
The Impact of COVID-19 on Amputation and Mortality Rates in Patients with Acute Limb Ischemia: A Systematic Review and Meta-Analysis


 , ,
, ,  and
and
Abstract
1. Introduction
2. Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Assessment of Risk of Bias
2.4. Data Synthesis Methods for Meta-Analysis
3. Results
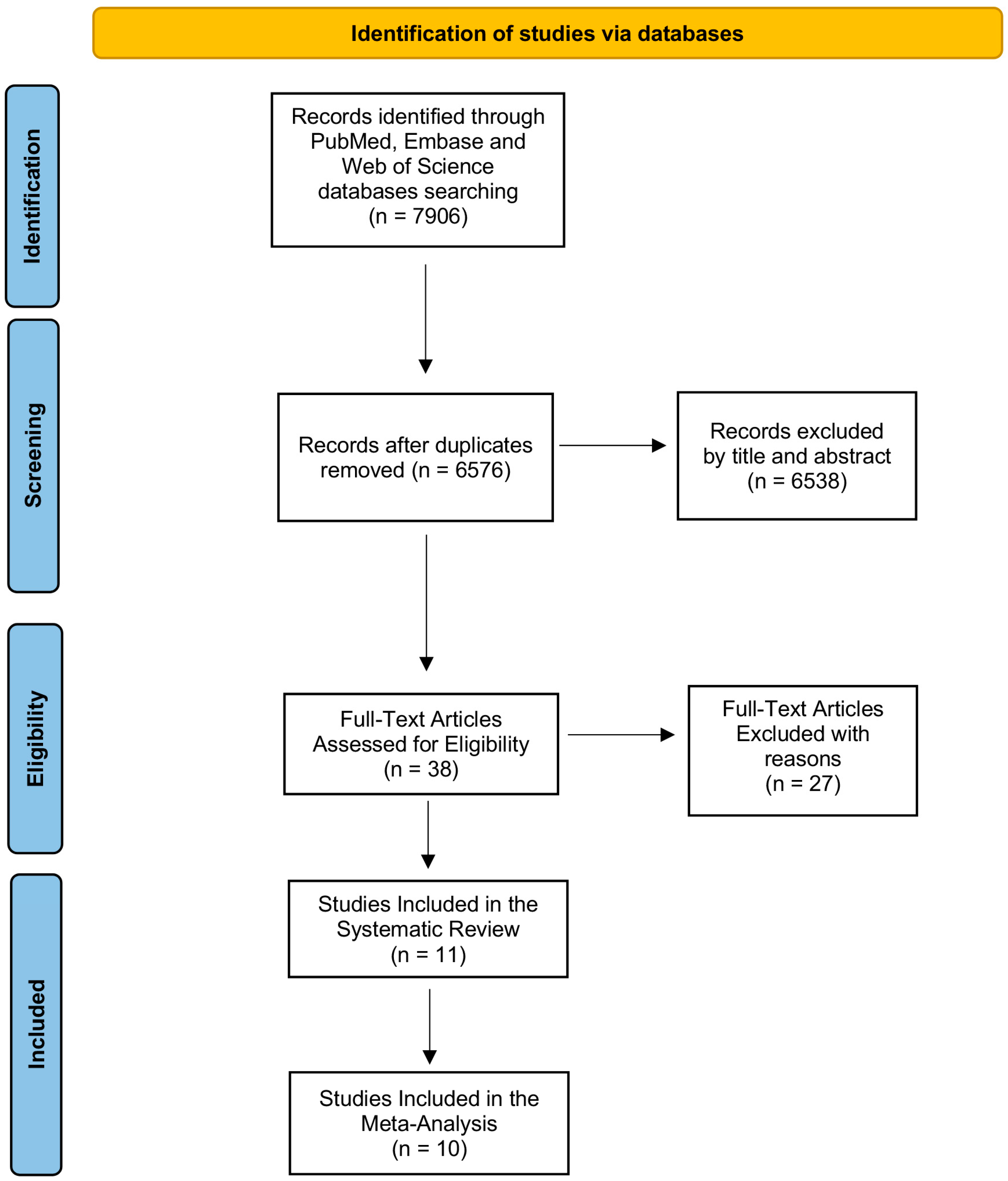
3.1. Findings from Systematic Search
3.2. Description of Included Studies in the Systematic Review
3.3. Meta-Analysis
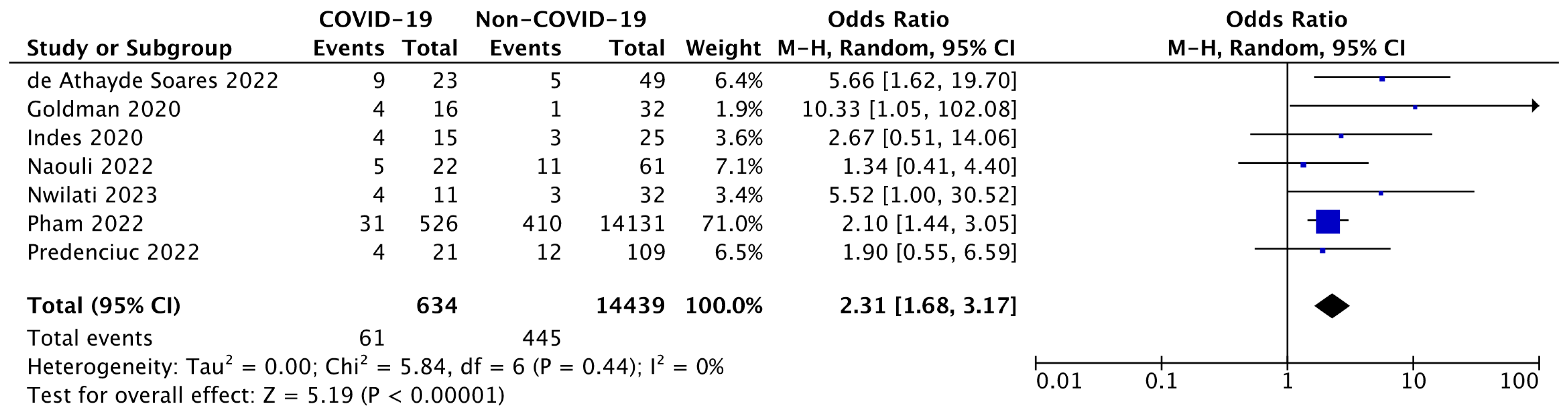
3.3.1. Evaluation of ALI-Related Amputation in COVID-19 Patients
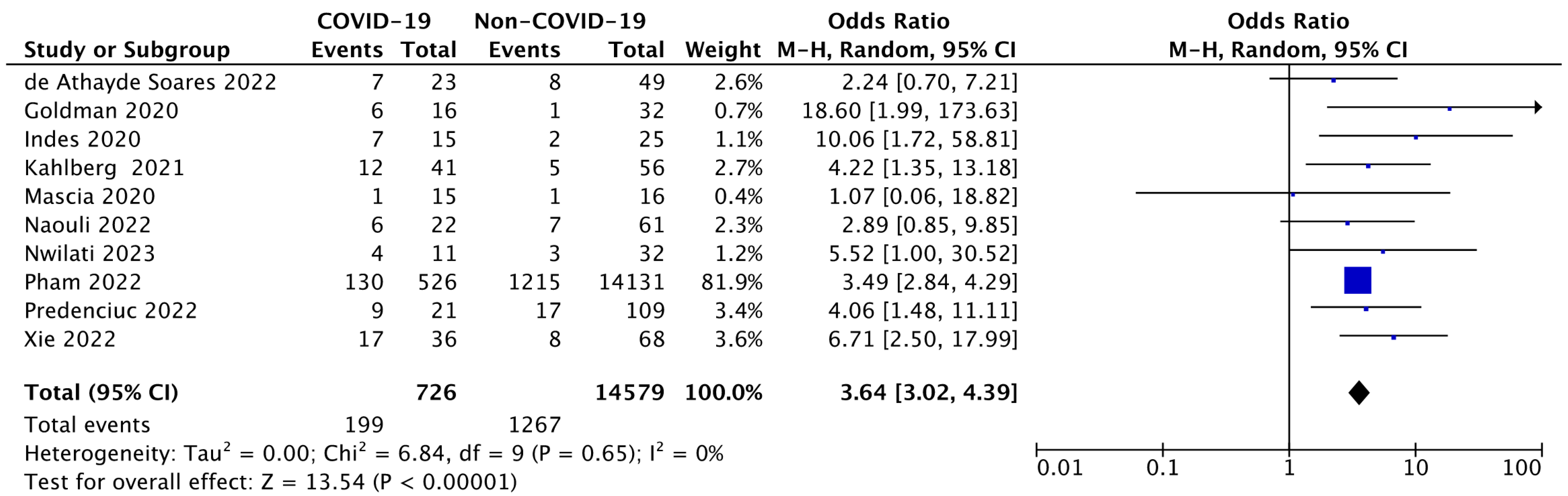
3.3.2. Evaluation of the Mortality Rate Following ALI in COVID-19 Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef]
- V’Kovski, P.; Kratzel, A.; Steiner, S.; Stalder, H.; Thiel, V. Coronavirus biology and replication: Implications for SARS-CoV-2. Nat. Rev. Microbiol. 2021, 19, 155–170. [Google Scholar] [CrossRef]
- Wang, M.Y.; Zhao, R.; Gao, L.J.; Gao, X.F.; Wang, D.P.; Cao, J.M. SARS-CoV-2: Structure, Biology, and Structure-Based Therapeutics Development. Front. Cell. Infect. Microbiol. 2020, 10, 587269. [Google Scholar] [CrossRef]
- Sharma, A.; Ahmad Farouk, I.; Lal, S.K. COVID-19: A Review on the Novel Coronavirus Disease Evolution, Transmission, Detection, Control and Prevention. Viruses 2021, 13, 202. [Google Scholar] [CrossRef]
- Lamers, M.M.; Haagmans, B.L. SARS-CoV-2 pathogenesis. Nat. Rev. Microbiol. 2022, 20, 270–284. [Google Scholar] [CrossRef]
- Beyerstedt, S.; Casaro, E.B.; Rangel, E.B. COVID-19: Angiotensin-converting enzyme 2 (ACE2) expression and tissue susceptibility to SARS-CoV-2 infection. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 905–919. [Google Scholar] [CrossRef]
- Diamond, M.S.; Kanneganti, T.D. Innate immunity: The first line of defense against SARS-CoV-2. Nat. Immunol. 2022, 23, 165–176. [Google Scholar] [CrossRef]
- da Rosa Mesquita, R.; Francelino Silva Junior, L.C.; Santos Santana, F.M.; Farias de Oliveira, T.; Campos Alcantara, R.; Monteiro Arnozo, G.; Rodrigues da Silva Filho, E.; Galdino Dos Santos, A.G.; Oliveira da Cunha, E.J.; Salgueiro de Aquino, S.H.; et al. Clinical manifestations of COVID-19 in the general population: Systematic review. Wien. Klin. Wochenschr. 2021, 133, 377–382. [Google Scholar] [CrossRef]
- Mueller, A.L.; McNamara, M.S.; Sinclair, D.A. Why does COVID-19 disproportionately affect older people? Aging 2020, 12, 9959–9981. [Google Scholar] [CrossRef] [PubMed]
