Abstract
Personal and physical injuries are two of the most relevant costs to hospitals. Hospital laundries are sources of these costs due to the physical and health risks present in the clothes and the activities performed. Energy and environmental risk and infrastructure issues also incur operational costs to these organizations and to the health system. This research analyzes the social, environmental, and economic risk in the hospital laundry process, through a multiple-case-study design. Data collection methods include interviews regarding three hospital laundry services in Brazil. The processes of these laundry services have a high consumption of resources (water and energy) and a substantial generation of solid and liquid wastes. Cost reduction actions include pooled laundry services and material substitution. There are also social and environmental risks, the most frequent being ergonomic, biological, and chemical hazards, and injures from sharp devices inadequately disposed. Hospital laundries need more sustainable operations, not only in the infrastructure, but also mostly in the awareness of leaders and teams about the importance of their engagements to resource management and waste reduction in laundry. It is opportune to convince professionals and users about changing habits that do not prioritize sustainability, especially its social and environmental aspects.
1. Introduction
The search for quality improvement in goods and services by health institutions, public and private, is increasing. On one hand, society is increasingly demanding regarding its rights to and safety of services consumed [1,2]. On the other hand, health service providers are seeking to rationalize their costs (the costs were deemed as a risk factor for economic sustainability in this research) [3].
Hospitals are committed to the provision of services with quality, efficiency, and effectiveness [4]. This commitment requires that all sectors involved (such as administration, laboratories, operating rooms, resource management, laundry, cafeteria, and maintenance) interact to provide favorable working conditions for the care of patients in the best possible way [5,6].
The discussions about the topic of sustainability or management in organizations gained notoriety in recent years [7,8], mainly in health institutions [9]. According to Hamel [7], and Lawler and Worley [8], management is the combustion engine; it is a mature technology that must now be reinvented for a new era, in which people must be the priority; in other words, management is key for sustainability. For Lopes et al. [10,11], the theme of sustainability in healthcare is gaining notoriety in research, with proposals for improvement in the sustainability of both the internal and external context of hospitals. Sustainable development and health are interdependent, reducing hospital sustainability to cost reduction or social assistance.
Hospitals have critical roles in society and their operations have major social and environmental risk [12,13]. In fact, the operations of hospitals consume a high amount of resources and, consequently, generate an important amount of solid and liquid waste. The high consumption of the resources, materials, electricity [12], and water causes the hospitals [14] to have a significant negative effect on the environment, which directly affects the hospital’s sustainability [15] and has a direct relationship with environmental management [16,17].
Operational costs and personnel represent a significant amount of the hospital costing structure. In particular, service staff and infrastructure may represent a significant source of hidden costs, due to their nature of highly standardized and sequential processes. In many hospitals, such services are frequently relegated to a second or third level of priority by the managers, resulting in low investment and undertrained staff. Such a combination, along with the misconception that “commoditized services are similar everywhere” (thus excluding quality and efficiency from the costing equation), may result in increased costs, increased prices to patients, and sustainability risks to society.
Among the hospital supporting sectors, laundry services are responsible for processing clothes [18,19], bed linen, and surgical linen, restoring their condition for perfect hygiene and conservation, in addition to distributing adequate amounts in each hospital sector [20,21]. In the hospital laundry service, workers are exposed to physical, chemical, and biological threats due to waste, and they generally work in a place without ergonomic structures.
According to Medeiros et al. [22], in environments with unfavorable working conditions (such as those generated by the presence of hazardous wastes), workers can become victims of a major source of tension in the accomplishment of tasks, resulting in discomfort and dissatisfaction, increasing the risk of accidents, decreasing productivity, and even damaging the workers’ health [23]. Activities in the hospital laundry service require manipulation machines and clothes, and are most often performed improperly without giving the right importance to the attitudes of the workers and with excessive weight handling and inadequate management of clothing. These conditions may incur increased costs to the hospital due to physical injuries, labor lawsuits, absenteeism, and a waste of energy and resources.
In the long run, organizations should seek to build their sustainability with the social, environmental, and economic tripod under the triple bottom line (3BL) concept spread by Elkington [24]; as such, comprehensive views, such as sustainable transitions [25,26], would be beneficial for driving hospitals toward sustainability. For hospital laundry services, this paper spouses the concept of sustainability in which Laitala et al. [14] propose a three-dimensional view of social, environmental, and economic sustainability as described under the 3BL concept.
This research aims to analyze the social, environmental, and economic risk in the hospital laundry process. This research is divided into six sections, including this introduction. The second section describes the work process and risks in hospital laundry services. The third section presents the research methods. The fourth section describes the results, which demonstrate the social, environmental, and economic risk. The fifth section discusses the results. The sixth section finalizes the paper with conclusions.
