
Safety and Efficacy of GLP-1 Receptor Agonists in Type 2 Diabetes Mellitus with Advanced and End-Stage Kidney Disease: A Systematic Review and Meta-Analysis

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
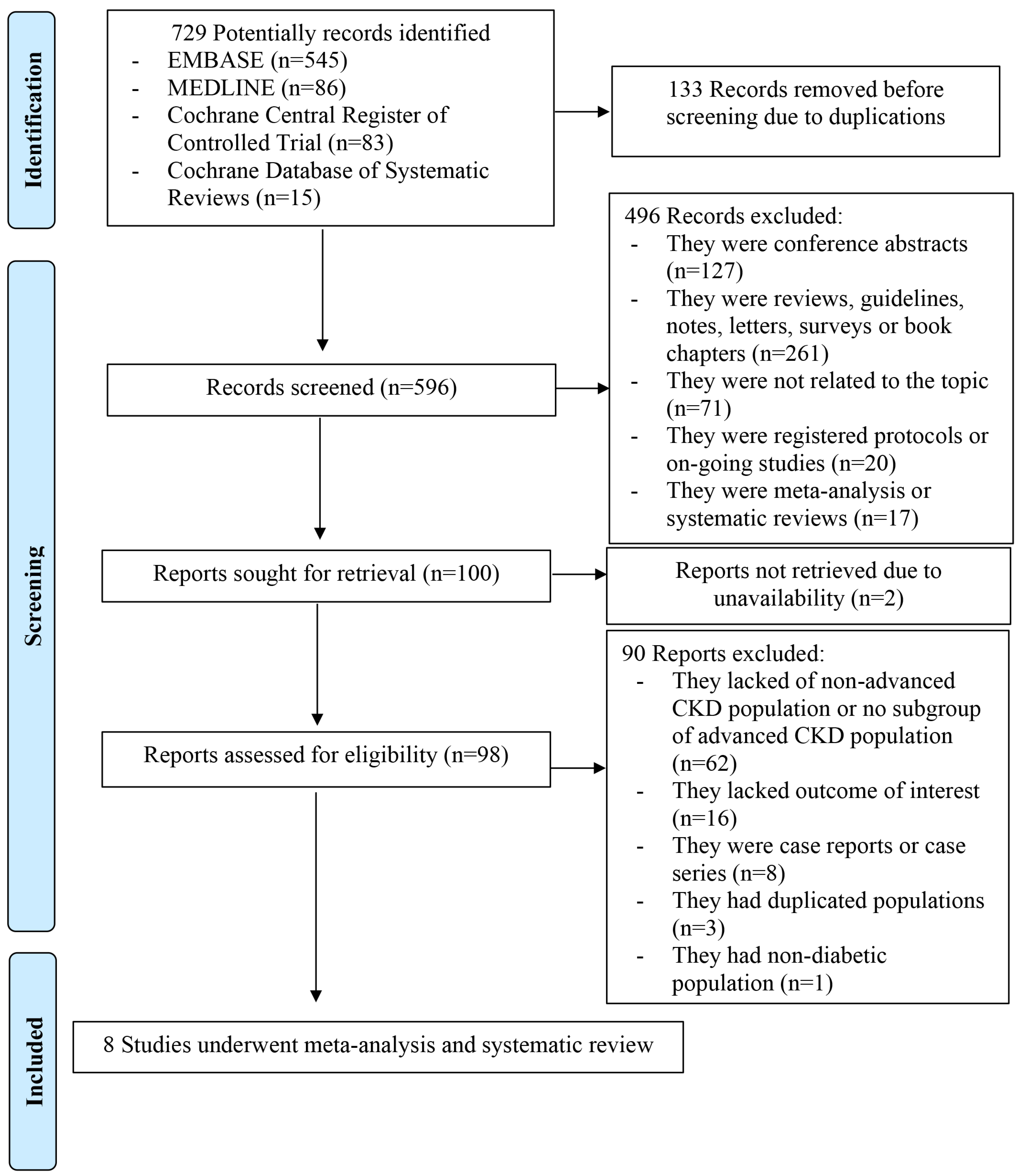
2.1. Search Strategy and StudyEligilbility
2.2. Data Extraction and Quality Assessment
2.3. Statisical Analysis
3. Results
3.1. Study Characteristics
3.2. Efficacy of GLP-1RAs on Mortality
3.3. Efficacy of GLP-1RAs on Cardiovascular Outcomes
3.4. Efficacy of GLP-1RAs on Blood Glucose
3.5. Efficacy of GLP-1RAs on Weight Reduction
3.6. Efficacy of GLP-1RAs on Renal Outcomes
3.7. Safety of GLP-1RAs
4. Evaluation of Publication Bias
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Bowe, B.; Mokdad, A.H.; Xian, H.; Yan, Y.; Li, T.; Maddukuri, G.; Tsai, C.Y.; Floyd, T.; Al-Aly, Z. Analysis of the Global Burden of Disease study highlights the global, regional, and national trends of chronic kidney disease epidemiology from 1990 to 2016. Kidney Int. 2018, 94, 567–581. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.T.; Xu, X.; Lim, P.S.; Hung, K.Y. Worldwide Epidemiology of Diabetes-Related End-Stage Renal Disease, 2000–2015. Diabetes Care 2021, 44, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M.; Benjamin, I.J.; Burke, G.L.; Chait, A.; Eckel, R.H.; Howard, B.V.; Mitch, W.; Smith, S.C., Jr.; Sowers, J.R. Diabetes and cardiovascular disease: A statement for healthcare professionals from the American Heart Association. Circulation 1999, 100, 1134–1146. [Google Scholar] [CrossRef]
- United States Renal Data System. 2022 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States; National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2022.
- Kidney Disease: Improving Global Outcomes Diabetes Work, G. KDIGO 2022 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease. Kidney Int. 2022, 102, S1–S127. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice Committee. 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022, 45, S125–S143. [Google Scholar] [CrossRef]
- Grespan, E.; Guolo, A.; Muscelli, E.; Ferrannini, E.; Mari, A. Loss of the Incretin Effect in Type 2 Diabetes: A Systematic Review and Meta-analysis. J. Clin. Endocrinol. Metab. 2022, 107, 2092–2100. [Google Scholar] [CrossRef]
- Drucker, D.J. Mechanisms of Action and Therapeutic Application of Glucagon-like Peptide-1. Cell Metab. 2018, 27, 740–756. [Google Scholar] [CrossRef]
- Gerstein, H.C.; Colhoun, H.M.; Dagenais, G.R.; Diaz, R.; Lakshmanan, M.; Pais, P.; Probstfield, J.; Riesmeyer, J.S.; Riddle, M.C.; Ryden, L.; et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): A double-blind, randomised placebo-controlled trial. Lancet 2019, 394, 121–130. [Google Scholar] [CrossRef]
