
Feasibility of Application of the Newly Developed Nano-Biomaterial, β-TCP/PDLLA, in Maxillofacial Reconstructive Surgery: A Pilot Rat Study

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
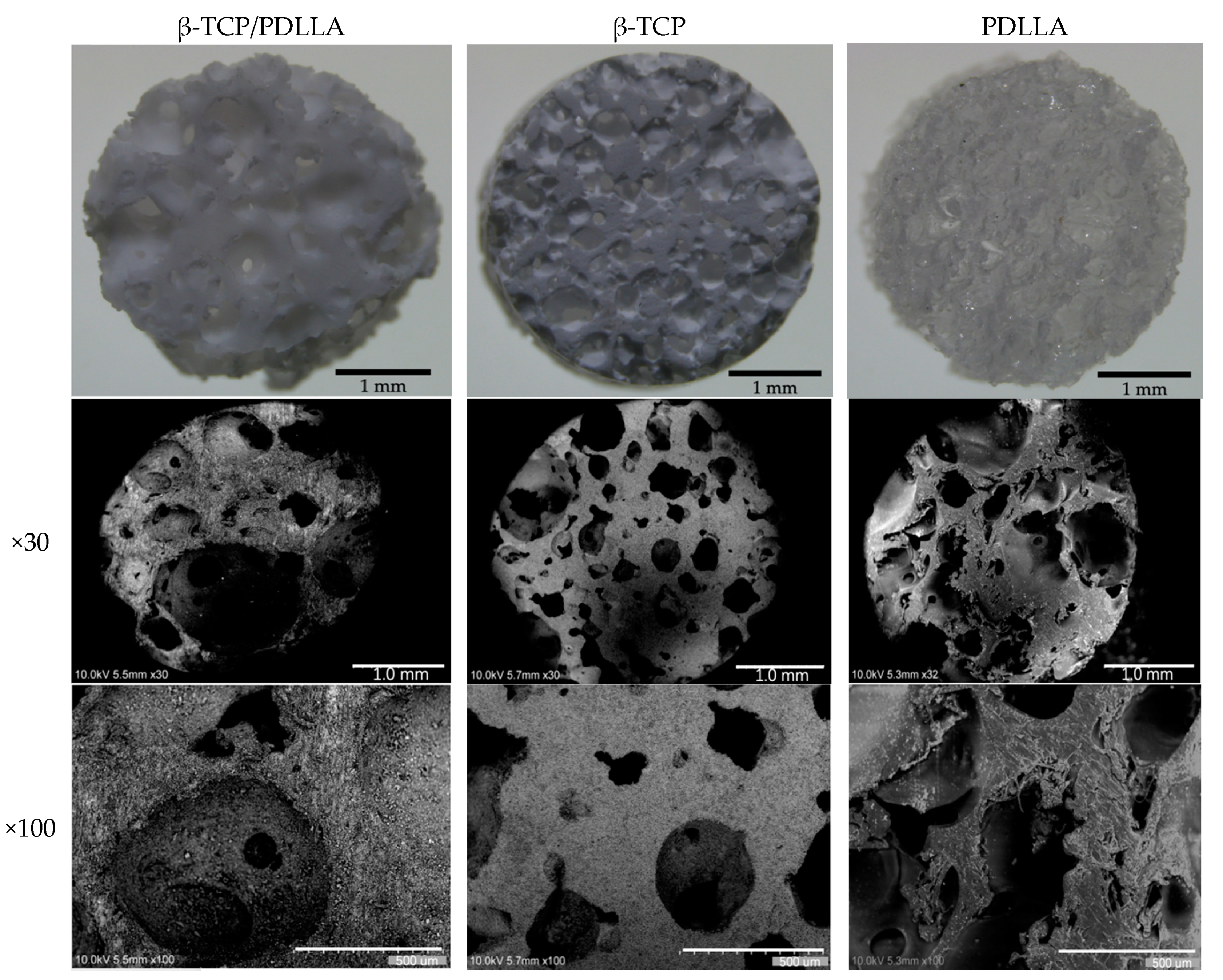
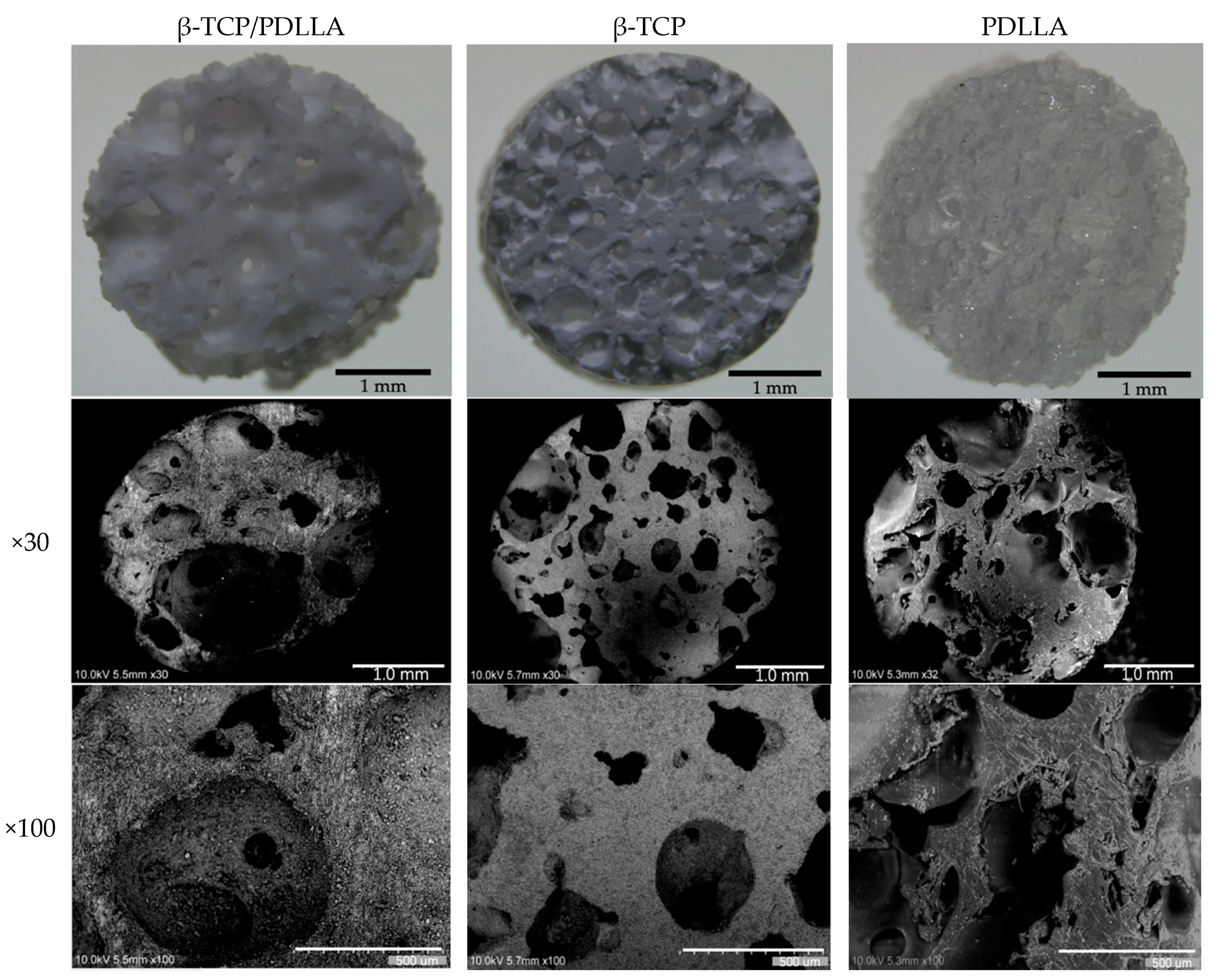
2.1. Materials
2.2. Animals
2.3. Anesthetic Agents
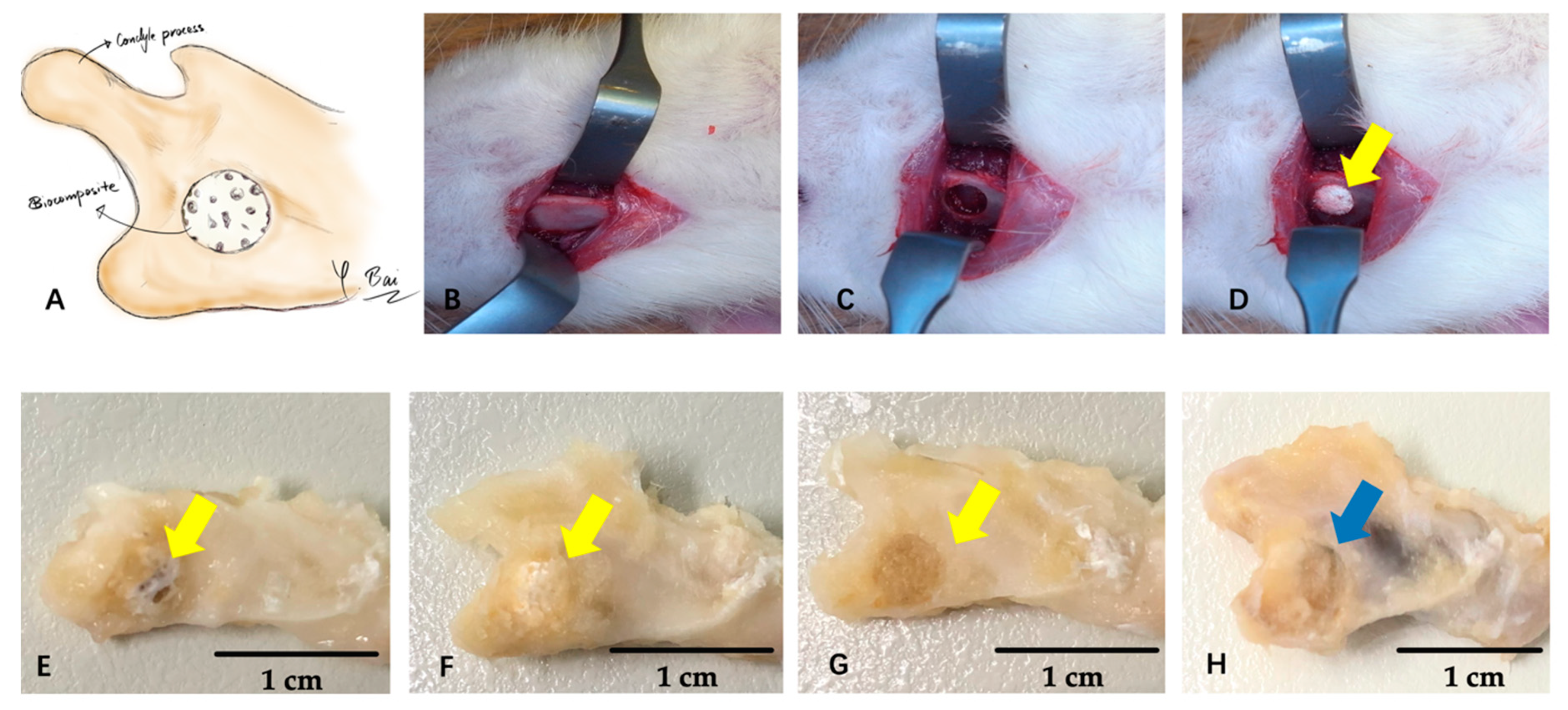
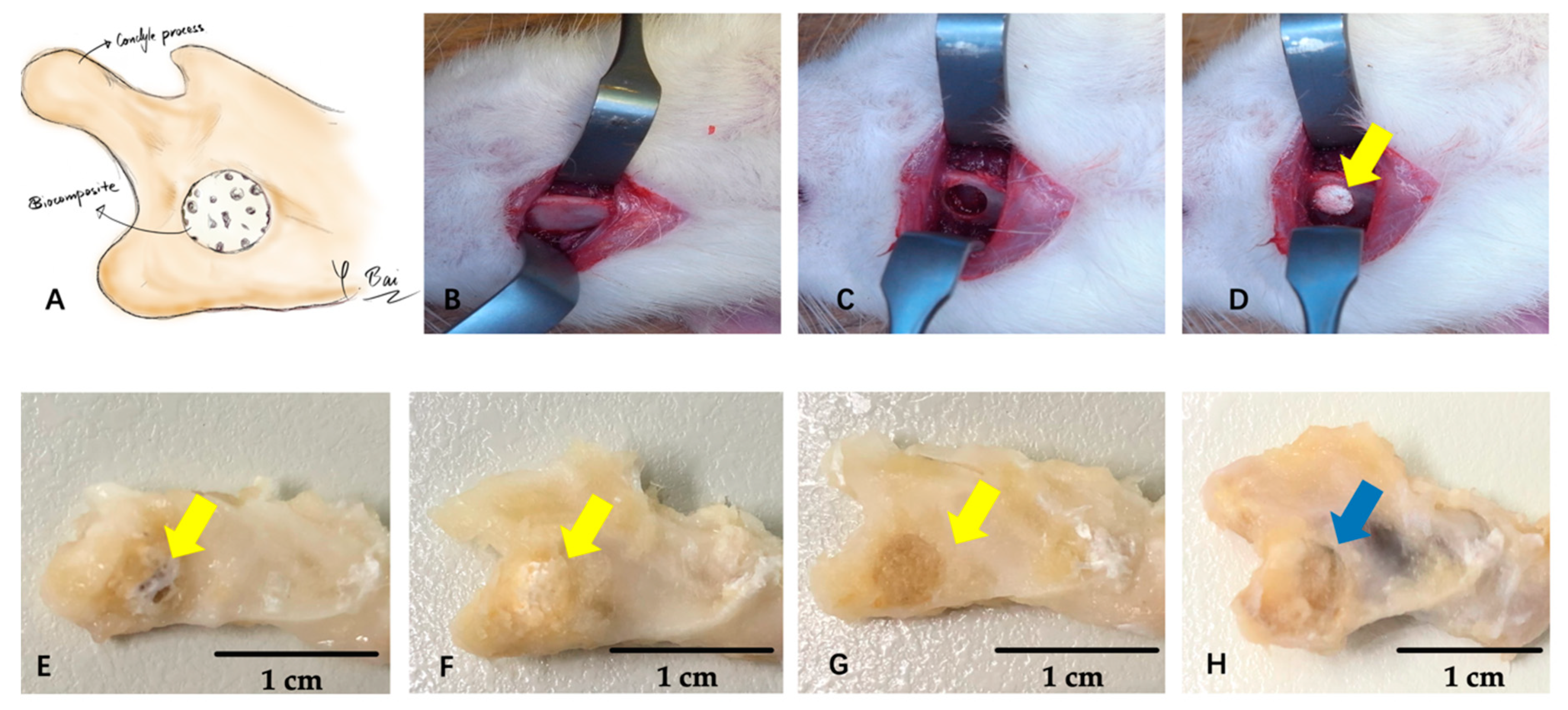
2.4. Surgical Procedures
2.5. Micro-Computed Tomography
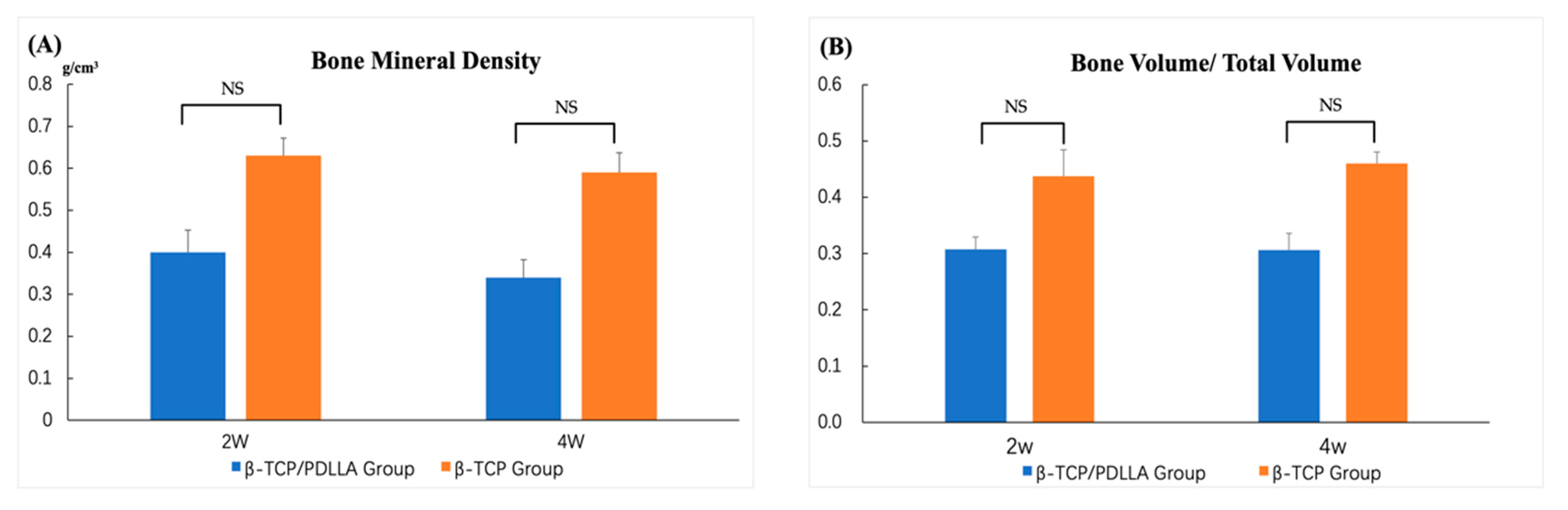
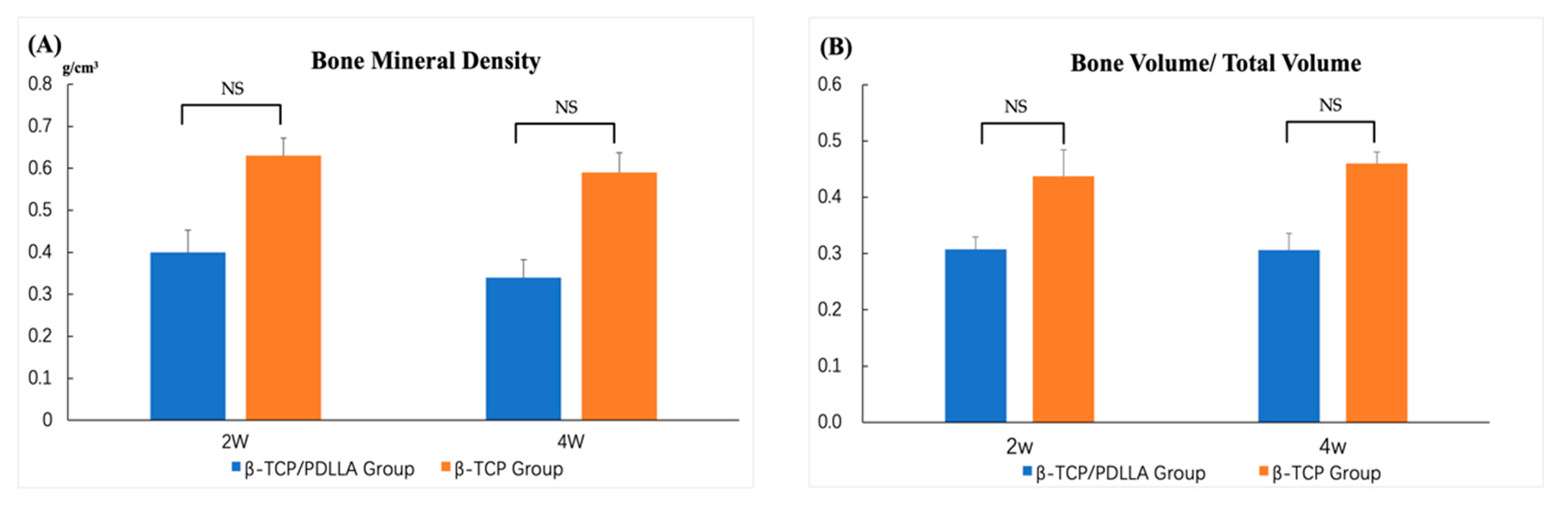
2.6. Bone Mineral Density and the Bone Volume to Total Volume Ratio
2.7. Histochemical Staining
2.8. Optical Density Assessment
2.9. Statistical Analysis
3. Results
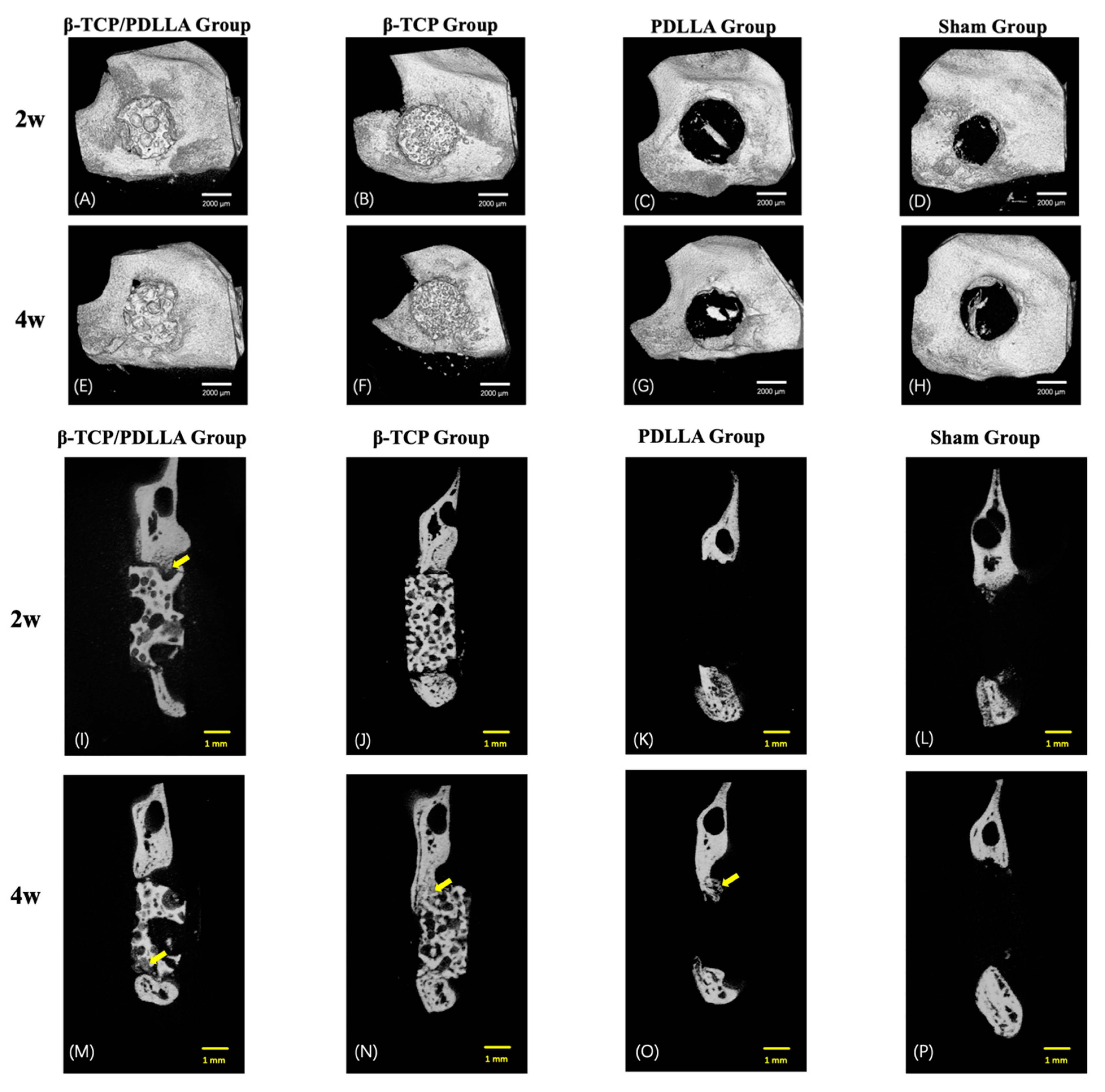
3.1. Micro-CT
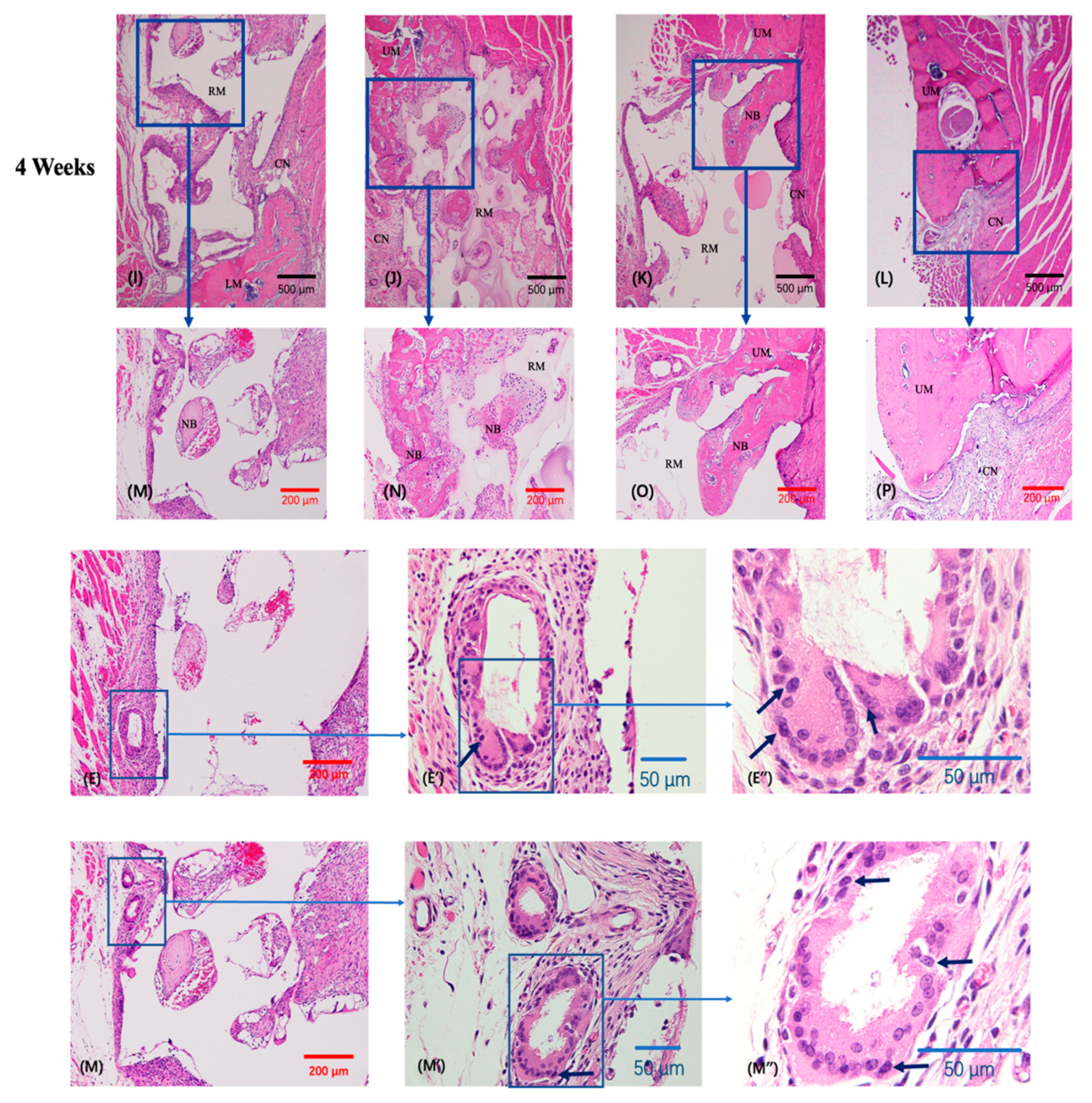
3.2. Histochemical Staining
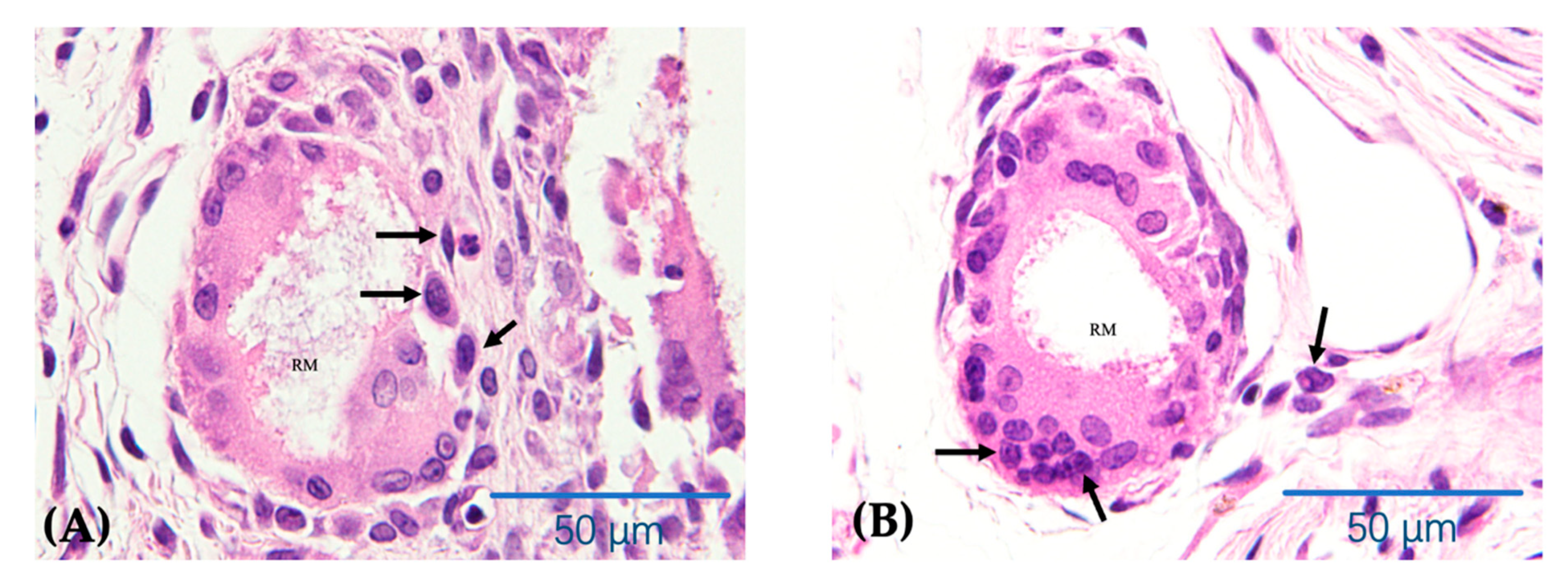
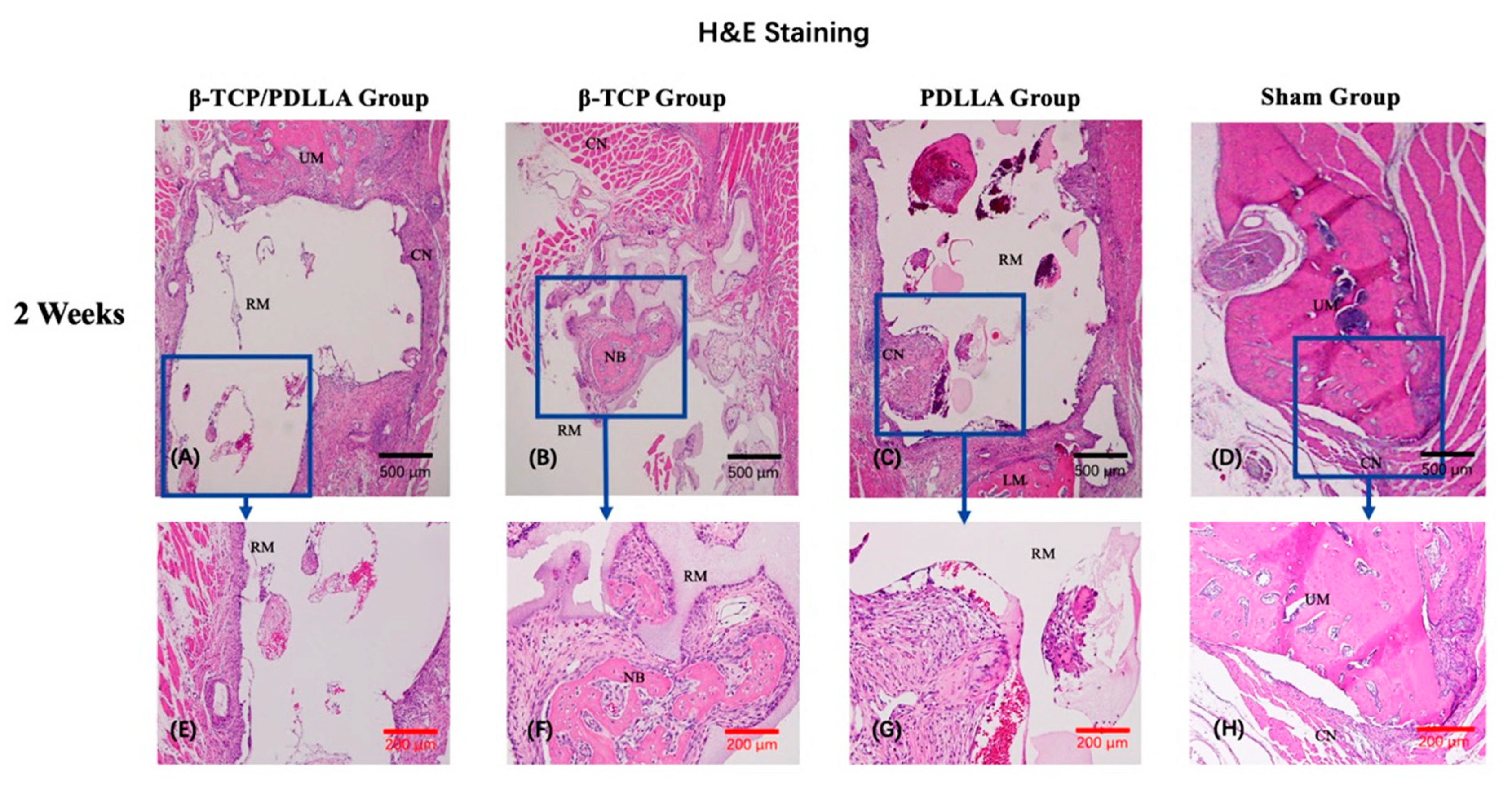
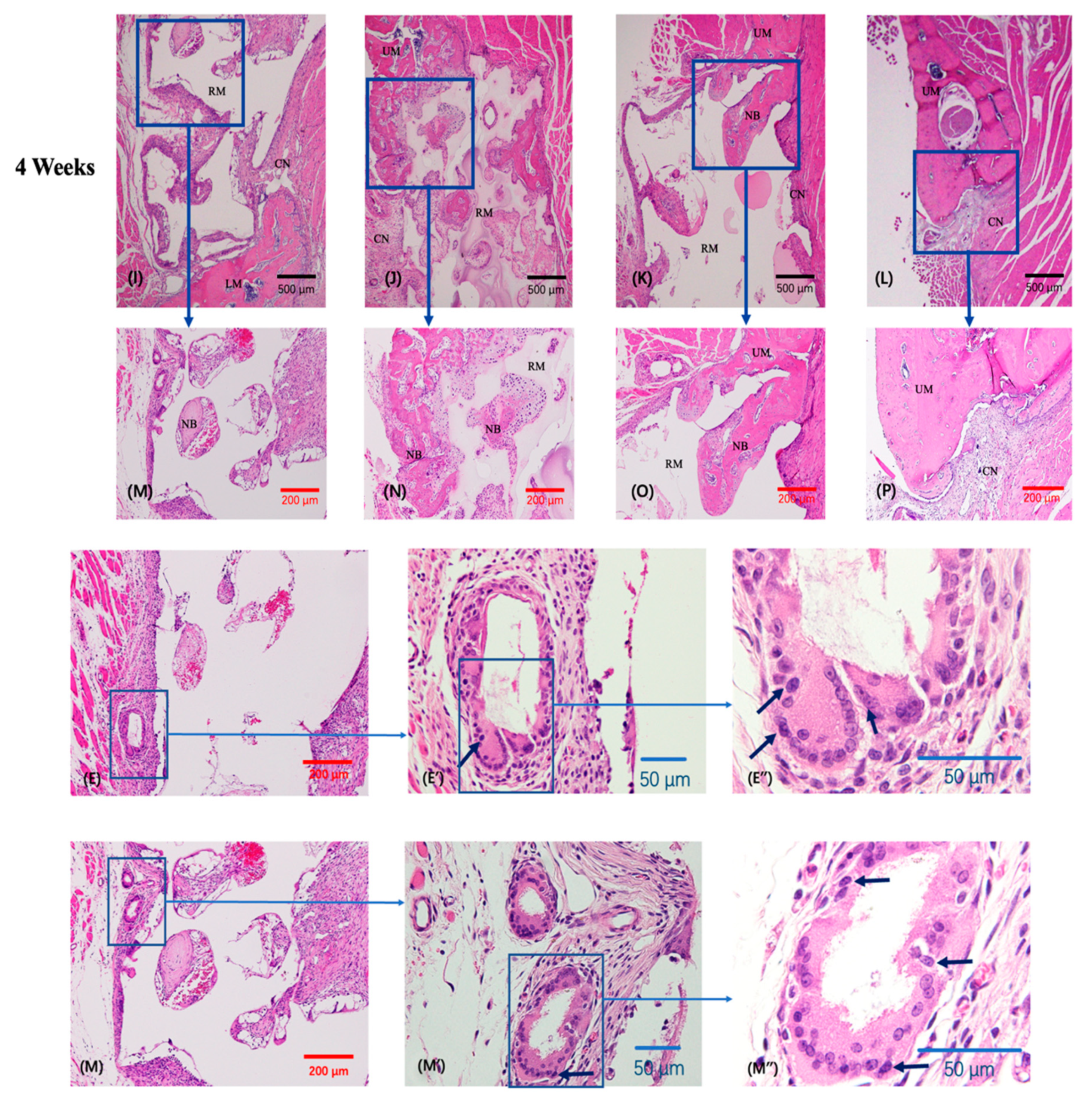
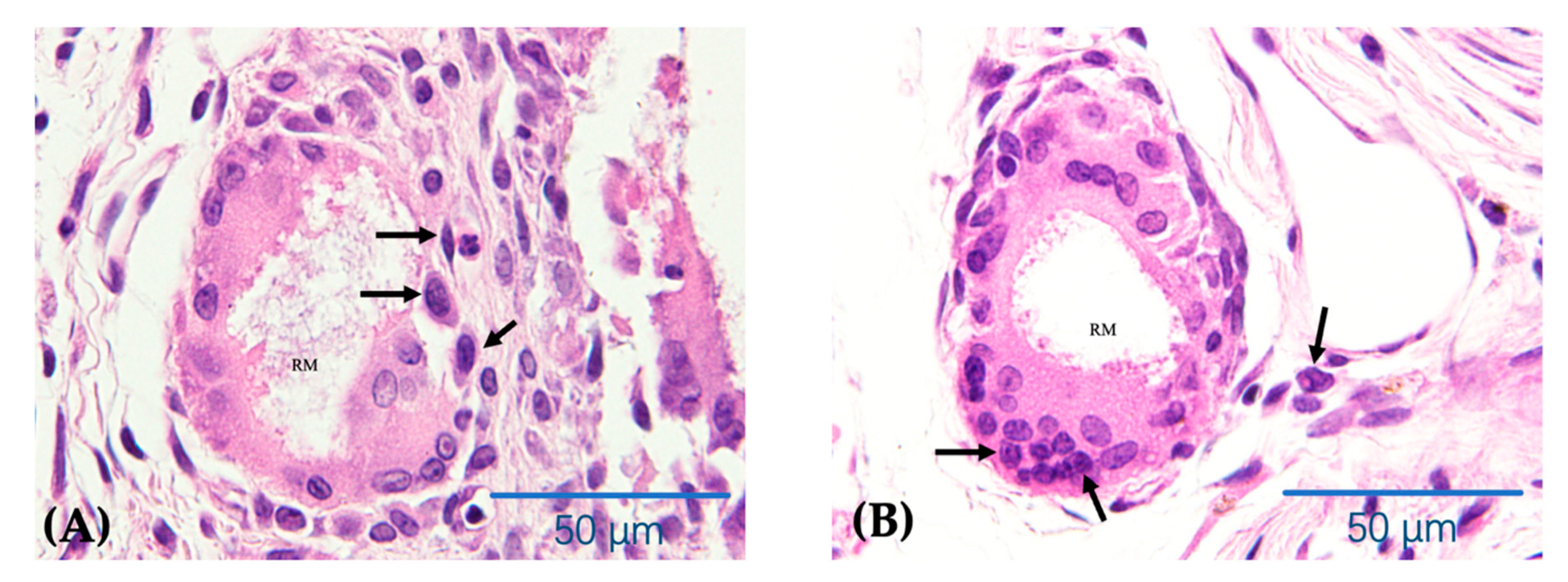
3.2.1. H&E Staining
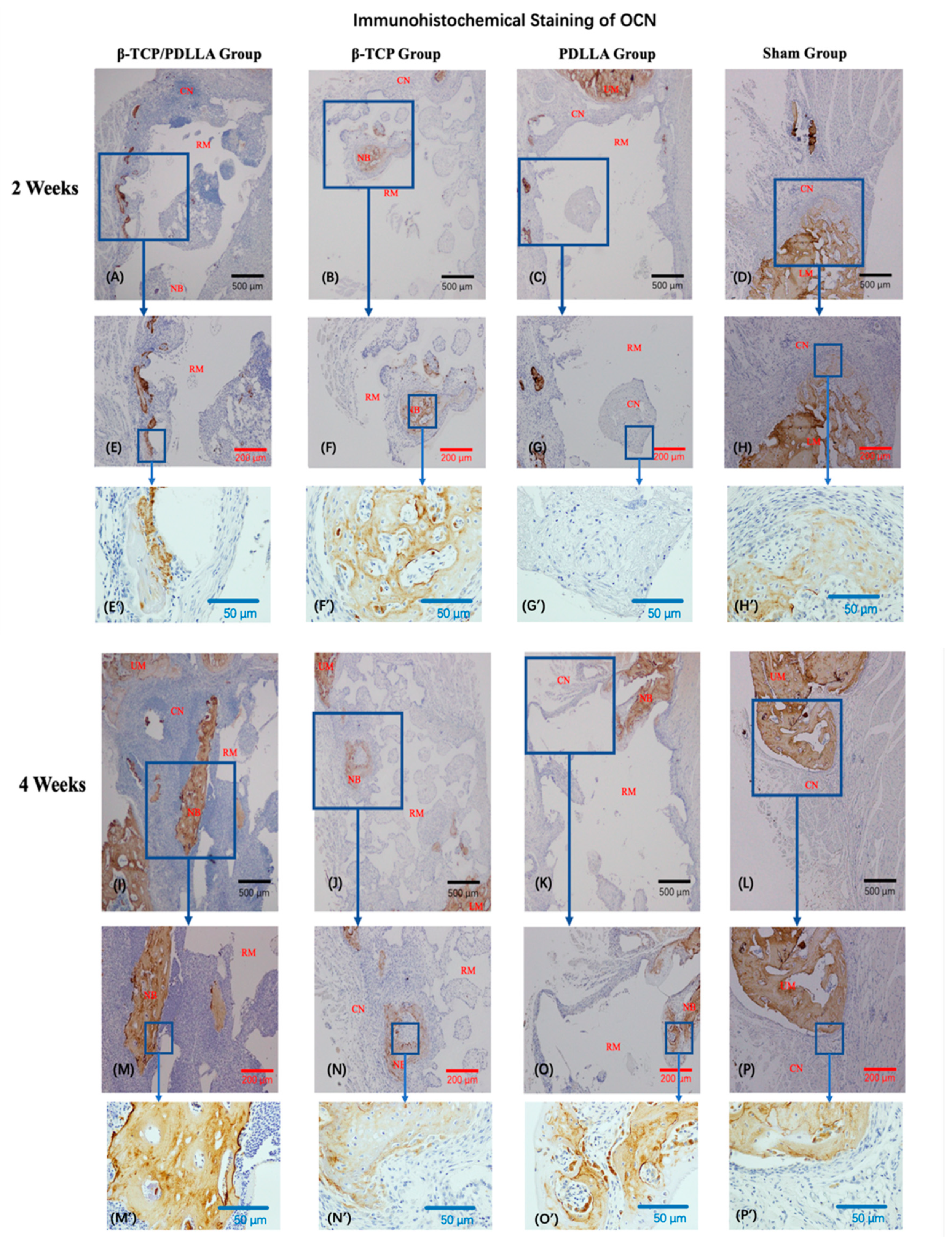
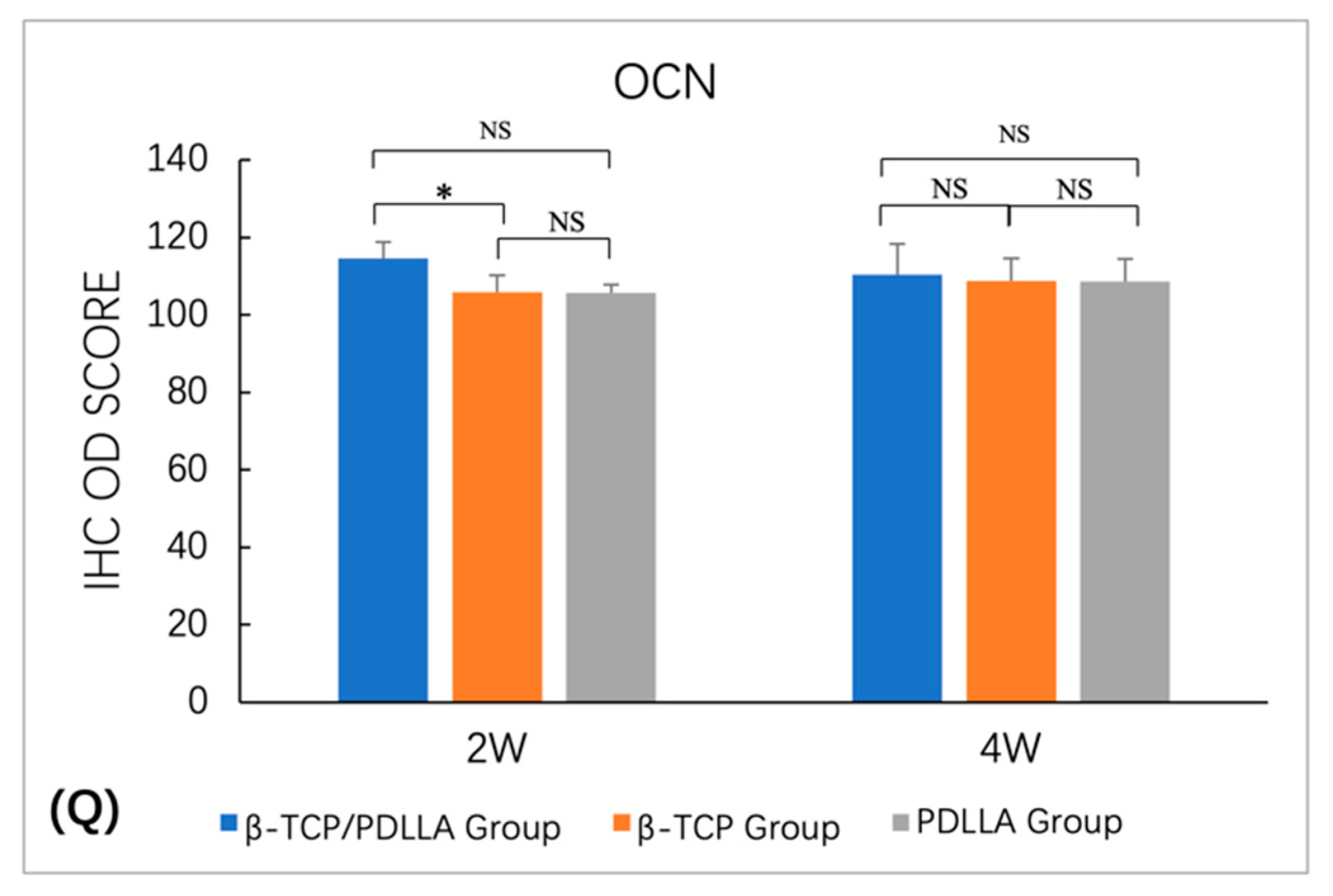
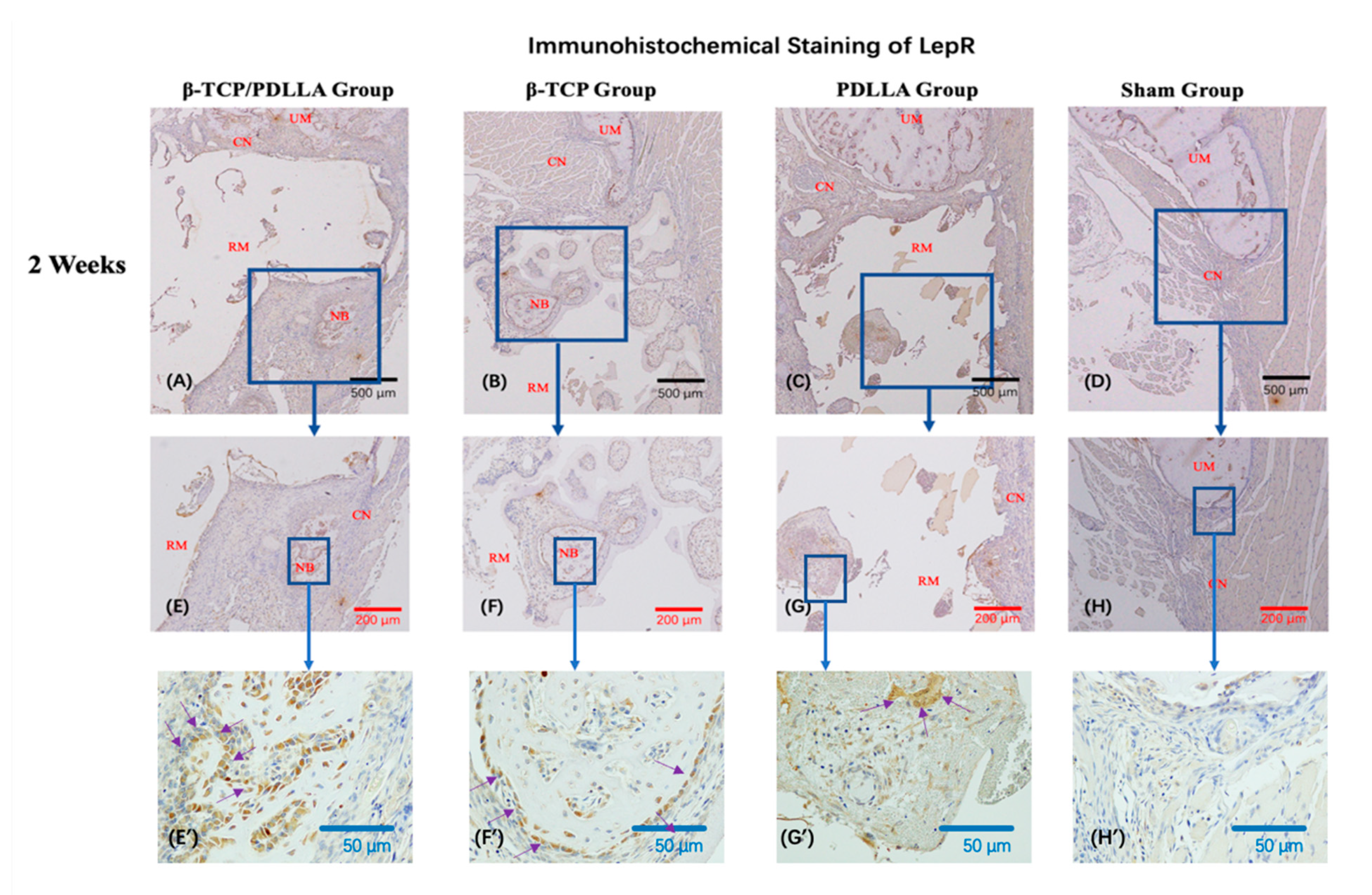
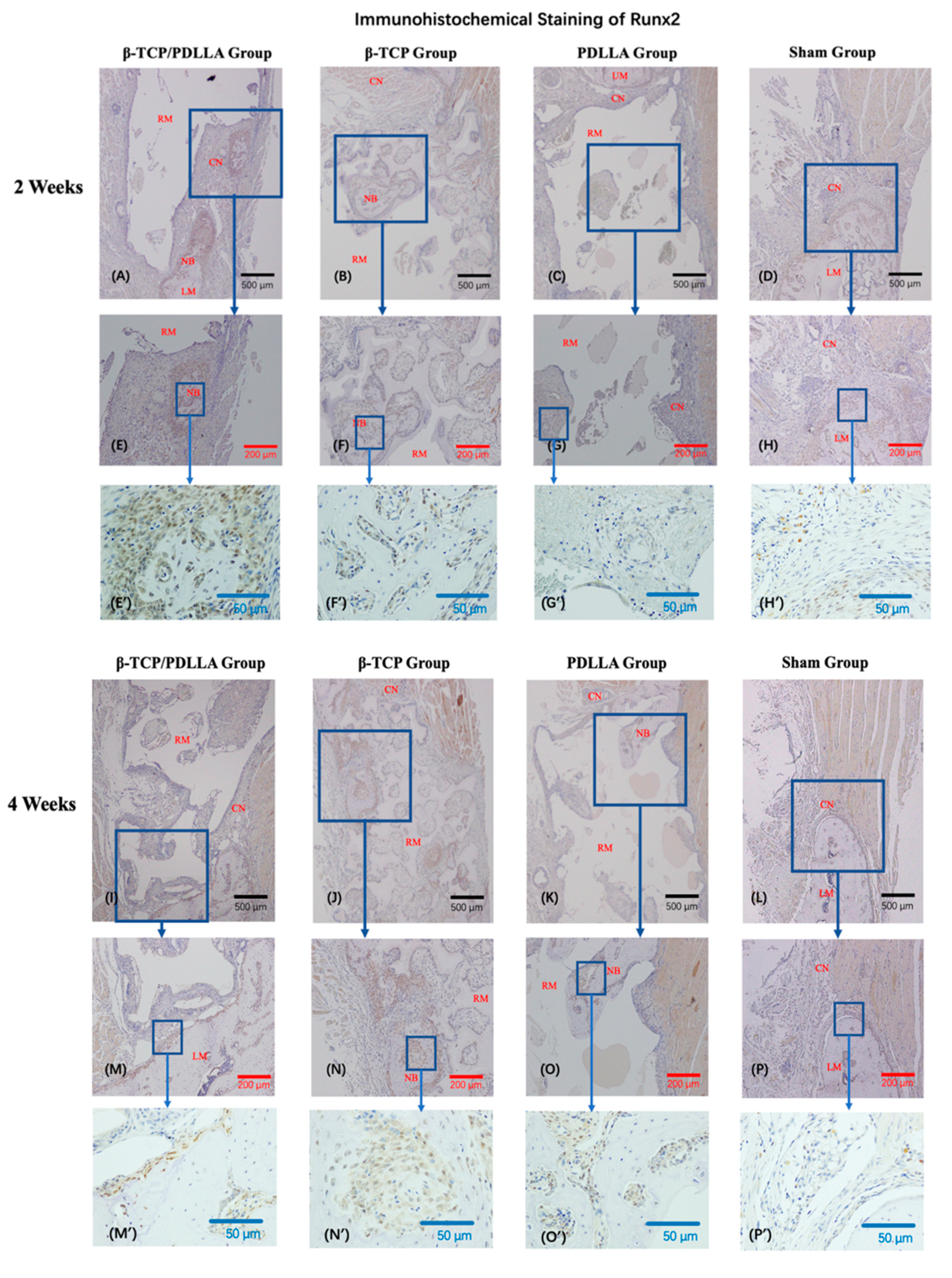
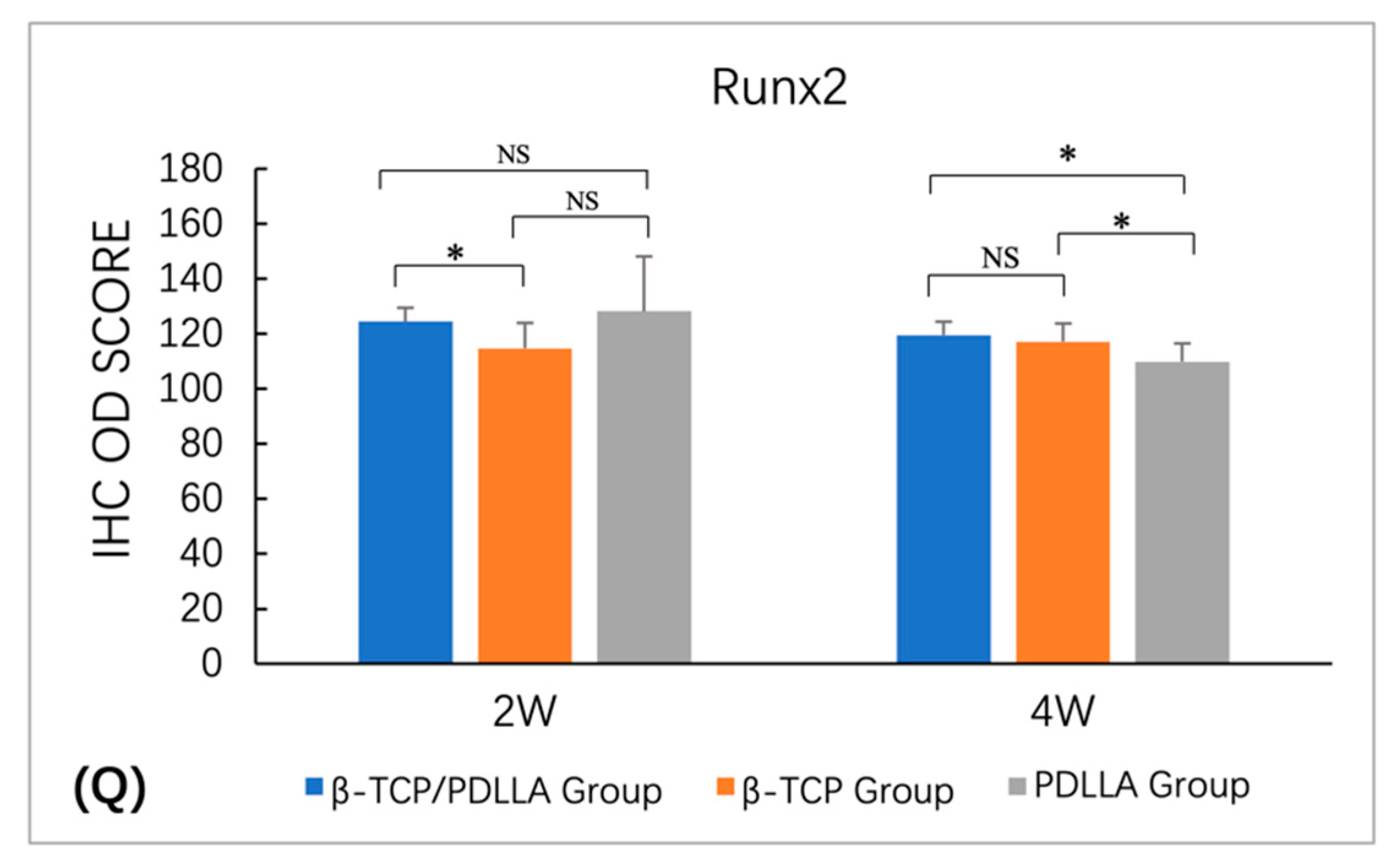
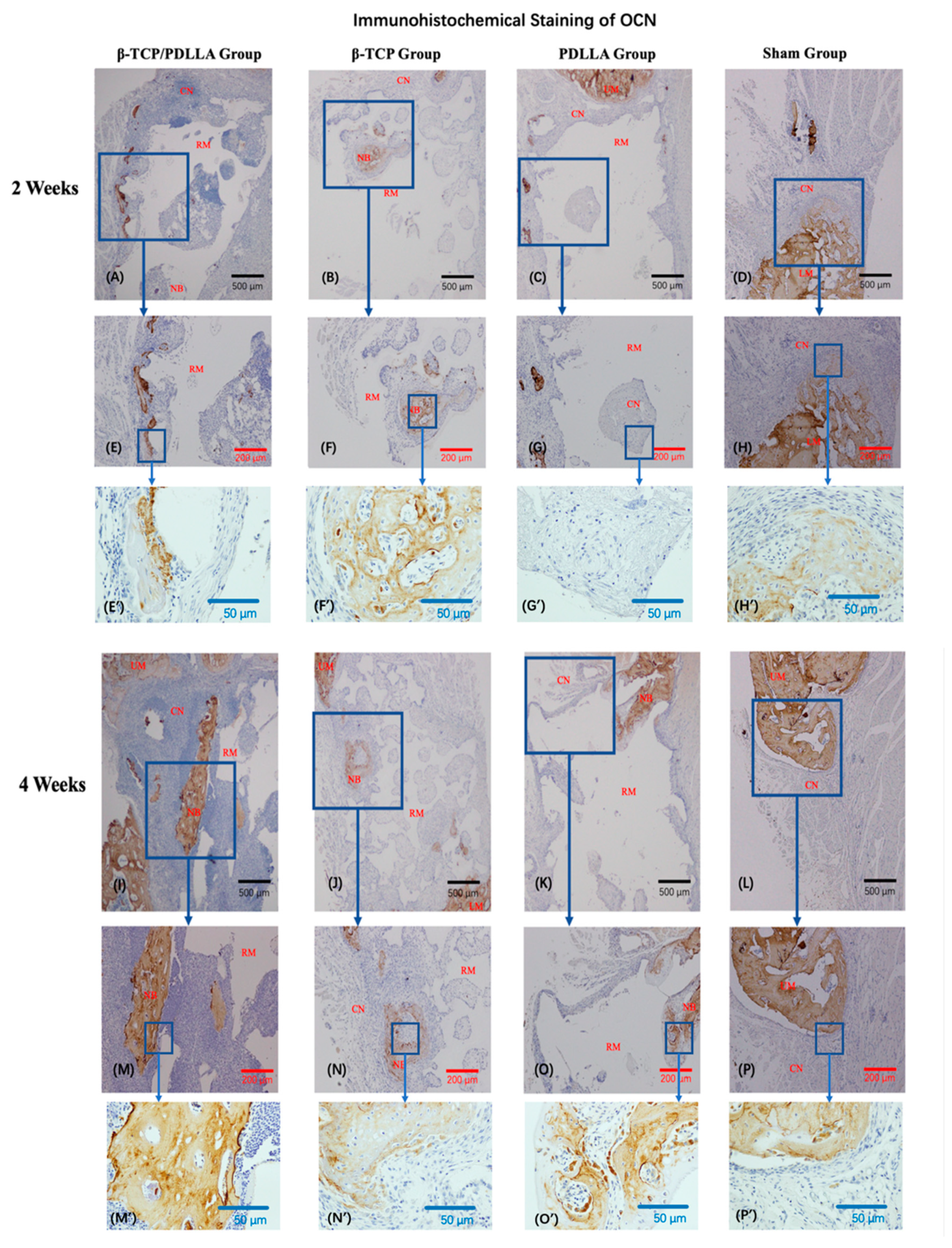
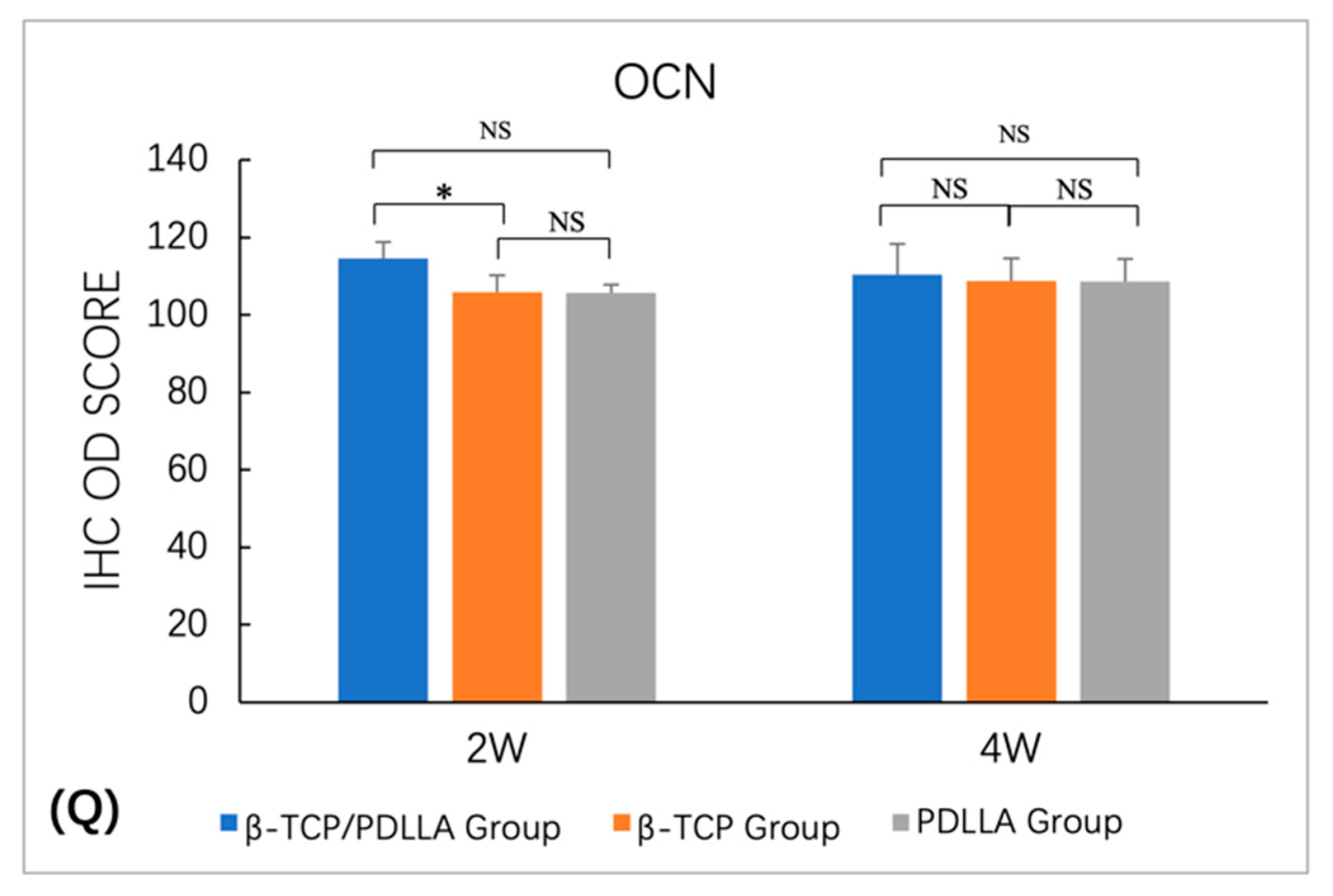
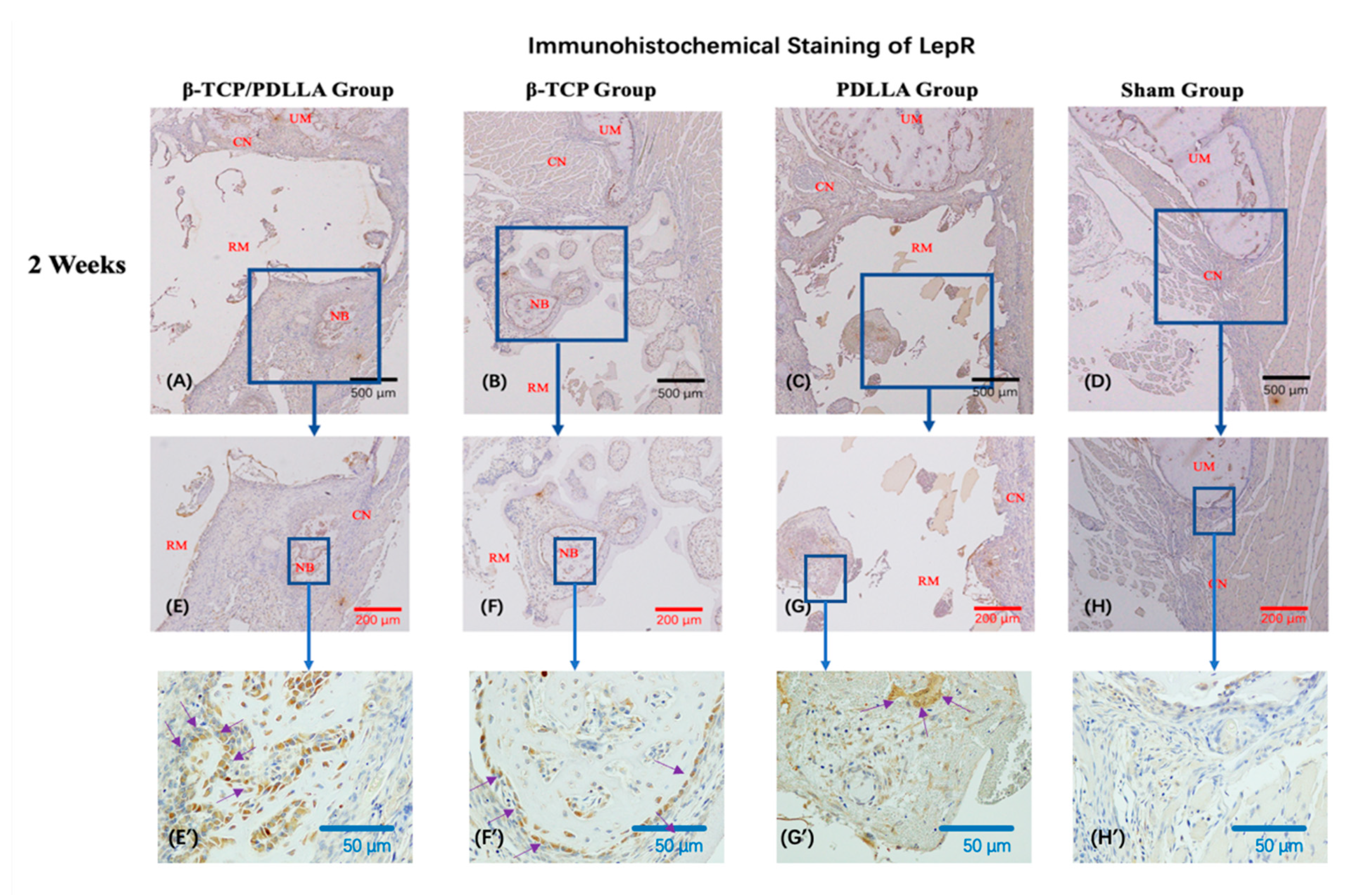
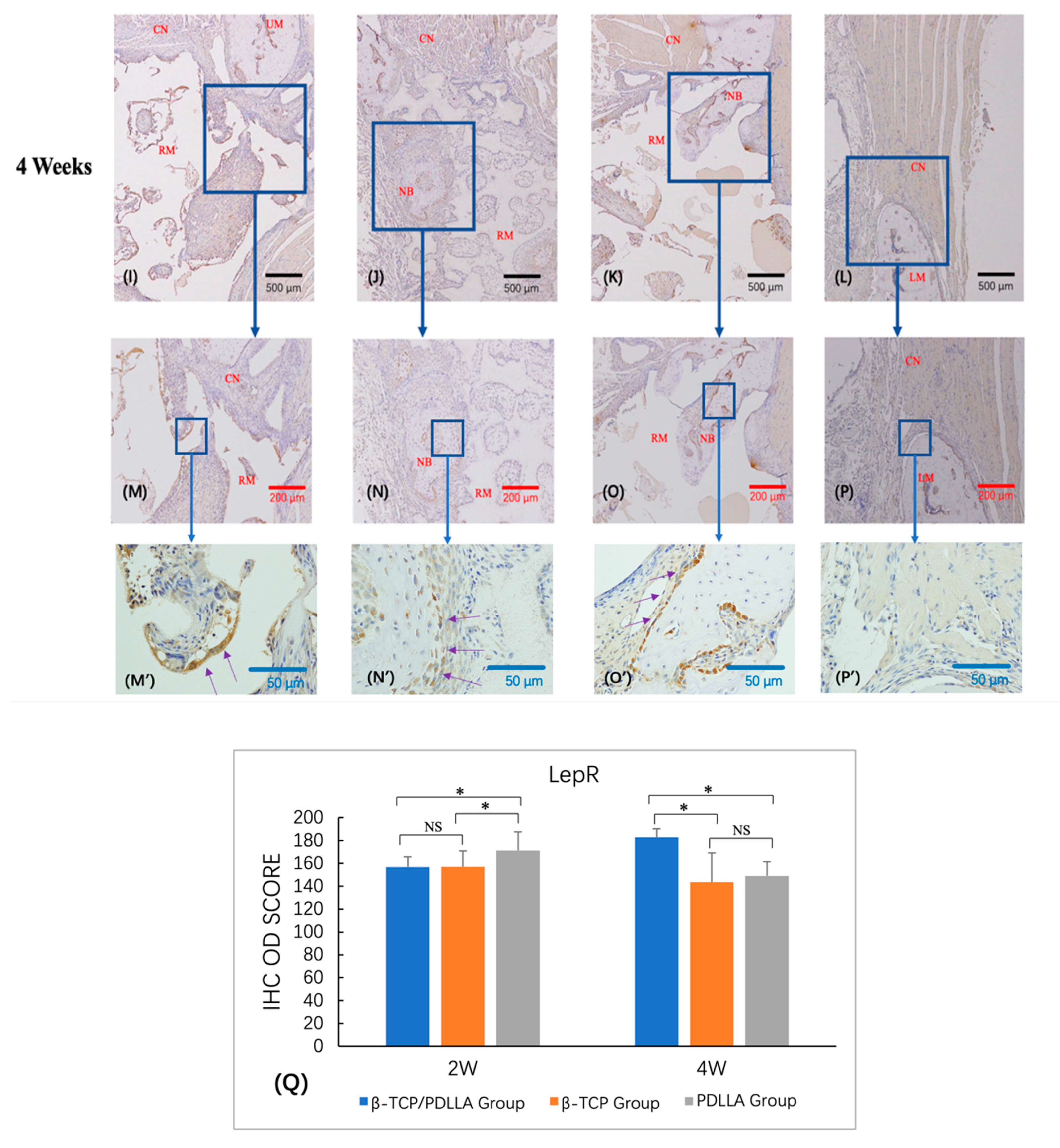
3.2.2. IHC Staining
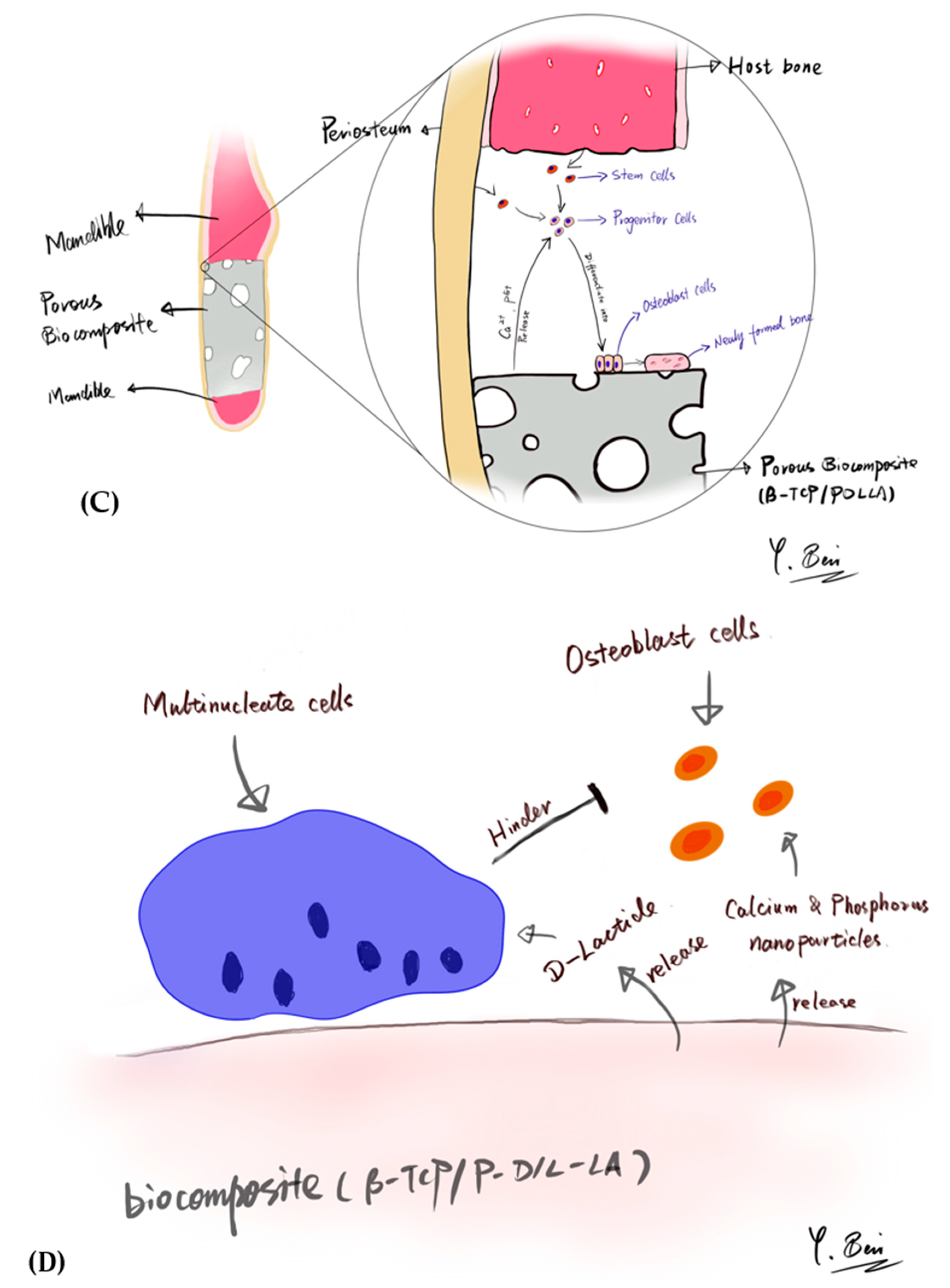
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mobini, S.; Ayoub, A. Bone tissue engineering in the maxillofacial region: The state-of-the-art practice and future prospects. Bone Tissue Eng. 2016, 1. [Google Scholar] [CrossRef]
- Hasegawa, S.; Tamura, J.; Neo, M.; Goto, K.; Shikinami, Y.; Saito, M.; Kita, M.; Nakamura, T. In vivo evaluation of a porous hydroxyapatite/poly-DL-lactide composite for use as a bone substitute. Biomed. Mater. Res. Part A 2005, 75, 567–579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sukegawa, S.; Kanno, T.; Shibata, A.; Matsumoto, K.; Sukegawa-Takahashi, Y.; Sakaida, K.; Furuki, Y. Use of the bioactive resorbable plate system for zygoma and zygomatic arch replacement and fixation with modified Crockett’s method for maxillectomy: A technical note. Mol. Clin. Oncol. 2017, 7, 47–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sen, M.K.; Miclau, T. Autologous iliac crest bone graft: Should it still be the gold standard for treating nonunions? Injury 2007, 38, S75–S80. [Google Scholar] [CrossRef]
