Is Sleep Associated with the S-Klotho Anti-Aging Protein in Sedentary Middle-Aged Adults? The FIT-AGEING Study


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Protocol and Participants
2.2. Measurements
2.2.1. Anthropometry and Body Composition
2.2.2. Sleep Quantity and Quality
2.2.3. S-Klotho Plasma Levels
2.3. Statistical Analysis
3. Results
3.1. Study Participants
3.2. Association between Objective Sleep Quantity and Quality and S-Klotho
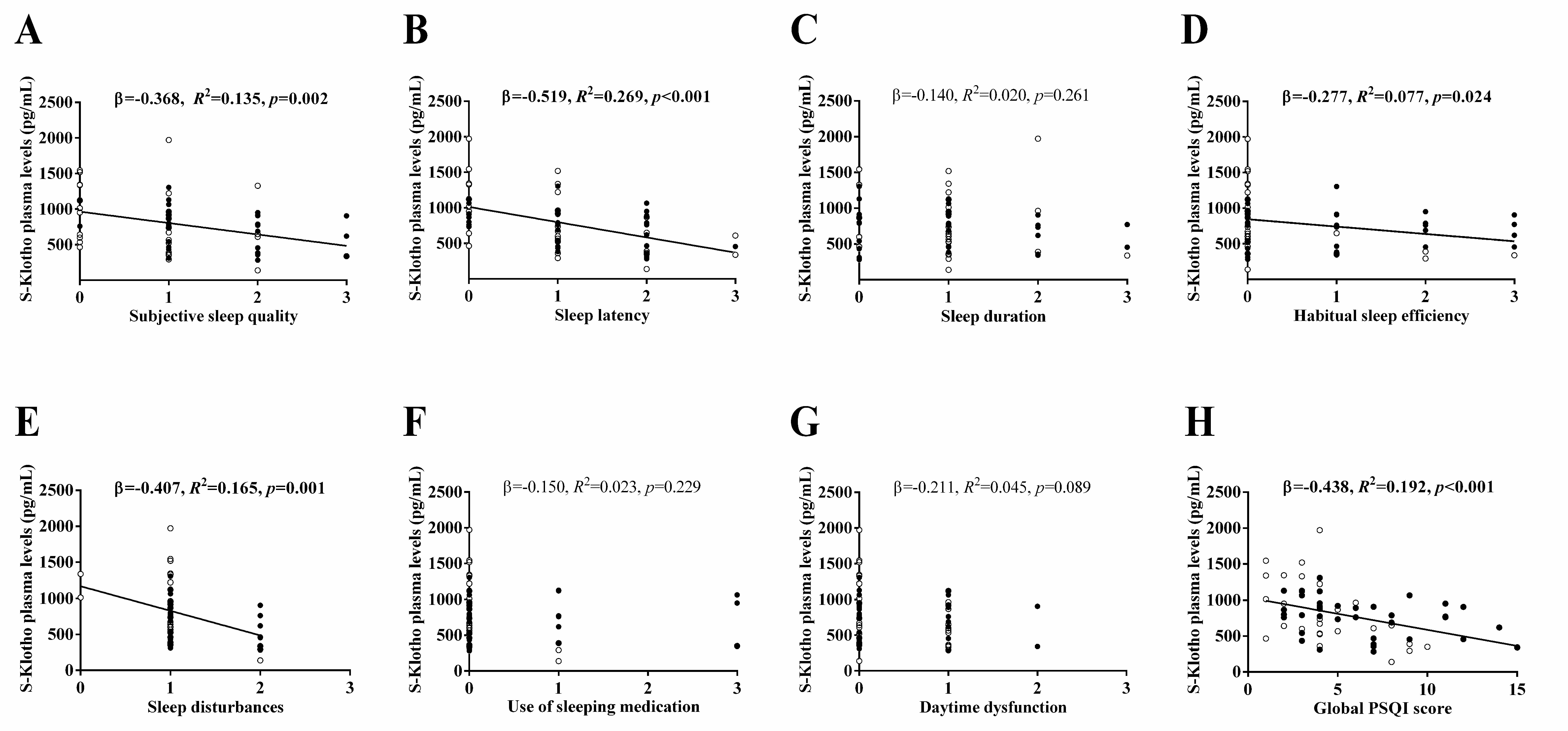
3.3. Association between Subjective Sleep Quantity and Quality and S-Klotho
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Stanaway, J.D.; Afshin, A.; Gakidou, E.; Lim, S.S.; Abate, D.; Abate, K.H.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1923–1994. [Google Scholar] [CrossRef] [Green Version]
- Chang, A.Y.; Skirbekk, V.F.; Tyrovolas, S.; Kassebaum, N.J.; Dieleman, J.L. Measuring population ageing: An analysis of the Global Burden of Disease Study 2017. Lancet Public Health 2019, 4, e159–e167. [Google Scholar] [CrossRef] [Green Version]
- WHO. Global Strategy and Action Plan on Ageing and Health; World Health Organization: Geneva, Switzerland, 2017; ISBN 9789241513500. [Google Scholar]
- Beard, J.R.; Officer, A.; De Carvalho, I.A.; Sadana, R.; Pot, A.M.; Michel, J.P.; Lloyd-Sherlock, P.E.; Epping-Jordan, J.; Peeters, G.M.E.E.; Mahanani, W.R.; et al. The World report on ageing and health: A policy framework for healthy ageing. Lancet 2015, 387, 2145–2154. [Google Scholar] [CrossRef] [Green Version]
- Blagosklonny, M.V. Disease or not, aging is easily treatable. Aging 2018, 10, 3067–3078. [Google Scholar] [CrossRef]
- Son, D.H.; Park, W.J.; Lee, Y.J. Recent advances in anti-aging medicine. Korean J. Fam. Med. 2019, 40, 289–296. [Google Scholar] [CrossRef]
- Longo, V.D.; Antebi, A.; Bartke, A.; Barzilai, N.; Brown-Borg, H.M.; Caruso, C.; Curiel, T.J.; De Cabo, R.; Franceschi, C.; Gems, D.; et al. Interventions to slow aging in humans: Are we ready? Aging Cell 2015, 14, 497–510. [Google Scholar] [CrossRef]
- Viña, J.; Borras, C.; Miquel, J. Theories of ageing. IUBMB Life 2007, 59, 249–254. [Google Scholar] [CrossRef]
- Rudzińska, M.; Parodi, A.; Balakireva, A.V.; Chepikova, O.E.; Venanzi, F.M.; Zamyatnin, J.A.A. Cellular aging characteristics and their association with age-related disorders. Antioxidants 2020, 9, 94. [Google Scholar] [CrossRef] [Green Version]
- Dierickx, P.; Van Laake, L.W.; Geijsen, N. Circadian clocks: From stem cells to tissue homeostasis and regeneration. EMBO Rep. 2017, 19, 18–28. [Google Scholar] [CrossRef]
- Porkka-Heiskanen, T. Sleep homeostasis. Curr. Opin. Neurobiol. 2013, 23, 799–805. [Google Scholar] [CrossRef]
- Åkerstedt, T.; Nilsson, P.M. Sleep as restitution: An introduction. J. Intern. Med. 2003, 254, 6–12. [Google Scholar] [CrossRef]
- St-Onge, M. Sleep-obesity relation: Underlying mechanisms and consequences for treatment. Obes. Rev. 2017, 18, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Spiegel, K.; Tasali, E.; Leproult, R.; Van Cauter, E. Effects of poor and short sleep on glucose metabolism and obesity risk. Nat. Rev. Endocrinol. 2009, 5, 253–261. [Google Scholar] [CrossRef]
