.; Albert, A.; Jansen, O.; Pincemail, J. Supplementation effect of a combination of olive (Olea europea L.) leaf and fruit extracts in the clinical management of hypertension and metabolic syndrome. Antioxidants 2020, 9, 872. [Google Scholar] [CrossRef]
- Romero, M.; Toral, M.; Gómez-Guzmán, M.; Jiménez, R.; Galindo, P.; Sánchez, M.; Olivares, M.; Gálvez, J.; Duarte, J. Antihypertensive effects of oleuropein-enriched olive leaf extract in spontaneously hypertensive rats. Food Funct. 2016, 7, 584–593. [Google Scholar] [CrossRef]
- Susalit, E.; Agus, N.; Effendi, I.; Tjandrawinata, R.R.; Nofiarny, D.; Perrinjaquet-Moccetti, T.; Verbruggen, M. Olive (Olea europaea) leaf extract effective in patients with stage-1 hypertension: Comparison with Captopril. Phytomedicine 2011, 18, 251–258. [Google Scholar] [CrossRef]
- Ruparelia, N.; Chai, J.T.; Fisher, E.A.; Choudhury, R.P. Inflammatory processes in cardiovascular disease: A route to targeted therapies. Nat. Rev. Cardiol. 2016, 14, 133–144. [Google Scholar] [CrossRef]
- Giner, E.; Recio, M.C.; Ríos, J.L.; Cerdá-Nicolás, J.M.; Giner, R.M. Chemopreventive effect of oleuropein in colitis-associated colorectal cancer in c57bl/6 mice. Mol. Nutr. Food Res. 2016, 60, 242–255. [Google Scholar] [CrossRef] [PubMed]
- Huguet-Casquero, A.; Xu, Y.; Gainza, E.; Pedraz, J.L.; Beloqui, A. Oral delivery of oleuropein-loaded lipid nanocarriers alleviates inflammation and oxidative stress in acute colitis. Int. J. Pharm. 2020, 586, 119515. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.B.; Zhuang, H.Z.; Ji, X.J.; Dong, L.; Duan, M.L. Hydroxytyrosol suppresses LPS-induced intrahepatic inflammatory responses via inhibition of ERK signaling pathway activation in acute liver injury. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 6455–6462. [Google Scholar] [CrossRef] [PubMed]
- Jin, H.X.; Zhang, Y.H.; Guo, R.N.; Zhao, S.N. Inhibition of MEK/ERK/STAT3 signaling in oleuropein treatment inhibits myocardial ischemia/reperfusion. Int. J. Mol. Med. 2018, 42, 1034–1043. [Google Scholar] [CrossRef] [PubMed]
- Kitade, H.; Chen, G.; Ni, Y.; Ota, T. Nonalcoholic fatty liver disease and insulin resistance: New insights and potential new treatments. Nutrients 2017, 9, 387. [Google Scholar] [CrossRef]
- Ma, Y.; Ding, X.; Gu, J.; Zhou, S.; Jiang, Y. Effects of olive oil on hepatic steatosis and liver enzymes: A systematic review. J. Funct. Foods 2023, 109, 105815. [Google Scholar] [CrossRef]
- Tsamos, G.; Kalopitas, G.; Evripidou, K.; Vasdeki, D.; Koufakis, T.; Kanavas, V.; Antza, C.; Germanidis, G.; Chourdakis, M. The effects of olive oil consumption on biochemical parameters and body mass index of people with nonalcoholic fatty liver disease: A systematic review and meta-analysis of randomized controlled trials. Nutrients 2024, 16, 857. [Google Scholar] [CrossRef]
- Varela-Lopez, A.; Pérez-López, M.P.; Ramirez-Tortosa, C.L.; Battino, M.; Granados-Principal, S.; Ramirez-Tortosa, M.d.C.; Ochoa, J.J.; Vera-Ramirez, L.; Giampieri, F.; Quiles, J.L. Gene pathways associated with mitochondrial function, oxidative stress and telomere length are differentially expressed in the liver of rats fed lifelong on virgin olive, sunflower or fish oils. J. Nutr. Biochem. 2018, 52, 36–44. [Google Scholar] [CrossRef]
- Miao, F.; Geng, S.; Ning, D. Hydroxytyrosol ameliorates LPS-induced acute liver injury (ALI) in mice by modulating the balance between M1/M2 phenotype macrophage and inhibiting TLR4/NF-κB activation. J. Funct. Foods 2023, 102, 105455. [Google Scholar] [CrossRef]
