


Clinical Features of COVID-19 Vaccine-Associated Autoimmune Hepatitis: A Systematic Review

Abstract
1. Introduction
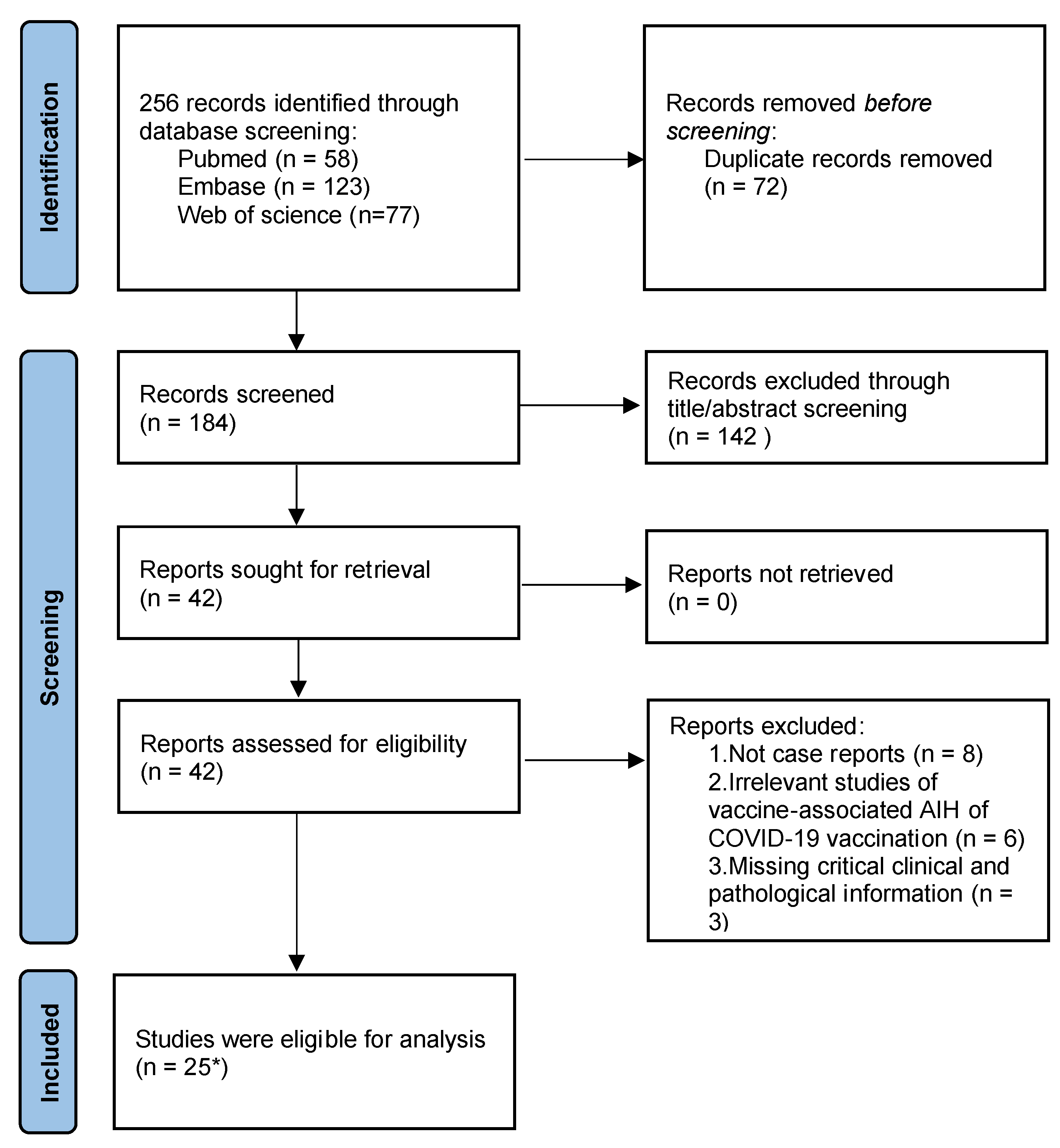
2. Methods
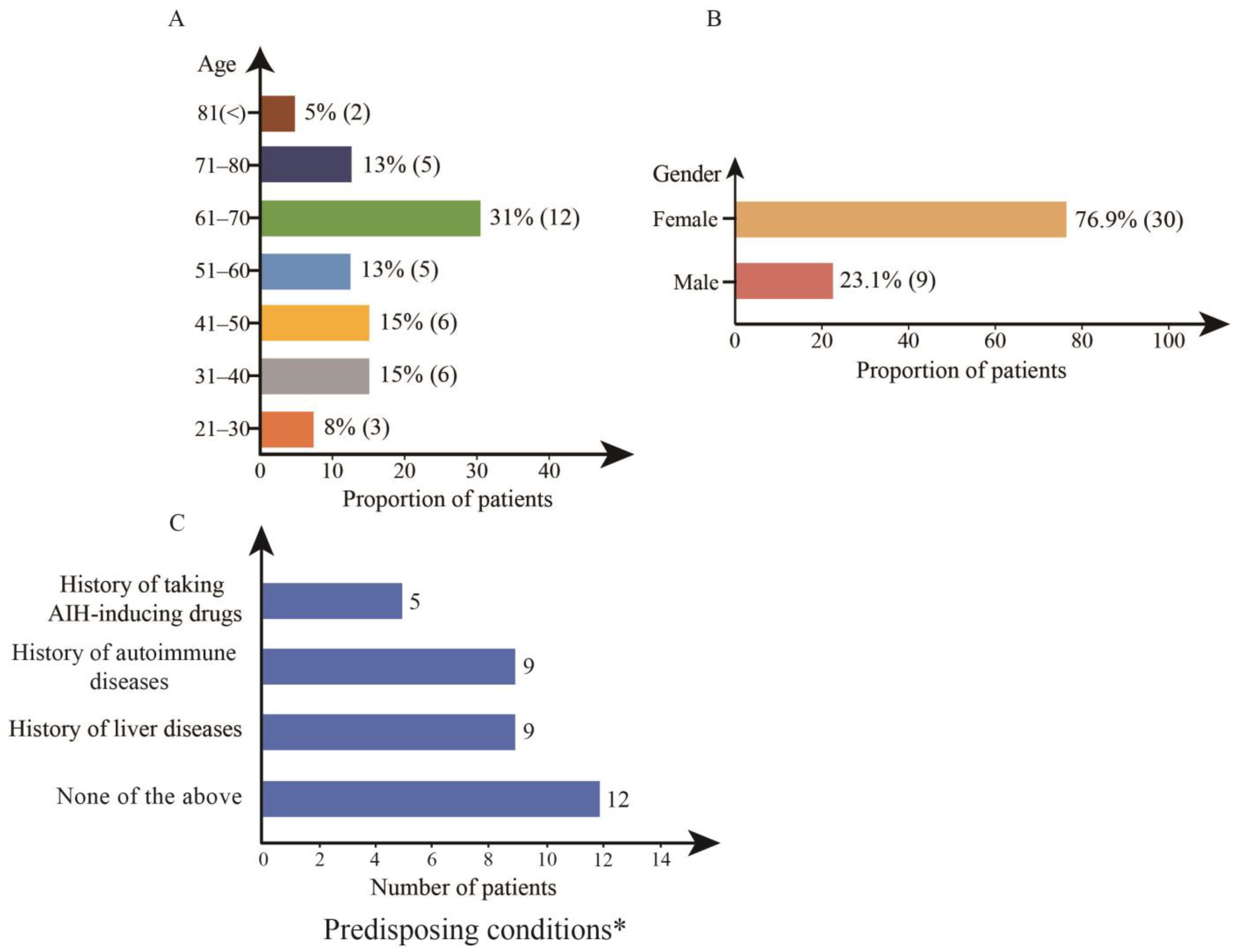
3. Characteristics of Patients with Vaccine-Associated AIH before Vaccination
4. Characteristics of Patients with Vaccine-Associated AIH after Vaccination
4.1. Time of Onset of Symptoms
4.2. Clinical Presentation of Patients with Vaccine-Associated AIH