- Reynolds, A.C.; Dorrian, J.; Liu, P.Y.; Van Dongen, H.P.A.; Wittert, G.A.; Harmer, L.J.; Banks, S. Impact of five nights of sleep restriction on glucose metabolism, leptin and testosterone in young adult men. PLoS ONE 2012, 7, e41218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benedict, C.; Vogel, H.; Jonas, W.; Woting, A.; Blaut, M.; Schürmann, A.; Cedernaes, J. Gut microbiota and glucometabolic alterations in response to recurrent partial sleep deprivation in normal-weight young individuals. Mol. Metab. 2016, 5, 1175–1186. [Google Scholar] [CrossRef] [PubMed]
- Gao, Q.; Kou, T.; Zhuang, B.; Ren, Y.; Dong, X.; Wang, Q. The association between vitamin D deficiency and sleep disorders: A systematic review and meta-analysis. Nutrients 2018, 10, 1395. [Google Scholar] [CrossRef] [Green Version]
- Chattu, S.K.; Manzar, D.; Kumary, S.; Burman, D.; Spence, D.W.; Pandi-Perumal, S.R. The global problem of insufficient sleep and its serious public health implications. Health 2018, 7, 1. [Google Scholar] [CrossRef] [Green Version]
- Ong, C.W.; O’Driscoll, D.M.; Truby, H.; Naughton, M.T.; Hamilton, G.S. The reciprocal interaction between obesity and obstructive sleep apnoea. Sleep Med. Rev. 2013, 17, 123–131. [Google Scholar] [CrossRef]
- McHill, A.W.; Wright, K.P.; Wright, K.P.J. Role of sleep and circadian disruption on energy expenditure and in metabolic predisposition to human obesity and metabolic disease. Obes. Rev. 2017, 18, 15–24. [Google Scholar] [CrossRef]
- Javaheri, S.; Redline, S. Insomnia and risk of cardiovascular disease. Chest 2017, 152, 435–444. [Google Scholar] [CrossRef]
- Aurora, R.N.; Punjabi, N.M. Obstructive sleep apnoea and type 2 diabetes mellitus: A bidirectional association. Lancet Respir. Med. 2013, 1, 329–338. [Google Scholar] [CrossRef]
- Grandner, M.A.; Seixas, A.; Shetty, S.; Shenoy, S. Sleep duration and diabetes risk: Population trends and potential mechanisms. Curr. Diabetes Rep. 2016, 16, 106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheungpasitporn, W.; Thongprayoon, C.; Gonzalez-Suarez, M.L.; Srivali, N.; Ungprasert, P.; Kittanamongkolchai, W.; Caples, S.M.; Erickson, S.B. The effects of short sleep duration on proteinuria and chronic kidney disease: A systematic review and meta-analysis. Nephrol. Dial. Transplant. 2016, 32, 991–996. [Google Scholar] [CrossRef]
- Goldstein, A.N.; Walker, M.P. The role of sleep in emotional brain function. Annu. Rev. Clin. Psychol. 2014, 10, 679–708. [Google Scholar] [CrossRef] [Green Version]
- Kuro-O, M.; Matsumura, Y.; Aizawa, H.; Kawaguchi, H.; Suga, T.; Utsugi, T.; Ohyama, Y.; Kurabayashi, M.; Kaname, T.; Kume, E.; et al. Mutation of the mouse klotho gene leads to a syndrome resembling ageing. Nature 1997, 390, 45–51. [Google Scholar] [CrossRef]
- Kuro-O, M. Klotho. Pflügers Arch. 2010, 459, 333–343. [Google Scholar] [CrossRef]
- Bian, A.; Neyra, J.A.; Zhan, M.; Hu, M.C. Klotho, stem cells, and aging. Clin. Interv. Aging 2015, 10, 1233–1243. [Google Scholar] [CrossRef] [Green Version]
- Xu, Y.; Sun, Z. Molecular basis of Klotho: From gene to function in aging. Endocr. Rev. 2015, 36, 174–193. [Google Scholar] [CrossRef] [Green Version]
- Cheikhi, A.; Barchowsky, A.; Sahu, A.; Shinde, S.N.; Pius, A.; Clemens, Z.J.; Li, H.; Kennedy, C.A.; Hoeck, J.D.; Franti, M.; et al. Klotho: An elephant in aging research. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2019, 74, 1031–1042. [Google Scholar] [CrossRef]