- Tan, L.Y.; Komarasamy, T.V.; Rmt Balasubramaniam, V. Hyperinflammatory Immune Response and COVID-19: A Double Edged Sword. Front. Immunol. 2021, 12, 742941. [Google Scholar] [CrossRef] [PubMed]
- Montazersaheb, S.; Hosseiniyan Khatibi, S.M.; Hejazi, M.S.; Tarhriz, V.; Farjami, A.; Ghasemian Sorbeni, F.; Farahzadi, R.; Ghasemnejad, T. COVID-19 infection: An overview on cytokine storm and related interventions. Virol. J. 2022, 19, 92. [Google Scholar] [CrossRef]
- Mondal, S.; Quintili, A.L.; Karamchandani, K.; Bose, S. Thromboembolic disease in COVID-19 patients: A brief narrative review. J. Intensive Care 2020, 8, 70. [Google Scholar] [CrossRef] [PubMed]
- Capra, A.P.; Ardizzone, A.; Panto, G.; Paterniti, I.; Campolo, M.; Crupi, L.; Squeri, R.; Esposito, E. The Prognostic Value of Pentraxin-3 in COVID-19 Patients: A Systematic Review and Meta-Analysis of Mortality Incidence. Int. J. Mol. Sci. 2023, 24, 3537. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.W.; Kim, D.Y.; Yun, N.; Kim, D.M. Coronavirus Disease 2019-Associated Coagulopathy. Microorganisms 2022, 10, 1556. [Google Scholar] [CrossRef]
- Olinic, D.M.; Stanek, A.; Tataru, D.A.; Homorodean, C.; Olinic, M. Acute Limb Ischemia: An Update on Diagnosis and Management. J. Clin. Med. 2019, 8, 1215. [Google Scholar] [CrossRef]
- Obara, H.; Matsubara, K.; Kitagawa, Y. Acute Limb Ischemia. Ann. Vasc. Dis. 2018, 11, 443–448. [Google Scholar] [CrossRef]
- Galyfos, G.; Sianou, A.; Frountzas, M.; Vasilios, K.; Vouros, D.; Theodoropoulos, C.; Michalopoulou, V.; Sigala, F.; Filis, K. Acute limb ischemia among patients with COVID-19 infection. J. Vasc. Surg. 2022, 75, 326–342. [Google Scholar] [CrossRef]
- Arnold, J.; Koyfman, A.; Long, B. High risk and low prevalence diseases: Acute limb ischemia. Am. J. Emerg. Med. 2023, 74, 152–158. [Google Scholar] [CrossRef]
- Ferrer, C.; Cannizzaro, G.A.; Borlizzi, A.; Caruso, C.; Giudice, R. Acute ischemia of the upper and lower limbs: Tailoring the treatment to the underlying etiology. Semin. Vasc. Surg. 2023, 36, 211–223. [Google Scholar] [CrossRef]
- Kulezic, A.; Acosta, S. Epidemiology and Prognostic Factors in Acute Lower Limb Ischaemia: A Population Based Study. Eur. J. Vasc. Endovasc. Surg. 2022, 63, 296–303. [Google Scholar] [CrossRef]
