Maternal Antioxidant Status in Early Pregnancy and Development of Fetal Complications in Twin Pregnancies: A Pilot Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population of Study
2.2. Maternal Blood Parameters
2.3. Maternal Plasma Oxidative Status Parameters
2.4. Maternal Plasma Hormones
2.5. Statistical Analysis
3. Results
3.1. Population of the Study
3.2. Maternal Blood Parameters
3.3. Maternal Oxidative Status Parameters
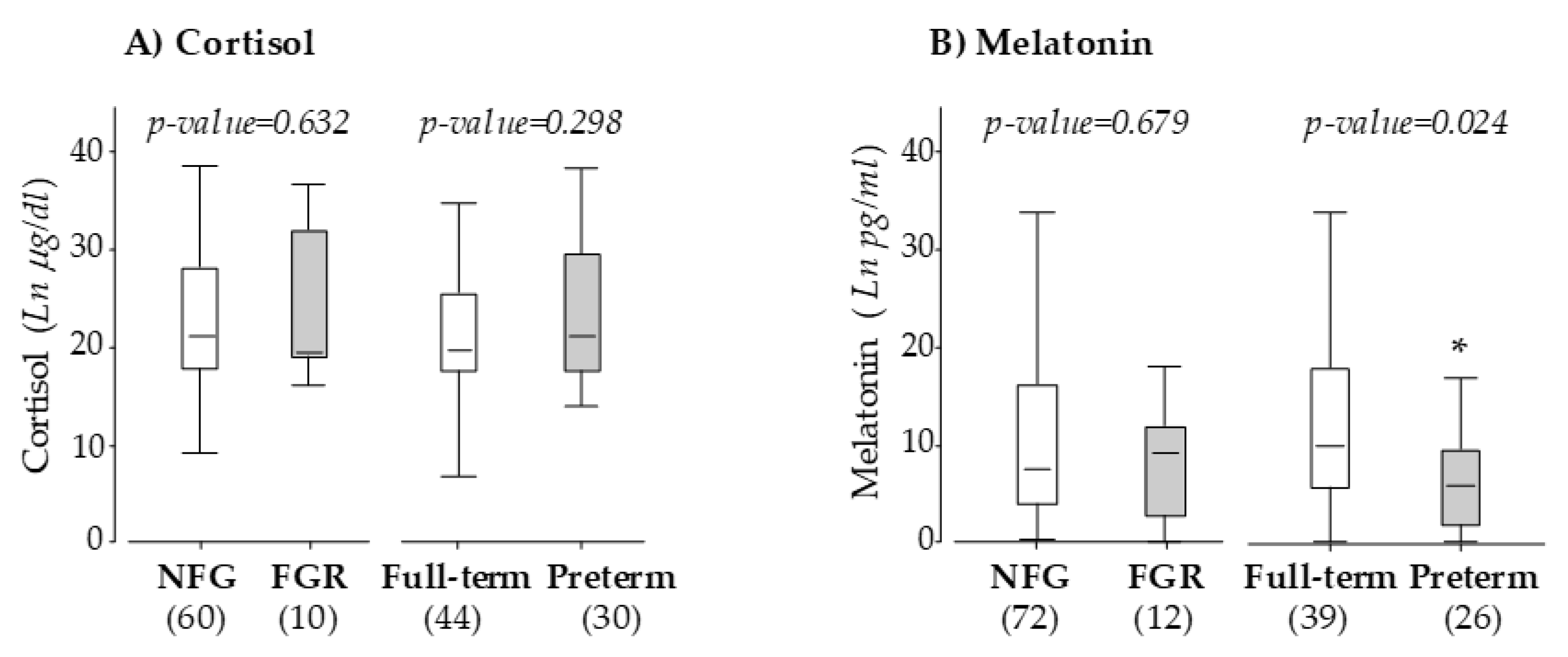
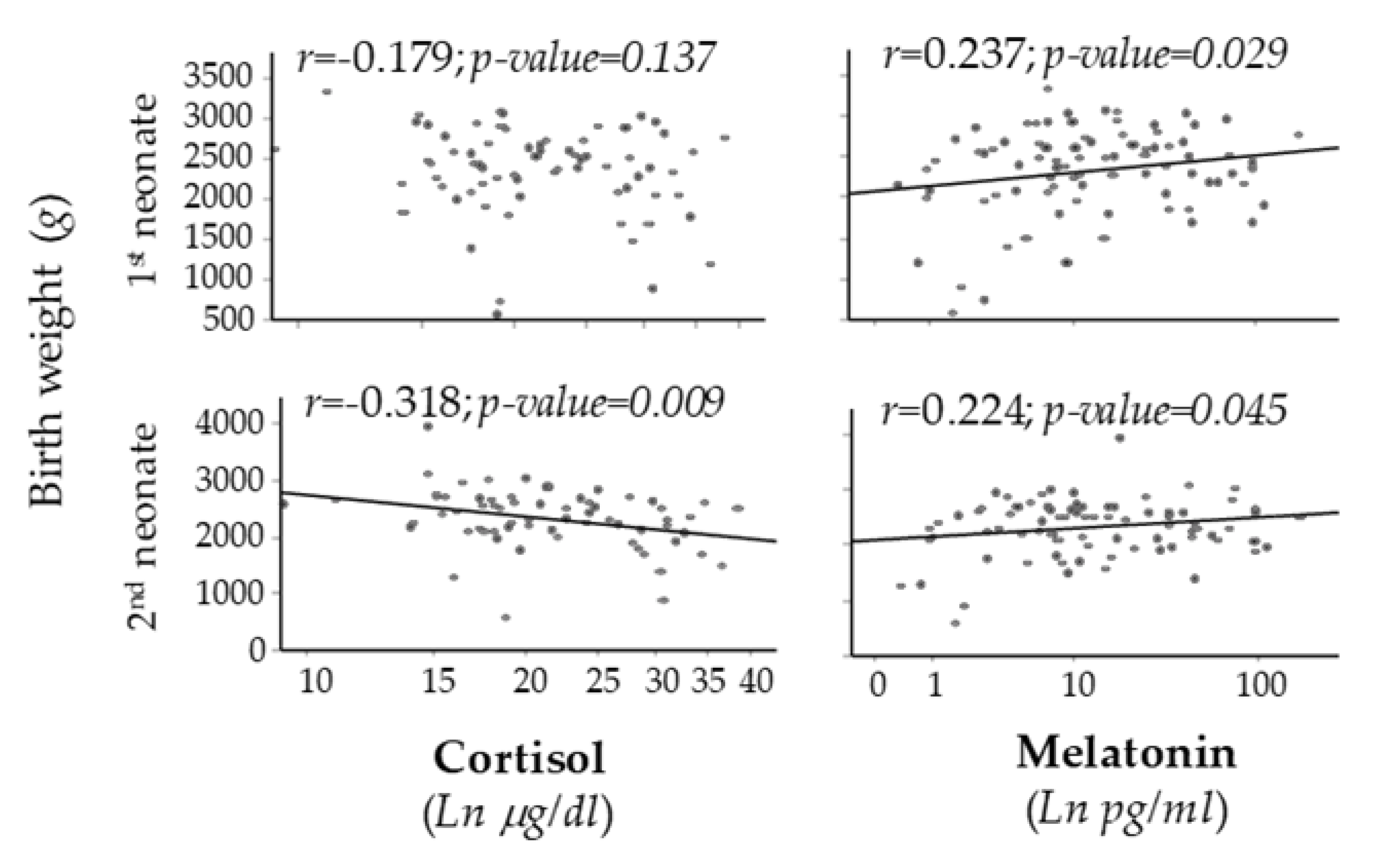
3.4. Maternal Hormones
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Conde-Agudelo, A.; Romero, R. Prediction of preterm birth in twin gestations using biophysical and biochemical tests. Am. J. Obstet. Gynecol. 2014, 211, 583–595. [Google Scholar] [CrossRef]
- Breart, G.; Barros, H.; Wagener, Y.; Prati, S. Characteristics of the childbearing population in Europe. Eur. J. Obstet. Gynecol. Reprod. Biol. 2003, 111 (Suppl. 1), S45–S52. [Google Scholar] [CrossRef]
- Ventura, S.J.; Abma, J.C.; Mosher, W.D.; Henshaw, S.K. Estimated pregnancy rates for the United States, 1990–2005: An update. Natl. Vital. Stat. Rep. 2009, 58, 1–14. [Google Scholar]
- Modena, A.B.; Berghella, V. Antepartum management of multifetal pregnancies. Clin. Perinatol. 2005, 32, 443–454. [Google Scholar] [CrossRef] [PubMed]
- Carolan, M.; Frankowska, D. Advanced maternal age and adverse perinatal outcome: A review of the evidence. Midwifery 2011, 27, 793–801. [Google Scholar] [CrossRef] [PubMed]
- Morag, I.; Stern Levkovitz, O.; Siman-Tov, M.; Frisch, M.; Pinhas-Hamiel, O.; Strauss, T. Postnatal Growth Disadvantage of the Small for Gestational Age Preterm Twins. Nutrients 2018, 10, 476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gluckman, P.D.; Hanson, M.A.; Cooper, C.; Thornburg, K.L. Effect of in utero and early-life conditions on adult health and disease. N. Engl. J. Med. 2008, 359, 61–73. [Google Scholar] [CrossRef] [Green Version]
- Tarrade, A.; Panchenko, P.; Junien, C.; Gabory, A. Placental contribution to nutritional programming of health and diseases: Epigenetics and sexual dimorphism. J. Exp. Biol. 2015, 218, 50–58. [Google Scholar] [CrossRef] [Green Version]
