
Efficacy and Safety of Plasma Rich in Growth Factor in Patients with Congenital Aniridia and Dry Eye Disease

 , , ,
, , ,  , , and
, , and
Abstract
1. Introduction
2. Material and Methods
2.1. Patients
2.2. Treatment
PRGF Preparation
2.3. Clinical Tests
2.3.1. Ocular Surface Symptom Assessment
2.3.2. Visual Acuity
2.3.3. Ocular Redness
2.3.4. Fluorescein Staining
2.3.5. Presence and Level of AAK
2.3.6. Stability of the Tear Film
2.3.7. Tear Volume
2.3.8. Meibography
2.3.9. Impression Cytology
2.3.10. Statistical Analysis
3. Results
3.1. General Condition at Baseline
3.2. Clinical Test Results after Treatment
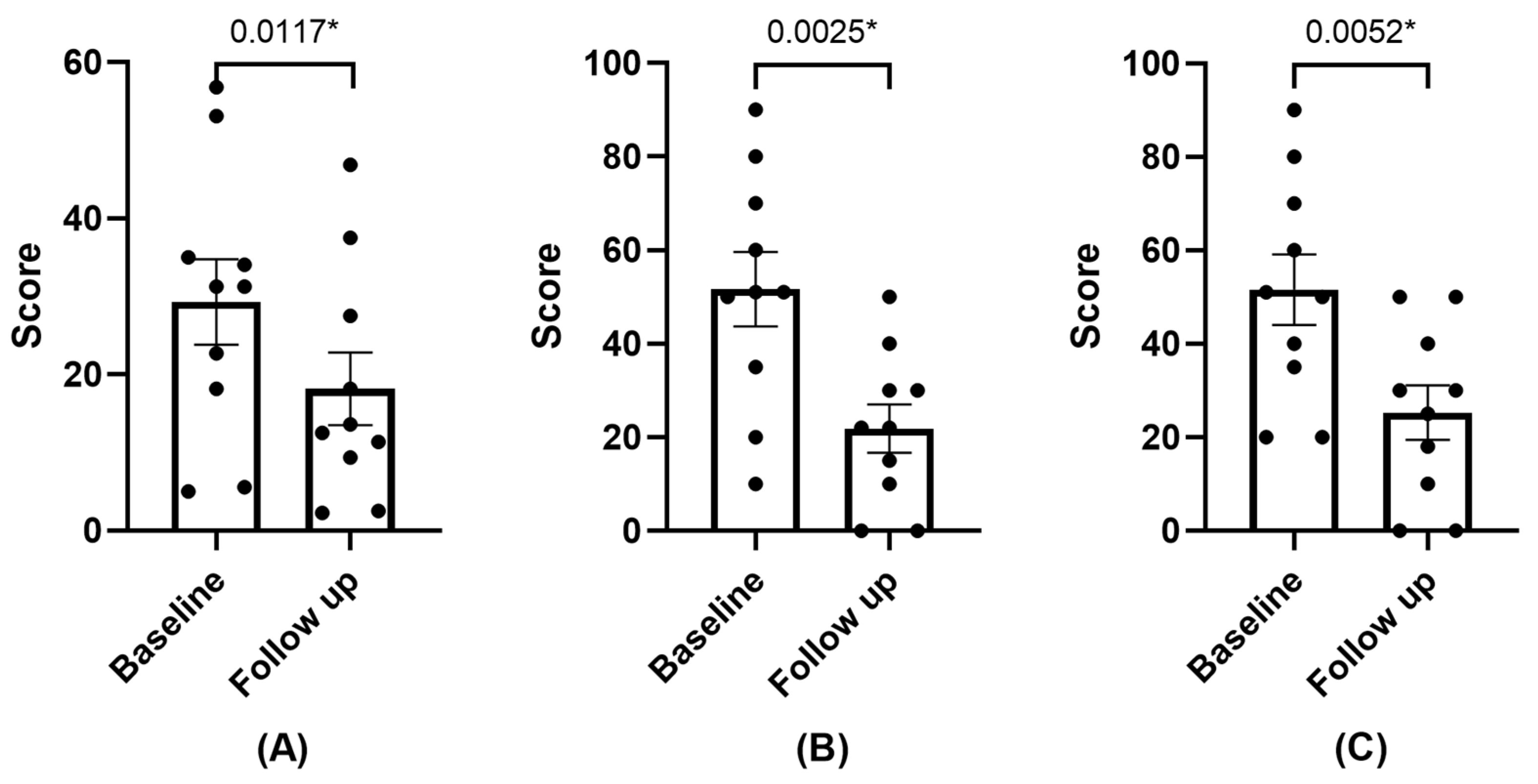
