
Dynamics of Cytokine, SARS-CoV-2-Specific IgG, and Neutralizing Antibody Levels in COVID-19 Patients Treated with Convalescent Plasma

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. COVID-19 Patients
2.2. Sample Collection
2.3. COVID-19 Convalescent Plasma Donors
2.4. RT-PCR Detection
2.5. Antibody Assays
2.5.1. Detection of Anti-SARS-CoV-2 Spike Protein Antibody
2.5.2. Detection of Anti-SARS-CoV-2 Nucleocapsid Protein Antibody
2.5.3. SARS-CoV-2 Neutralizing Antibodies
2.6. Cytokine Measurements
2.7. Measurement of Serum Biochemical Markers
2.8. Data Analysis
3. Results
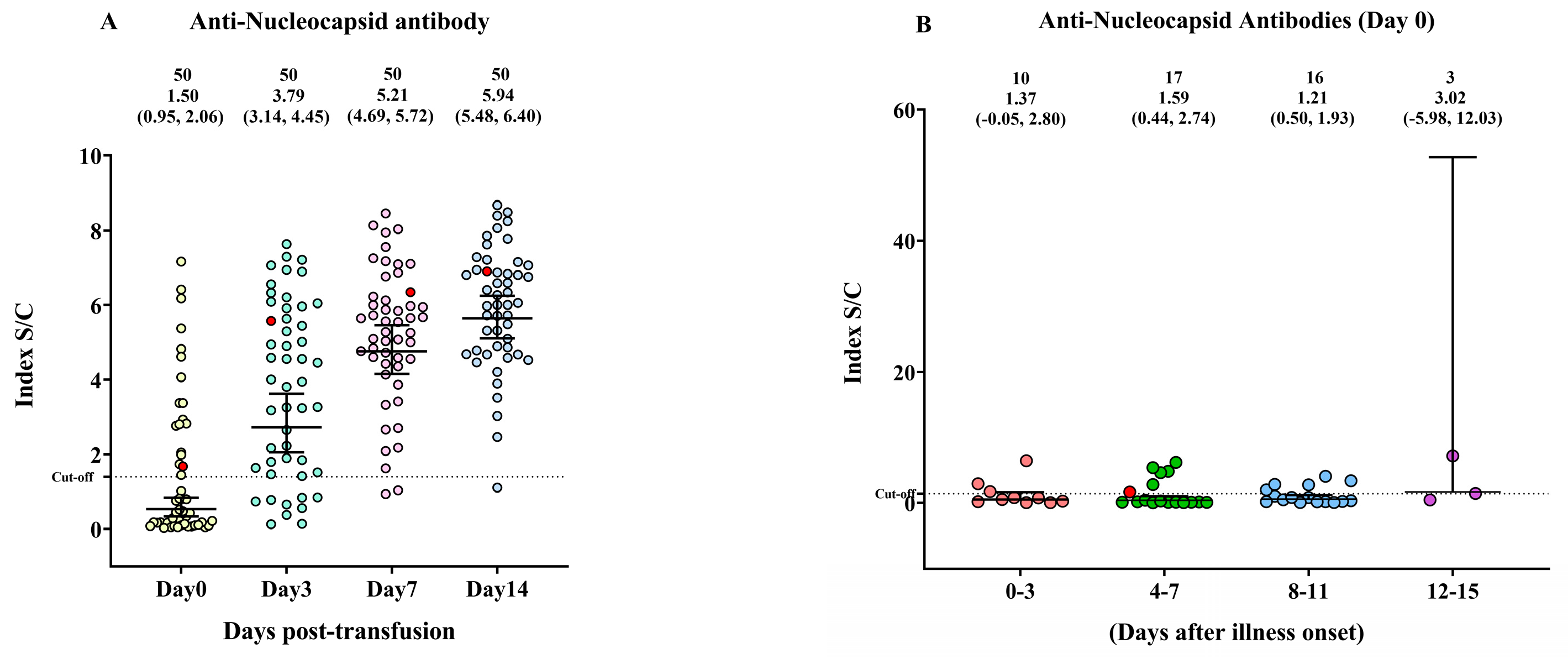
3.1. The Anti-Nucleocapsid Protein IgG Antibody Response in Patients with COVID-19
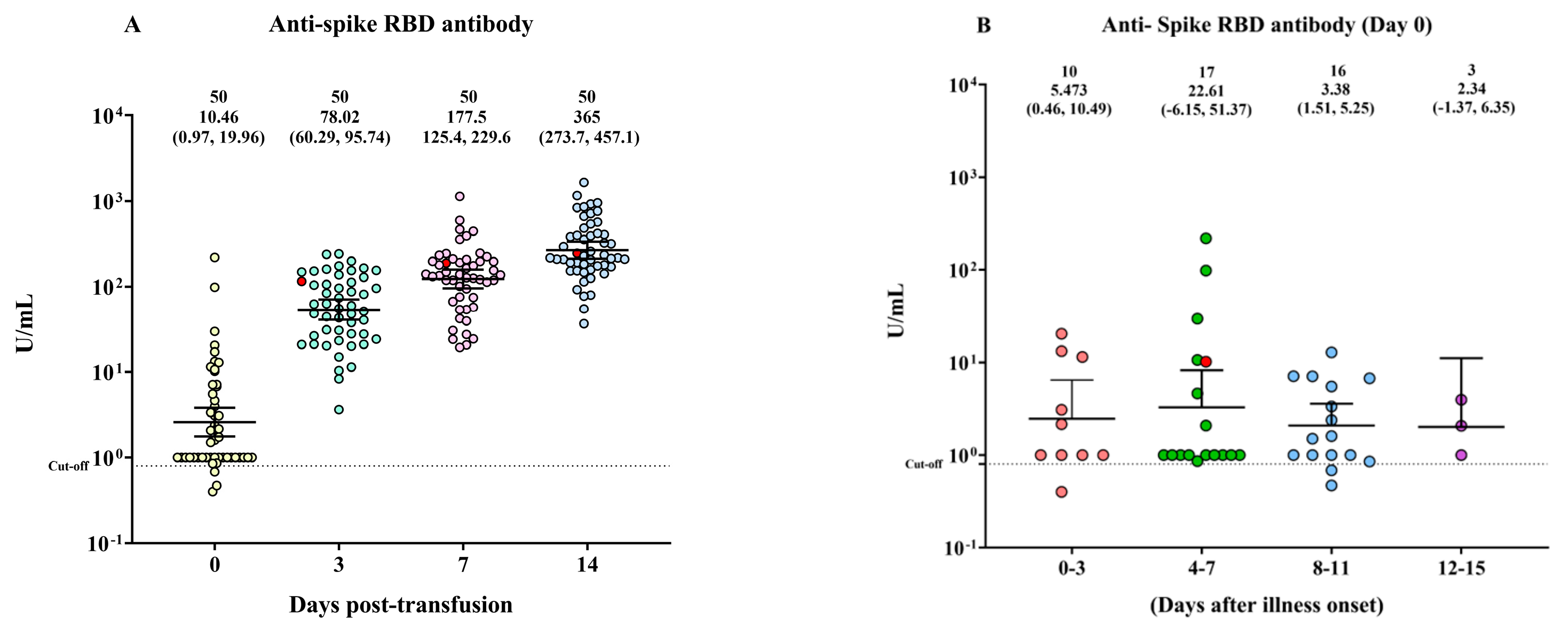
3.2. The Anti-Spike RBD Protein IgG Antibody Response in Patients with COVID-19
3.3. The Neutralizing Antibody Titer in Patients with COVID-19
3.4. The Levels of Laboratory Markers and Circulating Cytokines
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ghayda, R.A.; Lee, J.; Lee, J.Y.; Kim, D.K.; Lee, K.H.; Hong, S.H.; Han, Y.J.; Kim, J.S.; Yang, J.W.; Kronbichler, A.; et al. Correlations of Clinical and Laboratory Characteristics of COVID-19: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 5026. [Google Scholar] [CrossRef]
- Grant, M.C.; Geoghegan, L.; Arbyn, M.; Mohammed, Z.; McGuinness, L.; Clarke, E.L.; Wade, R.G. The prevalence of symptoms in 24,410 adults infected by the novel coronavirus (SARS-CoV-2; COVID-19): A systematic review and meta-analysis of 148 studies from 9 countries. PLoS ONE 2020, 15, e0234765. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.D.; Ding, M.; Dong, X.; Zhang, J.J.; Kursat Azkur, A.; Azkur, D.; Gan, H.; Sun, Y.L.; Fu, W.; Li, W.; et al. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy 2021, 76, 428–455. [Google Scholar] [CrossRef] [PubMed]
- Wendel Garcia, P.D.; Fumeaux, T.; Guerci, P.; Heuberger, D.M.; Montomoli, J.; Roche-Campo, F.; Schuepbach, R.A.; Hilty, M.P. Prognostic factors associated with mortality risk and disease progression in 639 critically ill patients with COVID-19 in Europe: Initial report of the international RISC-19-ICU prospective observational cohort. EClinicalMedicine 2020, 25, 100449. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Wolff, D.; Nee, S.; Hickey, N.S.; Marschollek, M. Risk factors for COVID-19 severity and fatality: A structured literature review. Infection 2021, 49, 15–28. [Google Scholar] [CrossRef]