4.3. Serological Profile of Patients with Vaccine-Associated AIH
4.4. Liver Histology with Vaccine-Associated AIH
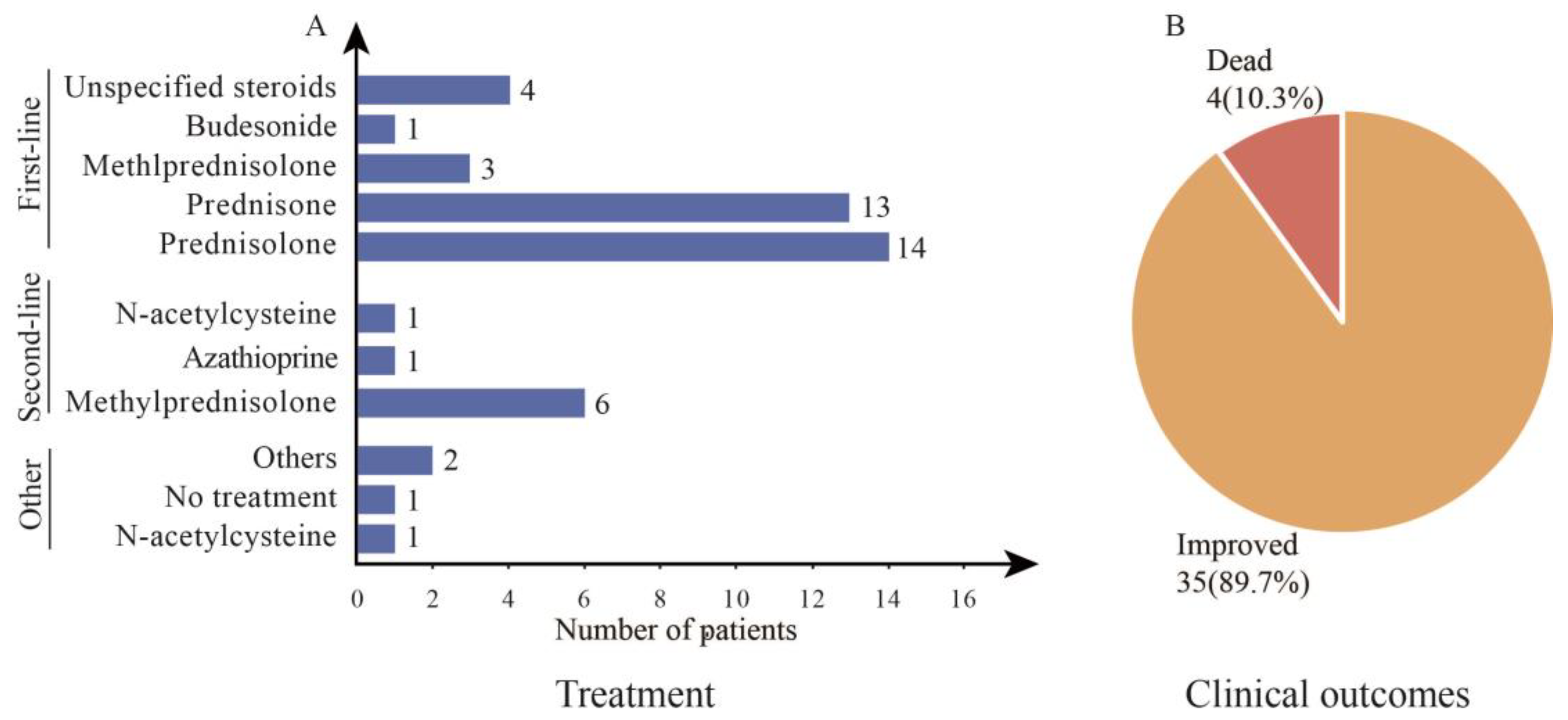
5. Treatment and Outcomes in Patients with Vaccine-Associated AIH
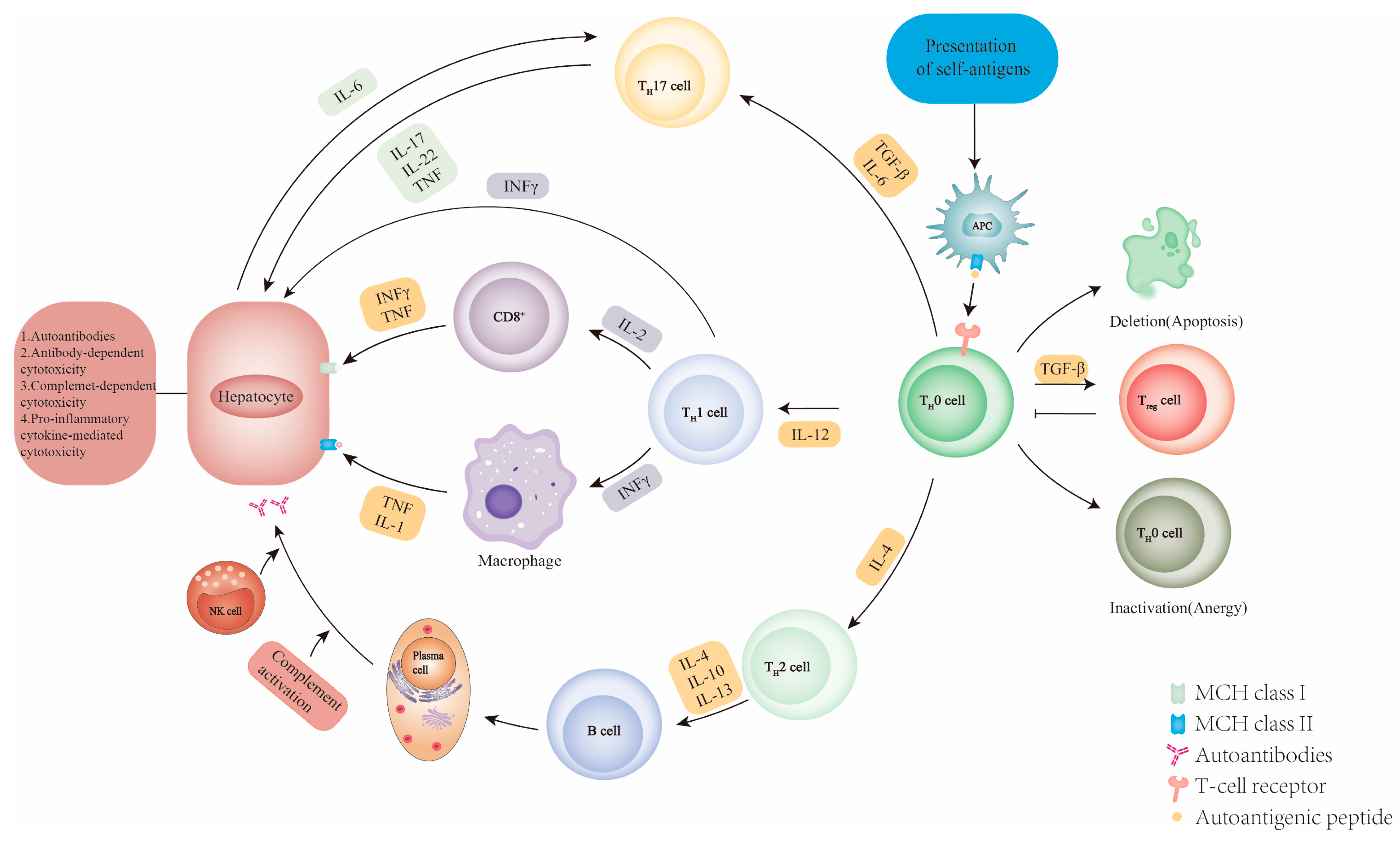
6. The Potential Mechanism of the Pathogenesis of AIH
7. Limitations
8. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pascarella, G.; Strumia, A.; Piliego, C.; Bruno, F.; Del Buono, R.; Costa, F.; Scarlata, S.; Agrò, F.E. COVID-19 diagnosis and management: A comprehensive review. J. Intern. Med. 2020, 288, 192–206. [Google Scholar] [CrossRef] [PubMed]
- Slaoui, M.; Hepburn, M. Developing Safe and Effective Covid Vaccines-Operation Warp Speed‘s Strategy and Approach. N. Engl. J. Med. 2020, 383, 1701–1703. [Google Scholar] [CrossRef] [PubMed]
- Ho, R.J.Y. Warp-Speed Covid-19 Vaccine Development: Beneficiaries of Maturation in Biopharmaceutical Technologies and Public-Private Partnerships. J. Pharm. Sci. 2021, 110, 615–618. [Google Scholar] [CrossRef] [PubMed]
- Fiolet, T.; Kherabi, Y.; MacDonald, C.J.; Ghosn; Peiffer-Smadja, N. Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against SARS-CoV-2 and variants of concern: A narrative review. Clin. Microbiol. Infect. 2022, 28, 202–221. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus Pandemic (COVID-19). Available online: https://ourworldindata.org/coronavirus#citation (accessed on 16 May 2023).