2. The Hospital Laundry
The processing healthcare is an activity of support that greatly influences the quality of healthcare, especially with regards to the security and comfort of the patient and the worker [27,28,29]. Although the activities carried out in this service have not undergone major changes in recent years [5], there was a maturation in relation to the risk and the need for greater control of the resources and sanitary control of their activities. Therefore, it is necessary to update the guidelines relating to the processing of clothes used in health services [14,29] focusing on the control and prevention of risks associated with this activity [15,30].
The Brazilian National Health Surveillance Agency (ANVISA), as a coordinator of the Brazilian National Health Surveillance System, made a reference guide to the activities involved in processing healthcare clothes, focusing on the risks associated with these activities. The concept of risk is the main theoretical reference of health surveillance activities, and the elimination of risks refers to a minimization of its manifestation to statistically significant levels. The definition of risk encompasses a variety of probability measures including those based on statistical data or subjective judgments [14,31].
Risk is the probability of an occurrence of a harmful event to health [1], related to concrete objects under sanitary control [32], i.e., the probability of an adverse event that, in the case of health services [33], affects the integrity of the patient, the healthcare team, or the community where the service is located [34]. The clothing processing unit performs various activities involving risks to the health of workers, users, and the environment and, therefore, it is a major concern for health monitoring [33]. The clothing processing service is an area of little health study, which can pose a serious problem, particularly for the conditions and risks of the workers in this sector, which undergoes physical, chemical, biological, ergonomic, psychosocial, and accidental issues [33,35,36,37].
Hospitals are typically considered unhealthy places and, often, due to concern for the quality of service and the safety of users, they neglect the occupational hazards to which workers are exposed [27,38]. According to the Organic Law of the Brazilian Health, the prevention of occupational diseases can add value to humans. According to Figure 1, hospital laundry services aim to transform all the dirty or contaminated clothing used in the hospital into clean clothes through their collection, separation, processing, manufacture, repair, renovation, supply, and distribution [14,39]. The processing of the clothes should be carried out so that they do not pose a contamination threat to vehicle users and workers [40,41].
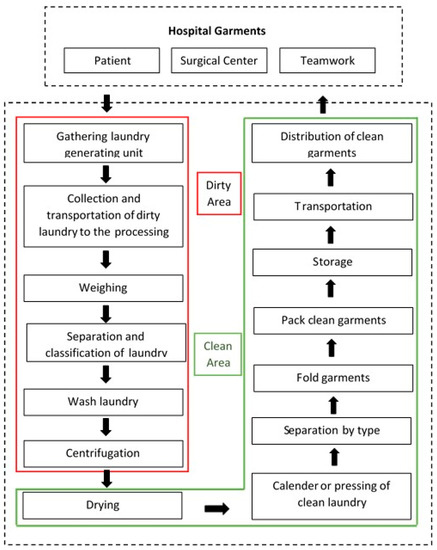
Figure 1.
The process steps in laundry services.
Microbial barriers separate the laundry process into two distinct areas: the dirty room for receiving, weighing, and sorting the laundry, and the clean room with areas for centrifugation, drying, separation, folding, storage, distribution, calendaring, pressing, ironing, and sewing. These barriers will only be effective if there are washers with two access doors, one for each area. They should preferably be located on a single floor, on the ground floor next to the central supply, because of the limited access and movement of the workers in this sector. The unit should also have personal protective resources such as private clothes, boots/anti-slip footwear, waterproof aprons, apron long sleeves, rubber gloves, caps, masks, and eye protection.
A study conducted in order to identify the risks for workers in the dirty area of a laundry service identified significant exposure of these individuals to biological agents, especially for materials such as syringes, scalpel blades, surgical clamps, and scissors; these are instruments capable of causing communicable diseases such as hepatitis and acquired immunodeficiency syndrome (AIDS) [14]. The study also cited other utensils found coming with the clothing that can injure workers, such as basins, thermal bags, food trays, and hospital waste.
Like other sectors of the hospital, the laundry service can pose risks for workers including lesions with sharp objects, hearing problems caused by noise of the machines, accidents, and musculoskeletal injuries due to exposure to chemical, biological, physical, mechanical, accidental, non-ergonomic, and psychosocial items [40,42]. Therefore, it is mandatory for employers to plan an environmental risk prevention program (ERPP) that anticipates the recognition, the evaluation, and the consequent control of the occurrence of risks that may exist in the workplace in order to ensure disease prevention for all workers. Laitala et al. [14] and Vecchio et al. [27] found hospital laundry workers doing their activities in poor working conditions in relation to the environment and devices, and that the workers reported some discomfort in some part of their bodies.