- Nishida, J.; Shimamura, T. Methods of reconstruction for bone defect after tumor excision: A review of alternatives. Med. Sci. Monit. 2008, 14, RA107–RA113. [Google Scholar]
- Wang, W.; Yeung, K.W.K. Bone grafts and biomaterials substitutes for bone defect repair: A review. Bioact. Mater. 2017, 2, 224–247. [Google Scholar] [CrossRef]
- Kanno, T.; Sukegawa, S.; Furuki, Y.; Nariai, Y.; Sekine, J. Overview of innovative advances in bioresorbable plate systems for oral and maxillofacial surgery. Jpn. Dent. Sci. Rev. 2018, 54, 127–138. [Google Scholar] [CrossRef]
- van Bakelen, N.B.; Buijs, G.J.; Jansma, J.; de Visscher, J.G.A.M.; Hoppenreijs, T.J.M.; Bergsma, J.E.; Stegenga, B.; Bos, R.R.M. Decision-Making considerations in application of biodegradable fixation systems in maxillofacial surgery—A retrospective cohort study. J. Cranio Maxillofac. Surg. 2014, 42, 417–422. [Google Scholar] [CrossRef]
- Schumann, P.; Lindhorst, D.; Wagner, M.E.H.; Schramm, A.; Gellrich, N.-C.; Rücker, M. Perspectives on resorbable osteosynthesis materials in craniomaxillofacial surgery. Pathobiology 2013, 80, 211–217. [Google Scholar] [CrossRef]
- Sukegawa, S.; Kanno, T.; Nagano, D.; Shibata, A.; Sukegawa-Takahashi, Y.; Furuki, Y. The clinical feasibility of newly developed thin flat-type bioresorbable osteosynthesis devices for the internal fixation of zygomatic fractures: Is there a difference in healing between bioresorbable materials and titanium osteosynthesis? J. Craniofac. Surg. 2016, 27, 2124–2129. [Google Scholar] [CrossRef] [Green Version]
- Park, Y.-W. Bioabsorbable osteofixation for orthognathic surgery. Maxillofac. Plast. Reconstr. Surg. 2015, 37, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sukegawa, S.; Kanno, T.; Katase, N.; Shibata, A.; Takahashi, Y.; Furuki, Y. Clinical evaluation of an unsintered hydroxyapatite/poly-l-lactide osteoconductive composite device for