
The Association between Marital Status and Obesity: A Systematic Review and Meta-Analysis

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Methods
2.2. Selection Criteria
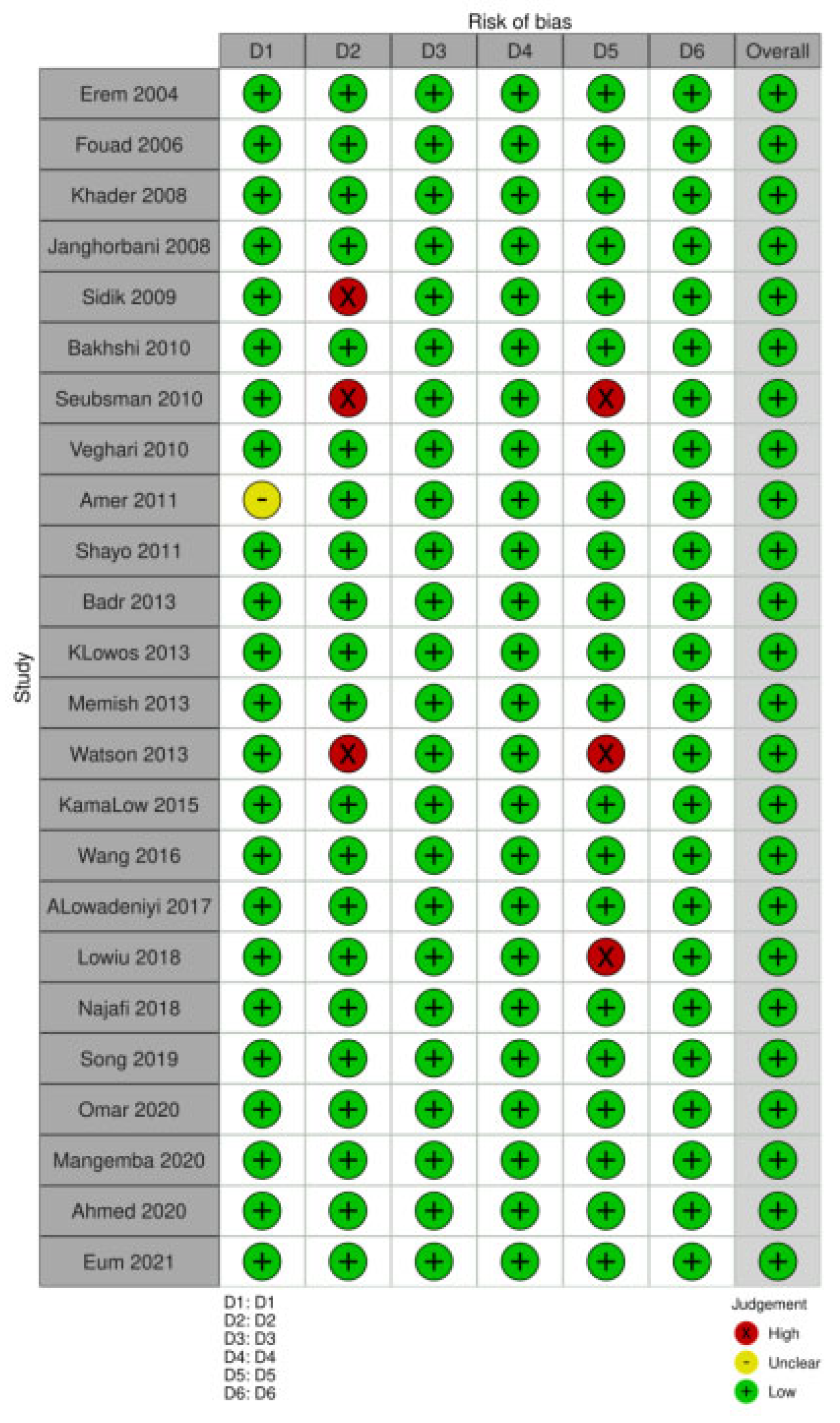
2.3. Data Extraction and Quality Assessment
2.4. Data Synthesis and Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- WHO. Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation on Obesity, Geneva, 3–5 June 1997; WHO: Geneva, Switzerland, 1998. [Google Scholar]
- Hjartåker, A.; Langseth, H.; Weiderpass, E. Obesity and diabetes epidemics: Cancer repercussions. Adv. Exp. Med. Biol. 2008, 630, 72–93. [Google Scholar] [CrossRef]
- World Health Organization. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 26 June 2023).