- Kim, J.H.; Hwang, K.H.; Park, K.S.; Kong, I.D.; Cha, S.K. Biological role of anti-aging protein Klotho. J. Lifestyle Med. 2015, 5, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Kuro-O, M. The Klotho proteins in health and disease. Nat. Rev. Nephrol. 2018, 15, 27–44. [Google Scholar] [CrossRef] [PubMed]
- Dalton, G.D.; Xie, J.; An, S.-W.; Huang, C.-L. New insights into the mechanism of action of soluble Klotho. Front. Endocrinol. 2017, 8. [Google Scholar] [CrossRef] [Green Version]
- Saghiv, M.; Ben Sira, D.; Goldhammer, E.; Sagiv, M. The effects of aerobic and anaerobic exercises on circulating soluble-Klotho and IGF-I in young and elderly adults and in CAD patients. J. Circ. Biomark. 2017, 6, 1849454417733388. [Google Scholar] [CrossRef] [PubMed]
- Morgan, D.; Tsai, S.C. Sleep and the endocrine system. Crit. Care Clin. 2015, 31, 403–418. [Google Scholar] [CrossRef] [PubMed]
- Dote-Montero, M.; Amaro-Gahete, F.J.; De-La-O, A.; Jurado-Fasoli, L.; Gutierrez, A.; Castillo, M.J. Study of the association of DHEAS, testosterone and cortisol with S-Klotho plasma levels in healthy sedentary middle-aged adults. Exp. Gerontol. 2019, 121, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Amaro-Gahete, F.J.; De-La-O, A.; Jurado-Fasoli, L.; Ruiz, J.R.; Castillo, M.J. Association of basal metabolic rate and fuel oxidation in basal conditions and during exercise, with plasma S-klotho: The FIT-AGEING study. Aging 2019, 11, 5319–5333. [Google Scholar] [CrossRef]
- Besedovsky, L.; Lange, T.; Born, J. Sleep and immune function. Pflügers Arch. 2011, 463, 121–137. [Google Scholar] [CrossRef] [Green Version]
- Zhu, L.; Stein, L.R.; Kim, D.; Ho, K.; Yu, G.Q.; Zhan, L.; Larsson, T.E.; Mucke, L. Klotho controls the brain-immune system interface in the choroid plexus. Proc. Natl. Acad. Sci. USA 2018, 115, E11388–E11396. [Google Scholar] [CrossRef] [Green Version]
- Singh, R.; Kiloung, J.; Singh, S.; Sharma, D. Effect of paradoxical sleep deprivation on oxidative stress parameters in brain regions of adult and old rats. Biogerontology 2008, 9, 153–162. [Google Scholar] [CrossRef]
- Patel, S.R.; Zhu, X.; Storfer-Isser, A.; Mehra, R.; Jenny, N.S.; Tracy, R.; Redline, S. Sleep duration and biomarkers of inflammation. Sleep 2009, 32, 200–204. [Google Scholar] [CrossRef] [Green Version]
- Hall, M.H.; Smagula, S.F.; Boudreau, R.M.; Ayonayon, H.N.; Goldman, S.E.; Harris, T.B.; Naydeck, B.L.; Rubin, S.M.; Samuelsson, L.B.; Satterfield, S.; et al. Association between sleep duration and mortality is mediated by markers of inflammation and health in older adults: The health, aging and body composition study. Sleep 2015, 38, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Liguori, I.; Russo, G.; Curcio, F.; Bulli, G.; Aran, L.; Della-Morte, D.; Gargiulo, G.; Testa, G.; Cacciatore, F.; Bonaduce, D.; et al. Oxidative stress, aging, and diseases. Clin. Interv. Aging 2018, 13, 757–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, H.Y.; Kim, D.H.; Lee, E.K.; Chung, K.W.; Chung, S.; Lee, B.; Seo, A.Y.; Chung, J.H.; Jung, Y.S.; Im, E.; et al. Redefining chronic inflammation in aging and age-related diseases: Proposal of the senoinflammation concept. Aging Dis. 2019, 10, 367–382. [Google Scholar] [CrossRef] [Green Version]