the internal fixation of maxillofacial fractures. J. Craniofac. Surg. 2016, 27, 1391–1397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanno, T.; Karino, M.; Yoshino, A.; Koike, T.; Ide, T.; Tatsumi, H.; Tsunematsu, K.; Yoshimatsu, H.; Sekine, J. Feasibility of single folded unsintered hydroxyapatite particles/poly-l-lactide composite sheet in combined orbital floor and medial wall fracture reconstruction. J. Hard Tissue Biol. 2017, 26, 237–244. [Google Scholar] [CrossRef]
- Bai, Y.; Sha, J.; Kanno, T.; Miyamoto, K.; Hideshima, K.; Matsuzaki, Y. Comparison of the bone regenerative capacity of three-dimensional uncalcined and unsintered hydroxyapatite/poly-d/l-lactide and beta-tricalcium phosphate used as bone graft substitutes. J. Investig. Surg. 2019, 1, 14. [Google Scholar] [CrossRef]
- Bai, Y.; Kanno, T.; Tatsumi, H.; Miyamoto, K.; Sha, J.; Hideshima, K.; Matsuzaki, Y. Feasibility of a three-dimensional porous uncalcined and unsintered hydroxyapatite/poly-d/l-lactide composite as a regenerative biomaterial in maxillofacial surgery. Materials 2018, 11, 2047. [Google Scholar] [CrossRef] [Green Version]
- Sha, J.; Kanno, T.; Miyamoto, K.; Bai, Y.; Hideshima, K.; Matsuzaki, Y. Application of a bioactive/bioresorbable three-dimensional porous uncalcined and unsintered hydroxyapatite/poly-d/l-lactide composite with human mesenchymal stem cells for bone regeneration in maxillofacial surgery: A pilot animal study. Materials 2019, 12, 705. [Google Scholar] [CrossRef] [Green Version]
- Dong, Q.N.; Kanno, T.; Bai, Y.; Sha, J.; Hideshima, K. Bone regeneration potential of uncalcined and unsintered hydroxyapatite/poly l-lactide bioactive/osteoconductive sheet used for maxillofacial reconstructive surgery: An in vivo study. Materials 2019, 12, 2931. [Google Scholar] [CrossRef] [Green Version]
- Akagi, H.; Ochi, H.; Soeta, S.; Kanno, N.; Yoshihara, M.; Okazaki, K.; Yogo, T.; Harada, Y.; Amasaki, H.; Hara, Y. A comparison of the process of remodeling of hydroxyapatite/poly-d/l-lactide and beta-tricalcium phosphate in a loading site. BioMed. Res. Int. 2015, 2015, 730105. [Google Scholar] [CrossRef] [Green Version]
