Emerging Nanotechnology in Non-Surgical Periodontal Therapy in Animal Models: A Systematic Review



Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol
- Participants/population: animals with experimental periodontitis
- Intervention/exposure: use of nanoparticles systems as non-surgical periodontal therapy (i.e., injected in the periodontal pocket without involving incisions and flap elevation)
- Comparator/control: untreated animals
- Outcome: decrease of alveolar bone loss
2.2. Search Strategy for the Identification of the Studies
2.3. Eligibility Criteria
2.4. Outcome Measures
2.5. Data Extraction and Analysis
2.6. Study Quality Assessment
3. Results
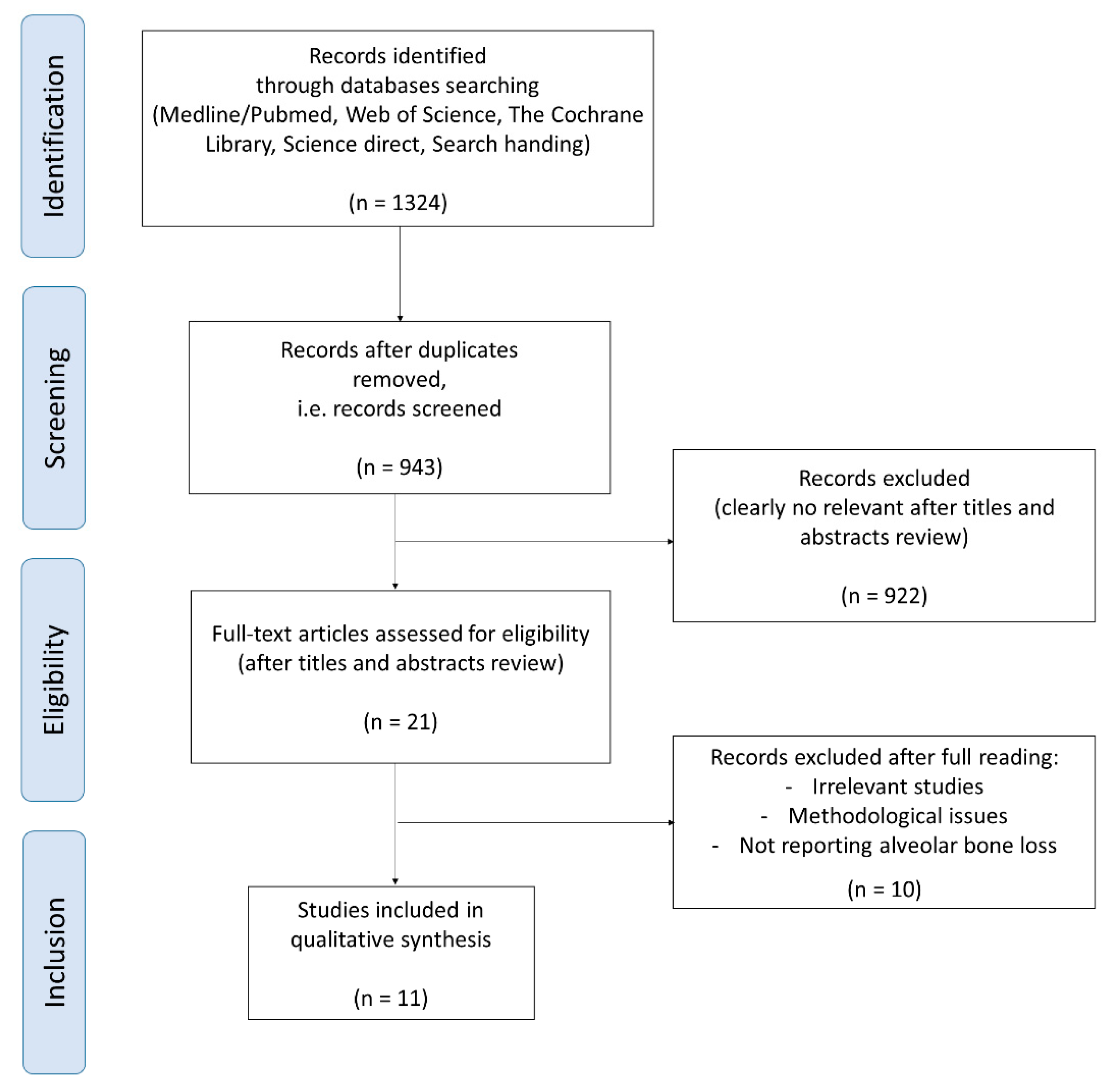
3.1. Study Selection
3.2. Characteristics of the Included Studies
3.3. Nanoparticles Type
3.4. Reported Outcomes
3.5. Main Results
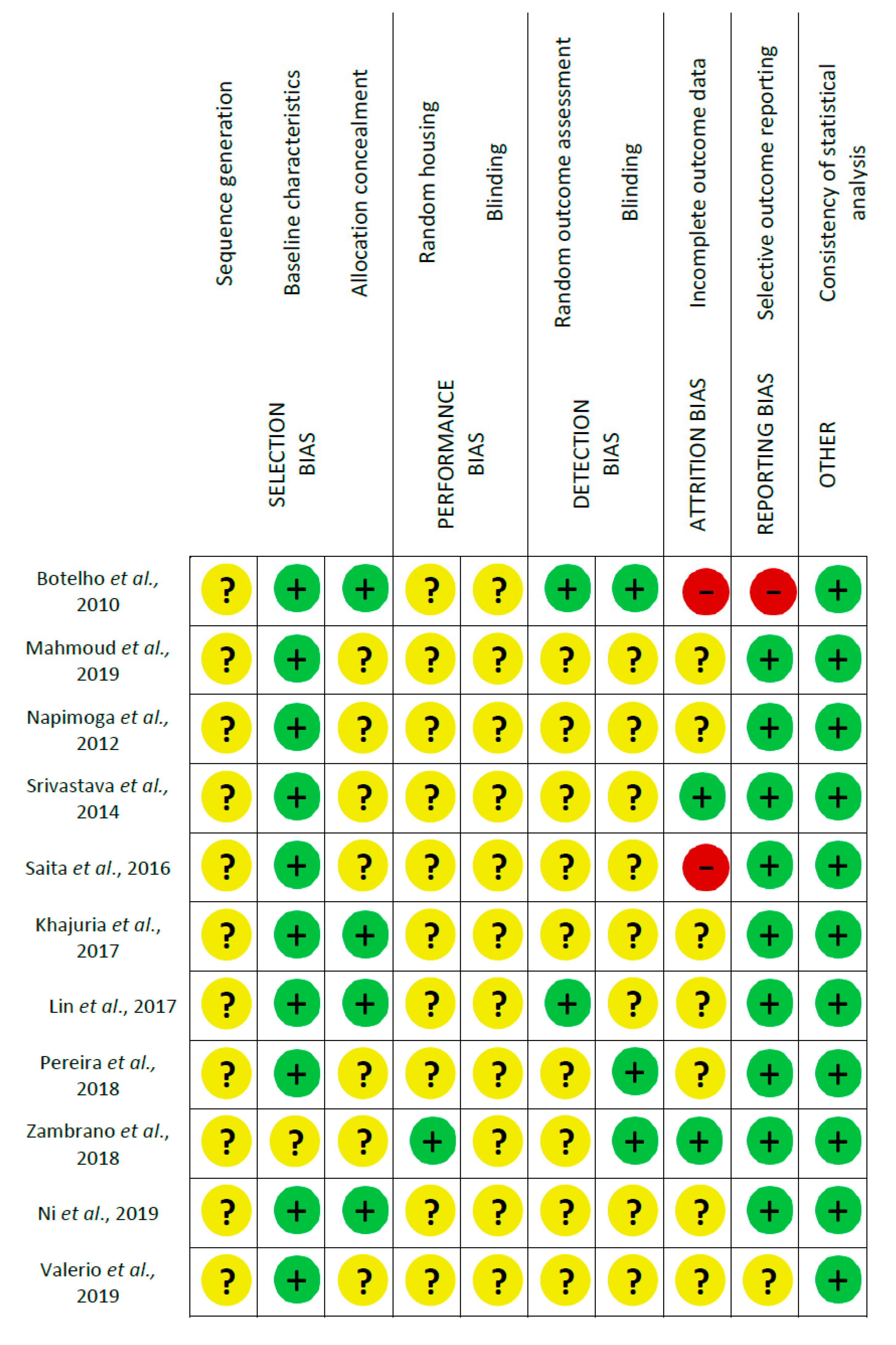
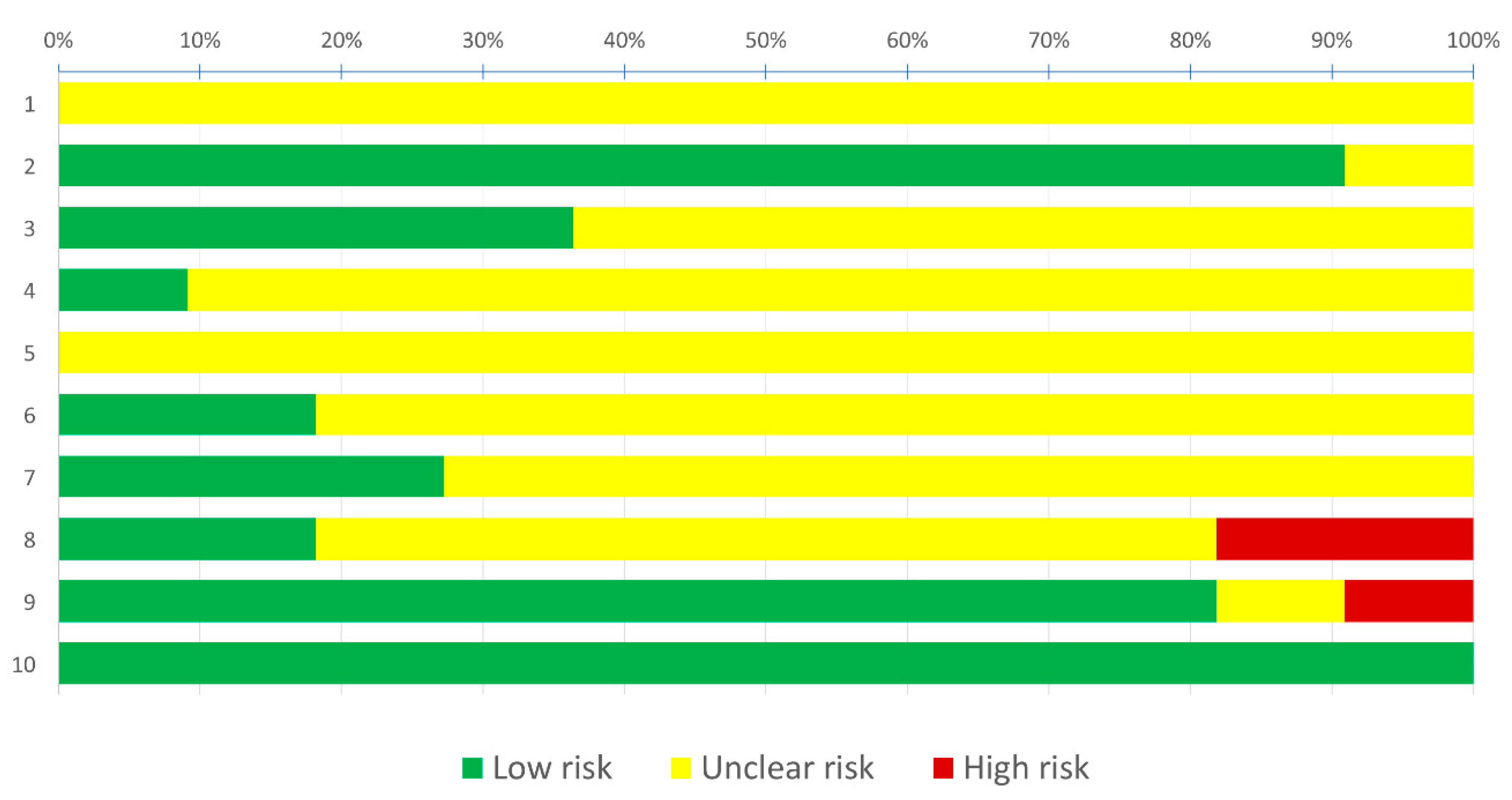
3.6. Risk of Bias Assessment
4. Discussion
4.1. Application of Nanotechnology in Periodontology
4.2. Nanotechnologies and Antibacterial Agents
4.3. Nanotechnologies and Host Modulation Therapies
4.4. Toxicity
4.5. Methodological Heterogeneity and Limitations
4.6. Risk of Bias
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.L.; Marcenes, W. Global burden of severe periodontitis in 1990-2010: A systematic review and meta-regression. J. Dent. Res. 2014, 93, 1045–1053. [Google Scholar] [CrossRef] [PubMed]
- Hajishengallis, G.; Lamont, R.J. Beyond the red complex and into more complexity: The polymicrobial synergy and dysbiosis (PSD) model of periodontal disease etiology. Mol. Oral Microbiol. 2012, 27, 409–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savage, A.; Eaton, K.A.; Moles, D.R.; Needleman, I. A systematic review of definitions of periodontitis and methods that have been used to identify this disease. J. Clin. Periodontol. 2009, 36, 458–467. [Google Scholar] [CrossRef] [PubMed]
- Smiley, C.J.; Tracy, S.L.; Abt, E.; Michalowicz, B.S.; John, M.T.; Gunsolley, J.; Cobb, C.M.; Rossmann, J.; Harrel, S.K.; Forrest, J.L.; et al. Systematic review and meta-analysis on the nonsurgical treatment of chronic periodontitis by means of scaling and root planing with or without adjuncts. J. Am. Dent. Assoc. 2015, 146, 508–524. [Google Scholar] [CrossRef]
- Haffajee, A.D.; Cugini, M.A.; Dibart, S.; Smith, C.; Kent, R.L.; Socransky, S.S. The effect of SRP on the clinical and microbiological parameters of periodontal diseases. J. Clin. Periodontol. 1997, 24, 324–334. [Google Scholar] [CrossRef]
- Graziani, F.; Karapetsa, D.; Alonso, B.; Herrera, D. Nonsurgical and surgical treatment of periodontitis: How many options for one disease? Periodontology 2000 2017, 75, 152–188. [Google Scholar] [CrossRef]
- Herrera, D.; Matesanz, P.; Bascones-Martínez, A.; Sanz, M. Local and Systemic Antimicrobial Therapy in Periodontics. J. Evid. Based Dent. Pract. 2012, 12, 50–60. [Google Scholar] [CrossRef]
- Keestra, J.A.J.; Grosjean, I.; Coucke, W.; Quirynen, M.; Teughels, W. Non-surgical periodontal therapy with systemic antibiotics in patients with untreated aggressive periodontitis: A systematic review and meta-analysis. J. Periodontal Res. 2015, 50, 689–706. [Google Scholar] [CrossRef]
- Keestra, J.A.J.; Grosjean, I.; Coucke, W.; Quirynen, M.; Teughels, W. Non-surgical periodontal therapy with systemic antibiotics in patients with untreated chronic periodontitis: A systematic review and meta-analysis. J. Periodontal Res. 2015, 50, 294–314. [Google Scholar] [CrossRef]