- Zuo, L.; Prather, E.R.; Stetskiv, M.; Garrison, D.E.; Meade, J.R.; Peace, T.I.; Zhou, T. Inflammaging and oxidative stress in human diseases: From molecular mechanisms to novel treatments. Int. J. Mol. Sci. 2019, 20, 4472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Royce, G.H.; Brown-Borg, H.M.; Deepa, S.S. The potential role of necroptosis in inflammaging and aging. GeroScience 2019, 41, 795–811. [Google Scholar] [CrossRef]
- Pako, J.; Kunos, L.; Meszaros, M.; Tarnoki, D.L.; Tarnoki, A.D.; Horvath, I.; Bikov, A. Decreased levels of anti-aging klotho in obstructive sleep apnea. Rejuvenation Res. 2020, 23, 256–261. [Google Scholar] [CrossRef]
- Saghiv, M.; Cook, K.; Backes, B.; Frank, S. The effects of partial sleep deprivation and the sub-maximal NDKS exercise testing protocol on S-Klotho and hemodynamic responses in men. Ann. Cardiol. Vasc. Med. 2018, 1, 1006. [Google Scholar] [CrossRef] [Green Version]
- Nakanishi, K.; Nishida, M.; Taneike, M.; Yamamoto, R.; Adachi, H.; Moriyama, T.; Yamauchi-Takihara, K. Implication of alpha-Klotho as the predictive factor of stress. J. Investig. Med. 2019, 67, 1082–1086. [Google Scholar] [CrossRef]
- Amaro-Gahete, F.J.; De-La-O, A.; Jurado-Fasoli, L.; Espuch-Oliver, A.; Robles-Gonzalez, L.; Navarro-Lomas, G.; De Haro, T.; Femia, P.; Castillo, M.J.; Gutierrez, A. Exercise training as S-Klotho protein stimulator in sedentary healthy adults: Rationale, design, and methodology. Contemp. Clin. Trials Commun. 2018, 11, 10–19. [Google Scholar] [CrossRef] [PubMed]
- WHO. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 22 May 2020).
- Migueles, J.H.; Cadenas-Sanchez, C.; Ekelund, U.; Nyström, C.D.; Mora-Gonzalez, J.; Löf, M.; Labayen, I.; Ruiz, J.R.; Ortega, F.B. Accelerometer data collection and processing criteria to assess physical activity and other outcomes: A systematic review and practical considerations. Sports Med. 2017, 47, 1821–1845. [Google Scholar] [CrossRef] [PubMed]
- Van Hees, V.T.; Fang, Z.; Langford, J.; Assah, F.; Mohammad, A.; Da Silva, I.C.M.; Trenell, M.I.; White, T.; Wareham, N.J.; Brage, S. Autocalibration of accelerometer data for free-living physical activity assessment using local gravity and temperature: An evaluation on four continents. J. Appl. Physiol. 2014, 117, 738–744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Hees, V.T.; Sabia, S.; Anderson, K.; Denton, S.J.; Oliver, J.; Catt, M.; Abell, J.; Kivimäki, M.; Trenell, M.I.; Singh-Manoux, A. A novel, open access method to assess sleep duration using a wrist-worn accelerometer. PLoS ONE 2015, 10, e0142533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shrivastava, D.; Jung, S.; Saadat, M.; Sirohi, R.; Crewson, K. How to interpret the results of a sleep study. J. Community Hosp. Intern. Med. Perspect. 2014, 4, 24983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. Neuroimaging 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Mander, B.A.; Winer, J.R.; Walker, M.P. Sleep and human aging. Neuron 2017, 94, 19–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miner, B.; Kryger, M.H. Sleep in the aging population. Sleep Med. Clin. 2016, 12, 31–38. [Google Scholar] [CrossRef] [Green Version]