Hospital occupational accidents incur increased costs, reducing margins, and, in the long run, increased pressure for higher prices or financial support from governments. Most accidents occur due to injuries caused by needles discarded improperly. Vecchio et al. [27] shed light on the performance of serological tests for hepatitis, AIDS, and antiretroviral therapy. The lack of systematic data on occupational accidents with biological or chemical support in this area, among others, makes it difficult to understand the magnitude of these diseases, avoiding the intervention of control measures [43].
3. Materials and Methods
This study is a multiple-case-study research. The three hospital laundry services were located in the central region of Rio Grande do Sul, Brazil. Two of the hospitals were small (HE with 136 beds, and HR with 120 beds) and the third hospital was a mid-range size (HS with 234 beds). The three hospitals serve private health plans and the Unified Brazilian Health System (SUS). At the three hospital laundry services, all employees completed high school, and the transportation of patients to the hospital occurs via car, bus, and walking.
We used data triangulation for the analysis of results. According to Yin [44], triangulation allows for greater reliability and validity of results than when conclusions are reached based on a sole source of information. It equally offers more accurate results, as different sources are compared against each other. These case studies are based on unstructured face-to-face interviews and observations that the researchers conducted in the laundry services of three hospitals.
This study used direct observation [44] during the field visits to the sites, with the purpose of observing behavior or relevant environmental conditions. The unstructured face-to-face interviews and observations followed a guide based on the hospital field experiences (on average five years) of the four researchers of this paper. Firstly, each of them separately listed issues about the sustainability in the laundry services (12, 16, 19, and 28 issues); afterward, they met and discussed all issues and reached a consensus on 28 final issues for the guide, as depicted in Table 1.

Table 1.
The guide for sustainability in laundry services.
The interviews had two rounds. During the first round, the researchers conducted the interviews based on the guide; immediately after the first round, the researchers met to analyze the data and to find inconsistencies between the workers interviewed. The second round aimed at reaching consensus between the workers interviewed. These interviews were intended to help gain a deeper understanding of the linkages between motives and risks of sustainability in hospital laundry services. The unstructured face-to-face interviews were conducted with all the employees of the laundry that were present at the moment of the site visits. HS was the only hospital with a night shift. For comparability purposes, only the morning and afternoon shifts were interviewed in all three sites. Table 2 provides general information about the hospitals and site visits.
Table 2.
An overview of the characteristics of the three hospitals (HS, HE, and HR).
3.1. HS Laundry Service
HS is situated in the center of a city with a population of about 130,000 inhabitants. This city is the 12th best city in the state Rio Grande do Sul to live and it is among the top 100 best cities to live in Brazil; this annual survey monitors the socioeconomic levels, assessing the conditions of education, health, employment, and income of more than five thousand Brazilian municipalities (FIRJAN’s Municipal Development Index—IFDM, 2015). Tobacco plantations and cigarette manufacturing generate around 60% of the local economy.
HS is a university hospital and its beds are available to the SUS, health plans, and private care. It is currently the main health center of its region. It has about 23,000 square meters of building area, about 900 employees in three work shifts (24 h/365 days), and 211 physicians who make up the medical staff; they received in 2012 the Top Human Being award in the business category (Brazilian Association of Human Resources—ABRH-RS). It is a charity, non-profit organization, recognized as a federal, state, and municipal public utility, which allows it to receive public funding from these three levels. It offers services to inpatients and outpatients, mainly to the SUS, and it provides diagnostic services and treatment procedures.
The interview was firstly performed with the laundry supervisor, an engineering graduate with HS laundry experience of one year and three months; he was hired to take over the supervision of the HS laundry process. The HS laundry process has a team of 15 laundry assistants (10 men and five women) with an average age of 38 years, with the highest and lowest ages of 43 and 21. The longest time of experience in the laundry service is nine years, and the shortest time is nine months.
3.2. HE Laundry Service
HE is situated in the center of a city with a population of about 30,600 inhabitants. It is one of the largest industrial centers of the region and it had great momentum with the installation of roads and a hydro-railway junction. The economy is based on industry (especially manufacturing), trade, and agriculture.
HE has about 12,000 square meters of built area. The team consists of approximately 320 employees and 69 doctors of the medical staff, providing 119 beds for hospitalization and 17 beds for outpatient observation. The interview was first performed with the laundry supervisor, a student who has experience in laundry for two years and seven months and has worked for three years at HE. The laundry process has a team of 12 laundry assistants (10 men and two women) with an average age of 33, with the highest age of 48 the lowest age of 23. The longest time of experience in the laundry process is 6.5 years, and the shortest time is two years.