- Maestre, J.R.; Bascones, A.; Sánchez, P.; Matesanz, P.; Aguilar, L.; Giménez, M.J.; Pérez-Balcabao, I.; Granizo, J.J.; Prieto, J. Odontogenic bacteria in periodontal disease and resistance patterns to common antibiotics used as treatment and prophylaxis in odontology in Spain. Rev. Esp. Quimioter. 2007, 20, 61–67. [Google Scholar]
- Da Rocha, H.A.J.; Silva, C.F.; Santiago, F.L.; Martins, L.G.; Dias, P.C.; De Magalhães, D. Local Drug Delivery Systems in the Treatment of Periodontitis: A Literature Review. J. Int. Acad. Periodontol. 2015, 17, 82–90. [Google Scholar]
- Qin, Y.; Yuan, M.; Li, L.; Li, W.; Xue, J. Formulation and evaluation of in situ forming PLA implant containing tinidazole for the treatment of periodontitis. J. Biomed. Mater. Res. B 2012, 100, 2197–2202. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Pini-Prato, G.; Cortellini, P. Principles and clinical applications of periodontal controlled drug delivery with tetracycline fibers. Int. J. Periodontics Restorative Dent. 1994, 14, 421–435. [Google Scholar] [PubMed]
- Food and Drug Administration. Considering Whether an FDA-Regulated Product Involves the Application of Nanotechnology; FDA: Washington, DC, USA, 2014. [Google Scholar]
- Duncan, R. The dawning era of polymer therapeutics. Nat. Rev. Drug Discov. 2003, 2, 347–360. [Google Scholar] [CrossRef]
- Bapat, R.A.; Joshi, C.P.; Bapat, P.; Chaubal, T.V.; Pandurangappa, R.; Jnanendrappa, N.; Gorain, B.; Khurana, S.; Kesharwani, P. The use of nanoparticles as biomaterials in dentistry. Drug Discov. Today 2019, 24, 85–98. [Google Scholar] [CrossRef] [PubMed]
- Yadav, S.K.; Khan, G.; Mishra, B. Advances in patents related to intrapocket technology for the management of periodontitis. Recent Pat. Drug Deliv. Formul. 2015, 9, 129–145. [Google Scholar] [CrossRef]
- Patravale, V.B.; Date, A.A.; Kulkarni, R.M. Nanosuspensions: A promising drug delivery strategy. J. Pharm. Pharmacol. 2004, 56, 827–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pragati, S.; Ashok, S.; Kuldeep, S. Recent advances in periodontal drug delivery systems. Int. J. Drug Deliv. 2011, 1, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Brun, A.; Moignot, N.; Colombier, M.L.; Dursun, E. Towards the nano-control of periodontal inflammation? Oral Dis. 2019, 26, 245–248. [Google Scholar] [CrossRef]
- Carrouel, F.; Viennot, S.; Ottolenghi, L.; Gaillard, C.; Bourgeois, D. Nanoparticles as anti-microbial, anti-inflammatory, and remineralizing agents in oral care cosmetics: A review of the current situation. Nanomaterials 2020, 10, 140. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 62, e1–e34. [Google Scholar] [CrossRef] [Green Version]
- Stone, P.W. Popping the (PICO) question in research and evidence-based practice. Appl. Nurs. Res. 2002, 15, 197–198. [Google Scholar] [CrossRef]
- Hooijmans, C.R.; Rovers, M.M.; de Vries, R.B.; Leenaars, M.; Ritskes-Hoitinga, M.; Langendam, M.W. SYRCLE’s risk of bias tool for animal studies. BMC Med. Res. Methodol. 2014, 14, 43. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Botelho, M.A.; Martins, J.G.; Ruela, R.S.; Queiroz, D.B.; Ruela, W.S. Nanotechnology in ligature-induced periodontitis: Protective effect of a doxycycline gel with nanoparticules. J. Appl. Oral Sci. 2010, 18, 335–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahmoud, M.Y.; Steinbach-Rankins, J.M.; Demuth, D.R. Functional assessment of peptide-modified PLGA nanoparticles against oral biofilms in a murine model of periodontitis. J. Control. Release 2019, 297, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Napimoga, M.H.; da Silva, C.A.T.; Carregaro, V.; Farnesi-de-Assunção, T.S.; Duarte, P.M.; de Melo, N.F.S.; Fraceto, L.F. Exogenous Administration of 15d-PGJ 2 –Loaded Nanocapsules Inhibits Bone Resorption in a Mouse Periodontitis Model. J. Immunol. 2012, 189, 1043–1052. [Google Scholar] [CrossRef] [Green Version]