- Steponenaite, A.; Biello, S.M.; Lall, G.S. Aging clocks: Disrupted circadian rhythms. Aging 2018, 10, 3065–3066. [Google Scholar] [CrossRef]
- Brown, S.A.; Schmitt, K.; Eckert, A. Aging and circadian disruption: Causes and effects. Aging 2011, 3, 813–817. [Google Scholar] [CrossRef] [Green Version]
- Medic, G.; Wille, M.; Hemels, M.E. Short- and long-term health consequences of sleep disruption. Nat. Sci. Sleep 2017, 9, 151–161. [Google Scholar] [CrossRef] [Green Version]
- Bollu, P.C.; Kaur, H. Sleep medicine: Insomnia and sleep. Mo. Med. 2019, 116, 68–75. [Google Scholar]
- Cappuccio, F.P.; D’elia, L.; Strazzullo, P.; Miller, M.A. Sleep duration and all-cause mortality: A systematic review and meta-analysis of prospective studies. Sleep 2010, 33, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Moreno, J.A.; Izquierdo, M.C.; Sanchez-Niño, M.D.; Suárez-Alvarez, B.; Lopez-Larrea, C.; Jakubowski, A.; Blanco, J.; Ramirez, R.; Selgas, R.; Ruiz-Ortega, M.; et al. The inflammatory cytokines TWEAK and TNFα reduce renal klotho expression through NFκB. J. Am. Soc. Nephrol. 2011, 22, 1315–1325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Komaba, H.; Fukagawa, M. Vitamin D and secreted Klotho: A long-awaited panacea for vascular calcification? Kidney Int. 2012, 82, 1248–1250. [Google Scholar] [CrossRef] [Green Version]
- Saito, Y.; Yamagishi, T.; Nakamura, T.; Ohyama, Y.; Aizawa, H.; Suga, T.; Matsumura, Y.; Masuda, H.; Kurabayashi, M.; Kuro-O, M.; et al. Klotho protein protects against endothelial dysfunction. Biochem. Biophys. Res. Commun. 1998, 248, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Chen, K.; Lei, H.; Sun, Z. Klotho gene deficiency causes salt-sensitive hypertension via monocyte chemotactic protein-1/CC chemokine receptor 2–mediated inflammation. J. Am. Soc. Nephrol. 2014, 26, 121–132. [Google Scholar] [CrossRef] [Green Version]
- Grandner, M.A. Epidemiology of Insufficient Sleep and Poor Sleep Quality; Elsevier BV: Amsterdam, The Netherlands, 2019; pp. 11–20. [Google Scholar]
- Ferrie, J.E.; Kumari, M.; Salo, P.; Singh-Manoux, A.; Kivimäki, M. Sleep epidemiology-a rapidly growing field. Int. J. Epidemiol. 2011, 40, 1431–1437. [Google Scholar] [CrossRef] [PubMed]
- Senaratna, C.V.; Perret, J.L.; Lodge, C.J.; Lowe, A.; Campbell, B.; Matheson, M.; Hamilton, G.S.; Dharmage, S.C. Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med. Rev. 2017, 34, 70–81. [Google Scholar] [CrossRef]
- Theorell-Haglöw, J.; Miller, C.; Bartlett, D.J.; Yee, B.J.; Openshaw, H.D.; Grunstein, R.R. Gender differences in obstructive sleep apnoea, insomnia and restless legs syndrome in adults—What do we know? A clinical update. Sleep Med. Rev. 2018, 38, 28–38. [Google Scholar] [CrossRef]
- Hafner, M.; Stepanek, M.; Taylor, J.; Troxel, W.M.; Stolk van, C. Why sleep matters—The economic costs of insufficient sleep: A cross-country comparative analysis. Rand Health Q 2017, 6, 11. [Google Scholar]
- Olesen, J.; Gustavsson, A.; Svensson, M.; Wittchen, H.-U.; Jönsson, B.; on behalf of the CDBE2010 study group; the European Brain Council. The economic cost of brain disorders in Europe. Eur. J. Neurol. 2011, 19, 155–162. [Google Scholar] [CrossRef]