- Hernandez, A.F.; Green, J.B.; Janmohamed, S.; D’Agostino, R.B., Sr.; Granger, C.B.; Jones, N.P.; Leiter, L.A.; Rosenberg, A.E.; Sigmon, K.N.; Somerville, M.C.; et al. Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes): A double-blind, randomised placebo-controlled trial. Lancet 2018, 392, 1519–1529. [Google Scholar] [CrossRef]
- Marso, S.P.; Bain, S.C.; Consoli, A.; Eliaschewitz, F.G.; Jodar, E.; Leiter, L.A.; Lingvay, I.; Rosenstock, J.; Seufert, J.; Warren, M.L.; et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 1834–1844. [Google Scholar] [CrossRef] [PubMed]
- Marso, S.P.; Daniels, G.H.; Brown-Frandsen, K.; Kristensen, P.; Mann, J.F.; Nauck, M.A.; Nissen, S.E.; Pocock, S.; Poulter, N.R.; Ravn, L.S.; et al. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Sattar, N.; Lee, M.M.Y.; Kristensen, S.L.; Branch, K.R.H.; Del Prato, S.; Khurmi, N.S.; Lam, C.S.P.; Lopes, R.D.; McMurray, J.J.V.; Pratley, R.E.; et al. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: A systematic review and meta-analysis of randomised trials. Lancet Diabetes Endocrinol. 2021, 9, 653–662. [Google Scholar] [CrossRef] [PubMed]
- Muskiet, M.H.A.; Tonneijck, L.; Smits, M.M.; van Baar, M.J.B.; Kramer, M.H.H.; Hoorn, E.J.; Joles, J.A.; van Raalte, D.H. GLP-1 and the kidney: From physiology to pharmacology and outcomes in diabetes. Nat. Rev. Nephrol. 2017, 13, 605–628. [Google Scholar] [CrossRef] [PubMed]
- Gerstein, H.C.; Sattar, N.; Rosenstock, J.; Ramasundarahettige, C.; Pratley, R.; Lopes, R.D.; Lam, C.S.P.; Khurmi, N.S.; Heenan, L.; Del Prato, S.; et al. Cardiovascular and Renal Outcomes with Efpeglenatide in Type 2 Diabetes. N. Engl. J. Med. 2021, 385, 896–907. [Google Scholar] [CrossRef]
- Holman, R.R.; Bethel, M.A.; Mentz, R.J.; Thompson, V.P.; Lokhnygina, Y.; Buse, J.B.; Chan, J.C.; Choi, J.; Gustavson, S.M.; Iqbal, N.; et al. Effects of Once-Weekly Exenatide on Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2017, 377, 1228–1239. [Google Scholar] [CrossRef]
- Husain, M.; Birkenfeld, A.L.; Donsmark, M.; Dungan, K.; Eliaschewitz, F.G.; Franco, D.R.; Jeppesen, O.K.; Lingvay, I.; Mosenzon, O.; Pedersen, S.D.; et al. Oral Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N. Engl. J. Med. 2019, 381, 841–851. [Google Scholar] [CrossRef]
- Pfeffer, M.A.; Claggett, B.; Diaz, R.; Dickstein, K.; Gerstein, H.C.; Kober, L.V.; Lawson, F.C.; Ping, L.; Wei, X.; Lewis, E.F.; et al. Lixisenatide in Patients with Type 2 Diabetes and Acute Coronary Syndrome. N. Engl. J. Med. 2015, 373, 2247–2257. [Google Scholar] [CrossRef]