- Santini, S.J.; Porcu, C.; Tarantino, G.; Amicarelli, F.; Balsano, C. Oleuropein overrides liver damage in steatotic mice. J. Funct. Foods 2020, 65, 103756. [Google Scholar] [CrossRef]
- Chin, K.Y.; Pang, K.L. Therapeutic effects of olive and its derivatives on osteoarthritis: From bench to bedside. Nutrients 2017, 9, 1060. [Google Scholar] [CrossRef]
- Cardoso, C.K.d.S.; Santos, A.S.e.A.d.C.; Rosa, L.P.d.S.; Mendonça, C.R.; Vitorino, P.V.d.O.; Peixoto, M.d.R.G.; Silveira, É.A. Effect of extra virgin olive oil and traditional brazilian diet on the bone health parameters of severely obese adults: A randomized controlled trial. Nutrients 2020, 12, 403. [Google Scholar] [CrossRef]
- Hekmatpou, D.; Mortaji, S.; Rezaei, M.; Shaikhi, M. The effectiveness of olive oil in controlling morning inflammatory pain of phalanges and knees among women with rheumatoid arthritis: A randomized clinical trial. Rehabil. Nurs. 2020, 45, 106–113. [Google Scholar] [CrossRef]
- Impellizzeri, D.; Esposito, E.; Mazzon, E.; Paterniti, I.; Di Paola, R.; Morittu, V.M.; Procopio, A.; Britti, D.; Cuzzocrea, S. Oleuropein aglycone, an olive oil compound, ameliorates development of arthritis caused by injection of collagen type II in mice. J. Pharmacol. Exp. Ther. 2011, 339, 859–869. [Google Scholar] [CrossRef] [PubMed]
- Takuma, M.; Haruka, K.; Mutsuto, W.; Toshiki, M.; Kenshiro, M.; Akane, T.; Hiroshi, M.; Yoshihiro, N. Olive leaf extract prevents cartilage degeneration in osteoarthritis of STR/ort mice. Biosci. Biotechnol. Biochem. 2018, 82, 1101–1106. [Google Scholar] [CrossRef]
- Feng, Z.; Li, X.; Lin, J.; Zheng, W.; Hu, Z.; Xuan, J.; Ni, W.; Pan, X. Oleuropein inhibits the IL-1β-induced expression of inflammatory mediators by suppressing the activation of NF-κB and MAPKs in human osteoarthritis chondrocytes. Food Funct. 2017, 8, 3737–3744. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Lapiscina, E.H.; Clavero, P.; Toledo, E.; San Julian, B.; Sanchez-Tainta, A.; Corella, D.; Lamuela-Raventos, R.M.; Martinez, J.A.; Martinez-Gonzalez, M.A. Virgin olive oil supplementation and long-term cognition: The PREDIMED-NAVARRA randomized, trial. J. Nutr. Health Aging 2013, 17, 544–552. [Google Scholar] [CrossRef] [PubMed]
- Tessier, A.J.; Cortese, M.; Yuan, C.; Bjornevik, K.; Ascherio, A.; Wang, D.D.; Chavarro, J.E.; Stampfer, M.J.; Hu, F.B.; Willett, W.C.; et al. Consumption of olive oil and diet quality and risk of dementia-related death. JAMA Netw. Open 2024, 7, E2410021. [Google Scholar] [CrossRef]
- Leri, M.; Natalello, A.; Bruzzone, E.; Stefani, M.; Bucciantini, M. Oleuropein aglycone and hydroxytyrosol interfere differently with toxic Aβ 1-42 aggregation. Food Chem. Toxicol. 2019, 129, 1–12. [Google Scholar] [CrossRef]
- Arunsundar, M.; Shanmugarajan, T.S.; Ravichandran, V. 3,4-dihydroxyphenylethanol attenuates spatio-cognitive deficits in an Alzheimer’s disease mouse model: Modulation of the molecular signals in neuronal survival-apoptotic programs. Neurotox. Res. 2015, 27, 143–155. [Google Scholar] [CrossRef] [PubMed]
- Qin, C.; Hu, S.; Zhang, S.; Zhao, D.; Wang, Y.; Li, H.; Peng, Y.; Shi, L.; Xu, X.; Wang, C.; et al. Hydroxytyrosol acetate improves the cognitive function of APP/PS1 transgenic mice in ERβ-dependent manner. Mol. Nutr. Food Res. 2021, 65, e2000797. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Criteria | Descriptions |
|---|---|
| Population | Adult participants (aged > 18 years) regardless of their health status, with the exclusion of pregnant individuals. |
| Intervention | Standardized supplement, pure compounds, or enriched foods with OLE and/or HT as part of the intervention. |