3.3. HR Laundry Service
HR is located in the center of a city that has a population of about 37,600 people and is in the central region of Rio Grande do Sul. The economy of the city counts on agriculture, livestock, and industrial activities, focused on the processing of agricultural products and the production of metallurgy, clothing, iron window frames, furniture, steel appliances, and wooden frames. The beds in HR are available exclusively to the SUS. The team consists of 166 workers and six doctors of the medical staff.
The interview was first carried out with the laundry coordinator, who has full high-school education and has laundry experience of four years and five months, with six years in HR. The laundry process has a team of eight (all men) with an average age of 36, with the highest age of 42 and the lowest age of 21. The longest time of experience is six years, and the shortest time is two years.
3.4. Unstructured Face-to-Face Interviews and Observations
Table 3 shows a summary of similarities and differences between the three hospital laundry services, according to the guide (Table 1), from which the interviews and observations were derived.
Table 3.
The implementation of the guide in the laundry services.
4. Results
This research addressed the social and environmental risks in the three hospital laundry services (HE, HS, and HR) through the analyses of biological, physical, ergonomic, chemical hazards, and accidents. Analyses were carried out together with workers and the leadership of each laundry service. A well-planned clothing processing unit might be efficient in its processes, saving operating and maintenance costs, while providing reliability, safety, and comfort for all users, i.e., patients, caregivers, and professionals.
Based on the unstructured face-to-face interviews and observations, it was possible to develop a map of the area showing the risks in each area of the laundry sector. Figure 2 depicts the map and shows the flow of collecting the hospital linen, the washing process, and the process for clean clothes. It provides an overview of risks and, consequently, the costs of hospital laundry services. The map was validated by the heads of the laundry services. It will be used in future training sessions with workers in order to attain a better understanding of the activities as a tool for continuous improvement of the process.
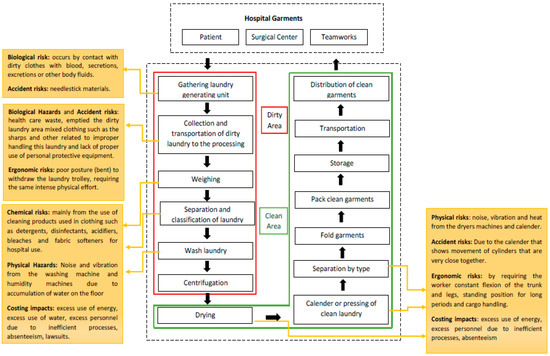
Figure 2.
Identification of risks in laundry services.
It was observed that the area with the greatest risk is the soiled area, due to risks of contamination, handling, chemical, and ergonomic hazards. The interviews were useful for the analysis of risk in laundry services in the social, environmental, and economic dimensions of sustainability.
4.1. Social Risks
It was observed that workers in the laundry sector need to carry out their activities with high productivity, often generating discomfort related to the environment and location of the devices. According to them, the discomfort can be related to certain activities they consider to be “heavier”. According to issues I-13 and I-14 in Table 3, the majority of the interviewees acknowledged that there are risks in the laundry services. The prevalence of risks lies in biological agents and physical and chemical accidents. Although less frequent, ergonomic risks were also mentioned by some interviewees (item I-9). According to issue I-4, the main reason for the removal of laundry workers is the prevalence of cold and flu in the winter.
All heads of laundries reported some kind of industrial accident last year in the laundry area with sharp objects, by fall or repetitive activity. According to issues I-5, I-6, I-7, and I-8, accidents occurred at work in the laundry process, which characterized it as a hazardous area. They were due to an improper disposal of sharp objects, due to the lack of attention from the nursing and medical staff in areas of direct patient care. Materials like needles, scalpels, and surgical instruments favoring accidents were mixed with clothes by mistake.
The Collegiate Board Resolution of the Brazilian National Health Surveillance Agency (ANVISA) n. 306/2004 states that sharp objects are to be disposed separately at the site of their generation, immediately after use, in suitable containers to prevent puncture, rupture, and leak. It also regulates that all workers of the institution must know the system adopted for waste management, including the practice of segregation and packaging for accident prevention.
4.2. Environmental Risks
The observed environmental risks mentioned during the research with regards to the environment and the population are enlisted in issues I-22, I-23, I-24, and I-25: high consumption of water, high energy consumption, smoke emission by boilers, generation of solid and liquid waste, and processing and disposal of water with chemicals used in decontamination and sterilization processes. During the interview, it was commented that most hospitals are concerned about the environmental risks of the laundry process. Regarding training (issue I-10), the workers participated annually in one or two training sessions focused on environmental management in order to update them about the new operating procedures.