- Auda, M.E.; Ratner, M.; Pezold, M.; Rockman, C.; Sadek, M.; Jacobowitz, G.; Berland, T.; Siracuse, J.J.; Teter, K.; Johnson, W.; et al. Short-term outcomes of endovascular management of acute limb ischemia using aspiration mechanical thrombectomy. Vascular, 2024; epub ahead of print. [Google Scholar] [CrossRef]
- Pham, A.; Heib, A.; Goodman, E.; Lipsitz, E.; Indes, J. Outcomes of acute limb ischemia in COVID-19. J. Vasc. Surg. 2022, 76, 1006–1013.e3. [Google Scholar] [CrossRef] [PubMed]
- Jongkind, V.; Earnshaw, J.J.; Bastos Goncalves, F.; Cochennec, F.; Debus, E.S.; Hinchliffe, R.; Menyhei, G.; Svetlikov, A.V.; Tshomba, Y.; Van Den Berg, J.C.; et al. Editor’s Choice-Update of the European Society for Vascular Surgery (ESVS) 2020 Clinical Practice Guidelines on the Management of Acute Limb Ischaemia in Light of the COVID-19 Pandemic, Based on a Scoping Review of the Literature. Eur. J. Vasc. Endovasc. Surg. 2022, 63, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Capra, A.P.; Ardizzone, A.; Briuglia, S.; La Rosa, M.A.; Mondello, S.; Campolo, M.; Esposito, E. A Systematic Review and Meta-Analysis of the Association between the FV H1299R Variant and the Risk of Recurrent Pregnancy Loss. Biology 2022, 11, 1608. [Google Scholar] [CrossRef] [PubMed]
- Ardizzone, A.; Capra, A.P.; Mondello, S.; Briuglia, S.; La Rosa, M.A.; Campolo, M.; Esposito, E. H1299R Variant in Factor V and Recurrent Pregnancy Loss: A Systematic Review and Meta-Analysis Protocol. Genes 2022, 13, 1019. [Google Scholar] [CrossRef] [PubMed]
- Goldman, I.A.; Ye, K.; Scheinfeld, M.H. Lower-extremity Arterial Thrombosis Associated with COVID-19 Is Characterized by Greater Thrombus Burden and Increased Rate of Amputation and Death. Radiology 2020, 297, E263–E269. [Google Scholar] [CrossRef]
- Indes, J.E.; Koleilat, I.; Hatch, A.N.; Choinski, K.; Jones, D.B.; Aldailami, H.; Billett, H.; Denesopolis, J.M.; Lipsitz, E. Early experience with arterial thromboembolic complications in patients with COVID-19. J. Vasc. Surg. 2021, 73, 381–389.e1. [Google Scholar] [CrossRef]
- Malkoc, A.; GnanaDev, R.; Botea, L.; Jeney, A.; Glover, K.; Retamozo, M.; GnanaDev, D.; Schwartz, S. A Comparative Analysis of Critical Limb Ischemia in the Intensive Care Unit since the COVID-19 Pandemic. Ann. Vasc. Surg. 2023, 90, 39–47. [Google Scholar] [CrossRef]
- Naouli, H.; Jiber, H.; Bouarhroum, A. Acute Limb Ischemia in COVID-19 Patients: A Single University Center Experience. Cureus 2022, 14, e32829. [Google Scholar] [CrossRef]