- Srivastava, M.; Neupane, Y.R.; Kumar, P.; Kohli, K. Nanoemulgel (NEG) of Ketoprofen with eugenol as oil phase for the treatment of ligature-induced experimental periodontitis in Wistar rats. Drug Deliv. 2014, 23, 2228–2234. [Google Scholar] [CrossRef]
- Saita, M.; Kaneko, J.; Sato, T.; Takahashi, S.; Wada-Takahashi, S.; Kawamata, R.; Sakurai, T.; Lee, M.-C.; Hamada, N.; Kimoto, K.; et al. Novel antioxidative nanotherapeutics in a rat periodontitis model: Reactive oxygen species scavenging by redox injectable gel suppresses alveolar bone resorption. Biomaterials 2016, 76, 292–301. [Google Scholar] [CrossRef]
- Khajuria, D.K.; Zahra, S.F.; Razdan, R. Effect of locally administered novel biodegradable chitosan based risedronate/zinc-hydroxyapatite intra-pocket dental film on alveolar bone density in rat model of periodontitis. J. Biomater. Sci. Polym. Ed. 2017, 29, 74–91. [Google Scholar] [CrossRef] [PubMed]
- De Pereira, A.S.B.F.; de Brito, G.A.C.; de Lima, M.L.S.; da Silva Júnior, A.A.; Silva, E.D.S.; de Rezende, A.A.; Bortolin, R.H.; Galvan, M.; Pirih, F.Q.; de Araújo Júnior, R.F.; et al. Metformin Hydrochloride-Loaded PLGA Nanoparticle in Periodontal Disease Experimental Model Using Diabetic Rats. Int. J. Mol. Sci. 2018, 19, 3488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zambrano, L.M.G.; Brandao, D.A.; Rocha, F.R.G.; Marsiglio, R.P.; Longo, I.B.; Primo, F.L.; Tedesco, A.C.; Guimaraes-Stabili, M.R.; Rossa Junior, C. Local administration of curcumin-loaded nanoparticles effectively inhibits inflammation and bone resorption associated with experimental periodontal disease. Sci. Rep. 2018, 8, 6652. [Google Scholar] [CrossRef]
- Ni, C.; Zhou, J.; Kong, N.; Bian, T.; Zhang, Y.; Huang, X.; Xiao, Y.; Yang, W.; Yan, F. Gold nanoparticles modulate the crosstalk between macrophages and periodontal ligament cells for periodontitis treatment. Biomaterials 2019, 206, 115–132. [Google Scholar] [CrossRef]
- Valerio, M.S.; Alexis, F.; Kirkwood, K.L. Functionalized nanoparticles containing MKP-1 agonists reduce periodontal bone loss. J. Periodontol. 2019, 90, 894–902. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.-H.; Feng, F.; Yu, M.-C.; Wang, C.-H.; Chang, P.-C. Modulation of periodontitis progression using pH-responsive nanosphere encapsulating metronidazole or N-phenacylthialzolium bromide. J. Periodontal Res. 2017, 53, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Cafferata, E.A.; Alvarez, C.; Diaz, K.T.; Maureira, M.; Monasterio, G.; González, F.E.; Covarrubias, C.; Vernal, R. Multifunctional nanocarriers for the treatment of periodontitis: Immunomodulatory, antimicrobial, and regenerative strategies. Oral Dis. 2019, 25, 1866–1878. [Google Scholar] [CrossRef]
- Zenobia, C.; Hajishengallis, G. Basic biology and role of interleukin-17 in immunity and inflammation. Periodontology 2000 2015, 69, 142–159. [Google Scholar] [CrossRef]
- Golub, L.M.; McNamara, T.F.; Ryan, M.E.; Kohut, B.; Blieden, T.; Payonk, G.; Sipos, T.; Baron, H.J. Adjunctive treatment with subantimicrobial doses of doxycycline: Effects on gingival fluid collagenase activity and attachment loss in adult periodontitis. J. Clin. Periodontol. 2001, 28, 146–156. [Google Scholar] [CrossRef]