4.3. Economic Risks
With regards to the economic risks of laundry services, the observed processes need improved management and increased efficiency in resource allocation. Excess motion, lack of well-defined processes, lack of visual controls, and rework were found as the most frequent causes of excess personnel. In addition, poor maintenance and low investment result in excess waste of energy and water, leading to increased costs. Thus, most of the risks in the social and environmental dimensions undermine the economic dimension, generating unnecessary costs for hospitals.
Hospital managers mentioned concerns about low investment in their laundry services. Nevertheless, all the interviewees mentioned an absence of funds to invest in low-priority areas. Even maintenance was mentioned as low priority. One of the hospitals’ managers also referred to using only corrective maintenance for the laundry equipment, and, in the case of equipment failure, contracting external services at higher costs. This would be an alternative if planned under a strategic service, but evidence shows that the case mentioned was due to a poor systemic understanding of the costing structure. This leads to a vicious circle of increased waste leading to reduced margins, thus leading to low investment capacity to reduce waste.
Positive outcomes were also identified, yet not implemented. One hospital mentioned a pilot study on using disposable bed linen. Such linen, despite the higher material costs, eliminates the need for laundry services, thus reducing the associated global costs. Water and energy costs and waste are significantly reduced, as well as personnel costs. According to the supplier, the biodegradable materials used also contribute to reducing environmental risk associated with solid waste. Another hospital mentioned a study on creating a polled hospital laundry service center, co-managed by the associated hospitals. Preliminary forecasts indicate reduced costs, even when considering the increased footprint due to transportation. No assessment on environmental aspects was made.
5. Discussion
Currently, hospitals are at different points in their journey toward sustainability. In this case study, HS leads the development of best practices, while others are addressing the issue for the first time. The hospital’s management must consider options and define the best steps for their organizations, as the Hamel [7] study points out. Overall, hidden costs due to inadequate management, and social and environmental issues lead to inflated support operations in the hospitals. Lack of use of operation management principles lead to inefficient [7] installations, thus resulting in excess personnel, high energy consumption, high water consumption, and waste [8].
According to the Global Green and Healthy Hospitals Agenda [45], hospitals are responsible for about 10% of all Brazilian commercial energy consumption. In the United States (US), consumption is 5.5% of total commercial energy according to the US Energy Information Administration [46]. According to the report published by Scheider Electric [47], since 1995, energy consumption increased by 36% in the healthcare sector. It is now possible to adopt the green building concept in construction, with an architecture that favors natural lighting and ambient temperature maintenance through the use of materials for this purpose. This type of construction allows for savings in inputs like electricity, water, and heating.
Nevertheless, environmental sustainability in hospitals is more than buying a single piece of efficient energy device or regulation. The efficient hospitals create a culture of sustainability that provides lasting changes. Efforts lead to a sustainability that does not happen in hospitals without a long-term vision commitment. When these efforts result from a strategic thought, leaders who are committed to create a culture of change [7] increase the reduction in expenditures such as electricity and other costs through sustainability efforts. Boone [48] conducted an exploratory study examining the organizational approaches of eight healthcare systems with relatively successful sustainability initiatives. Boone [48] states that the values of the sustainability initiative must be reflected in the organization’s high-level mission, vision, or values, linking the high-level mission to help underscore the relationship between sustainable operations and patient care. This also defines organizational norms and helps guide decision-making. These attitudes are only possible if the hospitals find solutions that work by themselves. The hospitals that are searching for a sustainable performance depend on the awareness of their leaders and their teams [7,48], related to the need of commitment to change processes [8]. They need to convince people about the importance of changing habits that do not prioritize the environment. There are certifications, such as ISO 14001 (accreditation of the Environmental Management System) and certification by the Joint Commission International (JCI), to verify the awareness and the focus on minimizing the effect on the environment. In this context, patient care remains the priority of a hospital; anyway, the actions of the hospitals should also be related to the procedures and indicators that improve productivity by reducing environmental damage as a whole [48].
When interviewing the three hospitals about whether the institutions were concerned about sustainability embedded in its guidelines, it was observed that HR did not define its mission, vision, and institutional values, as reported in issue I-26 in Table 3. In relation to HS and HE, they already defined their missions, visions, and institutional values. The concern is greater, because there are several internal programs such as waste management, environmental management, and social actions with practices to promote community health. In addition to the previously mentioned factors, the treatments of wastewater and medical waste are items that deserve additional attention in hospitals. Exclusive sectors for these two areas are necessary due to the contamination risks they bring along. These processes are continuous and dynamic in the pursuit of reducing environmental and social risk.