- Reynolds, S.A.; Ebben, M.R. The cost of insomnia and the benefit of increased access to evidence-based treatment. Sleep Med. Clin. 2017, 12, 39–46. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Outcome | N | All | N | Men | N | Women | |||
|---|---|---|---|---|---|---|---|---|---|
| Age (years) | 74 | 53.66 | (5.14) | 35 | 54.39 | (5.27) | 39 | 53.01 | (5.00) |
| Geographical origin of the population (n/%) | 74 | 35 | 39 | ||||||
| Spain | 74 | (100.0) | 35 | (100.0) | 39 | (100.0) | |||
| Place of residence (n/%) | 74 | 35 | 39 | ||||||
| Urban | 63 | (85.1) | 30 | (84.7) | 33 | (84.6) | |||
| Rural | 11 | (14.9) | 5 | (15.3) | 6 | (15.4) | |||
| Socio-professional category (n/%) | 74 | 35 | 39 | ||||||
| Technicians and professional intellectual scientists | 1 | (1.35) | 0 | (0.00) | 1 | (2.56) | |||
| Technicians and associate professionals | 3 | (4.05) | 1 | (2.86) | 2 | (5.13) | |||
| Service and sales workers | 4 | (5.41) | 0 | (0.00) | 4 | (10.26) | |||
| Skilled agricultural, forestry and fishery workers | 43 | (58.11) | 23 | (65.71) | 20 | (51.28) | |||
| Unemployed | 2 | (2.70) | 2 | (5.71) | 0 | (0.00) | |||
| Elementary occupations | 16 | (21.62) | 6 | (17.14) | 10 | (25.64) | |||
| Others | 5 | (6.76) | 3 | (8.58) | 2 | (5.13) | |||
| S-Klotho plasma levels (pg/mL) | 73 | 775.3 | (363.7) | 34 | 814.1 | (452.2) | 39 | 741.4 | (265.6) |
| Antropometry and Body composition | |||||||||
| Height (cm) | 74 | 167.8 | (9.81) | 35 | 175.8 | (6.48) | 39 | 160.7 | (6.10) * |
| Weight (kg) | 74 | 75.73 | (14.98) | 35 | 87.38 | (10.95) | 39 | 65.28 | (9.32) * |
| Body mass index (kg/m2) | 74 | 26.72 | (3.76) | 35 | 28.32 | (3.61) | 39 | 25.27 | (3.31) * |
| Fat mass (%) | 74 | 39.90 | (9.06) | 35 | 34.75 | (7.99) | 39 | 44.52 | (7.36) * |
| Fat mass index (kg/m2) | 74 | 10.75 | (3.13) | 35 | 10.03 | (3.23) | 39 | 11.39 | (2.93) |
| Lean mass index (kg/m2) | 74 | 15.21 | (2.88) | 35 | 17.49 | (2.02) | 39 | 13.17 | (1.80) * |
| Sleep quantity and quality | |||||||||
| Objective sleep quantity and quality | |||||||||
| Total sleep time (min) | 71 | 359.9 | (48.85) | 34 | 340.1 | (47.72) | 37 | 378.1 | (42.88) * |
| Wake after sleep onset (min) | 71 | 63.90 | (27.44) | 34 | 71.28 | (32.70) | 37 | 57.12 | (19.63) * |
| Sleep efficiency (%) | 71 | 85.01 | (6.29) | 34 | 82.89 | (7.41) | 37 | 86.96 | (4.28) * |
| Subjective sleep quantity and quality | |||||||||
| Subjective sleep quality | 67 | 1.13 | (0.82) | 31 | 0.84 | (0.78) | 36 | 1.39 | (0.77) * |
| Sleep latency | 67 | 1.07 | (0.86) | 31 | 1.03 | (0.88) | 36 | 1.11 | (0.85) |
| Sleep duration | 67 | 0.99 | (0.77) | 31 | 0.97 | (0.66) | 36 | 1.00 | (0.86) |
| Habitual sleep efficiency | 67 | 0.60 | (0.95) | 31 | 0.32 | (0.75) | 36 | 0.83 | (1.06) * |
| Sleep disturbances | 67 | 1.13 | (0.42) | 31 | 1.03 | (0.41) | 36 | 1.22 | (0.42) |
| Use of sleeping medication | 67 | 0.31 | (0.76) | 31 | 0.19 | (0.60) | 36 | 0.42 | (0.87) |
| Daytime dysfunction | 67 | 0.37 | (0.55) | 31 | 0.39 | (0.50) | 36 | 0.36 | (0.59) |
| Global PSQI score | 67 | 5.61 | (3.47) | 31 | 4.77 | (3.15) | 36 | 6.33 | (3.62) |
| Model | All | Men | Women | ||||||
|---|---|---|---|---|---|---|---|---|---|