- Bartold, P.M.; Van Dyke, T.E. Host modulation: Controlling the inflammation to control the infection. Periodontology 2000 2017, 75, 317–329. [Google Scholar] [CrossRef]
- Hajishengallis, G. Periodontitis: From microbial immune subversion to systemic inflammation. Nat. Rev. Immunol. 2014, 15, 30–44. [Google Scholar] [CrossRef]
- White, P.C.; Chicca, I.J.; Cooper, P.R.; Milward, M.R.; Chapple, I.L. Neutrophil extracellular traps in periodontitis: A web of intrigue. J. Dent. Res. 2016, 95, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Preshaw, P.M. Host modulation therapy with anti-inflammatory agents. Periodontology 2000 2018, 76, 131–149. [Google Scholar] [CrossRef]
- Fröhlich, E.; Roblegg, E. Oral uptake of nanoparticles: Human relevance and the role of in vitro systems. Arch. Toxicol. 2016, 90, 2297–2314. [Google Scholar] [CrossRef] [PubMed]
- Buzea, C.; Pacheco, I.I.; Robbie, K. Nanomaterials and nanoparticles: Sources and toxicity. Biointerphases 2007, 2, MR17–MR71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, X.; Chen, A.; Zhang, Y.; Wang, J.; Shao, L.; Wei, L. Application of dental nanomaterials: Potential toxicity to the central nervous system. Int. J. Nanomed. 2015, 10, 3547–3565. [Google Scholar] [CrossRef] [Green Version]
- Monteiro-Riviere, N.A.; Inman, A.O.; Zhang, L.W. Limitations and relative utility of screening assays to assess engineered nanoparticle toxicity in a human cell line. Toxicol. Appl. Pharmacol. 2009, 234, 222–235. [Google Scholar] [CrossRef]
- De Molon, R.S.; de Avila, E.D.; Boas Nogueira, A.V.; Chaves de Souza, J.A.; Avila-Campos, M.J.; de Andrade, C.R.; Cirelli, J.A. Evaluation of the Host Response in Various Models of Induced Periodontal Disease in Mice. J. Periodontol. 2014, 85, 465–477. [Google Scholar] [CrossRef]
- Nakada, T.; Kato, T.; Numabe, Y. Effects of fatigue from sleep deprivation on experimental periodontitis in rats. J. Periodontal Res. 2015, 50, 131–137. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Treatment Type | Authors, Year | Drug Tested | Study Design/Models | Measures | Objectives | Main Results |
|---|---|---|---|---|---|---|
| Antibacterial agent | Botelho et al., 2010 [26] | Nanostructured doxycycline gel | Experimental periodontitis (EPD) in rats induced by ligatures. 4 groups (n = 6/group): naïve (no EPD), non-treated (NT), vehicle gel (VG), and DOX | Macroscopic evaluation | Test the efficacy of a locally applied 8.5% nanostructured doxycycline (DOX) gel in preventing alveolar bone loss (ABL) | After 11 days DOX gel reduced the ABL (0.1 mm), compared to the NT (0.7 mm) (p < 0.05) and the VG groups (0.4 mm) After 6 h, MPO activity in DOX group (8.5 U/mg) was reduced (p < 0.05) compared to NT group (36 U/mg) AFM showed several grooves were observed on the surface of the alveolar bone and other periodontal structures in the NT and VG groups, with significantly greater depths compared to the DOX group (p < 0.05) |
| Histopathological analysis | ||||||
| Myeloperoxydase (MPO) | ||||||
| Atomic force microscopy (AFM) | ||||||