- Zhang, J.J.; Cao, Y.Y.; Tan, G.; Dong, X.; Wang, B.C.; Lin, J.; Yan, Y.Q.; Liu, G.H.; Akdis, M.; Akdis, C.A.; et al. Clinical, radiological, and laboratory characteristics and risk factors for severity and mortality of 289 hospitalized COVID-19 patients. Allergy 2021, 76, 533–550. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, R.L.; Vaca, C.E.; Paredes, R.; Mera, J.; Webb, B.J.; Perez, G.; Oguchi, G.; Ryan, P.; Nielsen, B.U.; Brown, M.; et al. Early Remdesivir to Prevent Progression to Severe COVID-19 in Outpatients. N. Engl. J. Med. 2022, 386, 305–315. [Google Scholar] [CrossRef]
- Wu, C.R.; Yin, W.C.; Jiang, Y.; Xu, H.E. Structure genomics of SARS-CoV-2 and its Omicron variant: Drug design templates for COVID-19. Acta Pharmacol. Sin. 2022, 43, 3021–3033. [Google Scholar] [CrossRef]
- Cheng, Y.; Wong, R.; Soo, Y.O.; Wong, W.S.; Lee, C.K.; Ng, M.H.; Chan, P.; Wong, K.C.; Leung, C.B.; Cheng, G. Use of convalescent plasma therapy in SARS patients in Hong Kong. Eur. J. Clin. Microbiol. Infect. Dis. 2005, 24, 44–46. [Google Scholar] [CrossRef]
- Hung, I.F.; To, K.K.; Lee, C.K.; Lee, K.L.; Chan, K.; Yan, W.W.; Liu, R.; Watt, C.L.; Chan, W.M.; Lai, K.Y.; et al. Convalescent plasma treatment reduced mortality in patients with severe pandemic influenza A (H1N1) 2009 virus infection. Clin. Infect. Dis. 2011, 52, 447–456. [Google Scholar] [CrossRef]
- Mair-Jenkins, J.; Saavedra-Campos, M.; Baillie, J.K.; Cleary, P.; Khaw, F.M.; Lim, W.S.; Makki, S.; Rooney, K.D.; Nguyen-Van-Tam, J.S.; Beck, C.R. The effectiveness of convalescent plasma and hyperimmune immunoglobulin for the treatment of severe acute respiratory infections of viral etiology: A systematic review and exploratory meta-analysis. J. Infect. Dis. 2015, 211, 80–90. [Google Scholar] [CrossRef] [PubMed]