3.2.1. Symptomatology
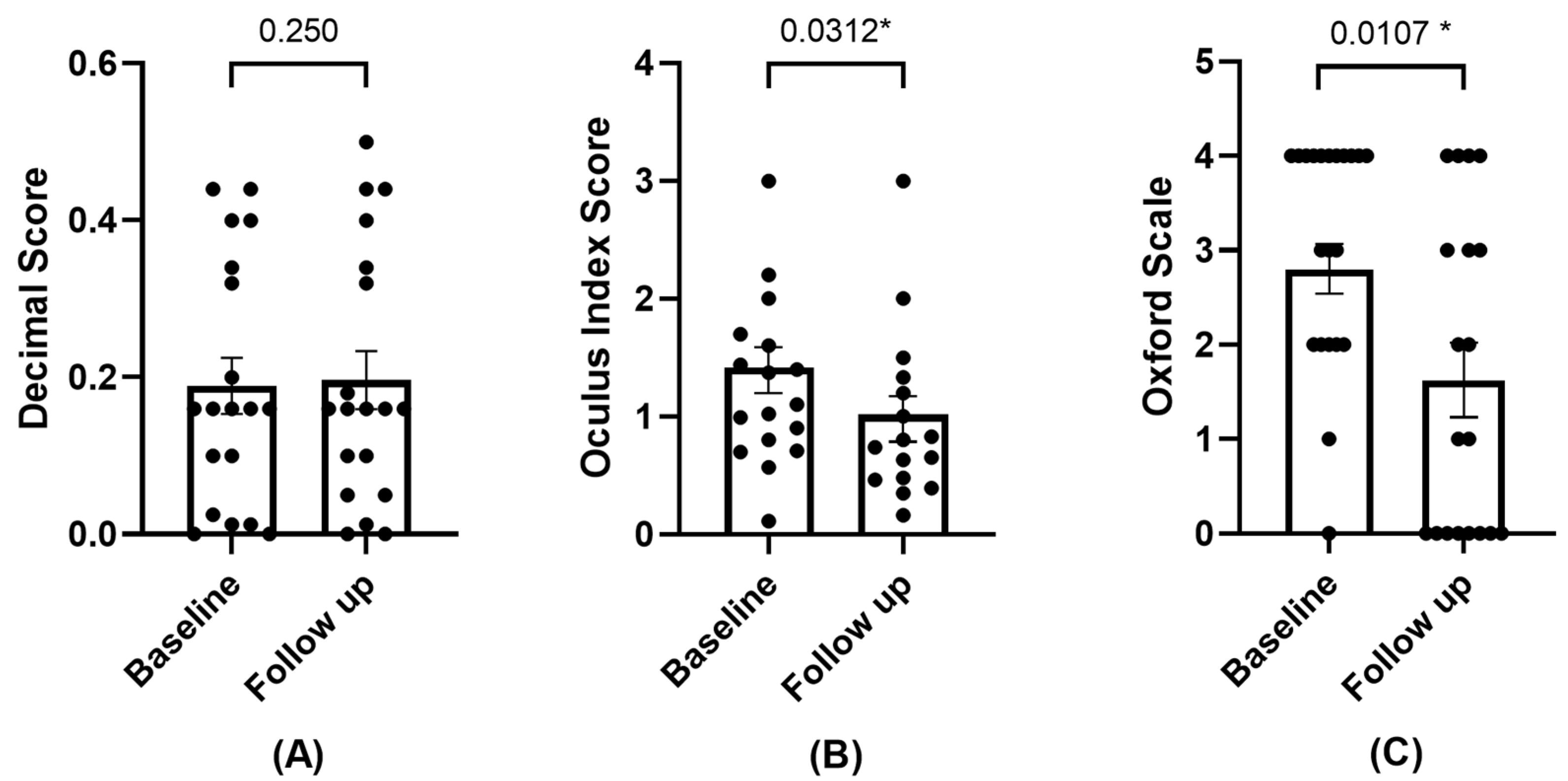
3.2.2. BCVA, Ocular Redness, and Damage
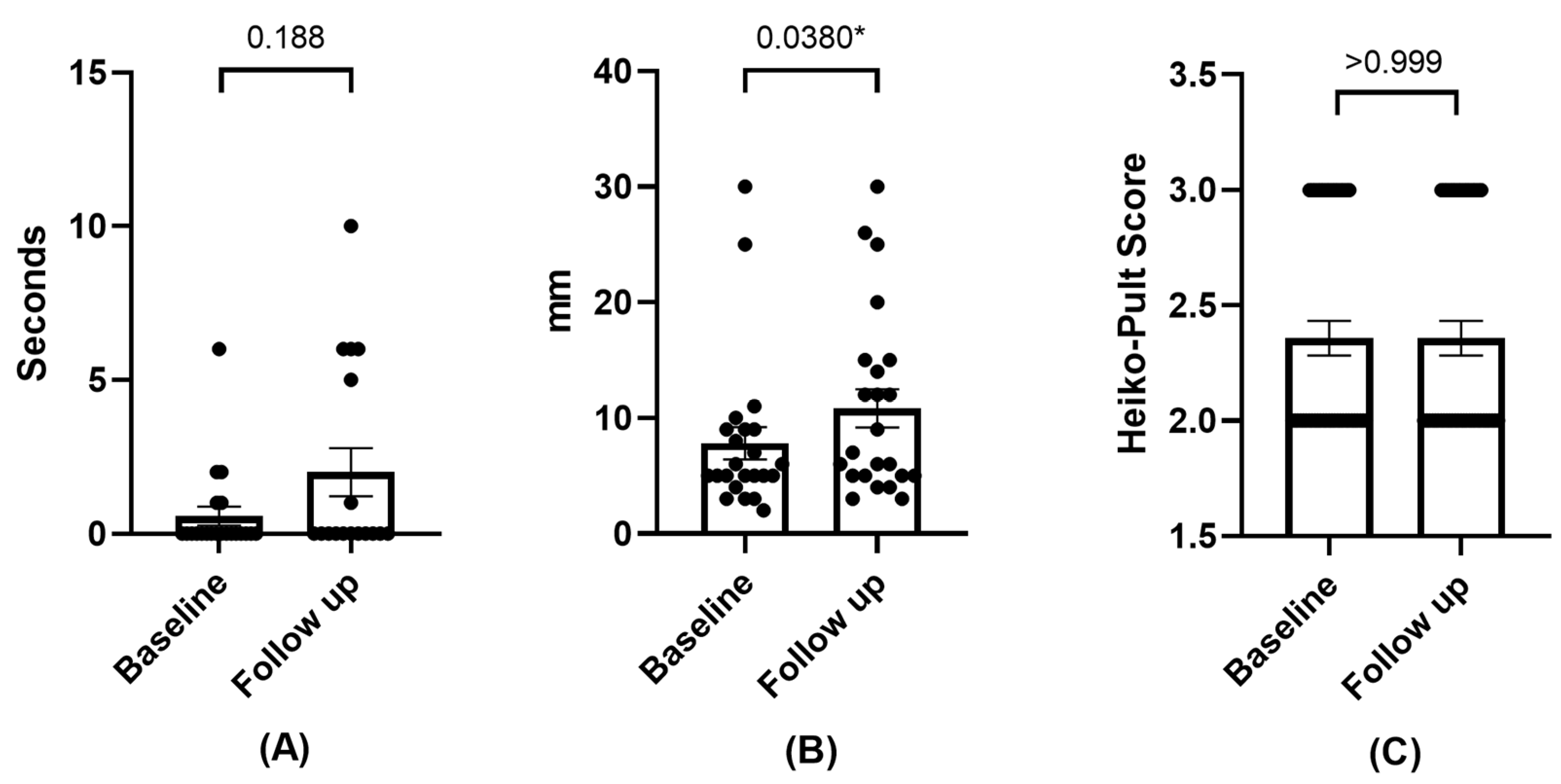
3.2.3. Effects on Tear Film
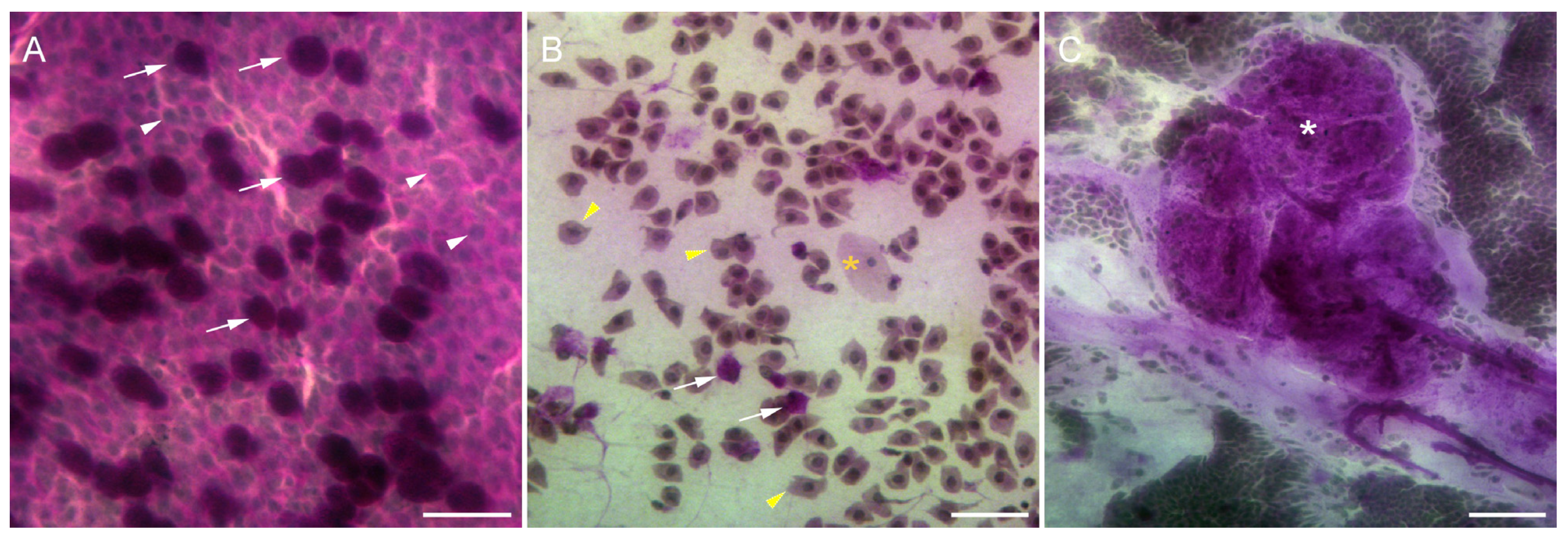
3.2.4. Impression Cytology
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Moosajee, M.; Hingorani, M.; Moore, A.T. PAX6-Related Aniridia; University of Washington, Seattle: Seattle, WA, USA, 1993. [Google Scholar]
- Landsend, E.C.S.; Pedersen, H.R.; Utheim, Ø.A.; Xiao, J.; Adil, M.Y.; Tashbayev, B.; Lagali, N.; Dartt, D.A.; Baraas, R.C.; Utheim, T.P. Meibomian Gland Dysfunction and Keratopathy Are Associated with Dry Eye Disease in Aniridia. Br. J. Ophthalmol. 2019, 103, 119–124. [Google Scholar] [CrossRef] [PubMed]
- López-García, J.S.; García-Lozano, I.; Rivas, L.; Martínez-Garchitorena, J. Manejo Terapéutico de La Queratopatía Asociada a Aniridia Congénita. Arch. Soc. Esp. Oftalmol. 2006, 81, 435–444. [Google Scholar] [CrossRef] [PubMed]
- Orphanet. Available online: https://www.orpha.net/consor4.01/www/cgi-bin/Disease_Search.php?lng=ES&data_id=19593&Disease_Disease_Search_diseaseGroup=aniridia&Disease_Disease_Search_diseaseType=Pat&Enfermedad(es)/grupo%20de%20enfermedades=Aniridia-aislada&title=Aniridia%20aislada&search=Disease_Search_Simple (accessed on 1 February 2024).