| β | R2 | p | β | R2 | p | β | R2 | p | |
| Total sleep time | |||||||||
| Model 0 | −0.111 | 0.012 | 0.362 | −0.094 | 0.009 | 0.601 | −0.065 | 0.004 | 0.702 |
| Model 1 | −0.057 | 0.482 | <0.001 | −0.033 | 0.657 | <0.001 | 0.102 | 0.419 | <0.001 |
| Model 2 | 0.031 | 0.106 | 0.023 | −0.029 | 0.060 | 0.393 | 0.065 | 0.251 | 0.007 |
| Model 3 | −0.094 | 0.015 | 0.597 | −0.106 | 0.010 | 0.857 | −0.038 | 0.043 | 0.476 |
| Model 4 | 0.137 | 0.356 | <0.001 | −0.069 | 0.722 | <0.001 | 0.162 | 0.549 | <0.001 |
| Wake after sleep onset | |||||||||
| Model 0 | 0.100 | 0.010 | 0.409 | 0.071 | 0.005 | 0.693 | 0.098 | 0.010 | 0.566 |
| Model 1 | 0.108 | 0.491 | <0.001 | −0.028 | 0.656 | <0.001 | 0.156 | 0.433 | <0.001 |
| Model 2 | −0.012 | 0.106 | 0.024 | −0.007 | 0.060 | 0.398 | 0.036 | 0.248 | 0.008 |
| Model 3 | 0.083 | 0.014 | 0.633 | 0.082 | 0.006 | 0.912 | 0.083 | 0.048 | 0.433 |
| Model 4 | −0.054 | 0.343 | <0.001 | 0.002 | 0.717 | <0.001 | 0.036 | 0.526 | <0.001 |
| Sleep efficiency | |||||||||
| Model 0 | −0.099 | 0.010 | 0.413 | −0.062 | 0.004 | 0.732 | −0.103 | 0.011 | 0.544 |
| Model 1 | −0.107 | 0.491 | <0.001 | 0.013 | 0.656 | <0.001 | −0.108 | 0.421 | <0.001 |
| Model 2 | 0.035 | 0.106 | 0.023 | 0.020 | 0.060 | 0.396 | −0.011 | 0.247 | 0.008 |
| Model 3 | −0.081 | 0.013 | 0.644 | −0.073 | 0.005 | 0.932 | −0.080 | 0.048 | 0.436 |
| Model 4 | 0.093 | 0.348 | <0.001 | −0.004 | 0.717 | <0.001 | 0.000 | 0.525 | <0.001 |
| Model | All | Men | Women | ||||||
|---|---|---|---|---|---|---|---|---|---|
| β | R2 | p | β | R2 | p | β | R2 | p | |
| Subjective sleep quality | |||||||||
| Model 0 | −0.368 | 0.135 | 0.002 | −0.351 | 0.123 | 0.057 | −0.412 | 0.170 | 0.013 |
| Model 1 | −0.275 | 0.573 | <0.001 | −0.146 | 0.633 | <0.001 | −0.318 | 0.599 | <0.001 |
| Model 2 | −0.250 | 0.191 | 0.001 | −0.302 | 0.166 | 0.087 | −0.188 | 0.399 | <0.001 |
| Model 3 | −0.349 | 0.139 | 0.009 | −0.354 | 0.124 | 0.168 | −0.334 | 0.224 | 0.015 |
| Model 4 | −0.131 | 0.332 | <0.001 | −0.063 | 0.696 | <0.001 | −0.195 | 0.535 | <0.001 |
| Sleep latency | |||||||||
| Model 0 | −0.519 | 0.269 | <0.001 | −0.565 | 0.319 | 0.001 | −0.483 | 0.234 | 0.003 |
| Model 1 | −0.350 | 0.611 | <0.001 | −0.354 | 0.726 | <0.001 | −0.319 | 0.594 | <0.001 |
| Model 2 | −0.451 | 0.331 | <0.001 | −0.528 | 0.336 | 0.004 | −0.335 | 0.473 | <0.001 |
| Model 3 | −0.505 | 0.275 | <0.001 | −0.572 | 0.322 | 0.005 | −0.432 | 0.304 | 0.003 |
| Model 4 | −0.384 | 0.453 | <0.001 | −0.196 | 0.722 | <0.001 | −0.295 | 0.581 | <0.001 |
| Sleep duration | |||||||||
| Model 0 | −0.140 | 0.020 | 0.261 | −0.153 | 0.023 | 0.420 | −0.147 | 0.021 | 0.394 |
| Model 1 | −0.101 | 0.509 | <0.001 | −0.091 | 0.622 | <0.001 | −0.113 | 0.512 | <0.001 |
| Model 2 | −0.119 | 0.156 | 0.005 | −0.107 | 0.091 | 0.277 | −0.163 | 0.397 | <0.001 |
| Model 3 | −0.136 | 0.046 | 0.228 | −0.152 | 0.023 | 0.726 | −0.162 | 0.150 | 0.068 |
| Model 4 | −0.095 | 0.328 | <0.001 | 0.015 | 0.693 | <0.001 | −0.128 | 0.518 | <0.001 |
| Habitual sleep efficiency | |||||||||
| Model 0 | −0.277 | 0.077 | 0.024 | −0.443 | 0.197 | 0.014 | −0.140 | 0.020 | 0.414 |
| Model 1 | −0.209 | 0.542 | <0.001 | −0.252 | 0.673 | <0.001 | −0.087 | 0.507 | <0.001 |
| Model 2 | −0.215 | 0.186 | 0.002 | −0.424 | 0.258 | 0.018 | −0.123 | 0.385 | <0.001 |