- Barrère, F.; van Blitterswijk, C.A.; de Groot, K. Bone regeneration: Molecular and cellular interactions with calcium phosphate ceramics. Int. J. Nanomed. 2006, 1, 317. [Google Scholar]
- Shimizu, S.; Tsuchiya, S.; Hirakawa, A.; Kato, K.; Ando, M.; Mizuno, M.; Osugi, M.; Okabe, K.; Katagiri, W.; Hibi, H. Design of a Randomized Controlled Clinical Study of Tissue-Engineered Osteogenic Materials Using Bone Marrow-Derived Mesenchymal Cells for Maxillomandibular Bone Defects in Japan: The TEOM Study Protocol. BMC Oral Health 2019, 19, 69. [Google Scholar] [CrossRef] [Green Version]
- Bhatt, R.A.; Rozental, T.D. Bone graft substitutes. Hand Clin. 2012, 28, 457–468. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.-J.; Shen, H.; Wang, Y.-P.; Jiang, Y.; Zhang, X.-L.; Yuan, G.-Y. Effect of beta-tricalcium phosphate/poly-l-lactide composites on radial bone defects of rabbit. Asian Pac. J. Trop. Med. 2013, 6, 753–756. [Google Scholar] [CrossRef] [Green Version]
- Abert, J.; Amella, A.; Weigelt, S.; Fischer, H. Degradation and swelling issues of poly-(d,l-lactide)/β-tricalcium phosphate/calcium carbonate composites for bone replacement. J. Mech. Behav. Biomed. Mater. 2016, 54, 82–92. [Google Scholar] [CrossRef]
- ASTM International. Standard test methods for apparent porosity, water absorption, apparent specific gravity and bulk density of burned refractory brick and shapes by boiling water. In West Conshohocken: ASTM C20-00; ASTM International: West Conshohocken, PA, USA, 2015; pp. 1–3. [Google Scholar]
- Kirihara, Y.; Takechi, M.; Kurosaki, K.; Kobayashi, Y.; Saito, Y.; Takeuchi, T. Effects of an anesthetic mixture of medetomidine, midazolam, and butorphanol in rats—strain difference and antagonism by atipamezole. Exp. Anim. 2016, 65, 27–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruker-Micro, C.T. Bone Mineral Density (BMD) and Tissue Mineral Density (TMD) Calibration and Measurement by Micro-CT Using Bruker-Micro CT; Bruker-Micro CT: Kontich, Belgium, 2010; pp. 1–30. [Google Scholar]
- Gaêta-Araujo, H.; Nascimento, E.H.L.; Brasil, D.M.; Madlum, D.V.; Haiter-Neto, F.; Oliveira-Santos, C. Influence of reconstruction parameters of micro-computed tomography on the analysis of bone mineral density. Imaging Sci. Dent. 2020, 50, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Bruker-Micro, C.T. Analysis of Bone by Micro-CT General Information; Bruker-Micro CT: Kontich, Belgium, 2013; pp. 1–41. [Google Scholar]