- Aizer, A.A.; Chen, M.-H.; McCarthy, E.P.; Mendu, M.L.; Koo, S.; Wilhite, T.J.; Graham, P.L.; Choueiri, T.K.; Hoffman, K.E.; Martin, N.E.; et al. Marital Status and Survival in Patients with Cancer. J. Clin. Oncol. 2013, 31, 3869–3876. [Google Scholar] [CrossRef] [PubMed]
- Krajc, K.; Miroševič, Š.; Sajovic, J.; Ketiš, Z.K.; Spiegel, D.; Drevenšek, G.; Drevenšek, M. Marital status and survival in cancer patients: A systematic review and meta-analysis. Cancer Med. 2022, 12, 1685–1708. [Google Scholar] [CrossRef]
- Wong, C.W.; Kwok, C.S.; Narain, A.; Gulati, M.; Mihalidou, A.S.; Wu, P.; Alasnag, M.; Myint, P.K.; A Mamas, M. Marital status and risk of cardiovascular diseases: A systematic review and meta-analysis. Heart 2018, 104, 1937–1948. [Google Scholar] [CrossRef]
- Sommerlad, A.; Ruegger, J.; Singh-Manoux, A.; Lewis, G.; Livingston, G. Research paper: Marriage and risk of dementia: Systematic review and meta-analysis of observational studies. J. Neurol. Neurosurg. Psychiatry 2018, 89, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Jiao, Y.; Nie, J.; O’neil, A.; Huang, W.; Zhang, L.; Han, J.; Liu, H.; Zhu, Y.; Yu, C.; et al. Sex differences in the association between marital status and the risk of cardiovascular, cancer, and all-cause mortality: A systematic review and meta-analysis of 7,881,040 individuals. Glob. Health Res. Policy 2020, 5, 1–16. [Google Scholar] [CrossRef]
- Dinour, L.; Leung, M.M.; Tripicchio, G.; Khan, S.; Yeh, M.-C. The Association between Marital Transitions, Body Mass Index, and Weight: A Review of the Literature. J. Obes. 2012, 2012, 1–16. [Google Scholar] [CrossRef] [PubMed]
- WHO Expert Consultation Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004, 363, 157–163. [CrossRef]
- Aballay, L.R.; Osella, A.R.; Celi, A.; Díaz, M.d.P. Overweight and obesity: Prevalence and their association with some social characteristics in a random sample population-based study in Córdoba city, Argentina. Obes. Res. Clin. Pract. 2009, 3, 75–83. [Google Scholar] [CrossRef]
- Abdeen, Z.; Jildeh, C.; Dkeideek, S.; Qasrawi, R.; Ghannam, I.; Al Sabbah, H. Overweight and Obesity among Palestinian Adults: Analyses of the Anthropometric Data from the First National Health and Nutrition Survey (1999–2000). J. Obes. 2012, 2012, 1–12. [Google Scholar] [CrossRef]
- Addo, P.N.O.; Nyarko, K.M.; Sackey, S.O.; Akweongo, P.; Sarfo, B. Prevalence of obesity and overweight and associated factors among financial institution workers in Accra Metropolis, Ghana: A cross sectional study. BMC Res. Notes 2015, 8, 599. [Google Scholar] [CrossRef]
- Aladeniyi, I.; Adeniyi, O.V.; Fawole, O.; Adeolu, M.; Ter Goon, D.; Ajayi, A.I.; Owolabi, E.O. Pattern and correlates of obesity among public service workers in Ondo State, Nigeria: A cross-sectional study. South Afr. Fam. Pract. 2017, 59, 195–200. [Google Scholar] [CrossRef]
- Aldossari, K.K.; Shubair, M.M.; Al-Ghamdi, S.; Al-Zahrani, J.; AlAjmi, M.; Alshahrani, S.M.; Alsalamah, M.; Al-Khateeb, B.F.; Bahkali, S.; El-Metwally, A. The association between overweight/obesity and psychological distress: A population based cross-sectional study in Saudi Arabia. Saudi J. Biol. Sci. 2021, 28, 2783–2788. [Google Scholar] [CrossRef] [PubMed]
- Al-Ghamdi, S.; Shubair, M.M.; Aldiab, A.; Al-Zahrani, J.M.; Aldossari, K.K.; Househ, M.; Nooruddin, S.; Razzak, H.A.; El-Metwally, A. Prevalence of overweight and obesity based on the body mass index; a cross-sectional study in Alkharj, Saudi Arabia. Lipids Health Dis. 2018, 17, 1–8. [Google Scholar] [CrossRef]