- Soo, Y.O.; Cheng, Y.; Wong, R.; Hui, D.S.; Lee, C.K.; Tsang, K.K.; Ng, M.H.; Chan, P.; Cheng, G.; Sung, J.J. Retrospective comparison of convalescent plasma with continuing high-dose methylprednisolone treatment in SARS patients. Clin. Microbiol. Infect. 2004, 10, 676–678. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, A.P.H.; Wendel, S.; Bonet-Bub, C.; Fachini, R.M.; Dametto, A.P.F.; Blumm, F.; Dutra, V.F.; Candelaria, G.T.P.; Sakashita, A.M.; Machado, R.R.G.; et al. COVID-19 convalescent plasma cohort study: Evaluation of the association between both donor and recipient neutralizing antibody titers and patient outcomes. Transfusion 2021, 61, 2295–2306. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Liu, S.; Tan, T.; Huang, W.; Dong, Y.; Chen, L.; Chen, Q.; Zhang, L.; Zhong, Q.; Zhang, X.; et al. Treatment With Convalescent Plasma for Critically Ill Patients With Severe Acute Respiratory Syndrome Coronavirus 2 Infection. Chest 2020, 158, e9–e13. [Google Scholar] [CrossRef]
- Duan, K.; Liu, B.; Li, C.; Zhang, H.; Yu, T.; Qu, J.; Zhou, M.; Chen, L.; Meng, S.; Hu, Y.; et al. Effectiveness of convalescent plasma therapy in severe COVID-19 patients. Proc. Natl. Acad. Sci. USA 2020, 117, 9490–9496. [Google Scholar] [CrossRef]
- Ye, M.; Fu, D.; Ren, Y.; Wang, F.; Wang, D.; Zhang, F.; Xia, X.; Lv, T. Treatment with convalescent plasma for COVID-19 patients in Wuhan, China. J. Med. Virol. 2020, 92, 1890–1901. [Google Scholar] [CrossRef]
- Shen, C.; Wang, Z.; Zhao, F.; Yang, Y.; Li, J.; Yuan, J.; Wang, F.; Li, D.; Yang, M.; Xing, L.; et al. Treatment of 5 Critically Ill Patients with COVID-19 with Convalescent Plasma. JAMA 2020, 323, 1582–1589. [Google Scholar] [CrossRef]
- Vacharathit, V.; Srichatrapimuk, S.; Manopwisedjaroen, S.; Kirdlarp, S.; Srisaowakarn, C.; Setthaudom, C.; Inrueangsri, N.; Pisitkun, P.; Kunakorn, M.; Hongeng, S.; et al. SARS-CoV-2 neutralizing antibodies decline over one year and patients with severe COVID-19 pneumonia display a unique cytokine profile. Int. J. Infect. Dis. 2021, 112, 227–234. [Google Scholar] [CrossRef]
- Fazeli, A.; Sharifi, S.; Behdad, F.; Okati, S.; Esmaielifar, G.; Jelveh, N.; Eshghi, P.; Mohammadi, S. Early high-titer convalescent plasma therapy in patients with moderate and severe COVID-19. Transfus. Apher. Sci. 2022, 61, 103321. [Google Scholar] [CrossRef] [PubMed]