- Hingorani, M.; Williamson, K.A.; Moore, A.T.; van Heyningen, V. Detailed Ophthalmologic Evaluation of 43 Individuals with PAX6 Mutations. Investig. Opthalmology Vis. Sci. 2009, 50, 2581. [Google Scholar] [CrossRef] [PubMed]
- Edén, U.; Iggman, D.; Riise, R.; Tornqvist, K. Epidemiology of Aniridia in Sweden and Norway. Acta Ophthalmol. 2008, 86, 727–729. [Google Scholar] [CrossRef] [PubMed]
- Holland, E.J.; Djalilian, A.R.; Schwartz, G.S. Management of Aniridic Keratopathy with Keratolimbal Allograft: A Limbal Stem Cell Transplantation Technique. Ophthalmology 2003, 110, 125–130. [Google Scholar] [CrossRef]
- Tan, D.T.H.; Ficker, L.A.; Buckley, R.J. Limbal Transplantation. Ophthalmology 1996, 103, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Landsend, E.C.S.; Lagali, N.; Utheim, T.P. Congenital Aniridia—A Comprehensive Review of Clinical Features and Therapeutic Approaches. Surv. Ophthalmol. 2021, 66, 1031–1050. [Google Scholar] [CrossRef]
- Ihnatko, R.; Eden, U.; Fagerholm, P.; Lagali, N. Congenital Aniridia and the Ocular Surface. Ocul. Surf. 2016, 14, 196–206. [Google Scholar] [CrossRef] [PubMed]
- Samant, M.; Chauhan, B.K.; Lathrop, K.L.; Nischal, K.K. Congenital Aniridia: Etiology, Manifestations and Management. Expert Rev. Ophthalmol. 2016, 11, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Ralph, R.A.; Doane, M.G.; Dohlman, C.H. Clinical Experience with a Mobile Ocular Perfusion Pump. Arch. Ophthalmol. 1975, 93, 1039–1043. [Google Scholar] [CrossRef]
- López-García, J.S.; Rivas, L.; García-Lozano, I.; Murube, J. Autologous Serum Eyedrops in the Treatment of Aniridic Keratopathy. Ophthalmology 2008, 115, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Anitua, E.; Muruzabal, F.; Tayebba, A.; Riestra, A.; Perez, V.L.; Merayo-Lloves, J.; Orive, G. Autologous Serum and Plasma Rich in Growth Factors in Ophthalmology: Preclinical and Clinical Studies. Acta Ophthalmol. 2015, 93, e605–e614. [Google Scholar] [CrossRef] [PubMed]
- Anitua, E.; Muruzabal, F.; De la Fuente, M.; Merayo-Lloves, J.; Orive, G. Effects of Heat-Treatment on Plasma Rich in Growth Factors-Derived Autologous Eye Drop. Exp. Eye Res. 2014, 119, 27–34. [Google Scholar] [CrossRef]
- Anitua, E.; Sanchez, M.; Merayo-Lloves, J.; De la Fuente, M.; Muruzabal, F.; Orive, G. Plasma Rich in Growth Factors (PRGF-Endoret) Stimulates Proliferation and Migration of Primary Keratocytes and Conjunctival Fibroblasts and Inhibits and Reverts TGF-Β1–Induced Myodifferentiation. Investig. Opthalmology Vis. Sci. 2011, 52, 6066. [Google Scholar] [CrossRef] [PubMed]
- Yoon, K.-C.; Jeong, I.-Y.; Park, Y.-G.; Yang, S.-Y. Interleukin-6 and Tumor Necrosis Factor-α Levels in Tears of Patients With Dry Eye Syndrome. Cornea 2007, 26, 431–437. [Google Scholar] [CrossRef]
- Pflugfelder, S.C.; Jones, D.; Ji, Z.; Afonso, A.; Monroy, D. Altered Cytokine Balance in the Tear Fluid and Conjunctiva of Patients with Sjogren’s Syndrome Keratoconjunctivitis Sicca. Curr. Eye Res. 1999, 19, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Landsend, E.C.S.; Utheim, Ø.A.; Pedersen, H.R.; Aass, H.C.D.; Lagali, N.; Dartt, D.A.; Baraas, R.C.; Utheim, T.P. The Level of Inflammatory Tear Cytokines Is Elevated in Congenital Aniridia and Associated with Meibomian Gland Dysfunction. Investig. Opthalmology Vis. Sci. 2018, 59, 2197–2204. [Google Scholar] [CrossRef]
- Ogino, Y.; Ayukawa, Y.; Tsukiyama, Y.; Koyano, K. The Effect of Platelet-Rich Plasma on the Cellular Response of Rat Bone Marrow Cells in Vitro. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2005, 100, 302–307. [Google Scholar] [CrossRef]
- López-Plandolit, S.; Morales, M.C.; Freire, V.; Grau, A.E.; Durán, J.A. Efficacy of Plasma Rich in Growth Factors for the Treatment of Dry Eye. Cornea 2011, 30, 1312–1317. [Google Scholar] [CrossRef] [PubMed]