| Mahmoud et al., 2019 [27] | BAR-modified nanoparticles (BNP) of poly(lactic-co-glycolic acid) (PLGA) | Experimental periodontitis in mice induced by oral delivering of S. gordonii and P. gingivalis 7 groups (n = 8/group): control (without infection), S. gordonii only, P. gingivalis only, 0.7 µM BAR, 3.4 µM BAR, 0.7 BNP | Dissecting microscope fitted with a video imaging marker measurement system | Determine the efficacy of BNP by inhibiting the adhesion of P. gingivalis to S. gordonii | Treatment of P. gingivalis/S. gordonii infected mice with BNPs reduced bone loss (−0.24 ± 0.05 mm) compare to sham-infected mice (−1.37 ± 0.31 mm, p ≤ 0.0001) and to a greater extent than treatment with 0.7 or 3.4 μM free BAR (−0.69 ± 0.1mm, −0.56 ± 0.09mm, p ≤ 0.0001) BNP also reduced IL-17 expression almost to the levels of sham-infected mice, whereas the gingival tissue of P. gingivalis/S. gordonii infected mice and mice treated with 0.7 µM free BAR demonstrated a statistically significant increase in IL-17 gingival tissue fluorescence (≈2 fold more) compared to uninfected mice (p ≤ 0.0001 and p ≤ 0.01 respectively) | |
| Histological and immunofluorescence assessment | ||||||
| Anti-inflammatory agent | Napimoga et al., 2012 [28] | 15d-PGJ2-loaded poly (D,L-lactide-coglycolide) (PLGA) nanocapsules (NC) | Experimental periodontitis in mice induced by oral delivering of A. actinomycetemcomitans JP2 with a micropipette 3 groups (n = 5/group): uninfected, infected and saline, infected and 15d-PGJ2-NC | Dissecting microscope | Test the efficacy of PLGA nanocapsules loaded with 15d-PGJ2 in bone loss and immunoinflammatory responses | After 15 days: The treatment by 15d-PGJ2 NC at 10 µg/kg showed significantly lower ABL (0.07 mm) compared to infected and saline group (0.12 mm) (p < 0.05) The gingival tissues of 15d-PGJ2 NC treated group showed significantly: lower submandibular lymph nodes infiltration by lymphocytes (CD4, CD8) (p < 0.05), lower RANK-L and mRNA (IL-17, IL-6, FOXP3, CCL-22, IL-10, TGF-ß) expression and MPO activity compared to PBS group (p < 0.05) and higher CD55 expression and 15d-PGJ2 amount compared to PBS group (p < 0.05) No significant differences between 15d-PGJ2-NC and infected and saline groups were shown, in terms of IgG anti-A. actinomycetemcomitans production, OPG, IL-15 mRNA expression |
| Elisa immunoassays | ||||||
| Histomorphometrical assessments | ||||||
| Flow cytometry analysis | ||||||
| Spectrophotometry measurement | ||||||
| Western-blotting | ||||||
| RT-PCR | ||||||
| Srivastava et al., 2014 [29] | Nanoemulgel (NEG) of ketoprofen (KP) containing eugenol | Experimental periodontitis (EPD) in rats induced by ligatures 4 groups (n = 6/group): control (no EPD), ligature only, NEG and ligature, KP loaded NEG and ligatures (NEG + KP) | Evaluation of clinical periodontal parameters: gingival index (GI), tooth mobility (TM) | Assess the efficacy of KP loaded NEG containing eugenol | After 11 days: The NEG+KP treatment showed significantly lower ABL (0.14 mm) compared to the ligature only group (0.68 mm) (p < 0,05) The NEG+KP treatment also showed significantly lower GI, TM (p < 0,05) and cytokines expression (IL-1β, TNF-α) Histopathology of the periodontium showed a reduced inflammatory cell infiltration, alveolar bone and cementum resorption for the NEG + KP group, in comparison with ligature only group AFM showed a reduction of roughness of alveolar bone surface in the NEG+KP group, in comparison with ligature only group | |
| Histopathological assessment | ||||||
| Elisa immunoassays | ||||||
| Dissecting microscope | ||||||
| Atomic force microscopy | ||||||