- Smilowitz, N.R.; Kunichoff, D.; Garshick, M.; Shah, B.; Pillinger, M.; Hochman, J.S.; Berger, J.S. C-reactive protein and clinical outcomes in patients with COVID-19. Eur. Heart J. 2021, 42, 2270–2279. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Abbaspour, N.; Hurrell, R.; Kelishadi, R. Review on iron and its importance for human health. J. Res. Med. Sci. 2014, 19, 164–174. [Google Scholar] [PubMed]
- Dahan, S.; Segal, G.; Katz, I.; Hellou, T.; Tietel, M.; Bryk, G.; Amital, H.; Shoenfeld, Y.; Dagan, A. Ferritin as a Marker of Severity in COVID-19 Patients: A Fatal Correlation. Isr. Med. Assoc. J. 2020, 22, 494–500. [Google Scholar]
- Lucas, C.; Klein, J.; Sundaram, M.E.; Liu, F.; Wong, P.; Silva, J.; Mao, T.; Oh, J.E.; Mohanty, S.; Huang, J.; et al. Delayed production of neutralizing antibodies correlates with fatal COVID-19. Nat. Med. 2021, 27, 1178–1186. [Google Scholar] [CrossRef]
- Martin-Vicente, M.; Almansa, R.; Martínez, I.; Tedim, A.P.; Bustamante, E.; Tamayo, L.; Aldecoa, C.; Gómez, J.M.; Renedo, G.; Berezo, J.; et al. Low anti-SARS-CoV-2 S antibody levels predict increased mortality and dissemination of viral components in the blood of critical COVID-19 patients. J. Intern. Med. 2022, 291, 232–240. [Google Scholar] [CrossRef]
- Klein, M.N.; Wang, E.W.; Zimand, P.; Beauchamp, H.; Donis, C.; Ward, M.D.; Martinez-Hernandez, A.; Tabatabai, A.; Baddley, J.W.; Bloch, E.M.; et al. Kinetics of SARS-CoV-2 antibody responses pre-COVID-19 and post-COVID-19 convalescent plasma transfusion in patients with severe respiratory failure: An observational case-control study. J. Clin. Pathol. 2022, 75, 564–571. [Google Scholar] [CrossRef]
- Costela-Ruiz, V.J.; Illescas-Montes, R.; Puerta-Puerta, J.M.; Ruiz, C.; Melguizo-Rodríguez, L. SARS-CoV-2 infection: The role of cytokines in COVID-19 disease. Cytokine Growth Factor Rev. 2020, 54, 62–75. [Google Scholar] [CrossRef]