- Nwilati, A.E.; Shafiei, M.; Mehanna, R.; Kokash, D.; Syed Iqbaluddin, J.; Hallak, F.; Abdalla, S.F. Incidence of Major Limb Arterial Thrombosis in Positive versus Negative COVID-19 Patients: A Cross-Sectional Retrospective Study. Dubai Med. J. 2023, 6, 181–187. [Google Scholar] [CrossRef]
- Xie, B.; Semaan, D.B.; Binko, M.A.; Agrawal, N.; Kulkarni, R.N.; Andraska, E.A.; Sachdev, U.; Chaer, R.A.; Eslami, M.H.; Makaroun, M.S.; et al. COVID-associated acute limb ischemia during the Delta surge and the effect of vaccines. J. Vasc. Surg. 2023, 77, 1165–1173.e1. [Google Scholar] [CrossRef]
- de Athayde Soares, R.; Futigami, A.Y.; Barbosa, A.G.; Sacilotto, R. Acute Arterial Occlusions in COVID-19 Times: A Comparison Study Among Patients with Acute Limb Ischemia With or Without COVID-19 Infection. Ann. Vasc. Surg. 2022, 83, 80–86. [Google Scholar] [CrossRef]
- Kahlberg, A.; Mascia, D.; Bellosta, R.; Attisani, L.; Pegorer, M.; Socrate, A.M.; Ferraris, M.; Trabattoni, P.; Rinaldi, E.; Melloni, A.; et al. Vascular Surgery During COVID-19 Emergency in Hub Hospitals of Lombardy: Experience on 305 Patients. Eur. J. Vasc. Endovasc. Surg. 2021, 61, 306–315. [Google Scholar] [CrossRef]
- Predenciuc, A.; Casian, D.; Culiuc, V. Outcomes of Surgical Revascularization for Acute Limb Ischemia in COVID-19 Patients Comparing to Noninfected Cohort: A Single-Center Observational Prospective Study. Ann. Vasc. Surg. 2023, 91, 81–89. [Google Scholar] [CrossRef]
- Mascia, D.; Kahlberg, A.; Melloni, A.; Rinaldi, E.; Melissano, G.; Chiesa, R. Single-Center Vascular Hub Experience after 7 weeks of COVID-19 Pandemic in Lombardy (Italy). Ann. Vasc. Surg. 2020, 69, 90–99. [Google Scholar] [CrossRef]
- Creager, M.A.; Kaufman, J.A.; Conte, M.S. Clinical practice. Acute limb ischemia. N. Engl. J. Med. 2012, 366, 2198–2206. [Google Scholar] [CrossRef]
- Hardman, R.L.; Jazaeri, O.; Yi, J.; Smith, M.; Gupta, R. Overview of classification systems in peripheral artery disease. Semin. Interv. Radiol. 2014, 31, 378–388. [Google Scholar] [CrossRef]
- Rutherford, R.B.; Baker, J.D.; Ernst, C.; Johnston, K.W.; Porter, J.M.; Ahn, S.; Jones, D.N. Recommended standards for reports dealing with lower extremity ischemia: Revised version. J. Vasc. Surg. 1997, 26, 517–538. [Google Scholar] [CrossRef]
- Yang, H.; Rao, Z. Structural biology of SARS-CoV-2 and implications for therapeutic development. Nat. Rev. Microbiol. 2021, 19, 685–700. [Google Scholar] [CrossRef] [PubMed]