| Comparison | Placebo that resembled the intervention but lacked the presence of OLE and/or HT. |
| Outcome | Evaluation of the effects of OLE and/or HT supplementation on systemic health outcomes, including but not limited to lipid markers (TC, LDL-C, HDL-C, TAG), glucose metabolism indicators (FBG, HbA1c), blood pressure measurements (SBP, DBP), inflammation markers (CRP, IL-6, etc.), liver function tests (ALT, AST, GGT), cognitive health tests, etc. |
| Study | RCT applying either a crossover or parallel trial design, with a duration of at least two weeks. |
| Items of Modified Jadad Score | Scoring Criteria | Points |
|---|---|---|
| Randomization | Proper randomization described | 2 |
| Study described as randomized but without proper randomization | 1 | |
| Randomization absent or inappropriate | 0 | |
| Concealment of allocation | Proper allocation concealment described | 2 |
| Study mentioned using an allocation concealment method but without proper description | 1 | |
| Allocation concealment method not described | 0 | |
| Blinding | Proper blinding with identical placebo/control | 2 |
| Inadequate or undisclosed blinding | 1 | |
| Double blinding inappropriate or absent | 0 | |
| Withdrawals and dropouts | Numbers and reasons for withdrawals and dropouts detailed | 1 |
| Numbers and reasons for withdrawals and dropouts not detailed | 0 | |
| Total score | Sum of scores across all components | 0–7 |
| Study (Year), Country | Study Design | Participants | Type of Intervention | Intervention/d | Control | Duration | Total Sample (I/C) | Measured Outcomes |
|---|---|---|---|---|---|---|---|---|
| Vázquez-Velasco et al. (2011), Spain [35] | Randomized, single-blinded, placebo-controlled, crossover trial | Healthy subjects | ESO | 10–15 g/d of HT-ESO (45–50 mg HT) | 10–15 g/d of control sun- flower oil | 3 wk | 22 (11/11) | CVD risk factors: Lipid profile, inflammatory markers |
| de Bock et al. (2013), New Zealand [44] | Randomized, double-blinded, placebo-controlled, crossover trial | Overweight subjects | Pure compounds | 51.1 mg/d OLE and 9.7 mg/d HT | Placebo | 12 wk | 45 (23/22) | CVD risk factors: Insulin sensitivity, lipid profile, hormones, adiposity, blood pressure, liver parameters |
| Filip et al. (2015), Poland [41] | Randomized, double-blinded, placebo-controlled, parallel trial | Postmenopausal and osteopenic women | Standardized supplement | 250 mg/d olive extract (100 mg OLE) and 1000 mg Ca | Placebo and 1000 mg Ca | 12 m | 64 (32/32) | Bone metabolism and CVD risk factors: Bone health, lipid profile, inflammatory markers |
| Colica et al. (2017), Italy [36] | Randomized, double-blinded, placebo-controlled, crossover trial | Healthy subjects | Pure compound | 15 mg/d HT | Placebo | 3 wk | 28 (14/14) | Antioxidant and metabolic state: Body composition, antioxidant status, glucose metabolism, lipid profile, gene expression |
| Lockyer et al. (2017), New Zealand [45] | Randomized, double-blinded, placebo-controlled, crossover trial | Pre-hypertensive subjects | Pure compounds | 136.2 mg/d OLE and 6.4 mg/d HT | Placebo | 6 wk | 60 (30/30) | CVD risk factors: Blood pressure, lipid profile, glucose metabolism, inflammatory markers |
| Araki et al. (2019), Japan [46] | Randomized, unblinded, placebo-controlled, parallel trial | Prediabetic subjects | OLI | 990 mL/d OLI (320.8 mg OLE and 11.9 mg HT) | 990 mL/d OLI (23.8 mg OLE and 3 mg HT) | 12 wk | 57 (28/29) | CVD risk factors: Anthropometric parameters, glucose metabolism, lipid profile |