- Vabret, N.; Britton, G.J.; Gruber, C.; Hegde, S.; Kim, J.; Kuksin, M.; Levantovsky, R.; Malle, L.; Moreira, A.; Park, M.D.; et al. Immunology of COVID-19: Current State of the Science. Immunity 2020, 52, 910–941. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Liu, X.; Wu, S.; Chen, S.; Li, Y.; Nong, L.; Lie, P.; Huang, L.; Cheng, L.; Lin, Y.; et al. Definition and Risks of Cytokine Release Syndrome in 11 Critically Ill COVID-19 Patients with Pneumonia: Analysis of Disease Characteristics. J. Infect. Dis. 2020, 222, 1444–1451. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Sun, J.; Pan, H.; Yao, F.; Yuan, Y.; Zeng, M.; Ye, G.; Yang, G.; Zheng, B.; Fan, J.; et al. Aberrant cytokine expression in COVID-19 patients: Associations between cytokines and disease severity. Cytokine 2021, 143, 155523. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Narazaki, M.; Kishimoto, T. IL-6 in inflammation, immunity, and disease. Cold Spring Harb. Perspect. Biol. 2014, 6, a016295. [Google Scholar] [CrossRef]
- Heinrich, P.C.; Castell, J.V.; Andus, T. Interleukin-6 and the acute phase response. Biochem. J. 1990, 265, 621–636. [Google Scholar] [CrossRef]
- McKinstry, K.K.; Strutt, T.M.; Buck, A.; Curtis, J.D.; Dibble, J.P.; Huston, G.; Tighe, M.; Hamada, H.; Sell, S.; Dutton, R.W.; et al. IL-10 deficiency unleashes an influenza-specific Th17 response and enhances survival against high-dose challenge. J. Immunol. 2009, 182, 7353–7363. [Google Scholar] [CrossRef]
- Han, H.; Ma, Q.; Li, C.; Liu, R.; Zhao, L.; Wang, W.; Zhang, P.; Liu, X.; Gao, G.; Liu, F.; et al. Profiling serum cytokines in COVID-19 patients reveals IL-6 and IL-10 are disease severity predictors. Emerg. Microbes Infect. 2020, 9, 1123–1130. [Google Scholar] [CrossRef]
- Gorham, J.; Moreau, A.; Corazza, F.; Peluso, L.; Ponthieux, F.; Talamonti, M.; Izzi, A.; Nagant, C.; Ndieugnou Djangang, N.; Garufi, A.; et al. Interleukine-6 in critically ill COVID-19 patients: A retrospective analysis. PLoS ONE 2020, 15, e0244628. [Google Scholar] [CrossRef]
- da Silva, R.P.; Gonçalves, J.I.B.; Zanin, R.F.; Schuch, F.B.; de Souza, A.P.D. Circulating Type I Interferon Levels and COVID-19 Severity: A Systematic Review and Meta-Analysis. Front. Immunol. 2021, 12, 657363. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | COVID-19 Patients (N = 49) |
|---|---|