- Ardizzone, A.; Capra, A.P.; Campolo, M.; Filippone, A.; Esposito, E.; Briuglia, S. Neurofibromatosis: New Clinical Challenges in the Era of COVID-19. Biomedicines 2022, 10, 940. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.N.; Choi, J.Y.; Cooper, B.; Renwick, B.; Mohamed, M.M.; Makris, S.A. Long-Term Impact of COVID-19 related disruption of NHS Elective services on Emergency Major Lower Limb Amputations. Ann. Vasc. Surg. 2024, 102, 84–91. [Google Scholar] [CrossRef]
- Hu, B.; Huang, S.; Yin, L. The cytokine storm and COVID-19. J. Med. Virol. 2021, 93, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Castanares-Zapatero, D.; Chalon, P.; Kohn, L.; Dauvrin, M.; Detollenaere, J.; Maertens de Noordhout, C.; Primus-de Jong, C.; Cleemput, I.; Van den Heede, K. Pathophysiology and mechanism of long COVID: A comprehensive review. Ann. Med. 2022, 54, 1473–1487. [Google Scholar] [CrossRef] [PubMed]
- Strambo, D.; Marto, J.P.; Ntaios, G.; Nguyen, T.N.; Michel, P.; Global COVID-19 Stroke Registry. Effect of Asymptomatic and Symptomatic COVID-19 on Acute Ischemic Stroke Revascularization Outcomes. Stroke 2024, 55, 78–88. [Google Scholar] [CrossRef] [PubMed]
- Bjorck, M.; Earnshaw, J.J.; Acosta, S.; Bastos Goncalves, F.; Cochennec, F.; Debus, E.S.; Hinchliffe, R.; Jongkind, V.; Koelemay, M.J.W.; Menyhei, G.; et al. Editor’s Choice-European Society for Vascular Surgery (ESVS) 2020 Clinical Practice Guidelines on the Management of Acute Limb Ischaemia. Eur. J. Vasc. Endovasc. Surg. 2020, 59, 173–218. [Google Scholar] [CrossRef] [PubMed]
- Natarajan, B.; Patel, P.; Mukherjee, A. Acute Lower Limb Ischemia-Etiology, Pathology, and Management. Int. J. Angiol. 2020, 29, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Mazzeffi, M.A.; Chow, J.H.; Tanaka, K. COVID-19 Associated Hypercoagulability: Manifestations, Mechanisms, and Management. Shock 2021, 55, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Conway, E.M.; Mackman, N.; Warren, R.Q.; Wolberg, A.S.; Mosnier, L.O.; Campbell, R.A.; Gralinski, L.E.; Rondina, M.T.; van de Veerdonk, F.L.; Hoffmeister, K.M.; et al. Understanding COVID-19-associated coagulopathy. Nat. Rev. Immunol. 2022, 22, 639–649. [Google Scholar] [CrossRef] [PubMed]
- Abou-Ismail, M.Y.; Diamond, A.; Kapoor, S.; Arafah, Y.; Nayak, L. The hypercoagulable state in COVID-19: Incidence, pathophysiology, and management. Thromb. Res. 2020, 194, 101–115. [Google Scholar] [CrossRef]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef]