- Al-Isa, A.N. Temporal Changes in Body Mass Index and Prevalence of Obesity among Kuwaiti Men. Ann. Nutr. Metab. 1997, 41, 307–314. [Google Scholar] [CrossRef]
- Amer, N.M.; Marcon, S.S.; Santana, R.G. Body mass index and hypertension in adult subjects in Brazil’s Midwest. Arq. Bras. Cardiol. 2011, 96, 47–53. [Google Scholar] [CrossRef]
- Aminde, L.N.; Atem, J.A.; Kengne, A.P.; Dzudie, A.; Veerman, J.L. Body mass index-measured adiposity and population attributability of associated factors: A population-based study from Buea, Cameroon. BMC Obes. 2017, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- de Andrade, F.B.; Junior, A.d.F.C.; Kitoko, P.M.; Batista, J.E.M.; de Andrade, T.B. Prevalence of overweight and obesity in elderly people from Vitória-ES, Brazil. Cienc. Saude Coletiva 2012, 17, 749–756. [Google Scholar] [CrossRef]
- Asahara, S.-I.; Miura, H.; Ogawa, W.; Tamori, Y. Sex difference in the association of obesity with personal or social background among urban residents in Japan. PLoS ONE 2020, 15, e0242105. [Google Scholar] [CrossRef]
- Asil, E.; Surucuoglu, M.S.; Cakiroglu, F.P.; Ucar, A.; Ozcelik, A.O.; Yilmaz, M.V.; Akan, L.S. Factors That Affect Body Mass Index of Adults. Pak. J. Nutr. 2014, 13, 255–260. [Google Scholar] [CrossRef]
- El Ati, J.; Traissac, P.; Delpeuch, F.; Aounallah-Skhiri, H.; Béji, C.; Eymard-Duvernay, S.; Bougatef, S.; Kolsteren, P.; Maire, B.; Ben Romdhane, H. Gender Obesity Inequities Are Huge but Differ Greatly According to Environment and Socio-Economics in a North African Setting: A National Cross-Sectional Study in Tunisia. PLoS ONE 2012, 7, e48153. [Google Scholar] [CrossRef]
- Badr, H.E.; Shah, N.M.; Shah, M.A. Obesity among Kuwaitis Aged 50 Years or Older: Prevalence, Correlates, and Comorbidities. Gerontologist 2012, 53, 555–566. [Google Scholar] [CrossRef] [PubMed]
- Baik, I. Forecasting obesity prevalence in Korean adults for the years 2020 and 2030 by the analysis of contributing factors. Nutr. Res. Pract. 2018, 12, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Bakhshi, E.; Mohammad, K.; Eshraghian, M.R.; Seifi, B. Factors related to obesity among Iranian men: Results from the National Health Survey. Public Health Nutr 2010, 13, 1389–1394. [Google Scholar] [CrossRef] [PubMed]
- Bakhshi, E.; Seifi, B.; Biglarian, A.; Mohammad, K. Changes in Body Mass Index across Age Groups in Iranian Women: Results from the National Health Survey. J. Nutr. Metab. 2012, 2012, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Barzin, M.; Piri, Z.; Serahati, S.; Valizadeh, M.; Azizi, F.; Hosseinpanah, F. Incidence of abdominal obesity and its risk factors among Tehranian adults. Public Health Nutr 2018, 21, 3111–3117. [Google Scholar] [CrossRef] [PubMed]
- Barzin, M.; Keihani, S.; Hosseinpanah, F.; Serahati, S.; Ghareh, S.; Azizi, F. Rising trends of obesity and abdominal obesity in 10 years of follow-up among Tehranian adults: Tehran Lipid and Glucose Study (TLGS). Public Health Nutr 2015, 18, 2981–2989. [Google Scholar] [CrossRef] [PubMed]
- Befort, C.A.; Nazir, N.; Perri, M.G. Prevalence of Obesity among Adults from Rural and Urban Areas of the United States: Findings from NHANES (2005–2008). J. Rural Health 2012, 28, 392–397. [Google Scholar] [CrossRef]
- Bell, C.N.; Thorpe, R.J. Income and Marital Status Interact on Obesity among Black and White Men. Am. J. Men’s Health 2019, 13, 1557988319829952. [Google Scholar] [CrossRef]