- Jafari, S.M.S.; Hunger, R.E. IHC optical density score: A new practical method for quantitative immunohistochemistry image analysis. Appl. Immunohistochem. Mol. Morphol. 2017, 25, e12–e13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruifrok, A.C.; Johnston, D.A. Quantification of histochemical staining by color deconvolution. Anal. Quant. Cytol. Histol. 2001, 23, 291–299. [Google Scholar] [PubMed]
- Langer, R.; Vacanti, J.P. Tissue engineering. Science 1993, 260, 920–926. [Google Scholar] [CrossRef] [Green Version]
- Mandrycky, C.; Wang, Z.; Kim, K.; Kim, D.-H. 3D bioprinting for engineering complex tissues. Biotechnol. Adv. 2016, 34, 422–434. [Google Scholar] [CrossRef] [Green Version]
- Jones, J.R.; Hench, L.L. Factors affecting the structure and properties of bioactive foam scaffolds for tissue engineering. J. Biomed. Mater. Res. Appl. Biomater. 2004, 68B, 36–44. [Google Scholar] [CrossRef]
- Lee, K.; Weir, M.D.; Lippens, E.; Mehta, M.; Wang, P.; Duda, G.N.; Kim, W.S.; Mooney, D.J.; Xu, H.H.K. Bone regeneration via novel macroporous CPC scaffolds in critical-sized cranial defects in rats. Dent. Mater. 2014, 30, e199–e207. [Google Scholar] [CrossRef] [PubMed]
- Colnot, C.; Zhang, X.; Tate, M.L.K. Current insights on the regenerative potential of the periosteum: Molecular, cellular, and endogenous engineering approaches. J. Orthop. Res. 2012, 30, 1869–1878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hallman, M.; Thor, A. Bone substitutes and growth factors as an alternative/complement to autogenous bone for grafting in implant dentistry. Periodontology 2000 2008, 47, 172–192. [Google Scholar] [CrossRef] [PubMed]
- Nageeb, M.; Nouh, S.R.; Bergman, K.; Nagy, N.B.; Khamis, D.; Kisiel, M.; Engstrand, T.; Hilborn, J.; Marei, M.K. Bone engineering by biomimetic injectable hydrogel. Mol. Cryst. Liq. Cryst. 2012, 555, 177–188. [Google Scholar] [CrossRef]