- Barda, N.; Dagan, N.; Ben-Shlomo, Y.; Kepten, E.; Waxman, J.; Ohana, R.; Hernán, M.A.; Lipsitch, M.; Kohane, I.; Netzer, D.; et al. Safety of the BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Setting. N. Engl. J. Med. 2021, 385, 1078–1090. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Bozkurt, B.; Kamat, I.; Hotez, P.J. Myocarditis With COVID-19 mRNA Vaccines. Circulation 2021, 144, 471–484. [Google Scholar] [CrossRef]
- Long, B.; Bridwell, R.; Gottlieb, M. Thrombosis with thrombocytopenia syndrome associated with COVID-19 vaccines. Am. J. Emerg. Med. 2021, 49, 58–61. [Google Scholar] [CrossRef]
- Garrido, I.; Lopes, S.; Simoes, M.S.; Liberal, R.; Lopes, J.; Carneiro, F.; Macedo, G. Autoimmune hepatitis after COVID-19 vaccine–more than a coincidence. J. Autoimmun. 2021, 125, 102741. [Google Scholar] [CrossRef]
- Avci, E.; Abasiyanik, F. Autoimmune hepatitis after SARS-CoV-2 vaccine: New-onset or flare-up? J. Autoimmun. 2021, 125, 102745. [Google Scholar] [CrossRef]
- Bril, F.; Al Diffalha, S.; Dean, M.; Fettig, D.M. Autoimmune hepatitis developing after coronavirus disease 2019 (COVID-19) vaccine: Causality or casualty? J. Hepatol. 2021, 75, 222–224. [Google Scholar] [CrossRef]
- Ghielmetti, M.; Schaufelberger, H.D.; Mieli-Vergani, G.; Cerny, A.; Dayer, E.; Vergani, D.; Terziroli Beretta-Piccoli, B. Acute autoimmune-like hepatitis with atypical anti-mitochondrial antibody after mRNA COVID-19 vaccination: A novel clinical entity? J. Autoimmun. 2021, 123, 102706. [Google Scholar] [CrossRef]
- Rocco, A.; Sgamato, C.; Compare, D.; Nardone, G. Autoimmune hepatitis following SARS-CoV-2 vaccine: May not be a casuality. J. Hepatol. 2021, 75, 728–729. [Google Scholar] [CrossRef]
- Tan, C.K.; Wong, Y.J.; Wang, L.M.; Ang, T.L.; Kumar, R. Autoimmune hepatitis following COVID-19 vaccination: True causality or mere association? J. Hepatol. 2021, 75, 1250–1252. [Google Scholar] [CrossRef]
- Clayton-Chubb, D.; Schneider, D.; Freeman, E.; Kemp, W.; Roberts, S.K. Autoimmune hepatitis developing after the ChA-dOx1 nCoV-19 (Oxford-AstraZeneca) vaccine. J. Hepatol. 2021, 75, 1249–1250. [Google Scholar] [CrossRef]
- Depret, F.; Bouam, S.; Schwarzinger, M.; Mallet, V. Demosthenes research g. Reply to: “Focus on the decisions to forego life-sustaining therapies during ICU stay of patients with cirrhosis and COVID-19: A case control study from the prospective COVID-ICU database”. J. Hepatol. 2022, 76, 744–747. [Google Scholar] [CrossRef]
- Lodato, F.; Larocca, A.; D‘Errico, A.; Cennamo, V. An unusual case of acute cholestatic hepatitis after m-RNABNT162b2 (Comirnaty) SARS-CoV-2 vaccine: Coincidence, autoimmunity or drug-related liver injury. J. Hepatol. 2021, 75, 1254–1256. [Google Scholar] [CrossRef]
- Ghelfi, J.; Brusset, B.; Thony, F.; Decaens, T. Successful management of refractory ascites in non-TIPSable patients using percutaneous thoracic duct stenting. J. Hepatol. 2022, 76, 216–218. [Google Scholar] [CrossRef]
- Mahalingham, A.; Duckworth, A.; Griffiths, W.J.H. First report of posttransplant autoimmune hepatitis recurrence following SARS-CoV-2 mRNA vaccination. Transpl. Immunol. 2022, 72, 101600. [Google Scholar] [CrossRef]
- Fimiano, F.; D‘Amato, D.; Gambella, A.; Marzano, A.; Saracco, G.M.; Morgando, A. Autoimmune hepatitis or drug-induced autoimmune hepatitis following Covid-19 vaccination? Liver Int. 2022, 42, 1204–1205. [Google Scholar] [CrossRef]
- Erard, D.; Villeret, F.; Lavrut, P.M.; Dumortier, J. Autoimmune hepatitis developing after COVID 19 vaccine: Presumed guilty? Clin. Res. Hepatol. Gastroenterol. 2022, 46, 101841. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.H.; Kim, M.Y.; Cho, M.Y.; Baik, S.K. Autoimmune Hepatitis Following Vaccination for SARS-CoV-2 in Korea: Coincidence or Autoimmunity? J. Korean Med. Sci. 2022, 37, e116. [Google Scholar] [CrossRef] [PubMed]