| Model 3 | −0.282 | 0.107 | 0.028 | −0.451 | 0.202 | 0.048 | −0.177 | 0.155 | 0.062 |
| Model 4 | −0.065 | 0.322 | <0.001 | −0.064 | 0.696 | <0.001 | 0.010 | 0.502 | <0.001 |
| Sleep disturbances | |||||||||
| Model 0 | −0.407 | 0.165 | 0.001 | −0.445 | 0.198 | 0.014 | −0.376 | 0.141 | 0.024 |
| Model 1 | −0.125 | 0.511 | <0.001 | −0.070 | 0.617 | <0.001 | −0.057 | 0.502 | <0.001 |
| Model 2 | −0.335 | 0.247 | <0.001 | −0.408 | 0.241 | 0.024 | −0.301 | 0.459 | <0.001 |
| Model 3 | −0.400 | 0.187 | 0.001 | −0.445 | 0.198 | 0.051 | −0.396 | 0.280 | 0.004 |
| Model 4 | −0.207 | 0.354 | <0.001 | −0.131 | 0.707 | <0.001 | −0.129 | 0.516 | <0.001 |
| Use of sleeping medication | |||||||||
| Model 0 | −0.150 | 0.023 | 0.229 | −0.378 | 0.143 | 0.039 | 0.062 | 0.004 | 0.720 |
| Model 1 | −0.158 | 0.523 | <0.001 | −0.228 | 0.663 | <0.001 | −0.010 | 0.500 | <0.001 |
| Model 2 | −0.088 | 0.149 | 0.006 | −0.323 | 0.175 | 0.074 | 0.069 | 0.375 | <0.001 |
| Model 3 | −0.143 | 0.048 | 0.214 | −0.378 | 0.143 | 0.125 | 0.051 | 0.127 | 0.107 |
| Model 4 | 0.009 | 0.319 | <0.001 | 0.103 | 0.700 | <0.001 | 0.135 | 0.520 | <0.001 |
| Daytime dysfunction | |||||||||
| Model 0 | −0.211 | 0.045 | 0.089 | −0.335 | 0.112 | 0.071 | −0.102 | 0.010 | 0.555 |
| Model 1 | −0.137 | 0.517 | <0.001 | −0.234 | 0.668 | <0.001 | −0.044 | 0.502 | <0.001 |
| Model 2 | −0.188 | 0.177 | 0.002 | −0.381 | 0.222 | 0.034 | 0.074 | 0.375 | <0.001 |
| Model 3 | −0.206 | 0.070 | 0.103 | −0.353 | 0.121 | 0.176 | −0.025 | 0.125 | 0.111 |
| Model 4 | −0.161 | 0.344 | <0.001 | −0.169 | 0.720 | <0.001 | 0.007 | 0.502 | <0.001 |
| Global PSQI score | |||||||||
| Model 0 | −0.438 | 0.192 | <0.001 | −0.563 | 0.317 | 0.001 | −0.323 | 0.104 | 0.055 |
| Model 1 | −0.304 | 0.587 | <0.001 | −0.323 | 0.704 | <0.001 | −0.209 | 0.542 | <0.001 |
| Model 2 | −0.355 | 0.255 | <0.001 | −0.525 | 0.339 | 0.004 | −0.197 | 0.407 | <0.001 |
| Model 3 | −0.423 | 0.204 | 0.001 | −0.563 | 0.317 | 0.006 | −0.292 | 0.208 | 0.021 |
| Model 4 | −0.236 | 0.364 | <0.001 | −0.131 | 0.704 | <0.001 | −0.118 | 0.515 | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mochón-Benguigui, S.; Carneiro-Barrera, A.; Castillo, M.J.; Amaro-Gahete, F.J. Is Sleep Associated with the S-Klotho Anti-Aging Protein in Sedentary Middle-Aged Adults? The FIT-AGEING Study. Antioxidants 2020, 9, 738. https://doi.org/10.3390/antiox9080738
Mochón-Benguigui S, Carneiro-Barrera A, Castillo MJ, Amaro-Gahete FJ. Is Sleep Associated with the S-Klotho Anti-Aging Protein in Sedentary Middle-Aged Adults? The FIT-AGEING Study. Antioxidants. 2020; 9(8):738. https://doi.org/10.3390/antiox9080738
Chicago/Turabian StyleMochón-Benguigui, Sol, Almudena Carneiro-Barrera, Manuel J. Castillo, and Francisco J. Amaro-Gahete. 2020. "Is Sleep Associated with the S-Klotho Anti-Aging Protein in Sedentary Middle-Aged Adults? The FIT-AGEING Study" Antioxidants 9, no. 8: 738. https://doi.org/10.3390/antiox9080738
APA StyleMochón-Benguigui, S., Carneiro-Barrera, A., Castillo, M. J., & Amaro-Gahete, F. J. (2020). Is Sleep Associated with the S-Klotho Anti-Aging Protein in Sedentary Middle-Aged Adults? The FIT-AGEING Study. Antioxidants, 9(8), 738. https://doi.org/10.3390/antiox9080738