- Soares, D.A.; Barreto, S.M. Overweight and abdominal obesity in adults in a quilombo community in Bahia State, Brazil. Cad. Saude Publica 2014, 30, 341–354. [Google Scholar] [CrossRef]
- Black, J.L.; Macinko, J. The Changing Distribution and Determinants of Obesity in the Neighborhoods of New York City, 2003–2007. Am. J. Epidemiology 2010, 171, 765–775. [Google Scholar] [CrossRef] [PubMed]
- Coll, J.L.; Bibiloni, M.d.M.; Salas, R.; Pons, A.; Tur, J.A. Prevalence and Related Risk Factors of Overweight and Obesity among the Adult Population in the Balearic Islands, a Mediterranean Region. Obes. Facts 2015, 8, 220–233. [Google Scholar] [CrossRef] [PubMed]
- Correia, L.L.; da Silveira, D.M.I.; Cavalcante, A.; Campos, J.S.; Machado, M.M.T.; Rocha, H.A.L.; da Cunha, A.J.L.A.; Lindsay, A.C. Prevalence and determinants of obesity and overweight among reproductive age women living in the semi-arid region of Brazil. Cienc. Saude Coletiva 2011, 16, 133–145. [Google Scholar] [CrossRef] [PubMed]
- Dahly, D.L.; Gordon-Larsen, P.; Popkin, B.M.; Kaufman, J.S.; Adair, L.S. Associations between Multiple Indicators of Socioeconomic Status and Obesity in Young Adult Filipinos Vary by Gender, Urbanicity, and Indicator Used. J. Nutr. 2010, 140, 366–370. [Google Scholar] [CrossRef] [PubMed]
- de Moraes, S.A.; Humberto, J.S.M.; de Freitas, I.C.M. Nutritional and socioeconomic status in adults living in Ribeirão Preto, SP, 2006. OBEDIARP Project. Rev. Bras. Epidemiol. 2011, 14, 662–676. [Google Scholar] [CrossRef] [PubMed]
- El Rhazi, K.; Nejjari, C.; Zidouh, A.; Bakkali, R.; Berraho, M.; Gateau, P.B. Prevalence of obesity and associated sociodemographic and lifestyle factors in Morocco. Public Health Nutr 2010, 14, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Erem, C.; Arslan, C.; Hacihasanoglu, A.; Deger, O.; Topbaş, M.; Ukinc, K.; Ersöz, H.; Telatar, M. Prevalence of Obesity and Associated Risk Factors in a Turkish Population (Trabzon City, Turkey). Obes. Res. 2004, 12, 1117–1127. [Google Scholar] [CrossRef] [PubMed]
- Eum, M.-J.; Jung, H.-S. The interplay of sleep duration, working hours, and obesity in Korean male workers: The 2010–2015 Korea National Health and Nutrition Examination Survey. PLoS ONE 2021, 16, e0247746. [Google Scholar] [CrossRef]
- Mashinya, F.; Alberts, M.; Cook, I.; Ntuli, S. Determinants of body mass index by gender in the Dikgale Health and Demographic Surveillance System site, South Africa. Glob. Health Action 2018, 11, 45–55. [Google Scholar] [CrossRef]
- Fouad, M.; Rastam, S.; Ward, K.; Maziak, W. Prevalence of obesity and its associated factors in Aleppo, Syria. Prev. Control. 2006, 2, 85–94. [Google Scholar] [CrossRef]
- Gallus, S.; Odone, A.; Lugo, A.; Bosetti, C.; Colombo, P.; Zuccaro, P.; La Vecchia, C. Overweight and obesity prevalence and determinants in Italy: An update to 2010. Eur. J. Nutr. 2012, 52, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Gong, S.; Wang, K.; Li, Y.; Zhou, Z.; Alamian, A. Ethnic group differences in obesity in Asian Americans in California, 2013–2014. BMC Public Health 2021, 21, 1–10. [Google Scholar] [CrossRef]
- Gouda, J.; Prusty, R.K. Overweight and obesity among women by economic stratum in urban india. J. Health Popul. Nutr. 2014, 32, 79–88. [Google Scholar] [PubMed]