- Shahrani, S.; Sooi, C.Y.; Hilmi, I.N.; Mahadeva, S. Autoimmune hepatitis (AIH) following coronavirus (COVID-19) vaccine-No longer exclusive to mRNA vaccine? Liver Int. 2022, 42, 2344–2345. [Google Scholar] [CrossRef] [PubMed]
- Lasagna, A.; Lenti, M.V.; Cassaniti, I.; Sacchi, P. Development of hepatitis triggered by SARS-CoV-2 vaccination in patient with cancer during immunotherapy: A case report. Immunotherapy 2022, 14, 915–925. [Google Scholar] [CrossRef]
- Goulas, A.; Kafiri, G.; Kranidioti, H.; Manolakopoulos, S. A typical autoimmune hepatitis (AIH) case following COVID-19 mRNA vaccination. More than a coincidence? Liver Int. 2022, 42, 254–255. [Google Scholar] [CrossRef]
- Pinazo-Bandera, J.M.; Hernandez-Albujar, A.; Garcia-Salguero, A.I.; Arranz-Salas, I.; Andrade, R.J.; Robles-Diaz, M. Acute hepatitis with autoimmune features after COVID-19 vaccine: Coincidence or vaccine-induced phenomenon? Gastroenterol. Rep. 2022, 10, goac014. [Google Scholar] [CrossRef]
- Bjornsson, H.K.; Bjornsson, E.S. Reply to: “Can azathioprine prevent infliximab-induced liver injury?”. J. Hepatol. 2022, 77, 555–556. [Google Scholar] [CrossRef]
- Londono, M.C.; Gratacos-Gines, J.; Saez-Penataro, J. Another case of autoimmune hepatitis after SARS-CoV-2 vaccination–Still casualty? J. Hepatol. 2021, 75, 1248–1249. [Google Scholar] [CrossRef]
- McShane, C.; Kiat, C.; Rigby, J.; Crosbie, O. The mRNA COVID-19 vaccine—A rare trigger of autoimmune hepatitis? J. Hepatol. 2021, 75, 1252–1254. [Google Scholar] [CrossRef]
- Rela, M.; Jothimani, D.; Vij, M.; Rajakumar, A.; Rammohan, A. Autoimmune hepatitis following COVID vaccination. J. Autoimmun. 2021, 123, 102688. [Google Scholar] [CrossRef]
- Palla, P.; Vergadis, C.; Sakellariou, S.; Androutsakos, T. Letter to the editor: Autoimmune hepatitis after COVID-19 vaccination: A rare adverse effect? Hepatology 2022, 75, 489–490. [Google Scholar] [CrossRef]
- Shroff, H.; Satapathy, S.K.; Crawford, J.M.; Todd, N.J.; VanWagner, L.B. Liver injury following SARS-CoV-2 vaccination: A multicenter case series. J. Hepatol. 2022, 76, 211–214. [Google Scholar] [CrossRef]
- Vuille-Lessard, E.; Montani, M.; Bosch, J.; Semmo, N. Autoimmune hepatitis triggered by SARS-CoV-2 vaccination. J. Autoimmun. 2021, 123, 102710. [Google Scholar] [CrossRef]
- Waldenstrom, J. Liver, blood proteins and food proteins. Dtsch. Z Verdau Stoffwechselkr. 1952, 12, 113–121. [Google Scholar]
- Mieli-Vergani, G.; Vergani, D.; Czaja, A.J.; Manns, M.P.; Krawitt, E.L.; Vierling, J.M.; Lohse, A.W.; Montano-Loza, A.J. Autoimmune hepatitis. Nat. Rev. Dis. Prim. 2018, 4, 18017. [Google Scholar] [CrossRef]
- Manns, M.P.; Lohse, A.W.; Vergani, D. Autoimmune hepatitis—Update 2015. J. Hepatol. 2015, 62, S100–S111. [Google Scholar] [CrossRef]
- Czaja, A.J. Global Disparities and Their Implications in the Occurrence and Outcome of Autoimmune Hepatitis. Dig. Dis. Sci. 2017, 62, 2277–2292. [Google Scholar] [CrossRef]
- Manns, M.P.; Czaja, A.J.; Gorham, J.D.; Krawitt, E.L.; Mieli-Vergani, G.; Vergani, D.; Vierling, J.M. Diagnosis and management of autoimmune hepatitis. Hepatology 2010, 51, 2193–2213. [Google Scholar] [CrossRef]
- European Association for the study of the Liver. EASL Clinical Practice Guidelines: Autoimmune hepatitis. J. Hepatol. 2015, 63, 971–1004. [Google Scholar] [CrossRef]
- van Gerven, N.M.; Verwer, B.J.; Witte, B.I.; van Erpecum, K.J.; van Buuren, H.R.; Maijers, I.; Visscher, A.P.; Verschuren, E.C.; van Hoek, B.; Coenraad, M.J.; et al. Epidemiology and clinical characteristics of autoimmune hepatitis in the Netherlands. Scand. J. Gastroenterol. 2014, 49, 1245–1254. [Google Scholar] [CrossRef]