6. Conclusions
When considering implementing the concept of sustainability in organizations, health systems and, in particular, hospitals are negatively at risk due to the growth of global sustainability issues such as climate change, energy crises, and the scarcity of natural resources. It is worth mentioning the responsibility of health systems in these problems, because in some cases they fail to exercise their primary function of promoting health, and they generate adverse effects on the environment, the society, and the economy.
The theme of sustainable development has synergy with the promotion of health. It is noteworthy that this correlation between them can be completed from the health promotion definition established by the World Health Organization, where it is seen as the process of enabling people to increase control over their health, thereby improving it. This process moves beyond a focus on individual behavior, heading toward a wide range of social, environmental, and economic interventions. Sustainability programs should reflect the unique needs and characteristics of each organization; these programs in enterprises require not only time, but significant cultural changes. In the hospitals, these programs eventually permeate all aspects of the institution, such as food, resource/material management, and nursing staff at all levels, and it embeds cultural and educational facets.
This research allowed an analysis of the effects on social, environmental, and economic sustainability from the point of view of leaders and workers in three Brazilian hospital laundry services. It was found that the hospital laundry services in some work situations favor physical, chemical, biological, ergonomic, and accidental risk exposures. Most managers recognize that there are risks in the laundry room and report a lack of care in the disposal of sharp objects by the nursing and medical staff as a major cause of risk exposure. This fact shows the importance of involving other sectors in preventing the aggravations of support services such as the laundry sector. Other risks visible and perceived by managers were the physical and chemical risks arising from the laundry process such as electric shock and the handling of chemicals without individual protection equipment, facilitating diseases by contact with chemicals.
In order to improve working conditions, consequently reducing the risk of accidents and diseases at work, it is necessary to lay preventive health promotion in the internal environment of the institution. Training can guide the use of personal protective resources and safe machine handling, as well as procedures of manual activities that can promote ergonomics and precautions for handling chemicals. Hidden costs due to poor management, lack of operation management principles, and inefficient handling of environmental and social risks of the laundry services result, in the long term, in increased costs to the hospital operation. The processes of the laundry services analyzed have a high consumption of water and energy and a substantial generation of solid and liquid wastes. As mentioned, cost reduction actions foreseen include pooled laundry services and material substitution.
Finally, hospital leadership needs to understand the role of their business in the face of social, environmental, and economic issues. The process of identifying the risk should help the hospitals in order to reduce actions that could harm the society and the environment. In relation to promoting the health of the hospital workers, it is necessary to seek alternatives that enable management to minimize this risk in the hospitals.
Author Contributions
Writing: C.M.L.; providing case and idea: C.M.L., A.J.S., and G.V.; providing revised advice: M.N.M.d.C., G.V. and A.L.K.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Campion, N.; Thiel, C.L.; Woods, N.C.; Swanzy, L.; Landis, A.E.; Bilec, M.M. Sustainable healthcare and environmental life-cycle risks of disposable supplies: A focus on disposable custom packs. J. Clean. Prod. 2015, 94, 46–55. [Google Scholar] [CrossRef]
- Vezzoli, C.; Ceschin, F.; Diehl, J.C.; Kohtala, C. New design challenges to widely implement ‘Sustainable Producte Service Systems’. J. Clean. Prod. 2015, 97, 1–12. [Google Scholar] [CrossRef]
- Boons, F.; Lüdeke-Freund, F. Business models for sustainable innovation: State-of-the-art and steps towards a research agenda. J. Clean. Prod. 2013, 45, 9–19. [Google Scholar] [CrossRef]