- Hajek, A.; Brettschneider, C.; van der Leeden, C.; Lühmann, D.; Oey, A.; Wiese, B.; Weyerer, S.; Werle, J.; Fuchs, A.; Pentzek, M.; et al. Prevalence and factors associated with obesity among the oldest old. Arch. Gerontol. Geriatr. 2020, 89, 104069. [Google Scholar] [CrossRef]
- Sarma, H.; Saquib, N.; Hasan, M.; Saquib, J.; Rahman, A.S.; Khan, J.R.; Uddin, J.; Cullen, M.R.; Ahmed, T. Determinants of overweight or obesity among ever-married adult women in Bangladesh. BMC Obes. 2016, 3, 13. [Google Scholar] [CrossRef]
- Hosseini, Z.; Veenstra, G.; Khan, N.A.; Conklin, A.I. Associations between social connections, their interactions, and obesity differ by gender: A population-based, cross-sectional analysis of the Canadian Longitudinal Study on Aging. PLoS ONE 2020, 15, e0235977. [Google Scholar] [CrossRef]
- Hosseinpanah, F.; Mirbolouk, M.; Mossadeghkhah, A.; Barzin, M.; Serahati, S.; Delshad, H.; Azizi, F. Incidence and potential risk factors of obesity among Tehranian adults. Prev. Med. 2015, 82, 99–104. [Google Scholar] [CrossRef]
- Hruby, A.; Hill, O.T.; Bulathsinhala, L.; McKinnon, C.J.; Montain, S.J.; Young, A.J.; Smith, T.J. Trends in overweight and obesity in soldiers entering the USArmy, 1989-2012. Obesity 2015, 23, 662–670. [Google Scholar] [CrossRef]
- Ajayi, I.O.; Adebamowo, C.; Adami, H.-O.; Dalal, S.; Diamond, M.B.; Bajunirwe, F.; Guwatudde, D.; Njelekela, M.; Nankya-Mutyoba, J.; Chiwanga, F.S.; et al. Urban–rural and geographic differences in overweight and obesity in four sub-Saharan African adult populations: A multi-country cross-sectional study. BMC Public Health 2016, 16, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Garstka, M.A.; Chai, Z.; Chen, Y.; Lipkova, V.; Cooper, M.E.; Mokoena, K.K.; Wang, Y.; Zhang, L. Marriage contributes to higher obesity risk in China: Findings from the China Health and Nutrition Survey. Ann. Transl. Med. 2021, 9, 564. [Google Scholar] [CrossRef]
- Janghorbani, M.; Amini, M.; Rezvanian, H.; Gouya, M.-M.; Delavari, A.; Alikhani, S.; Mahdavi, A. Association of body mass index and abdominal obesity with marital status in adults. Arch. Iran. Med. 2008, 11, 274–281. [Google Scholar] [PubMed]
- Kaboré, S.; Millogo, T.; Soubeiga, J.K.; Lanou, H.; Bicaba, B.; Kouanda, S. Prevalence and risk factors for overweight and obesity: A cross-sectional countrywide study in Burkina Faso. BMJ Open 2020, 10, e032953. [Google Scholar] [CrossRef] [PubMed]
- Kahn, H.S.; Williamson, D.F.; A Stevens, J. Race and weight change in US women: The roles of socioeconomic and marital status. Am. J. Public Health 1991, 81, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Kamal, S.M.; Hassan, C.H.; Alam, G.M. Dual Burden of Underweight and Overweight among Women in Bangladesh: Patterns, Prevalence, and Sociodemographic Correlates. J. Health Popul. Nutr. 2015, 33, 92–105. [Google Scholar] [PubMed]
- Kaplan, M.S.; Huguet, N.; Newsom, J.T.; McFarland, B.H.; Lindsay, J. Prevalence and Correlates of Overweight and Obesity among Older Adults: Findings from the Canadian National Population Health Survey. J. Gerontol. Ser. A 2003, 58, M1018–M1030. [Google Scholar] [CrossRef]
- Kee, C.C.; Jamaiyah, H.; Safiza, M.N.N.; Khor, G.L.; Suzana, S.; Jamalludin, A.R.; Rahmah, R.; Ahmad, A.Z.; Ruzita, A.T.; Wong, N.F.; et al. Abdominal Obesity in Malaysian Adults: National Health and Morbidity Survey III (NHMS III, 2006). Malays. J. Nutr. 2008, 14, 125–135. [Google Scholar]
- Khabazkhoob, M.; Emamian, M.H.; Hashemi, H.; Shariati, M.; Fotouhi, A. Prevalence of Overweight and Obesity in the Middle-age Population: A Priority for the Health System. Iran. J. Public Health 2017, 46, 827–834. [Google Scholar]