- Shikinami, Y.; Okazaki, K.; Saito, M.; Okuno, M.; Hasegawa, S.; Tamura, J.; Fujibayashi, S.; Nakamura, T. Bioactive and bioresorbable cellular cubic-composite scaffolds for use in bone reconstruction. J. R. Soc. Interface 2006, 3, 805–821. [Google Scholar] [CrossRef]
- Cirillo, D.; Rachiglio, A.M.; La Montagna, R.; Giordano, A.; Normanno, N. Leptin signaling in breast cancer: An overview. J. Cell. Biochem. 2008, 105, 956–964. [Google Scholar] [CrossRef]
- Tartaglia, L.A.; Dembski, M.; Weng, X.; Deng, N.; Culpepper, J.; Devos, R.; Richards, G.J.; Campfield, L.A.; Clark, F.T.; Deeds, J.; et al. Identification and expression cloning of a leptin receptor, OB-R. Cell 1995, 83, 1263–1271. [Google Scholar] [CrossRef] [Green Version]
- Winick, J.D.; Friedman, J.M.; Stoffel, M. Identification of microsatellite markers linked to the human leptin receptor gene on chromosome 1. Genomics 1996, 36. [Google Scholar] [CrossRef]
- Desai, B.N.; Krapivinsky, G.; Navarro, B.; Krapivinsky, L.; Carter, B.C.; Febvay, S.; Delling, M.; Penumaka, A.; Ramsey, I.S.; Manasian, Y.; et al. Cleavage of TRPM7 releases the kinase domain from the ion channel and regulates its participation in fas-induced apoptosis. Dev. Cell 2012, 22, 1149–1162. [Google Scholar] [CrossRef] [Green Version]
- Yang, M.; Arai, A.; Udagawa, N.; Hiraga, T.; Lijuan, Z.; Ito, S.; Komori, T.; Moriishi, T.; Matsuo, K.; Shimoda, K.; et al. Osteogenic factor runx2 marks a subset of leptin receptor-positive cells that sit atop the bone marrow stromal cell hierarchy. Sci. Rep. 2017, 7, 4928. [Google Scholar] [CrossRef]
- Zhou, B.O.; Yue, R.; Murphy, M.M.; Peyer, J.G.; Morrison, S.J. Leptin-Receptor-Expressing mesenchymal stromal cells represent the main source of bone formed by adult bone marrow. Cell Stem Cell 2014, 15, 154–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sowińska-Seidler, A.; Olech, E.M.; Socha, M.; Larysz, D.; Jamsheer, A. Novel 1q22-q23.1 duplication in a patient with lambdoid and metopic craniosynostosis, muscular hypotonia, and psychomotor retardation. J. Appl. Genet. 2018, 59, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Wu, J.; Jin, G.; Li, L.; Li, Z.; Li, C. Research of osteoblastic induced rat bone marrow mesenchymal stem cells cultured on β-TCP/PLLA porous scaffold. Int. J. Clin. Exp. Med. 2015, 8, 3202–3209. [Google Scholar] [PubMed]