- Luo, H.C.; You, C.Y.; Lu, S.W.; Fu, Y.Q. Characteristics of coagulation alteration in patients with COVID-19. Ann. Hematol. 2021, 100, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Are, E.B.; Song, Y.; Stockdale, J.E.; Tupper, P.; Colijn, C. COVID-19 endgame: From pandemic to endemic? Vaccination, reopening and evolution in low- and high-vaccinated populations. J. Theor. Biol. 2023, 559, 111368. [Google Scholar] [CrossRef] [PubMed]
- Robinson, P.C.; Liew, D.F.L.; Tanner, H.L.; Grainger, J.R.; Dwek, R.A.; Reisler, R.B.; Steinman, L.; Feldmann, M.; Ho, L.P.; Hussell, T.; et al. COVID-19 therapeutics: Challenges and directions for the future. Proc. Natl. Acad. Sci. USA 2022, 119, e2119893119. [Google Scholar] [CrossRef] [PubMed]
- Melissano, G.; Mascia, D.; Baccellieri, D.; Kahlberg, A.; Bertoglio, L.; Rinaldi, E.; Chiesa, R. Pattern of vascular disease in Lombardy, Italy, during the first month of the COVID-19 outbreak. J. Vasc. Surg. 2020, 72, 4–5. [Google Scholar] [CrossRef] [PubMed]
- Candeloro, M.; Schulman, S. Arterial Thrombotic Events in Hospitalized COVID-19 Patients: A Short Review and Meta-Analysis. Semin. Thromb. Hemost. 2023, 49, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Cheruiyot, I.; Kipkorir, V.; Ngure, B.; Misiani, M.; Munguti, J.; Ogeng’o, J. Arterial Thrombosis in Coronavirus Disease 2019 Patients: A Rapid Systematic Review. Ann. Vasc. Surg. 2021, 70, 273–281. [Google Scholar] [CrossRef]
- The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021. Available online: https://www.bmj.com/content/372/bmj.n71 (accessed on 29 March 2021).




{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Study types: Clinical Trials, Randomized Controlled Trials, Observational studies, Case-control studies, Cross-sectional studies, Cohort studies. Time range: 30 January 2023 up to 31 December 2023. Articles including both COVID-19 positive and negative subjects clearly reporting amputation and mortality rates related to ALI. | Case reports, editorials, letters, reviews, guidelines, abstracts and paper conferences, systematic reviews and meta-analyses, and ongoing studies. Articles not written in English. |
| ALI | ALI-Related Outcomes | COVID-19 |
|---|---|---|