- Jauniaux, E.; Watson, A.L.; Hempstock, J.; Bao, Y.P.; Skepper, J.N.; Burton, G.J. Onset of maternal arterial blood flow and placental oxidative stress. A possible factor in human early pregnancy failure. Am. J. Pathol. 2000, 157, 2111–2122. [Google Scholar] [CrossRef]
- Myatt, L. Review: Reactive oxygen and nitrogen species and functional adaptation of the placenta. Placenta 2010, 31, S66–S69. [Google Scholar] [CrossRef] [Green Version]
- Burton, G.J.; Jauniaux, E. Pathophysiology of placental-derived fetal growth restriction. Am. J. Obstet. Gynecol. 2018, 218, S745–S761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramiro-Cortijo, D.; Herrera, T.; Rodriguez-Rodriguez, P.; Lopez De Pablo, A.L.; De La Calle, M.; Lopez-Gimenez, M.R.; Mora-Urda, A.I.; Gutierrez-Arzapalo, P.Y.; Gomez-Rioja, R.; Aguilera, Y.; et al. Maternal plasma antioxidant status in the first trimester of pregnancy and development of obstetric complications. Placenta 2016, 47, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, C.; Mayo, J.C.; Sainz, R.M.; Antolin, I.; Herrera, F.; Martin, V.; Reiter, R.J. Regulation of antioxidant enzymes: A significant role for melatonin. J. Pineal Res. 2004, 36, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Reiter, R.J.; Tan, D.X.; Manchester, L.C.; Paredes, S.D.; Mayo, J.C.; Sainz, R.M. Melatonin and reproduction revisited. Biol. Reprod. 2009, 81, 445–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.C.; Sheen, J.M.; Tiao, M.M.; Tain, Y.L.; Huang, L.T. Roles of melatonin in fetal programming in compromised pregnancies. Int. J. Mol. Sci. 2013, 14, 5380–5401. [Google Scholar] [CrossRef] [Green Version]
- Murphy, V.E.; Smith, R.; Giles, W.B.; Clifton, V.L. Endocrine regulation of human fetal growth: The role of the mother, placenta, and fetus. Endocr. Rev. 2006, 27, 141–169. [Google Scholar] [CrossRef]
- Zhu, P.; Wang, W.; Zuo, R.; Sun, K. Mechanisms for establishment of the placental glucocorticoid barrier, a guard for life. Cell. Mol. Life Sci. 2019, 76, 13–26. [Google Scholar] [CrossRef]