- Barros, A.; Lozano-Sanroma, J.; Queiruga-Piñeiro, J.; Fernández-Vega Cueto, L.; Anitua, E.; Alcalde, I.; Merayo-Lloves, J. Recovery of Corneal Innervation after Treatment in Dry Eye Disease: A Confocal Microscopy Study. J. Clin. Med. 2023, 12, 1841. [Google Scholar] [CrossRef]
- Sanchez-Avila, R.M.; Merayo-Lloves, J.; Riestra, A.C.; Anitua, E.; Muruzabal, F.; Orive, G.; Fernández-Vega, L. The Effect of Immunologically Safe Plasma Rich in Growth Factor Eye Drops in Patients with Sjögren Syndrome. J. Ocul. Pharmacol. Ther. 2017, 33, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Avila, R.M.; Merayo-Lloves, J.; Muruzabal, F.; Orive, G.; Anitua, E. Plasma Rich in Growth Factors for the Treatment of Dry Eye from Patients with Graft versus Host Diseases. Eur. J. Ophthalmol. 2020, 30, 94–103. [Google Scholar] [CrossRef] [PubMed]
- Lozano-Sanroma, J.; Barros, A.; Alcalde, I.; Sánchez-Ávila, R.M.; Queiruga-Piñeiro, J.; Fernández-Vega Cueto, L.; Merayo-Lloves, J. Impact of Plasma Rich in Growth Factors (PRGF) Eye Drops on Ocular Redness and Symptomatology in Patients with Dry Eye Disease. Medicina 2023, 59, 928. [Google Scholar] [CrossRef]
- Merayo-Lloves, J.; Sanchez-Avila, R.M.; Riestra, A.C.; Anitua, E.; Begoña, L.; Orive, G.; Fernandez-Vega, L. Safety and Efficacy of Autologous Plasma Rich in Growth Factors Eye Drops for the Treatment of Evaporative Dry Eye. Ophthalmic Res. 2016, 56, 68–73. [Google Scholar] [CrossRef]
- Shiple, D.; Finklea, B.; Lauderdale, J.D.; Netland, P.A. Keratopathy, Cataract, and Dry Eye in a Survey of Aniridia Subjects. Clin. Ophthalmol. 2015, 9, 291–295. [Google Scholar] [CrossRef]
- Anitua, E.; de la Fuente, M.; Muruzabal, F.; Riestra, A.; Merayo-Lloves, J.; Orive, G. Plasma Rich in Growth Factors (PRGF) Eye Drops Stimulates Scarless Regeneration Compared to Autologous Serum in the Ocular Surface Stromal Fibroblasts. Exp. Eye Res. 2015, 135, 118–126. [Google Scholar] [CrossRef]
- Özcura, F.; Aydin, S.; Helvaci, M.R. Ocular Surface Disease Index for the Diagnosis of Dry Eye Syndrome. Ocul. Immunol. Inflamm. 2007, 15, 389–393. [Google Scholar] [CrossRef] [PubMed]
- Schaumberg, D.A.; Gulati, A.; Mathers, W.D.; Clinch, T.; Lemp, M.A.; Nelson, J.D.; Foulks, G.N.; Dana, R. Development and Validation of a Short Global Dry Eye Symptom Index. Ocul. Surf. 2007, 5, 50–57. [Google Scholar] [CrossRef]
- Jerchel, N.N.; Sickenberger, W.; Schulze, M.M. Objective Classification and Documentation of Bulbar Redness Using a Corneal Topographer. Contact Lens Anterior Eye 2012, 35, e18. [Google Scholar] [CrossRef]
- Fieguth, P.; Simpson, T. Automated Measurement of Bulbar Redness. Investig. Opthalmology Vis. Sci. 2002, 43, 340–347. [Google Scholar]
- Amparo, F.; Wang, H.; Emami-Naeini, P.; Karimian, P.; Dana, R. The Ocular Redness Index: A Novel Automated Method for Measuring Ocular Injection. Investig. Opthalmology Vis. Sci. 2013, 54, 4821–4826. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Hong, J.; Tian, L.; Cui, X.; Sun, X.; Xu, J. Assessment of Bulbar Redness with a Newly Developed Keratograph. Optom. Vis. Sci. 2015, 92, 892–899. [Google Scholar] [CrossRef]
- Lagali, N.; Wowra, B.; Fries, F.N.; Latta, L.; Moslemani, K.; Utheim, T.P.; Wylegala, E.; Seitz, B.; Käsmann-Kellner, B. PAX6 Mutational Status Determines Aniridia-Associated Keratopathy Phenotype. Ophthalmology 2020, 127, 273–275. [Google Scholar] [CrossRef]
- Tsubota, K.; Pflugfelder, S.C.; Liu, Z.; Baudouin, C.; Kim, H.M.; Messmer, E.M.; Kruse, F.; Liang, L.; Carreno-Galeano, J.T.; Rolando, M.; et al. Defining Dry Eye from a Clinical Perspective. Int. J. Mol. Sci. 2020, 21, 9271. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Deng, X.G.; He, M.F. Comparison of the Schirmer I Test with and without Topical Anesthesia for Diagnosing Dry Eye. Int. J. Ophthalmol. 2012, 5, 478–481. [Google Scholar] [CrossRef] [PubMed]