- Khader, Y.; Batieha, A.; Ajlouni, H.; El-Khateeb, M.; Ajlouni, K. Obesity in Jordan: Prevalence, Associated Factors, Comorbidities, and Change in Prevalence over Ten Years. Metab. Syndr. Relat. Disord. 2008, 6, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Klos, L.A.; Sobal, J. Marital status and body weight, weight perception, and weight management among U.S. adults. Eat. Behav. 2013, 14, 500–507. [Google Scholar] [CrossRef]
- Kowalkowska, J.; Poínhos, R.; Franchini, B.; Afonso, C.; Correia, F.; Pinhão, S.; de Almeida, M.D.V.; Rodrigues, S. General and abdominal adiposity in a representative sample of Portuguese adults: Dependency of measures and socio-demographic factors’ influence. Br. J. Nutr. 2015, 115, 185–192. [Google Scholar] [CrossRef]
- Ahmed, K.Y.; Rwabilimbo, A.G.; Abrha, S.; Page, A.; Arora, A.; Tadese, F.; Beyene, T.Y.; Seiko, A.; Endris, A.A.; Agho, K.E.; et al. Factors associated with underweight, overweight, and obesity in reproductive age Tanzanian women. PLoS ONE 2020, 15, e0237720. [Google Scholar] [CrossRef]
- Lee, J.; Shin, A.; Cho, S.; Choi, J.-Y.; Kang, D.; Lee, J.-K. Marital status and the prevalence of obesity in a Korean population. Obes. Res. Clin. Pract. 2020, 14, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Letamo, G. The prevalence of, and factors associated with, overweight and obesity in Botswana. J. Biosoc. Sci. 2011, 43, 75–84. [Google Scholar] [CrossRef]
- Liao, C.; Gao, W.; Cao, W.; Lv, J.; Yu, C.; Wang, S.; Pang, Z.; Cong, L.; Dong, Z.; Wu, F.; et al. Association of Educational Level and Marital Status with Obesity: A Study of Chinese Twins. Twin Res. Hum. Genet. 2018, 21, 126–135. [Google Scholar] [CrossRef]
- Mangemba, N.T.; Sebastian, M.S. Societal risk factors for overweight and obesity in women in Zimbabwe: A cross-sectional study. BMC Public Health 2020, 20, 1–8. [Google Scholar] [CrossRef]
- Memish, Z.A.; El Bcheraoui, C.; Tuffaha, M.; Robinson, M.; Daoud, F.; Jaber, S.; Mikhitarian, S.; Al Saeedi, M.; AlMazroa, M.A.; Mokdad, A.H.; et al. Obesity and Associated Factors—Kingdom of Saudi Arabia, 2013. Prev. Chronic Dis. 2014, 11, E174. [Google Scholar] [CrossRef]
- Mistretta, A.; Marventano, S.; Platania, A.; Godos, J.; Galvano, F.; Grosso, G. Metabolic profile of the Mediterranean healthy Eating, Lifestyle and Aging (MEAL) study cohort. Mediterr. J. Nutr. Metab. 2017, 10, 131–140. [Google Scholar] [CrossRef]
- Mkuu, R.S.; Epnere, K.; Chowdhury, M.A.B. Prevalence and Predictors of Overweight and Obesity among Kenyan Women. Prev. Chronic Dis. 2018, 15, E44. [Google Scholar] [CrossRef]
- Modjadji, P. Socio-demographic Determinants of Overweight and Obesity among Mothers of Primary School Children Living in a Rural Health and Demographic Surveillance System Site, South Africa. Open Public Health J. 2020, 13, 518–528. [Google Scholar] [CrossRef]
- Moise, I.K.; Kangmennaang, J.; Halwiindi, H.; Grigsby-Toussaint, D.S.; Fuller, D.O. Increase in Obesity among Women of Reproductive Age in Zambia, 2002–2014. J. Women’s Health 2019, 28, 1679–1687. [Google Scholar] [CrossRef]
- Mukora-Mutseyekwa, F.; Zeeb, H.; Nengomasha, L.; Adjei, N.K. Trends in Prevalence and Related Risk Factors of Overweight and Obesity among Women of Reproductive Age in Zimbabwe, 2005–2015. Int. J. Environ. Res. Public Health 2019, 16, 2758. [Google Scholar] [CrossRef] [PubMed]