- De la Flor, J.C.; Lorenzo, J.D.; Marschall, A.; Valga, F.; Vazquez, T.M.; Cicero, E.R. Efficacy and Safety of Semaglutide, a Glucagon-Like Peptide-1 Receptor Agonist in Real-Life: A Case Series of Patients in Maintenance Incremental Hemodialysis. Case Rep. Nephrol. Dial. 2022, 12, 238–247. [Google Scholar] [CrossRef]
- Hiramatsu, T.; Ozeki, A.; Asai, K.; Saka, M.; Hobo, A.; Furuta, S. Liraglutide Improves Glycemic and Blood Pressure Control and Ameliorates Progression of Left Ventricular Hypertrophy in Patients with Type 2 Diabetes Mellitus on Peritoneal Dialysis. Ther. Apher. Dial. 2015, 19, 598–605. [Google Scholar] [CrossRef]
- Idorn, T.; Knop, F.K.; Jorgensen, M.B.; Jensen, T.; Resuli, M.; Hansen, P.M.; Christensen, K.B.; Holst, J.J.; Hornum, M.; Feldt-Rasmussen, B. Safety and Efficacy of Liraglutide in Patients With Type 2 Diabetes and End-Stage Renal Disease: An Investigator-Initiated, Placebo-Controlled, Double-Blind, Parallel-Group, Randomized Trial. Diabetes Care 2016, 39, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Terawaki, Y.; Nomiyama, T.; Akehi, Y.; Takenoshita, H.; Nagaishi, R.; Tsutsumi, Y.; Murase, K.; Nagasako, H.; Hamanoue, N.; Sugimoto, K.; et al. The efficacy of incretin therapy in patients with type 2 diabetes undergoing hemodialysis. Diabetol. Metab. Syndr. 2013, 5, 10. [Google Scholar] [CrossRef] [PubMed]
- Touzot, M.; Urena-Torres, P.; Dupuy, O. Semaglutide for treatment of obesity in hemodialysis patients waiting for a kidney transplant: New hope? Clin. Kidney J. 2022, 15, 1782–1784. [Google Scholar] [CrossRef] [PubMed]
- Yajima, T.; Yajima, K.; Hayashi, M.; Takahashi, H.; Yasuda, K. Improved glycemic control with once-weekly dulaglutide in addition to insulin therapy in type 2 diabetes mellitus patients on hemodialysis evaluated by continuous glucose monitoring. J. Diabetes Complicat. 2018, 32, 310–315. [Google Scholar] [CrossRef] [PubMed]
- Yajima, T.; Yajima, K.; Takahashi, H.; Yasuda, K. The effect of dulaglutide on body composition in type 2 diabetes mellitus patients on hemodialysis. J. Diabetes Complicat. 2018, 32, 759–763. [Google Scholar] [CrossRef] [PubMed]
- Young, M.A.; Wald, J.A.; Matthews, J.E.; Yang, F.; Reinhardt, R.R. Effect of renal impairment on the pharmacokinetics, efficacy, and safety of albiglutide. Postgrad. Med. 2014, 126, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Hernan, M.A.; Reeves, B.C.; Savovic, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Easterbrook, P.J.; Gopalan, R.; Berlin, J.; Matthews, D.R. Publication bias in clinical research. Lancet 1991, 337, 867–872. [Google Scholar] [CrossRef]