- Tsubota, K.; Kaido, M.; Yagi, Y.; Fujihara, T.; Shimmura, S. Diseases Associated with Ocular Surface Abnormalities: The Importance of Reflex Tearing. Br. J. Ophthalmol. 1999, 83, 89–91. [Google Scholar] [CrossRef] [PubMed]
- Nelson, J.D. Impression Cytology. Cornea 1988, 7, 71–81. [Google Scholar] [CrossRef]
- Quartieri, E.; Marraccini, C.; Merolle, L.; Pulcini, S.; Buzzi, M.; Guardi, M.; Schiroli, D.; Baricchi, R.; Pertinhez, T.A. Metabolomics Comparison of Cord and Peripheral Blood-Derived Serum Eye Drops for the Treatment of Dry Eye Disease. Transfus. Apher. Sci. 2021, 60, 103155. [Google Scholar] [CrossRef] [PubMed]
- Yoon, K.-C.; Im, S.-K.; Park, Y.-G.; Jung, Y.-D.; Yang, S.-Y.; Choi, J. Application of Umbilical Cord Serum Eyedrops for the Treatment of Dry Eye Syndrome. Cornea 2006, 25, 268–272. [Google Scholar] [CrossRef] [PubMed]
- Galbis-Estrada, C.; Martinez-Castillo, S.; Morales, J.M.; Vivar-Llopis, B.; Monleón, D.; Díaz-Llopis, M.; Pinazo-Durán, M.D. Differential Effects of Dry Eye Disorders on Metabolomic Profile by 1H Nuclear Magnetic Resonance Spectroscopy. BioMed Res. Int. 2014, 2014, 542549. [Google Scholar] [CrossRef]
- Yazdani, M.; Elgstøen, K.B.P.; Rootwelt, H.; Shahdadfar, A.; Utheim, Ø.A.; Utheim, T.P. Tear Metabolomics in Dry Eye Disease: A Review. Int. J. Mol. Sci. 2019, 20, 3755. [Google Scholar] [CrossRef] [PubMed]
- Giannaccare, G.; Versura, P.; Buzzi, M.; Primavera, L.; Pellegrini, M.; Campos, E.C. Blood Derived Eye Drops for the Treatment of Cornea and Ocular Surface Diseases. Transfus. Apher. Sci. 2017, 56, 595–604. [Google Scholar] [CrossRef] [PubMed]
- Pan, Q.; Angelina, A.; Marrone, M.; Stark, W.J.; Akpek, E.K. Autologous Serum Eye Drops for Dry Eye. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef]
- Tsubota, K.; Goto, E.; Shimmura, S.; Shimazaki, J. Treatment of Persistent Corneal Epithelial Defect by Autologous Serum Application. Ophthalmology 1999, 106, 1984–1989. [Google Scholar] [CrossRef] [PubMed]
- Yoon, K.C.; Heo, H.; Im, S.K.; You, I.C.; Kim, Y.H.; Park, Y.G. Comparison of Autologous Serum and Umbilical Cord Serum Eye Drops for Dry Eye Syndrome. Am. J. Ophthalmol. 2007, 144, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Informe de La Agencia Española de Medicamentos y Productos Sanitarios Sobre El Uso de Plasma Rico En Plaquetas. Available online: https://www.aemps.gob.es/medicamentosUsoHumano/medSituacionesEspeciales/docs/PRP-AEMPS-DEF-mayo13.pdf (accessed on 10 April 2024).
- Oudelaar, B.W.; Peerbooms, J.C.; Huis in ‘t Veld, R.; Vochteloo, A.J.H. Concentrations of Blood Components in Commercial Platelet-Rich Plasma Separation Systems: A Review of the Literature. Am. J. Sports Med. 2019, 47, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Zallio, F.; Mazzucco, L.; Monaco, F.; Astori, M.R.; Passera, R.; Drago, G.; Tamiazzo, S.; Rapetti, M.; Dolcino, D.; Guaschino, R.; et al. A Single-Center Pilot Prospective Study of Topical Application of Platelet-Derived Eye Drops for Patients with Ocular Chronic Graft-versus-Host Disease. Biol. Blood Marrow Transplant. 2016, 22, 1664–1670. [Google Scholar] [CrossRef] [PubMed]
- Alio, J.L.; Colecha, J.R.; Pastor, S.; Rodriguez, A.; Artola, A. Symptomatic Dry Eye Treatment with Autologous Platelet-Rich Plasma. Ophthalmic Res. 2007, 39, 124–129. [Google Scholar] [CrossRef]
- Ribeiro, M.V.M.R.; Melo, V.F.D.; Barbosa, M.E.F.C.; Tozzi, M.U.D.F.; Ramos, M.S.B.; Gaia, N.M.S.R.S.; Santos, V.M.G.; Neri, W.D.O.; Barbosa, F.T.; Ribeiro, Ê.A.N. The Use of Platelet Rich-Plasma in Ophthalmology: A Literature Review. Rev. Bras. Oftalmol. 2017, 76, 319–324. [Google Scholar] [CrossRef]
- García-Conca, V.; Abad-Collado, M.; Hueso-Abancens, J.R.; Mengual-Verdú, E.; Piñero, D.P.; Aguirre-Balsalobre, F.; Molina, J.C. Efficacy and Safety of Treatment of Hyposecretory Dry Eye with Platelet-Rich Plasma. Acta Ophthalmol. 2019, 97, e170–e178. [Google Scholar] [CrossRef] [PubMed]