- Horowitz, R.; Mazor, Z.; Foitzik, C.; Prasad, H.; Rohrer, M.; Palti, A. β-tricalcium phosphate as bone substitute material: Properties and clinical applications. J. Osseointegration 2010, 2, 61–68. [Google Scholar]
- Lim, L.-T.; Cink, K.; Vanyo, T. Processing of poly (lactic acid). In Poly (Lactic Acid): Synthesis, Structures, Properties, Processing and Applications; Auras, R., Lim, L.T., Selke, S.E.M., Tsuji, H., Eds.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2010; pp. 189–215. [Google Scholar]
- Nazre, A.; Lin, S. Theoretical strength comparison of bioabsorbable (PLLA) plates and conventional stainless steel and titanium plates used in internal fracture fixation. Clin. Lab. Perform. Bone Plates 1994. [Google Scholar] [CrossRef]
- Ehrenfried, L.M.; Farrar, D.; Cameron, R.E. The degradation properties of co-continuous calcium phosphate polyester composites: Insights with synchrotron micro-computer tomography. J. R. Soc. Interface 2010, 7, S663–S674. [Google Scholar] [CrossRef] [Green Version]
- Lin, F.; Wang, X.; Wang, Y.; Yang, Y.; Li, Y. Preparation and biocompatibility of electrospinning PDLLA/β-TCP/collagen for peripheral nerve regeneration. RSC Adv. 2017, 7, 41593–41602. [Google Scholar] [CrossRef] [Green Version]
- Lin, F.-H.; Chen, T.-M.; Lin, C.-P.; Lee, C.-J. The merit of sintered PDLLA/TCP composites in management of bone fracture internal fixation. Artif. Organs 1999, 23, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Galow, A.-M.; Rebl, A.; Koczan, D.; Bonk, S.M.; Baumann, W.; Gimsa, J. Increased osteoblast viability at alkaline pH in vitro provides a new perspective on bone regeneration. Biochem. Biophys. Rep. 2017, 10, 17–25. [Google Scholar] [CrossRef]
- EPA. Biopesticides Registration Action Document L-Lactic Acid; EPA: Washington, DC, USA, 2009; pp. 1–22. [Google Scholar]