| Saita et al., 2016 [30] | Redox injectable gel (RIG) from nitroxide radicals containing polyion complex (PIC) flower micelles | Experimental periodontitis in rats induced by oral delivering of P. gingivalis 4 groups (n = 14/group): control (sham, without infection), P. gingivalis, noRIG+P. gingivalis (radical without nitroxide), RIG+P. gingivalis | Gingival blood flow measure | Evaluate the ROS-scavenging antioxidant-related anti-inflammatory and anti-P. gingivalis induced bone loss effects of the RIG | After 21 days: The amount of ABL was significantly lower in the RIG+P. gingivalis group (0.341 ± 0.035 mm) and control group (0.310 ± 0.026 mm) than in the P. gingivalis (0.479 ± 0.038 mm) and nRIG+P. gingivalis groups (0.470 ± 0.036 mm) (p < 0.01, n = 6) The gingival blood flow rate was significantly decreased in P. gingivalis and noRIG+P. gingivalis rats compared to the sham group (p < 0.05), while the RIG+P. gingivalis rats retained the same level of gingival blood flow as that of the control (sham) rats (n = 3) noRIG did not effectively suppress oxidative stress induced by P. gingivalis, while the MDA levels in the RIG group were consistent with significant suppression of oxidative stress at day 21 (p < 0.05, n = 4) No significant changes were observed in the levels of IL-1β and IL-6 The number of osteoclasts (TRAP) in the P. gingivalis and noRIG+P. gingivalis groups was significantly higher than that observed in the control and RIG+P. gingivalis groups (p < 0.001, n = 6) | |
| Histological assessment | ||||||
| Elisa immunoassays | ||||||
| µCT (computed tomography) analysis | ||||||
| Khajuria et al., 2017 [31] | Chitosan-based risedronate/zinc-hydroxyapatite nanoparticles intrapocket dental film (CRZHDF) | Experimental periodontitis in rats induced by gingival injections of P. gingivalis-LPS 5 groups (n = 12/group): healthy, untreated periodontitis, periodontitis + CRZHDF-0.1, periodontitis + CRZHDF-0.2, periodontitis + chitosan film | Elisa immunoassays | Develop a CRZHDF for applications in the treatment of ABL | CRZHDF reversed alveolar bone resorption (ABL: CRZHDF-0.1: 19.23 ± 0.61 mm; CRZHDF-0.2: 21.61 ± 0.38 mm) when compared to the untreated periodontitis group (ABL: 38.10 ± 0.88mm) (p < 0.001) CRZHDF also resulted in significant improvements in the mesial and distal periodontal bone support proportions (%) and bone mineral density b-ALP activity and TRACP 5b were lower in CRZHDF groups compared to the untreated periodontitis group (p < 0.0001) The expression of OCN was higher in CRZHDF groups compared to the untreated periodontitis group (p < 0.0001) | |
| µCT analysis | ||||||
| Histological assessment | ||||||
| Pereira et al., 2018 [32] | Metformin hydrochloride-loaded nanoparticles poly(D,L-lactide-co-glycolide) (MET-loaded PLGA) | Experimental periodontitis (PD) in diabetes (DM) rats induced by ligatures 9 groups (n = 20/group): sham (without DM, without PD), PD without DM, DM without PD, positive control with PD and DM, PLGA control with PD and DM (n = 6), Met50, Met100, MET-loaded PLGA 100, MET-loaded PLGA 10 | Elisa immunoassays | Evaluate the effect of MET-loaded PLGA | After 11 days: Bone loss was reduced when comparing positive control (0.97 ± 0.35 mm) to PLGA 10 mg/kg MET treatment (0.65 ± 0.14 mm) (non-significant) Treatment with MET-loaded PLGA 10 mg/kg showed: low inflammatory cells; weak staining by RANKL, cathepsin K, OPG, and OCN; reduced levels of IL-1β and TNF-α; increased AMPK expression gene; and decreased of NF-KB p65, HMGB1 and TAK-1 (p < 0.05) | |
| qRT-PCR | ||||||
| Histopathological and immunohistochemical assessment | ||||||
| µCT analysis | ||||||