- López-Plandolit, S.; Morales, M.C.; Freire, V.; Etxebarría, J.; Durán, J.A. Plasma Rich in Growth Factors as a Therapeutic Agent for Persistent Corneal Epithelial Defects. Cornea 2010, 29, 843–848. [Google Scholar] [CrossRef]
- Merayo-Lloves, J.; Sanchez, R.M.; Riestra, A.C.; Anitua, E.; Begoña, L.; Orive, G.; Fernandez-Vega, L. Autologous Plasma Rich in Growth Factors Eyedrops in Refractory Cases of Ocular Surface Disorders. Ophthalmic Res. 2016, 55, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Freire, V.; Andollo, N.; Etxebarria, J.; Durán, J.A.; Morales, M.C. In Vitro Effects of Three Blood Derivatives on Human Corneal Epithelial Cells. Investig. Opthalmology Vis. Sci. 2012, 53, 5571–5578. [Google Scholar] [CrossRef] [PubMed]
- Wróbel-Dudzińska, D.; Przekora, A.; Kazimierczak, P.; Ćwiklińska-Haszcz, A.; Kosior-Jarecka, E.; Żarnowski, T. The Comparison between the Composition of 100% Autologous Serum and 100% Platelet-Rich Plasma Eye Drops and Their Impact on the Treatment Effectiveness of Dry Eye Disease in Primary Sjogren Syndrome. J Clin Med 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Comparison of the Healing Properties on Corneal Cells of Growth Factor-Enriched Plasma and Autologous Serum From Aniridia Patients (CICASAND). Available online: https://clinicaltrials.gov/study/NCT05400590?cond=Congenital%20Aniridia&page=1&rank=2 (accessed on 16 August 2023).
- Schiffman, R.M.; Christianson, M.D.; Jacobsen, G.; Hirsch, J.D.; Reis, B.L. Reliability and Validity of the Ocular Surface Disease Index. Arch. Ophthalmol. 2000, 118, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.L.; Walt, J.G.; Mink, D.R.; Satram-Hoang, S.; Wilson, S.E.; Perry, H.D.; Asbell, P.A.; Pflugfelder, S.C. Minimal Clinically Important Difference for the Ocular Surface Disease Index. Arch. Ophthalmol. 2010, 128, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Bahreini, M.; Safaie, A.; Mirfazaelian, H.; Jalili, M. How Much Change in Pain Score Does Really Matter to Patients? Am. J. Emerg. Med. 2020, 38, 1641–1646. [Google Scholar] [CrossRef]
- Todd, K.H. Clinical Versus Statistical Significance in the Assessment of Pain Relief. Ann. Emerg. Med. 1996, 27, 439–441. [Google Scholar] [CrossRef]
- Barabino, S.; Chen, Y.; Chauhan, S.; Dana, R. Ocular Surface Immunity: Homeostatic Mechanisms and Their Disruption in Dry Eye Disease. Prog. Retin. Eye Res. 2012, 31, 271–285. [Google Scholar] [CrossRef] [PubMed]
- Papas, E.B. Key Factors in the Subjective and Objective Assessment of Conjunctival Erythema. Investig. Opthalmology Vis. Sci. 2000, 41, 687–691. [Google Scholar]
- Anitua, E.; de la Fuente, M.; Merayo-Lloves, J.; Muruzabal, F. Optimization of a Plasma Rich in Growth Factors Membrane for the Treatment of Inflammatory Ocular Diseases. Bioengineering 2022, 9, 508. [Google Scholar] [CrossRef]
- Haller-Schober, E.-M.; Schwantzer, G.; Berghold, A.; Fischl, M.; Theisl, A.; Horwath-Winter, J. Evaluating an Impression Cytology Grading System (IC Score) in Patients with Dry Eye Syndrome. Eye 2006, 20, 927–933. [Google Scholar] [CrossRef] [PubMed]
- Lemp, M.A.; Hamill, J.R. Factors Affecting Tear Film Breakup in Normal Eyes. Arch. Ophthalmol. 1973, 89, 103–105. [Google Scholar] [CrossRef] [PubMed]
- Wolffsohn, J.S.; Travé Huarte, S.; Jones, L.; Craig, J.P.; Wang, M.T.M. Clinical Practice Patterns in the Management of Dry Eye Disease: A TFOS International Survey. Ocul. Surf. 2021, 21, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Craig, J.P.; Nichols, K.K.; Akpek, E.K.; Caffery, B.; Dua, H.S.; Joo, C.-K.; Liu, Z.; Nelson, J.D.; Nichols, J.J.; Tsubota, K.; et al. TFOS DEWS II Definition and Classification Report. Ocul. Surf. 2017, 15, 276–283. [Google Scholar] [CrossRef] [PubMed]