- Takahashi, H.; Zeniya, M. Acute presentation of autoimmune hepatitis: Does it exist? A published work review. Hepatol. Res. 2011, 41, 498–504. [Google Scholar] [CrossRef] [PubMed]
- Mack, C.L.; Adams, D.; Assis, D.N.; Kerkar, N.; Manns, M.P.; Mayo, M.J.; Vierling, J.M.; Alsawas, M.; Murad, M.H.; Czaja, A.J. Diagnosis and Management of Autoimmune Hepatitis in Adults and Children: 2019 Practice Guidance and Guidelines from the American Association for the Study of Liver Diseases. Hepatology 2020, 72, 671–722. [Google Scholar] [CrossRef] [PubMed]
- Czaja, A.J.; Carpenter, H.A. Optimizing diagnosis from the medical liver biopsy. Clin. Gastroenterol. Hepatol. 2007, 5, 898–907. [Google Scholar] [CrossRef] [PubMed]
- Dienes, H.P.; Erberich, H.; Dries, V.; Schirmacher, P.; Lohse, A. Autoimmune hepatitis and overlap syndromes. Clin. Liver Dis. 2002, 6, 349–362. [Google Scholar] [CrossRef] [PubMed]
- Hennes, E.M.; Zeniya, M.; Czaja, A.J.; Parés, A.; Dalekos, G.N.; Krawitt, E.L.; Bittencourt, P.L.; Porta, G.; Boberg, K.M.; Hofer, H.; et al. Simplified criteria for the diagnosis of autoimmune hepatitis. Hepatology 2008, 48, 169–176. [Google Scholar] [CrossRef]
- Alvarez, F.; Berg, P.A.; Bianchi, F.B.; Bianchi, L.; Burroughs, A.K.; Cancado, E.L.; Chapman, R.W.; Cooksley, W.G.; Czaja, A.J.; Desmet, V.J.; et al. International Autoimmune Hepatitis Group Report: Review of criteria for diagnosis of autoimmune hepatitis. J. Hepatol. 1999, 31, 929–938. [Google Scholar] [CrossRef]
- Komori, A. Recent updates on the management of autoimmune hepatitis. Clin. Mol. Hepatol. 2021, 27, 58–69. [Google Scholar] [CrossRef]
- Harrington, C.; Krishnan, S.; Mack, C.L.; Cravedi, P.; Assis, D.N.; Levitsky, J. Noninvasive biomarkers for the diagnosis and management of autoimmune hepatitis. Hepatology 2022, 76, 1862–1879. [Google Scholar] [CrossRef]
- Beretta-Piccoli, T.; Mieli-Vergani, B.G.; Vergani, D. Autoimmune hepatitis: Standard treatment and systematic review of alternative treatments. World J. Gastroenterol. 2017, 23, 6030–6048. [Google Scholar] [CrossRef]
- Feld, J.J.; Dinh, H.; Arenovich, T.; Marcus, V.A.; Wanless, I.R.; Heathcote, E.J. Autoimmune hepatitis: Effect of symptoms and cirrhosis on natural history and outcome. Hepatology 2005, 42, 53–62. [Google Scholar] [CrossRef]
- Dufour, J.F.; Zimmermann, M.; Reichen, J. Severe autoimmune hepatitis in patients with previous spontaneous recovery of a flare. J. Hepatol. 2002, 37, 748–752. [Google Scholar] [CrossRef]
- Kogan, J.; Safadi, R.; Ashur, Y.; Shouval, D.; Ilan, Y. Prognosis of symptomatic versus asymptomatic autoimmune hepatitis: A study of 68 patients. J. Clin. Gastroenterol. 2002, 35, 75–81. [Google Scholar] [CrossRef]
- Segal Y, Shoenfeld Y: Vaccine-induced autoimmunity: The role of molecular mimicry and immune crossreaction. Cell. Mol. Immunol. 2018, 15, 586–594. [CrossRef]
- Segal, Y.; Dahan, S.; Calabrò, M.; Kanduc, D.; Shoenfeld, Y. HPV and systemic lupus erythematosus: A mosaic of potential crossreactions. Immunol. Res. 2017, 65, 564–571. [Google Scholar] [CrossRef]
- Segal, Y.; Calabrò, M.; Kanduc, D.; Shoenfeld, Y. Human papilloma virus and lupus: The virus, the vaccine and the disease. Curr. Opin. Rheumatol. 2017, 29, 331–342. [Google Scholar] [CrossRef]
- Cohen Tervaert, J.W.; Martinez-Lavin, M.; Jara, L.J.; Halpert, G.; Watad, A.; Amital, H.; Shoenfeld, Y. Autoimmune/inflammatory syndrome induced by adjuvants (ASIA) in 2023. Autoimmun. Rev. 2023, 22, 103287. [Google Scholar] [CrossRef]
- Seida, I.; Seida, R.; Elsalti, A.; Mahroum, N. Vaccines and Autoimmunity-From Side Effects to ASIA Syndrome. Medicina 2023, 59, 364. [Google Scholar] [CrossRef]