| “Acute limb ischemia”, ALI, ALLI, “Limb Ischemia”, “Limb ischaemia”, Ischemia, Ischemias, Ischaemia, Ischaemias, “limb hypoperfusion”, “extremities ischemia”, “leg ischemia”, “leg ischaemia” | Amputation, amputations, disarticulation, disarticulations, death, deaths, mortality, mortalities | COVID-19, COVID19, 2019-nCoV, “Coronavirus Disease 2019”, “Coronavirus Disease-19”, SARS-CoV-2, “SARS Coronavirus 2”, “Severe Acute Respiratory Syndrome Coronavirus”, Coronavirus, Coronaviruses |
| First Author and Year of Publication | Type of Study | Patients Included | Differences in Amputation Rate * | Differences in Mortality * | Reference |
|---|---|---|---|---|---|
| de Athayde Soares et al., 2022 | Prospective cohort study | Total (n: 72)
| ALI and COVID-19: 9/23 (39.1%) vs. ALI without COVID-19: 5/49 (10.2%) | ALI and COVID-19: 7/23 (30.4%) vs. ALI without COVID-19: 8/49 (16.7%) | [33] |
| Goldman et al., 2020 | Retrospective propensity score-matched study | Total (n: 48)
| ALI and COVID-19: 4/16 (25.0%) vs. ALI without COVID-19: 1/32 (3.1%) Amputations occurring during the index hospital admission | ALI and COVID-19: 6/16 (37.5%) vs. ALI without COVID-19: 1/32 (3.1%) Death occurring during the index hospital admission | [27] |
| Indes et al., 2020 | Retrospective cohort study | Total (n: 40)
| ALI and COVID-19: 4/15 (26.7%) vs. ALI without COVID-19: 3/25 (12.0%) | ALI and COVID-19: 7/15 (46.7%) vs. ALI without COVID-19: 2/25 (8.0%) | [28] |
| Kahlberg et al., 2021 | Prospective observational study | Total ALI patients (n: 97)
| - | ALI and COVID-19: 12/41 (29.3%) vs. ALI without COVID-19: 5/56 (8.9%) In hospital deaths | [34] |
| Malkoc et al., 2022 | Retrospective case-control study | Total (n: 498)
| 12/249 ICU COVID-19 positive patients developed a gangrene during the ICU stay (4.8%), 4/12 (33.4%) underwent a major amputation vs. 1/249 (0.4%) ICU COVID-19 negative patients developed a gangrene during the ICU-stay, 0/1 underwent any amputation. | Mortality among the COVID-19 positive patients that developed gangrene: 5/12 (41.7%) vs. Mortality among the ICU COVID-19 positive patients: 0/1 | [29] |
| Mascia et al., 2020 | Prospective/retrospective study | Total (n: 31)
| Total limb salvage rate, considering both COVID-19 positive and COVID-19 negative patients: 29/31 (93.5%) | ALI and COVID-19: 1/15 (6.7%) vs. ALI without COVID-19: 1/16 (6.2%) Death occurring during hospitalization | [36] |
| Naouli et al., 2022 | Retrospective observational study | Total (n: 83)
| ALI and COVID-19: 5/22 (22.7%) vs. ALI without COVID-19: 11/61 (18.0%) In hospital amputations | ALI and COVID-19: 6/22 (27.3%) vs. ALI without COVID-19: 7/61 (11.5%) In hospital deaths | [30] |