- van Setten, G.B.; Baudouin, C.; Horwath-Winter, J.; Böhringer, D.; Stachs, O.; Toker, E.; Al-Zaaidi, S.; Benitez-Del-castillo, J.M.; Beck, R.; Al-Sheikh, O.; et al. The Hylan m Study: Efficacy of 0.15% High Molecular Weight Hyaluronan Fluid in the Treatment of Severe Dry Eye Disease in a Multicenter Randomized Trial. J. Clin. Med. 2020, 9, 3536. [Google Scholar] [CrossRef] [PubMed]
- Pisella, P.J. Prevalence of Ocular Symptoms and Signs with Preserved and Preservative Free Glaucoma Medication. Br. J. Ophthalmol. 2002, 86, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Jaenen, N.; Baudouin, C.; Pouliquen, P.; Manni, G.; Figueiredo, A.; Zeyen, T. Ocular Symptoms and Signs with Preserved and Preservative-Free Glaucoma Medications. Eur. J. Ophthalmol. 2007, 17, 341–349. [Google Scholar] [CrossRef]
- Asiedu, K.; Abu, S.L. The Impact of Topical Intraocular Pressure Lowering Medications on the Ocular Surface of Glaucoma Patients: A Review. J. Curr. Ophthalmol. 2019, 31, 8–15. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AAK | Cataract | Glaucoma | Nystagmus | Photophobia | Transplant | Dryness | AS |
|---|---|---|---|---|---|---|---|
| 23 (100%) | 18 (78.3%) | 10 (43.5%) | 13 (56.5%) | 11 (47.8%) | 4 (17.4%) | 23 (100%) | 9 (39.1%) |
| AAK | N (RE:LE) | Cataract | Glaucoma | Nystagmus | Photophobia | Transplant | Dryness | AS |
|---|---|---|---|---|---|---|---|---|
| 1 | 4:3 | 6 (85.7%) | 5 (71.4%) | 5 (71.4%) | 2 (28.6%) | 0 (0%) | 7 (100%) | 2 (28.6%) |
| 2 | 1:4 | 5 (100%) | 5 (100%) | 3 (60%) | 2 (40%) | 0 (0%) | 5 (100%) | 2 (40%) |
| 3 | 5:0 | 4 (80%) | 3 (60%) | 1 (20%) | 5 (100%) | 1 (20%) | 5 (100%) | 2 (40%) |
| 4 | 2:4 | 3 (50%) | 2 (33.3%) | 4 (66.7%) | 2 (33.33%) | 3 (50%) | 6 (100%) | 3 (50%) |
| Baseline | Follow-Up | p-Value | |
|---|---|---|---|
| OSDI (score) | 30.54 ± 5.98 | 18.17 ± 5.22 | 0.01 * |
| SANDE Frequency (score) | 51.88 ± 10.09 | 21.88 ± 18.50 | 0.003 * |
| SANDE Severity (score) | 51.88 ± 9.54 | 23.13 ± 6.47 | 0.005 * |
| BCVA (decimal) | 0.19 ± 0.04 | 0.20 ± 0.04 | 0.25 |
| Ocular Redness Index | 1.47 ± 0.29 | 0.93 ± 0.31 | 0.03 * |
| Corneal Fluo Staining (Oxford) | 2.82 ± 0.30 | 1.82 ± 0.40 | 0.01 * |
| FBUT (s) | 0.73 ± 0.42 | 2.27 ± 0.86 | 0.19 |
| Schirmer (mm) | 7.83 ± 1.40 | 10.83 ± 1.65 | 0.04 * |
| Superior Meibography (score) | 2.37 ± 0.11 | 2.42 ± 0.12 | >0.99 |
| Inferior Meibography (score) | 2.40 ± 0.11 | 2.35 ± 0.11 | >0.99 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lozano-Sanroma, J.; Barros, A.; Alcalde, I.; Alvarado-Villacorta, R.; Sánchez-Ávila, R.M.; Queiruga-Piñeiro, J.; Cueto, L.F.-V.; Anitua, E.; Merayo-Lloves, J. Efficacy and Safety of Plasma Rich in Growth Factor in Patients with Congenital Aniridia and Dry Eye Disease. Diseases 2024, 12, 76. https://doi.org/10.3390/diseases12040076
Lozano-Sanroma J, Barros A, Alcalde I, Alvarado-Villacorta R, Sánchez-Ávila RM, Queiruga-Piñeiro J, Cueto LF-V, Anitua E, Merayo-Lloves J. Efficacy and Safety of Plasma Rich in Growth Factor in Patients with Congenital Aniridia and Dry Eye Disease. Diseases. 2024; 12(4):76. https://doi.org/10.3390/diseases12040076
Chicago/Turabian StyleLozano-Sanroma, Javier, Alberto Barros, Ignacio Alcalde, Rosa Alvarado-Villacorta, Ronald M. Sánchez-Ávila, Juan Queiruga-Piñeiro, Luis Fernández-Vega Cueto, Eduardo Anitua, and Jesús Merayo-Lloves. 2024. "Efficacy and Safety of Plasma Rich in Growth Factor in Patients with Congenital Aniridia and Dry Eye Disease" Diseases 12, no. 4: 76. https://doi.org/10.3390/diseases12040076
APA StyleLozano-Sanroma, J., Barros, A., Alcalde, I., Alvarado-Villacorta, R., Sánchez-Ávila, R. M., Queiruga-Piñeiro, J., Cueto, L. F.-V., Anitua, E., & Merayo-Lloves, J. (2024). Efficacy and Safety of Plasma Rich in Growth Factor in Patients with Congenital Aniridia and Dry Eye Disease. Diseases, 12(4), 76. https://doi.org/10.3390/diseases12040076