- Xin, Y. Comparison of hospital medical waste generation rate based on diagnosis-related groups. J. Clean. Prod. 2015, 100, 202–207. [Google Scholar] [CrossRef]
- Asandului, L.; Roman, M.; Fatulescu, P. The Efficiency of Healthcare Systems in Europe: A Data Envelopment Analysis Approach. Procedia Econ. Financ. 2014, 10, 261–268. [Google Scholar] [CrossRef]
- Bhakoo, V.; Choi, T. The iron cage exposed: Institutional pressures and heterogeneity across the healthcare supply chain. J. Oper. Manag. 2013, 31, 432–449. [Google Scholar] [CrossRef]
- Hamel, G. Moon shots for management. Harvard Bus. Rev. 2009, 87, 91–98. [Google Scholar]
- Lawler, E.E.; Worley, C.G. Designing organizations for sustainable effectiveness. Organ. Dyn. 2012, 4, 265–270. [Google Scholar] [CrossRef]
- Maley, J. Sustainability: The missing element in performance management. Asia-Pac. J. Bus. Adm. 2014, 6, 190–205. [Google Scholar] [CrossRef]
- Lopes, C.M.; Scavarda, A.; Vaccaro, G.; Pohlmann, C.; Korzenowski, A. Perspective of Business Models and Innovation for Sustainability Transition in Hospitals. Sustainability 2019, 11, 5. [Google Scholar] [CrossRef]
- Lopes, C.M.; Scavarda, A.J.; Carvalho, M.N.M.D.; Korzenowski, A.L. The Business Model and Innovation Analyses: The Sustainable Transition Obstacles and Drivers for the Hospital Supply Chains. Resources 2019, 8, 3. [Google Scholar] [CrossRef]
- Raza, S.S.; Janajreh, I.; Ghenail, C. Sustainability index approach as a selection criteria for energy storage system of an intermittent renewable energy source. Appl. Energy 2014, 136, 909–920. [Google Scholar] [CrossRef]
- Chen, D.Q.; Preston, D.S.; Xia, W. Enhancing hospital supply chain performance: A relational view and empirical test. J. Oper. Manag. 2013, 31, 391–408. [Google Scholar] [CrossRef]
- Laitala, K.; Boks, C.; Klepp, I.G. Potential for environmental improvements in laundering. Int. J. Consum. Stud. 2011, 35, 254–265. [Google Scholar] [CrossRef]
- Lega, F.; Prenestini, A.; Spurgeon, P. Is Management Essential to Improving the Performance and Sustainability of Health Care Systems and Organizations? A Systematic Review and a Roadmap for Future Studies. Value Health 2013, 16, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Thakur, V.; Ramesh, A. Healthcare waste management research: A structured analysis and review (2005–2014). Waste Manag. Res. 2015, 33, 855–870. [Google Scholar] [CrossRef] [PubMed]
- Altenbaher, B.; Turk, S.S.; Fijan, S. Ecological parameters and disinfection effect of low temperature laundering in hospitals in Slovenia. J. Clean. Prod. 2011, 19, 253–258. [Google Scholar] [CrossRef]
- Mersha, T. Enhancing the customer contact model. J. Oper. Manag. 1990, 9, 391–405. [Google Scholar] [CrossRef]
- Butler, T.W.; Leong, G.K.; Everett, L.N. The operations management role in hospital strategic planning. J. Oper. Manag. 1996, 14, 137–156. [Google Scholar] [CrossRef]
- Tucker, A.L. The risk of operational failures on hospital nurses and their patients. J. Oper. Manag. 2004, 22, 151–169. [Google Scholar] [CrossRef]
- Chase, R.B.; Apte, U.M. A history of research in service operations: What’s the big idea? J. Oper. Manag. 2007, 25, 375–386. [Google Scholar] [CrossRef]
- Medeiros, J.F.; Ribeiro, J.L.D.; Cortimiglia, M.N. Success factors for environmentally sustainable product innovation: A systematic literature review. J. Clean. Prod. 2014, 65, 76–86. [Google Scholar] [CrossRef]
- Lee, K.H.; Saen, R.F. Measuring corporate sustainability management: A data envelopment analysis approach. Int. J. Prod. Econ. 2012, 140, 219–226. [Google Scholar] [CrossRef]
- Elkington, J. Partnerships from cannibals with forks: The triple bottom line of 21st-century business. Environ. Qual. Manag. 1998, 8, 37–51. [Google Scholar] [CrossRef]
- Geels, F.W. Ontologies, socio-technical transitions (to sustainability), and the multi-level perspective. Res. Policy 2010, 39, 495–510. [Google Scholar] [CrossRef]
- Smith, A.; Voß, J.P.; Grin, J. Innovation studies and sustainability transitions: The allure of the multi-level perspective and its challenges. Res. Policy 2010, 39, 435–448. [Google Scholar] [CrossRef]
- Vecchio, D.; Sasco, A.J.; Cann, C.I. Occupational risk in health care and research. Am. J. Ind. Med. 2003, 43, 369–397. [Google Scholar] [CrossRef]
- Senot, C.; Chandrasekaran, A.; Ward, P.T. Collaboration between service professionals during the delivery of health care: Evidence from a multiple-case study in US hospitals. J. Oper. Mana. 2016, 42, 62–79. [Google Scholar] [CrossRef]