| Zambrano et al., 2018 [33] | Polylactic and polyglycolic acids nanoparticles (NP) loaded with curcumin | Experimental periodontitis in rat induced by gingival injections of E.Coli-LPS 4 groups (n = 4/group): PBS-empty NP, LPS-empty NP, PBS-curcumin NP, LPS-curcumin NP | µCT analysis | Assess the biological effect of the local administration of curcumin in a nanoparticle vehicle | After 28 days: Curcumin NP resulted in an inhibition of inflammatory bone resorption: PBS-curcumin NP and LPS-curcumin NP have a bone volume/total volume (BV/TV) of 64 and 65% respectively (non-significant); PBS-empty NPand LPS-empty NP have a BV/TV of: 65% and 47% respectively (p < 0.05)) Curcumin NP also resulted in a decrease of both osteoclast counts (p < 0.001) and inflammatory infiltrate (p < 0.05); as well as in a marked attenuation of p38 MAPK and NF-KB activation | |
| Histomorphometric analysis | ||||||
| Western blot | ||||||
| Ni et al., 2019 [34] | Gold nanoparticles (AuNP) coated with L-cysteine | Experimental periodontitis in rat induced by ligatures 3 groups (n = 6/group): control (no ligature), ligatures, ligatures+AuNP (Lig-AuNP) | µCT analysis | Evaluate the potential application of AuNP | After 14 days: The injection of AuNP could significantly alleviate the ABL surrounding the maxillary second molars caused by ligatures: Lig 0.69 mm vs. Lig-AuNP 0.38 mm and control 0.34mm (p < 0.001) The elastic and collagenous fibers were denser and more well-organized in the groups with Lig-AuNP The number of osteoclasts was decreased by AuNP when the ligation existed (p < 0.001) The AuNP could inhibit this inflammatory response and downregulate the level of iNOS (p < 0.01) | |
| Histological and immunohistochemical assessment | ||||||
| Valerio et al., 2019 [35] | Polyethylene glycol (PEG)-polylactide (PLA) (PEG-PLA) nanoparticles loaded with Auranofin (ARN) | Experimental periodontitis in rats induced by injections of A. actinomycetem comitans-LPS 4 groups (n = 10/group): PBS alone, NP only (no ARN), NP-ARN high (10 µM), NP-ARN low (1 µM) | µCT analysis | Determine if nanoparticles loaded with a pharmacological agent that induces mitogen-activated protein kinase phosphatase has potential clinical utility for management of ABL | After 14 days: NP-ARN low was significantly effective at inhibition of LPS-induced bone loss compare to PBS (BV/TV 24% vs. 31% respectively) | |
| Anti-inflammatory and antibacterial agent | Lin et al., 2017 [36] | Polylactide-glycolic acid co-polymer and chitosan (PLGA/chitosan) with metronidazole or N-phenacyl-thiazolium bromide (PTB) | Experimental periodontitis in rat induced by ligatures 4 groups (n = 4/group): periodontitis alone (PR), periodontitis with nanospheres alone, nanospheres encapsulating metronidazole (MT), nanospheres encapsulating PTB (PB) | µCT analysis | Develop pH-responsive PLGA/chitosan nanosphere as an inflammation-responsive vehicle Evaluate the potential of the nanosphere encapsulating metronidazole, an antibiotic, and N-phenacylthiazolium bromide (PTB), a host modulator | After 21 days: Progression of periodontal bone loss (PPBL) was significantly reduced in groups MT (−0.1 mm) and PB on day 4 (−0.17 mm) compared with group PR (0.03 mm) (p < 0.05). On day 21, PPBL was significantly lower in group PB (−0.04 mm) compared with group PR (0.13 mm) and group MT (0.07 mm) (p < 0.05) On day 21, inflammation was significantly reduced in groups MT and PB relative to groups PR and periodontitis with nanospheres alone (p < 0.05), and collagen deposition was greater relative to group PR (p < 0.05) |
| Histological assessment |
| Treatment Type | Authors, Year | Nanoparticle | Coating/Loading | Shape | Size (Mean ± SD) | Dose | Cytotoxicity | Degradability |
|---|---|---|---|---|---|---|---|---|