- Kang, K.P.; Lee, S.; Kang, S.K. D-Lactic acidosis in humans: Review of update. Electrolyte Blood Press. 2006, 4, 53. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Zachman, A.L.; Chun, Y.W.; Shen, F.-W.; Hwang, Y.-S.; Sung, H.-J. Polymeric stent materials dysregulate macrophage and endothelial cell functions: Implications for coronary artery stent. Int. J. Cardiol. 2014, 174, 688–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, H.; Wang, C.; Xu, Y.; Huang, X.; He, X.; Zhang, C.; Lu, J. Pressure-Controlled crystallization of stereocomplex crystals in enantiomeric polylactides with remarkably enhanced hydrolytic degradation. CrystEngComm 2018, 20, 7337–7347. [Google Scholar] [CrossRef]
- Ngo, H.X.; Dong, Q.N.; Bai, Y.; Sha, J.; Ishizuka, S.; Okui, T.; Sukegawa, S.; Kanno, T. Bone regeneration capacity of newly developed uncalcined/unsintered hydroxyapatite and poly-l-lactide-co-glycolide sheet in maxillofacial surgery: An in vivo study. Nanomaterials 2020, 11, 22. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Components (wt%) | Size (mm) Av. ± SD | Porosity (%) Av. ± S.D. | Weight (g) Av. ± SD | Density (g/cm3) Av. ± SD | |||
|---|---|---|---|---|---|---|---|
| β-TCP | PDLLA | Diameter | Thickness | ||||
| β-TCP/PDLLA | 70 | 30 | 4.0 ± 0.2 | 2.0 ± 0.2 | 70 ± 5 | 0.017 ± 0.001 | 0.68 ± 0.04 |
| β-TCP | 100 | 0 | 4.0 ± 0.2 | 2.0 ± 0.2 | 77.5 ± 4.5 | 0.016 ± 0.001 | 0.69 ± 0.06 |
| PDLLA | 0 | 100 | 4.0 ± 0.2 | 2.0 ± 0.2 | 70 ± 5 | 0.008 ± 0.001 | 0.37 ± 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toda, E.; Bai, Y.; Sha, J.; Dong, Q.N.; Ngo, H.X.; Suyama, T.; Miyamoto, K.; Matsuzaki, Y.; Kanno, T. Feasibility of Application of the Newly Developed Nano-Biomaterial, β-TCP/PDLLA, in Maxillofacial Reconstructive Surgery: A Pilot Rat Study. Nanomaterials 2021, 11, 303. https://doi.org/10.3390/nano11020303
Toda E, Bai Y, Sha J, Dong QN, Ngo HX, Suyama T, Miyamoto K, Matsuzaki Y, Kanno T. Feasibility of Application of the Newly Developed Nano-Biomaterial, β-TCP/PDLLA, in Maxillofacial Reconstructive Surgery: A Pilot Rat Study. Nanomaterials. 2021; 11(2):303. https://doi.org/10.3390/nano11020303
Chicago/Turabian StyleToda, Erina, Yunpeng Bai, Jingjing Sha, Quang Ngoc Dong, Huy Xuan Ngo, Takashi Suyama, Kenichi Miyamoto, Yumi Matsuzaki, and Takahiro Kanno. 2021. "Feasibility of Application of the Newly Developed Nano-Biomaterial, β-TCP/PDLLA, in Maxillofacial Reconstructive Surgery: A Pilot Rat Study" Nanomaterials 11, no. 2: 303. https://doi.org/10.3390/nano11020303