- Chen, J.J.; Wu, C.Y.; Jenq, C.C.; Lee, T.H.; Tsai, C.Y.; Tu, H.T.; Huang, Y.T.; Yen, C.L.; Yen, T.H.; Chen, Y.C.; et al. Association of Glucagon-Like Peptide-1 Receptor Agonist vs Dipeptidyl Peptidase-4 Inhibitor Use With Mortality Among Patients With Type 2 Diabetes and Advanced Chronic Kidney Disease. JAMA Netw. Open 2022, 5, e221169. [Google Scholar] [CrossRef] [PubMed]
- Hirose, N.; Tsujimoto, N.; Katayose, T.; Chin, R. Utilization of glucagon-like peptide-1 receptor agonists and changes in clinical characteristics in patients with type 2 diabetes by chronic kidney disease stage in Japan: A descriptive observational study using a nationwide electronic medical records database. Diabetes Obes. Metab. 2022, 24, 486–498. [Google Scholar] [CrossRef] [PubMed]
- Kondo, M.; Toyoda, M.; Kimura, M.; Ishida, N.; Fukagawa, M. Favorable Effect on Blood Volume Control in Hemodialysis Patients with Type 2 Diabetes after Switching from Insulin Therapy to Liraglutide, a Human Glucagon-like Peptide-1 Analog--Results from a Pilot Study in Japan. Tokai J. Exp. Clin. Med. 2017, 42, 52–57. [Google Scholar]
- Rossing, P.; Baeres, F.M.M.; Bakris, G.; Bosch-Traberg, H.; Gislum, M.; Gough, S.C.L.; Idorn, T.; Lawson, J.; Mahaffey, K.W.; Mann, J.F.E.; et al. The rationale, design and baseline data of FLOW, a kidney outcomes trial with once-weekly semaglutide in people with type 2 diabetes and chronic kidney disease. Nephrol. Dial. Transplant. 2023, 38, 2041–2051. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Gerstein, H.C.; Colhoun, H.M.; Dagenais, G.R.; Diaz, R.; Lakshmanan, M.; Pais, P.; Probstfield, J.; Botros, F.T.; Riddle, M.C.; Ryden, L.; et al. Dulaglutide and renal outcomes in type 2 diabetes: An exploratory analysis of the REWIND randomised, placebo-controlled trial. Lancet 2019, 394, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Mann, J.F.E.; Orsted, D.D.; Buse, J.B. Liraglutide and Renal Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2017, 377, 2197–2198. [Google Scholar] [CrossRef] [PubMed]
- Saito, S.; Nakao, T. Semaglutide, a newly available glucagon-like peptide receptor agonist, shows remarkable favorable effects in hemodialysis patients with obesity and Type 2 diabetes. Ther. Apher. Dial. 2022, 26, 242–243. [Google Scholar] [CrossRef]
- Sun, F.; Chai, S.; Yu, K.; Quan, X.; Yang, Z.; Wu, S.; Zhang, Y.; Ji, L.; Wang, J.; Shi, L. Gastrointestinal adverse events of glucagon-like peptide-1 receptor agonists in patients with type 2 diabetes: A systematic review and network meta-analysis. Diabetes Technol. Ther. 2015, 17, 35–42. [Google Scholar] [CrossRef]