- Vojdani, A.; Kharrazian, D. Potential antigenic cross-reactivity between SARS-CoV-2 and human tissue with a possible link to an increase in autoimmune diseases. Clin. Immunol. 2020, 217, 108480. [Google Scholar] [CrossRef]
- Hintermann, E.; Holdener, M.; Bayer, M.; Loges, S.; Pfeilschifter, J.M.; Granier, C.; Manns, M.P.; Christen, U. Epitope spreading of the anti-CYP2D6 antibody response in patients with autoimmune hepatitis and in the CYP2D6 mouse model. J. Autoimmun. 2011, 37, 242–253. [Google Scholar] [CrossRef]
- Milojevic, D.; Nguyen, K.D.; Wara, D.; Mellins, E.D. Regulatory T cells and their role in rheumatic diseases: A potential target for novel therapeutic development. Pediatr. Rheumatol. Online J. 2008, 6, 20. [Google Scholar] [CrossRef]
- Muratori, L.; Muratori, P.; Lanzoni, G.; Ferri, S.; Lenzi, M. Application of the 2010 American Association for the study of liver diseases criteria of remission to a cohort of Italian patients with autoimmune hepatitis. Hepatology 2010, 52, 1857. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, A.; Ma, X.; Yokosuka, O.; Weltman, M.; You, H.; Amarapurkar, D.N.; Kim, Y.J.; Abbas, Z.; Payawal, D.A.; Chang, M.L.; et al. Autoimmune liver diseases in the Asia-Pacific region: Proceedings of APASL symposium on AIH and PBC 2016. Hepatol. Int. 2016, 10, 909–915. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.H.; Kim, Y.J.; Jeong, S.H.; Tak, W.Y.; Ahn, S.H.; Lee, Y.J.; Jung, E.U.; Lee, J.I.; Yeon, J.E.; Hwang, J.S.; et al. Clinical features of autoimmune hepatitis and comparison of two diagnostic criteria in Korea: A nationwide, multicenter study. J. Gastroenterol. Hepatol. 2013, 28, 128–134. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Vaccines a | No. of Patients (%) | Autoantibodies d | No. of Patients (%) |
|---|---|---|---|
| Pfizer–BioNTech | 18 (46.2%) | ANA | 25 (78.1%) |
| Moderna | 15 (38.4%) | ASMA | 12 (37.5%) |
| Oxford–AstraZeneca | 6 (15.4%) | ds-DNA | 2 (6.3%) |
| Time of onset of symptoms b | No. of Patients (%) | Anti-SLA | 1 (3.1%) |
| First vaccination | 31 (81.6%) | Anti-LC1 | 1 (3.1%) |
| Second vaccination | 7 (18.4%) | ANCA | 1 (3.1%) |
| Symptoms c | No. of Patients (%) | None | 4 (12.5%) |
| Jaundice | 21 (75.0%) | Serum biochemical parameters e | Median (Range) |
| Fatigue | 7 (25.0%) | ALT(U/L) | 1038 (171–2664) |
| Anorexia | 5 (17.9%) | AST (U/L) | 862 (111–2314) |
| Choluria | 5 (17.9%) | ALP (U/L) | 186 (24–2252) |
| Anorexia | 5 (17.9%) | Tbil (U/L) | 3.84 (0.33–45) |
| Pruritus | 5 (17.9%) | GGT (U/L) | 345 (98–810) |
| Abdominal pain | 5 (17.9%) | Total IgG (mg/dL) | 1998 (1081–4260) |
| Fever | 5 (17.9%) | Liver biopsy a | No. of Patients (%) |
| Diarrhea | 1 (3.6%) | Interface hepatitis | 23 (59.0%) |
| Asymptomatic | 1 (3.6%) | pycnotic necrosis | 14 (35.9%) |
| Lymphocyte/plasma cells infiltration | 35 (89.7%) | ||
| Eosinophils | 11 (30.8%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, H.; Ye, Q. Clinical Features of COVID-19 Vaccine-Associated Autoimmune Hepatitis: A Systematic Review. Diseases 2023, 11, 80. https://doi.org/10.3390/diseases11020080
Zhou H, Ye Q. Clinical Features of COVID-19 Vaccine-Associated Autoimmune Hepatitis: A Systematic Review. Diseases. 2023; 11(2):80. https://doi.org/10.3390/diseases11020080
Chicago/Turabian StyleZhou, Hao, and Qing Ye. 2023. "Clinical Features of COVID-19 Vaccine-Associated Autoimmune Hepatitis: A Systematic Review" Diseases 11, no. 2: 80. https://doi.org/10.3390/diseases11020080
APA StyleZhou, H., & Ye, Q. (2023). Clinical Features of COVID-19 Vaccine-Associated Autoimmune Hepatitis: A Systematic Review. Diseases, 11(2), 80. https://doi.org/10.3390/diseases11020080