| Stevens et al. (2021), the Netherlands [42] | Randomized, double-blinded, placebo-controlled, parallel trial | Overweight/obese subjects | Standardized supplement | 500 mg/d olive leaf extract (83.5 mg OLE) | Placebo | 8 wk | 77 (39/38) | CVD risk factors: Anthropometric parameters, lipid profile, blood pressure, glucose metabolism, liver function |
| Fytili et al. (2022), Greece [37] | Randomized, double-blinded, placebo-controlled, parallel trial | Overweight/obese subjects | Pure compound | 5 or 15 mg/d HT | Placebo | 6 m | 29 (18/11) | CVD risk factors: Anthropometric parameters |
| Horcajada et al. (2022), Belgium [43] | Randomized, double-blinded, placebo-controlled, parallel trial | Subjects with knee pain | Standardized supplement | 250 mg/d olive leaf extract (100 mg OLE) | Placebo | 6 m | 124 (62/62) | Joint functional capacity: Joint health, cartilage degradation, inflammatory markers |
| Ikonomidis et al. (2023), Greece [38] | Randomized, double-blinded, placebo-controlled, crossover trial | Chronic coronary artery syndrome subjects | Standardized supplement | 1650 mg olive oil and 10 mg/d HT | 1650 mg olive oil | 4 wk | 30 (17/13) | CCD: Vascular function, oxidative stress, inflammatory markers, lipid profile |
| Binou et al. (2023), Greece [39] | Randomized, single-blinded, placebo-controlled, parallel trial | Overweight/obese and T2DM subjects | Enriched WWB | 60 g/d HT-enriched WWB (32.5 mg HT) | 60 g/d conventional WWBd | 12 wk | 75 (38/37) | CVD risk factors: Anthropometric parameters, glucose metabolism, blood pressure, lipid profile, liver parameters, inflammatory markers, hormones |
| Yoon et al. (2023), Japan [40] | Randomized, double-blinded, placebo-controlled, parallel trial | Healthy middle-aged and older subjects | Enriched DOTPs | 6 g/d HT-enriched DOTPs (97.2 HT) | 6 g/d DOTPs | 12 wk | 72 (36/36) | Cognitive function: Memory, attention, processing speed, executive function, reaction time, and motor skills |
| Study | Items of Modified Jadad Score | ||||
|---|---|---|---|---|---|
| Randomization | Concealment of Allocation | Double-Blinding | Withdrawals and Dropouts | Total Score | |
| Vázquez-Velasco et al. (2011) [35] | 2 | 0 | 2 | 1 | 5 |
| de Bock et al. (2013) [44] | 2 | 2 | 2 | 1 | 7 |
| Filip et al. (2015) [41] | 2 | 0 | 2 | 1 | 5 |
| Colica et al. (2017) [36] | 2 | 0 | 2 | 1 | 5 |
| Lockyer et al. (2017) [45] | 2 | 2 | 2 | 1 | 7 |
| Araki et al. (2019) [46] | 1 | 0 | 0 | 1 | 2 |
| Stevens et al. (2021) [42] | 2 | 2 | 2 | 1 | 7 |
| Fytili et al. (2022) [37] | 1 | 2 | 2 | 1 | 6 |
| Horcajada et al. (2022) [43] | 2 | 0 | 2 | 1 | 5 |
| Ikonomidis et al. (2023) [38] | 2 | 2 | 2 | 1 | 7 |
| Binou et al. (2023) [39] | 2 | 0 | 1 | 1 | 4 |
| Yoon et al. (2023) [40] | 2 | 1 | 2 | 1 | 6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frumuzachi, O.; Gavrilaș, L.I.; Vodnar, D.C.; Rohn, S.; Mocan, A. Systemic Health Effects of Oleuropein and Hydroxytyrosol Supplementation: A Systematic Review of Randomized Controlled Trials. Antioxidants 2024, 13, 1040. https://doi.org/10.3390/antiox13091040
Frumuzachi O, Gavrilaș LI, Vodnar DC, Rohn S, Mocan A. Systemic Health Effects of Oleuropein and Hydroxytyrosol Supplementation: A Systematic Review of Randomized Controlled Trials. Antioxidants. 2024; 13(9):1040. https://doi.org/10.3390/antiox13091040
Chicago/Turabian StyleFrumuzachi, Oleg, Laura Ioana Gavrilaș, Dan Cristian Vodnar, Sascha Rohn, and Andrei Mocan. 2024. "Systemic Health Effects of Oleuropein and Hydroxytyrosol Supplementation: A Systematic Review of Randomized Controlled Trials" Antioxidants 13, no. 9: 1040. https://doi.org/10.3390/antiox13091040