- Muller, L.M.; Gorter, K.J.; Hak, E.; Goudzwaard, W.L.; Schellevis, F.G.; Hoepelman, A.I.; Rutten, G.E. Increased risk of common infections in patients with type 1 and type 2 diabetes mellitus. Clin. Infect. Dis. 2005, 41, 281–288. [Google Scholar] [CrossRef]
- Schuetz, P.; Castro, P.; Shapiro, N.I. Diabetes and sepsis: Preclinical findings and clinical relevance. Diabetes Care 2011, 34, 771–778. [Google Scholar] [CrossRef] [PubMed]
- Shah, F.A.; Mahmud, H.; Gallego-Martin, T.; Jurczak, M.J.; O’Donnell, C.P.; McVerry, B.J. Therapeutic Effects of Endogenous Incretin Hormones and Exogenous Incretin-Based Medications in Sepsis. J. Clin. Endocrinol. Metab. 2019, 104, 5274–5284. [Google Scholar] [CrossRef] [PubMed]
- Steven, S.; Jurk, K.; Kopp, M.; Kroller-Schon, S.; Mikhed, Y.; Schwierczek, K.; Roohani, S.; Kashani, F.; Oelze, M.; Klein, T.; et al. Glucagon-like peptide-1 receptor signalling reduces microvascular thrombosis, nitro-oxidative stress and platelet activation in endotoxaemic mice. Br. J. Pharmacol. 2017, 174, 1620–1632. [Google Scholar] [CrossRef] [PubMed]
- Khunti, K.; Knighton, P.; Zaccardi, F.; Bakhai, C.; Barron, E.; Holman, N.; Kar, P.; Meace, C.; Sattar, N.; Sharp, S.; et al. Prescription of glucose-lowering therapies and risk of COVID-19 mortality in people with type 2 diabetes: A nationwide observational study in England. Lancet Diabetes Endocrinol. 2021, 9, 293–303. [Google Scholar] [CrossRef] [PubMed]
- Nikolaidis, L.A.; Mankad, S.; Sokos, G.G.; Miske, G.; Shah, A.; Elahi, D.; Shannon, R.P. Effects of glucagon-like peptide-1 in patients with acute myocardial infarction and left ventricular dysfunction after successful reperfusion. Circulation 2004, 109, 962–965. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.S.; Fonarow, G.C.; McGuire, D.K.; Hernandez, A.F.; Vaduganathan, M.; Rosenstock, J.; Handelsman, Y.; Verma, S.; Anker, S.D.; McMurray, J.J.V.; et al. Glucagon-Like Peptide 1 Receptor Agonists and Heart Failure: The Need for Further Evidence Generation and Practice Guidelines Optimization. Circulation 2020, 142, 1205–1218. [Google Scholar] [CrossRef] [PubMed]
- Ussher, J.R.; Drucker, D.J. Cardiovascular biology of the incretin system. Endocr. Rev. 2012, 33, 187–215. [Google Scholar] [CrossRef]
- ElSayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Hilliard, M.E.; Isaacs, D.; Johnson, E.L.; et al. 1. Improving Care and Promoting Health in Populations: Standards of Care in Diabetes-2023. Diabetes Care 2023, 46, S10–S18. [Google Scholar] [CrossRef]
- Hinnen, D. Glucagon-Like Peptide 1 Receptor Agonists for Type 2 Diabetes. Diabetes Spectr. 2017, 30, 202–210. [Google Scholar] [CrossRef]