| Age, mean (range) years | 46 (35–57) |
| Sex, female/male, n | 18/31 |
| Comorbidities, n = 16 | |
| Diabetes mellitus | 6 |
| Hypertension | 6 |
| Dyslipidemia | 3 |
| Obesity | 6 |
| Gout | 1 |
| Chronic kidney disease | 1 |
| Fatty liver disease | 1 |
| No underlying disease, n | 16 |
| No data available, n | 18 |
| The median (IQR) days from the onset of symptoms to hospital admission | 8 (5–10) |
| Median (IQR) days of hospitalization | 17.5 (17–22.5) |
| Clinical outcomes (survival, %) | 97.96% |
| Biochemical Marker | Pre-Transfusion | Post-Transfusion | p-Value | ||
|---|---|---|---|---|---|
| Day 0 | Day 3 | Day 7 | Day 14 | ||
| C-reactive protein (mg/L), normal range (0–6) | |||||
| Median | 31.610 | 9.935 | 2.065 | 5.945 | |
| Range | (0.6–244.2) | (0.6–130.64) | (0.6–201.26) | (0.6–222.21) | <0.0001 * |
| D-dimer (µg/mL) | |||||
| Median | 0.1900 | 0.2850 | 0.4550 | 0.2550 | |
| Range | (0.15–3.28) | (0.15–9.68) | (0.15–9.72) | (0.15–9.15) | 0.0008 * |
| Ferritin (ng/mL), normal range (13–400), age and gender dependent | |||||
| Median | 729.3 | 734.3 | 769.5 | 745.5 | |
| Range | (43.2–3021) | (26.3–3227.7) | (16.5–3137.7) | (28.1–3244.6) | 0.8896 |
| Circulating cytokine | |||||
| Interferon beta (IFN-β) (pg/mL) | |||||
| Median | 0.32 | 0.30 | 0.28 | 0.26 | |
| (Range) | (0.22–2.17) | (0.20–1.15) | (0.18–2.37) | (0.18–1.56) | |
| Mean ± SD | 0.53 ± 0.40 | 0.44 ± 0.28 | 0.42 ± 0.36 | 0.40 ± 0.30 | 0.0168 * |
| Soluble interleukin 6 receptor alpha (sIL-6R) | |||||
| (pg/mL) | |||||
| Median | 4500 | 5076 | 4382 | 3849 | |
| (Range) | (954.61–19614.51) | (1255.99–44828.6) | (1680.57–29896.14) | (1127.57–38273.86) | |
| Mean ± SD | 5507 ± 3702 | 6847 ± 6936 | 6592 ± 5957 | 7246 ± 7874 | 0.1110 |
| Interleukin-1 beta (IL-1β) | |||||
| Median | 0.10 | 0.05 | 0.05 | 0.10 | |
| Range | (0.03–3.80) | (0.03–8.37) | (0.03–2.72) | (0.03–16.76) | |
| Mean ± SD | 0.34 ± 0.64 | 0.53 ± 1.57 | 0.31 ± 0.54 | 0.99 ± 2.88 | 0.3450 |
| Interleukin-6 (IL-6) | |||||
| Median | 3.80 | 1.26 | 0.82 | 1.26 | |
| Range | (0.05–95.66) | (0.05–98.82) | (0.07–248.72) | (0.09–222.37) | |
| Mean ± SD | 7.648 ± 14.39 | 5.138 ± 14.54 | 7.563 ± 35.55 | 11.37 ± 38.70 | <0.0001 * |