- Gomez-Roig, M.D.; Mazarico, E.; Cardenas, D.; Fernandez, M.T.; Diaz, M.; Ruiz de Gauna, B.; Vela, A.; Gratacos, E.; Figueras, F. Placental 11B-Hydroxysteroid Dehydrogenase Type 2 mRNA Levels in Intrauterine Growth Restriction versus Small-for-Gestational-Age Fetuses. Fetal Diagn. Ther. 2016, 39, 147–151. [Google Scholar] [CrossRef]
- Emet, T.; Ustuner, I.; Guven, S.G.; Balik, G.; Ural, U.M.; Tekin, Y.B.; Senturk, S.; Sahin, F.K.; Avsar, A.F. Plasma lipids and lipoproteins during pregnancy and related pregnancy outcomes. Arch. Gynecol. Obstet. 2013, 288, 49–55. [Google Scholar] [CrossRef]
- Herrera, E.; Ortega-Senovilla, H. Lipid metabolism during pregnancy and its implications for fetal growth. Curr. Pharm. Biotechnol. 2014, 15, 24–31. [Google Scholar] [CrossRef]
- Condezo-Hoyos, L.; Rubio, M.; Arribas, S.M.; Espana-Caparros, G.; Rodriguez-Rodriguez, P.; Mujica-Pacheco, E.; Gonzalez, M.C. A plasma oxidative stress global index in early stages of chronic venous insufficiency. J. Vasc. Surg. 2013, 57, 205–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruiz-Hurtado, G.; Condezo-Hoyos, L.; Pulido-Olmo, H.; Aranguez, I.; Del Carmen Gonzalez, M.; Arribas, S.; Cerezo, C.; Segura, J.; Praga, M.; Fernandez-Alfonso, M.S.; et al. Development of albuminuria and enhancement of oxidative stress during chronic renin-angiotensin system suppression. J. Hypertens. 2014, 32, 2082–2091. [Google Scholar] [CrossRef] [PubMed]
- Karowicz-Bilinska, A.; Kedziora-Kornatowska, K.; Bartosz, G. Indices of oxidative stress in pregnancy with fetal growth restriction. Free Radic. Res. 2007, 41, 870–873. [Google Scholar] [CrossRef] [PubMed]
- Longini, M.; Perrone, S.; Kenanidis, A.; Vezzosi, P.; Marzocchi, B.; Petraglia, F.; Centini, G.; Buonocore, G. Isoprostanes in amniotic fluid: A predictive marker for fetal growth restriction in pregnancy. Free Radic. Biol. Med. 2005, 38, 1537–1541. [Google Scholar] [CrossRef] [PubMed]