- Iqbal, J.; Wu, H.X.; Hu, N.; Zhou, Y.H.; Li, L.; Xiao, F.; Wang, T.; Jiang, H.L.; Xu, S.N.; Huang, B.L.; et al. Effect of glucagon-like peptide-1 receptor agonists on body weight in adults with obesity without diabetes mellitus-a systematic review and meta-analysis of randomized control trials. Obes. Rev. 2022, 23, e13435. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Terawaki et al. [23] (2013) | Hiramatsu et al. [21] (2015) | Idorn et al. [22] (2016) | Kondo et al. [34] (2017) | Yajima et al. [1] (2018) | Yajima et al. [2] (2018) | Hirose et al. [33] (2021) | Chen et al. [32] (2022) |
|---|---|---|---|---|---|---|---|---|
| Study type | Crossover controlled trial | Non-randomized controlled study | Randomized controlled trial | Retrospective cohort | Non-randomized controlled study | Non-randomized controlled study | Retrospective cohort | Retrospective cohort |
| Site | Japan, single center | Japan, single center | Denmark, multicenter | Japan, single center | Japan, single center | Japan, single center | Japan, national database | Taiwan, national database |
| GLP-1RA name | Liraglutide | Liraglutide | Liraglutide | Liraglutide | Dulaglutide | Dulaglutide | 61.5% Dulaglutide, 36.5% Liraglutide, 2% Lixisenatide | N/A |
| GLP-1RA dosage | 0.3 mg daily | 0.6–0.9 mg daily | Titrate to a maximum dose of 1.8 mg daily | 0.3–0.9 mg daily | 0.75 mg weekly | 0.75 mg weekly | N/A | N/A |
| Use of GLP-1RA | Single therapy | Single therapy | Add on therapy | Single therapy | Add on therapy | Add on therapy | Both single and add on therapy | Both single and add on therapy |
| Concomitant insulin used with GLP-1RA, % | 0 | 0 | 80 | 0 | 100 | 100 | 34.1 | 16.3 |
| Control | Vildaglipin, alogliptin, and insulin | Standard therapy | Placebo | None | Teneligliptin | Insulin | None | DPP-4i |
| Total N GLP1-RA Control | 10 10 10 | 30 15 15 | 24 a (20 b) 14 a (10 b) 10 | 5 5 0 | 21 11 10 | 15 15 15 | 255 255 0 | 27,279 701 26,578 |
| Male, n (%) | 7 (70.0) | 22 (73.3) | 17 (85.0) | 4 (80.0) | 16 (76.2) | 13 (86.7) | 167 (65.5) | 14,789 (54.2) |
| Age, year | 62.9B ± 4.3 | 67.6 ± 7.0 | 67.1 ± 3.8 | 67.8 ± 4.3 | 68 (61, 72) c | 72 (66, 79) c | 66.5 ± 11.6 | 64.8 ± 13.0 |
| Body mass index, kg/m2 | 23.0 ± 1.5 | 24.8 ± 3.9 | 31.6 ± 2.4 | 23.2 ±1.2 | 23.1 (21.6, 26.3) c | 23.6 (22.9, 25.3) c | 24.5 ± 5.1 | N/A |
| Stage of advanced CKD | ESKD undergoing HD | ESKD undergoing PD | ESKD | ESKD undergoing HD | ESKD undergoing HD | ESKD undergoing HD | Stage 5 ND and ESKD | Stage 5 ND and ESKD |
| Duration of RRT | 4.1 ± 1.1 years | 10 ± 9.3 months | N/A | N/A | 13.5 (3.7, 30.8) months c | 12 (2, 82) months c | N/A | N/A |
| Duration of DM, years | 25.4 ± 2.3 | 17.6 ± 12 | 14.2 ± 2.4 | N/A | N/A | 22 (18, 32) c | 6.9 ± 6.9 | N/A |