| Interleukin-10 (IL-10) | |||||
| Median | 1.38 | 0.36 | 0.19 | 0.36 | |
| Range | (0.03–116.37) | (0.03–69.68) | (0.03–38.09) | (0.03–21.24) | |
| Mean ± SD | 4.263 ± 16.43 | 2.387 ± 9.912 | 1.352 ± 5.419 | 1.043 ± 3.111 | <0.0001 * |
| Interferon-alpha 2 (IFNα2) | |||||
| Median | 0.44 | 0.40 | 0.39 | 0.39 | |
| Range | (0.29–5.43) | (0.29–0.54) | (0.25–0.61) | (0.29–0.54) | |
| Mean ± SD | 0.7580 ± 1.099 | 0.41 ± 0.06 | 0.41 ± 0.07 | 0.40 ± 0.05 | 0.0005 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pratedrat, P.; Intharasongkroh, D.; Chansaenroj, J.; Vichaiwattana, P.; Srimuan, D.; Thatsanatorn, T.; Klinfueng, S.; Nilyanimit, P.; Chirathaworn, C.; Kupatawintu, P.; et al. Dynamics of Cytokine, SARS-CoV-2-Specific IgG, and Neutralizing Antibody Levels in COVID-19 Patients Treated with Convalescent Plasma. Diseases 2023, 11, 112. https://doi.org/10.3390/diseases11030112
Pratedrat P, Intharasongkroh D, Chansaenroj J, Vichaiwattana P, Srimuan D, Thatsanatorn T, Klinfueng S, Nilyanimit P, Chirathaworn C, Kupatawintu P, et al. Dynamics of Cytokine, SARS-CoV-2-Specific IgG, and Neutralizing Antibody Levels in COVID-19 Patients Treated with Convalescent Plasma. Diseases. 2023; 11(3):112. https://doi.org/10.3390/diseases11030112
Chicago/Turabian StylePratedrat, Pornpitra, Duangnapa Intharasongkroh, Jira Chansaenroj, Preeyaporn Vichaiwattana, Donchida Srimuan, Thaksaporn Thatsanatorn, Sirapa Klinfueng, Pornjarim Nilyanimit, Chintana Chirathaworn, Pawinee Kupatawintu, and et al. 2023. "Dynamics of Cytokine, SARS-CoV-2-Specific IgG, and Neutralizing Antibody Levels in COVID-19 Patients Treated with Convalescent Plasma" Diseases 11, no. 3: 112. https://doi.org/10.3390/diseases11030112
APA StylePratedrat, P., Intharasongkroh, D., Chansaenroj, J., Vichaiwattana, P., Srimuan, D., Thatsanatorn, T., Klinfueng, S., Nilyanimit, P., Chirathaworn, C., Kupatawintu, P., Chaiwanichsiri, D., Wanlapakorn, N., & Poovorawan, Y. (2023). Dynamics of Cytokine, SARS-CoV-2-Specific IgG, and Neutralizing Antibody Levels in COVID-19 Patients Treated with Convalescent Plasma. Diseases, 11(3), 112. https://doi.org/10.3390/diseases11030112