- Alers, N.O.; Jenkin, G.; Miller, S.L.; Wallace, E.M. Antenatal melatonin as an antioxidant in human pregnancies complicated by fetal growth restriction—A phase I pilot clinical trial: Study protocol. BMJ Open 2013, 3, e004141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berbets, A.; Koval, H.; Barbe, A.; Albota, O.; Yuzko, O. Melatonin decreases and cytokines increase in women with placental insufficiency. J. Maternal-Fetal Neonatal Med. 2019, 6, 1–6. [Google Scholar] [CrossRef]
- McCarthy, R.; Jungheim, E.S.; Fay, J.C.; Bates, K.; Herzog, E.D.; England, S.K. Riding the Rhythm of Melatonin Through Pregnancy to Deliver on Time. Front. Endocrinol. (Lausanne) 2019, 10, 616. [Google Scholar] [CrossRef] [Green Version]
- Tain, Y.L.; Huang, L.T.; Hsu, C.N. Developmental Programming of Adult Disease: Reprogramming by Melatonin? Int. J. Mol. Sci. 2017, 18, 426. [Google Scholar] [CrossRef] [Green Version]
- Cherak, S.J.; Giesbrecht, G.F.; Metcalfe, A.; Ronksley, P.E.; Malebranche, M.E. The effect of gestational period on the association between maternal prenatal salivary cortisol and birth weight: A systematic review and meta-analysis. Psychoneuroendocrinology 2018, 94, 49–62. [Google Scholar] [CrossRef]
- Mastorakos, G.; Ilias, I. Maternal and fetal hypothalamic-pituitary-adrenal axes during pregnancy and postpartum. Ann. N. Y. Acad. Sci. 2003, 997, 136–149. [Google Scholar] [CrossRef]
- Matthiesen, S.M.; Frederiksen, Y.; Ingerslev, H.J.; Zachariae, R. Stress, distress and outcome of assisted reproductive technology (ART): A meta-analysis. Hum. Reprod. 2011, 26, 2763–2776. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Maternal Age (years) | 35.1 ± 0.5 |
|---|---|
| ART (%) | 66.7 (68) |
| FGR (%) | 13.6 (14) |
| Birth weight 1st neonate (g) | 2339.8 ± 56.3 |
| Birth weight 2nd neonate (g) | 2323.9 ± 55.7 |
| Gestational age (weeks) | 36.1 ± 0.2 |
| Preterm labor (%) | 41.7 (43) |
| Parameter | NFG (60) | FGR (10) | p-Value | Full-Term (52) | Preterm (35) | p-Value |
|---|---|---|---|---|---|---|
| Glucose (mg/dL) | 91.3 ± 3.4 | 96.9 ± 10.2 | 0.554 | 91.5 ± 4.3 | 95.7 ± 4.8 | 0.520 |
| Cholesterol (mg/dL) | 182.0 ± 3.8 | 169.0 ± 6.4 | 0.183 | 180.0 ± 4.0 | 182.0 ± 5.3 | 0.725 |
| Triglycerides (mg/dL) | 97.9 ± 3.2 | 95.5 ± 7.8 | 0.580 | 96.1 ± 3.6 | 100.2 ± 4.8 | 0.412 |