- Johnson, K.M.; González, M.L.; Dueñas, L.; Gamero, M.; Relyea, G.; Luque, L.E.; Caniza, M.A. Improving waste segregation while reducing costs in a tertiary-care hospital in a lower–middle-income country in Central America. Waste Manag. Res. 2013, 31, 733–738. [Google Scholar] [CrossRef]
- Arce-Corrales, M.E.; Gomez-Alvarez, A.; Alvarez-Chavez, C.R. Chemical substances sources characterization in support of the health sector’s sustainability and quality in Sonora, Mexico. J. Clean. Prod. 2014, 64, 457–463. [Google Scholar] [CrossRef]
- Zhang, H.J.; Zhang, Y.H.; Wang, Y.; Yang, Y.H.; Zhang, J.; Wang, Y.L.; Wang, J.L. Investigation of medical waste management in Gansu province, China. Waste Manag. Res. 2013, 31, 655–659. [Google Scholar] [CrossRef] [PubMed]
- Allen, M.R. Effective pollution prevention in healthcare environments. J. Clean. Prod. 2006, 14, 610–615. [Google Scholar] [CrossRef]
- Fijan, S.; Cencic, A.; Sostar-Turk, S. Implementing hygiene monitoring systems in hospital laundries in order to reduce microbial contamination of hospital textiles. J. Hosp. Infect. 2005, 61, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Wood, L.C.; Chen Wang, C.; Abdul-Rahman, H.; Abdul-Nasir, N.S.J. Green hospital design: Integrating quality function deployment and end-user demands. J. Clean. Prod. 2016, 112, 903–913. [Google Scholar] [CrossRef]
- Idowu, I.; Alo, B.; Atherton, W.; Khaddar, R.A. Profile of medical waste management in two healthcare facilities in Lagos, Nigeria: A case study. Waste Manag. Res. 2013, 31, 494–501. [Google Scholar] [CrossRef] [PubMed]
- Tesfahun, E.; Kumie, A.; Legesse, W.; Kloos, H.; Beyene, A. Assessment of composition and generation rate of healthcare wastes in selected public and private hospitals of Ethiopia. Waste Manag. Res. 2014, 32, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Toktobaev, N.; Emmanuel, J.; Djumalieva, G.; Kravtsov, A.; Schüth, T. An innovative national health care waste management system in Kyrgyzstan. Waste Manag. Res. 2015, 33, 130–138. [Google Scholar]
- Clarke, C.L.; Keyes, S.E.; Wilkinson, H.; Alexjuk, J.; Wilcockson, J.; Robinson, L.; Corner, L.; Cattan, M. Organisational space for partnership and sustainability: Lessons from the implementation of the National Dementia Strategy for England. Health Soc. Care Community 2014, 22, 634–645. [Google Scholar] [CrossRef] [PubMed]
- Cai, S.; Chen, X.; Bose, I. Exploring the role of IT for environmental sustainability in China: An empirical analysis. Int. J. Prod. Econ. 2013, 146, 491–500. [Google Scholar] [CrossRef]
- Pakula, C.; Stamminger, R. Electricity and Water Consumption for Laundry Washing by Washing Machine Worldwide. In Energy Efficiency; Springer Publishing: Cham, The Netherlands, 2010. [Google Scholar]
- Ament, S.M.C.; Gillissen, F.; Moser, A.; Maessen, J.M.C.; Dirksen, C.D.; Meyenfeldt, M.F.; Weijden, T. Identification of promising strategies to sustain improvements in hospital practice: A qualitative case study. BMC Health Serv. Res. 2014, 14, 641. [Google Scholar] [CrossRef] [PubMed]
- Chesteen, S.; Helgheim, B.; Randall, T.; Wardell, D. Comparing quality of care in non-profit and for-profit nursing homes: A process perspective. J. Oper. Manag. 2005, 23, 229–242. [Google Scholar] [CrossRef]
- Gowen, C.R.; Mcfadden, K.L.; Hoobler, J.M.; Tallon, W.J. Exploring the efficacy of healthcare quality practices, employee commitment, and employee control. J. Oper. Manag. 2006, 24, 765–778. [Google Scholar] [CrossRef]
- Yin, R.K. Case Study Research: Design and Methods, 5th ed.; SAGE: London, UK, 2013. [Google Scholar]
- A Comprehensive Environmental Health Agenda for Hospitals and Health Systems Around the World. In Global Green and Healthy Hospitals Agenda; Health Care Without Harm: Reston, VA, USA, 2011.
- Energy Information Administration-US Large Hospitals Tend to Be Energy-Intensive. 2012. Available online: https://www.eia.gov/todayinenergy/detail.php?id=7670 (accessed on 13 April 2013).
- SCHNEIDER ELECTRIC. 2010 Annual Report the Global Specialist in Energy Management. Available online: https://www.schneider-electric.com/ww/2010/annual-report-2010-tcm50-274667.pdf (accessed on 13 April 2013).
- Boone, T. Creating a Culture of Sustainability; UIC Medical Center: Chicago, IL, USA, 2012. [Google Scholar]


© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).