| Baseline HbA1c, % | N/A | 5.9 ± 0.8 | 6.7 ± 0.4 | 6.0 ± 1.0 | N/A | 6.2 (5.3, 6.8) c | 7.4 ± 1.6 | N/A |
| Baseline glycated albumin, % | 24.1 ± 1.5 | 16.9 ± 0.4 | N/A | N/A | 22.3 (17.6, 25.1) c | 21.8 (17.9, 25.1) c | 24.9 ± 8.3 | N/A |
| Baseline Hemoglobin, mg/dL | N/A | N/A | N/A | 10.1± 0.5 | 10.4 (9.3, 11.6) c | 10.6 (9.5, 12.5) c | N/A | N/A |
| Comorbidities CAD, n (%) Stroke, n (%) HF, n (%) DR, n (%) | N/A N/A N/A 0 (0) | N/A | 7 (35) N/A N/A 9 (45) | N/A | N/A | N/A | 87 (34.1) 29 (11.4) 124 (48.6) 51 (20) | 5722 (21.0) 3387 (12.4) 4751 (17.4) N/A |
| Follow-up time | 3 months | 12 months | 3 months | 3 months | 6 months | 5 weeks | N/A | 4 years d |
| Source of funding | Ministry of health, labor and welfare, Japan | None | Drug company (Novo Nordisk) | None | N/A | N/A | Drug company (Eli Lilly) | Chang Gung memorial hospital and ministry of science and technology, Taiwan |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krisanapan, P.; Sanpawithayakul, K.; Pattharanitima, P.; Thongprayoon, C.; Miao, J.; Mao, M.A.; Suppadungsuk, S.; Tangpanithandee, S.; Craici, I.M.; Cheungpasitporn, W. Safety and Efficacy of GLP-1 Receptor Agonists in Type 2 Diabetes Mellitus with Advanced and End-Stage Kidney Disease: A Systematic Review and Meta-Analysis. Diseases 2024, 12, 14. https://doi.org/10.3390/diseases12010014
Krisanapan P, Sanpawithayakul K, Pattharanitima P, Thongprayoon C, Miao J, Mao MA, Suppadungsuk S, Tangpanithandee S, Craici IM, Cheungpasitporn W. Safety and Efficacy of GLP-1 Receptor Agonists in Type 2 Diabetes Mellitus with Advanced and End-Stage Kidney Disease: A Systematic Review and Meta-Analysis. Diseases. 2024; 12(1):14. https://doi.org/10.3390/diseases12010014
Chicago/Turabian StyleKrisanapan, Pajaree, Kanokporn Sanpawithayakul, Pattharawin Pattharanitima, Charat Thongprayoon, Jing Miao, Michael A. Mao, Supawadee Suppadungsuk, Supawit Tangpanithandee, Iasmina M. Craici, and Wisit Cheungpasitporn. 2024. "Safety and Efficacy of GLP-1 Receptor Agonists in Type 2 Diabetes Mellitus with Advanced and End-Stage Kidney Disease: A Systematic Review and Meta-Analysis" Diseases 12, no. 1: 14. https://doi.org/10.3390/diseases12010014
APA StyleKrisanapan, P., Sanpawithayakul, K., Pattharanitima, P., Thongprayoon, C., Miao, J., Mao, M. A., Suppadungsuk, S., Tangpanithandee, S., Craici, I. M., & Cheungpasitporn, W. (2024). Safety and Efficacy of GLP-1 Receptor Agonists in Type 2 Diabetes Mellitus with Advanced and End-Stage Kidney Disease: A Systematic Review and Meta-Analysis. Diseases, 12(1), 14. https://doi.org/10.3390/diseases12010014