| Nwilati et al., 2023 | Retrospective cross-sectional study | Total (n: 43)
| ALI and COVID-19: 4/11 (36.4%) vs. ALI without COVID-19: 3/32 (9.4%) Amputations occurring during the entire length of the hospitalization | ALI and COVID-19: 4/11 (36.4%) vs. ALI without COVID-19: 3/32 (9.4%) Death occurring during the entire length of the hospitalization | [31] |
| Pham et al., 2022 | Retrospective propensity score-matched study | Total (n: 14,657)
| ALI and COVID-19: 31/526 (7.0%) vs. ALI without COVID-19: 381/14,131 (2.7%) 180 days amputation rate | ALI and COVID-19: 130/526 (24.7%) vs. ALI without COVID-19: 1215/14,131 (8.6%) 180 days mortality | [22] |
| Predenciuc et al., 2022 | Prospective observational study | Total (n: 130)
| ALI and COVID-19: 4/21 (19.0%) vs. ALI without COVID-19: 12/109 (11.0%) | ALI and COVID-19: 9/21 (42.9%) vs. ALI without COVID-19: 17/109 (15.6%) | [35] |
| Xie et al., 2022 | Retrospective cohort study | Total (n: 104)
| ALI and COVID-19: 11/40 limbs (27.5%) vs. ALI without COVID-19: 2/74 limbs (2.7%) | ALI and COVID-19: 17/36 (47.2%) vs. ALI without COVID-19: 8/68 (11.8%) | [32] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crupi, L.; Ardizzone, A.; Calapai, F.; Scuderi, S.A.; Benedetto, F.; Esposito, E.; Capra, A.P. The Impact of COVID-19 on Amputation and Mortality Rates in Patients with Acute Limb Ischemia: A Systematic Review and Meta-Analysis. Diseases 2024, 12, 74. https://doi.org/10.3390/diseases12040074
Crupi L, Ardizzone A, Calapai F, Scuderi SA, Benedetto F, Esposito E, Capra AP. The Impact of COVID-19 on Amputation and Mortality Rates in Patients with Acute Limb Ischemia: A Systematic Review and Meta-Analysis. Diseases. 2024; 12(4):74. https://doi.org/10.3390/diseases12040074
Chicago/Turabian StyleCrupi, Lelio, Alessio Ardizzone, Fabrizio Calapai, Sarah Adriana Scuderi, Filippo Benedetto, Emanuela Esposito, and Anna Paola Capra. 2024. "The Impact of COVID-19 on Amputation and Mortality Rates in Patients with Acute Limb Ischemia: A Systematic Review and Meta-Analysis" Diseases 12, no. 4: 74. https://doi.org/10.3390/diseases12040074
APA StyleCrupi, L., Ardizzone, A., Calapai, F., Scuderi, S. A., Benedetto, F., Esposito, E., & Capra, A. P. (2024). The Impact of COVID-19 on Amputation and Mortality Rates in Patients with Acute Limb Ischemia: A Systematic Review and Meta-Analysis. Diseases, 12(4), 74. https://doi.org/10.3390/diseases12040074