| Antibacterial agent | Botelho et al., 2010 [26] | Nanostructured doxycycline gel | / | Spherical | Nanometer scale | 1 g | The nanoparticle is known to be biocompatible* | Known to be biodegradable * |
| Mahmoud et al., 2019 [27] | Poly(lactic-co-glycolic acid) (PLGA) | BAR peptide | Spherical | 87.9 ± 29.4nm (unhydrated) 333.8 ± 17.8 nm (hydrated) | 0.7 µM | BNPs were non-toxic within the evaluated concentration range of 1.3–3.4 μM. Telomerase immortalized gingival keratinocytes treated with BNPs or free BAR demonstrated > 90% viability and no significant lysis or apoptosis relative to untreated cells In addition, neither BNPs nor free BAR exhibited haemolytic activity | Biodegradable | |
| Anti-inflammatory agent | Napimoga et al., 2012 [28] | PLGA | 15-Deoxy-D12,14-PG J2 (15d-PGJ2) | Spherical | Nanometer scale | / | The nanoparticle is known to be biocompatible * | Biodegradable |
| Srivastava et al., 2014 [29] | Eugenol | Ketoprofen | Spherical | 37.230 ± 0.210 nm | / | The nanoparticle is known to be biocompatible * | Known to be biodegradable * | |
| Saita et al., 2016 [30] | Polyon complex composed of (PMNT-PEG-PMNT) triblock copolymer and anionic poly(acrylic acid) | / | Flower-like micelle | 79 nm | / | The nanoparticle is known to be biocompatible * | Known to be biodegradable * | |
| Khajuria et al., 2017 [31] | Zinc-hydroxyapatite (chitosan-based) | / | / | Nanometer scale | 0.2% w/v | The nanoparticle is known to be biocompatible * | Known to be biodegradable * | |
| Pereira et al., 2018 [32] | PLGA | Metformine hydrochloride | Spherical | 457.1 ± 48.9 nm | / | The nanoparticle is known to be biocompatible * | Biodegradable | |
| Zambrano et al., 2018 [33] | PLGA | Curcumin | / | Nanometer scale | / | The nanoparticle is known to be biocompatible * | Known to be biodegradable* | |
| Ni et al., 2019 [34] | Gold (Au) | L-cysteine | / | 45 nm | 0.25 µM | AuNP did not show any significant cytotoxicity on mouse macrophage cell line (cell viability, membrane integrity, ROS production assays) AuNPs did not affect cell viability of murine bone marrow-derived macrophage | Non-degradable | |
| Valerio et al., 2019 [35] | PEG-PLA | Auranofin (ARN) | Spherical | Nanometer scale | 1 or 10 µM | - ARN-NP did not significantly affect cell viability of murine macrophage, in contrast to higher doses of free ARN | Biodegradable | |
| Anti-inflammatory and antibacterial agent | Lin et al., 2017 [36] | PLGA and chitosan | Metronidazole or N-phenacyl-thiazolium bromide | Spherical | 499 ± 21.24 nm | / | The nanoparticle is known to be biocompatible * | Biodegradable |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brun, A.; Moignot, N.; Colombier, M.-L.; Dursun, E. Emerging Nanotechnology in Non-Surgical Periodontal Therapy in Animal Models: A Systematic Review. Nanomaterials 2020, 10, 1414. https://doi.org/10.3390/nano10071414
Brun A, Moignot N, Colombier M-L, Dursun E. Emerging Nanotechnology in Non-Surgical Periodontal Therapy in Animal Models: A Systematic Review. Nanomaterials. 2020; 10(7):1414. https://doi.org/10.3390/nano10071414
Chicago/Turabian StyleBrun, Adrian, Nicolas Moignot, Marie-Laure Colombier, and Elisabeth Dursun. 2020. "Emerging Nanotechnology in Non-Surgical Periodontal Therapy in Animal Models: A Systematic Review" Nanomaterials 10, no. 7: 1414. https://doi.org/10.3390/nano10071414
APA StyleBrun, A., Moignot, N., Colombier, M.-L., & Dursun, E. (2020). Emerging Nanotechnology in Non-Surgical Periodontal Therapy in Animal Models: A Systematic Review. Nanomaterials, 10(7), 1414. https://doi.org/10.3390/nano10071414