| Hematocrit (%) | 38.3 ± 0.4 | 39.9 ± 0.9 | 0.170 | 38.8 ± 0.5 | 38.1 ± 0.5 | 0.310 |
| Leucocytes (106/mL) | 8.7 ± 0.2 | 8.7 ± 0.7 | 0.967 | 8.6 ± 0.2 | 8.9 ± 0.3 | 0.538 |
| Parameter | NFG (72) | FGR (12) | p-Value | Full-Term (52) | Preterm (39) | p-Value |
|---|---|---|---|---|---|---|
| Catalase activity (U CAT/mg prot.) | 0.4 ± 0.03 | 0.5 ± 0.2 | 0.384 | 0.5 ± 0.05 | 0.4 ± 0.07 | 0.550 |
| SOD activity (U SOD/mg prot.) | 1.3 ± 0.1 | 1.1 ± 0.3 | 0.598 | 1.4 ± 0.2 | 1.2 ± 0.2 | 0.518 |
| Glutathione (mg GSH/mg prot.) | 0.7 ± 0.09 | 0.9 ± 0.2 | 0.440 | 0.8 ± 0.1 | 0.9 ± 0.1 | 0.407 |
| Thiol groups (µM GSH/mg prot.) | 4.7 ± 0.1 | 4.8 ± 0.6 | 0.684 | 4.7 ± 0.2 | 4.6 ± 0.2 | 0.778 |
| Phenolic compounds (mg GAE/L) | 300 ± 6.7 | 271 ± 26.4 | 0.149 | 290 ± 8.4 | 294 ± 10.5 | 0.805 |
| Malondialdehyde (µmol/L) | 6.5 ± 0.5 | 8.8 ± 1.7 | 0.101 | 7.2 ± 0.6 | 6.4 ± 0.6 | 0.359 |
| Carbonyl groups (nmol/mg prot.) | 0.9 ± 0.1 | 0.7 ± 0.2 | 0.530 | 0.8 ± 0.1 | 0.8 ± 0.1 | 0.626 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramiro-Cortijo, D.; Calle, M.d.l.; Rodríguez-Rodríguez, P.; Pablo, Á.L.L.d.; López-Giménez, M.R.; Aguilera, Y.; Martín-Cabrejas, M.A.; González, M.d.C.; Arribas, S.M. Maternal Antioxidant Status in Early Pregnancy and Development of Fetal Complications in Twin Pregnancies: A Pilot Study. Antioxidants 2020, 9, 269. https://doi.org/10.3390/antiox9040269
Ramiro-Cortijo D, Calle Mdl, Rodríguez-Rodríguez P, Pablo ÁLLd, López-Giménez MR, Aguilera Y, Martín-Cabrejas MA, González MdC, Arribas SM. Maternal Antioxidant Status in Early Pregnancy and Development of Fetal Complications in Twin Pregnancies: A Pilot Study. Antioxidants. 2020; 9(4):269. https://doi.org/10.3390/antiox9040269
Chicago/Turabian StyleRamiro-Cortijo, David, María de la Calle, Pilar Rodríguez-Rodríguez, Ángel L. López de Pablo, María R. López-Giménez, Yolanda Aguilera, María A. Martín-Cabrejas, María del Carmen González, and Silvia M. Arribas. 2020. "Maternal Antioxidant Status in Early Pregnancy and Development of Fetal Complications in Twin Pregnancies: A Pilot Study" Antioxidants 9, no. 4: 269. https://doi.org/10.3390/antiox9040269