- Mustafa, J.; Salle, N.M.; Isa, Z.M.; Gha, H.F. Overweight Problem among Primary Health Care Workers in Suburban District of Hulu Langat, Selangor, Malaysia. Pak. J. Nutr. 2013, 12, 291–296. [Google Scholar] [CrossRef]
- Najafi, F.; Pasdar, Y.; Hamzeh, B.; Rezaei, S.; Nazar, M.M.; Soofi, M. Measuring and Decomposing Socioeconomic Inequalities in Adult Obesity in Western Iran. J. Prev. Med. Public Health 2018, 51, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Oguoma, V.M.; Coffee, N.T.; Alsharrah, S.; Abu-Farha, M.; Al-Refaei, F.H.; Al-Mulla, F.; Daniel, M. Prevalence of overweight and obesity, and associations with socio-demographic factors in Kuwait. BMC Public Health 2021, 21, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Okop, K.J.; Levitt, N.; Puoane, T. Factors Associated with Excessive Body Fat in Men and Women: Cross-Sectional Data from Black South Africans Living in a Rural Community and an Urban Township. PLoS ONE 2015, 10, e0140153. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, A.J.; Rostila, M.; de Leon, A.P.; Lopes, C.S. The influence of social relationships on obesity: Sex differences in a longitudinal study. Obesity 2013, 21, 1540–1547. [Google Scholar] [CrossRef]
- Omar, S.M.; Taha, Z.; Hassan, A.A.; Al-Wutayd, O.; Adam, I. Prevalence and factors associated with overweight and central obesity among adults in the Eastern Sudan. PLoS ONE 2020, 15, e0232624. [Google Scholar] [CrossRef]
- Ortiz-Moncada, R.; García, M.; González-Zapata, L.I.; Fernandez, E.; Álvarez-Dardet, C. Incidence of overweight and obesity in a Mediterranean population-based cohort: The Cornellà Health Interview Survey Follow-up Study (CHIS.FU). Prev. Med. 2010, 50, 45–49. [Google Scholar] [CrossRef]
- Pereko, K.K.; Setorglo, J.; Owusu, W.B.; Tiweh, J.M.; Achampong, E.K. Overnutrition and associated factors among adults aged 20 years and above in fishing communities in the urban Cape Coast Metropolis, Ghana. Public Health Nutr 2012, 16, 591–595. [Google Scholar] [CrossRef]
- Puciato, D.; Rozpara, M. Demographic and Socioeconomic Determinants of Body Mass Index in People of Working Age. Int. J. Environ. Res. Public Health 2020, 17, 8168. [Google Scholar] [CrossRef]
- Qureshi, S.A.; Straiton, M.; Gele, A.A. Associations of socio-demographic factors with adiposity among immigrants in Norway: A secondary data analysis. BMC Public Health 2020, 20, 772. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Zhang, P.; Gao, C.; Li, Z.; Lv, X.; Song, Y.; Yu, Y.; Li, B. Prevalence of overweight and obesity and some associated factors among adult residents of northeast China: A cross-sectional study. BMJ Open 2016, 6, e010828. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, S.L.; Hagedorn, A.; Yeom, J.; Saito, Y.; Yokoyama, E.; Crimmins, E.M. A Tale of Two Countries---the United States and Japan: Are Differences in Health Due to Differences in Overweight? J. Epidemiology 2008, 18, 280–290. [Google Scholar] [CrossRef] [PubMed]
- Tu, R.; Hou, J.; Liu, X.; Li, R.; Dong, X.; Pan, M.; Yin, S.; Hu, K.; Mao, Z.; Huo, W.; et al. Low socioeconomic status aggravated associations of exposure to mixture of air pollutants with obesity in rural Chinese adults: A cross-sectional study. Environ. Res. 2020, 194, 110632. [Google Scholar] [CrossRef] [PubMed]
- Santos, A.-C.; Barros, H. Prevalence and determinants of obesity in an urban sample of Portuguese adults. Public Health 2003, 117, 430–437. [Google Scholar] [CrossRef]
- Sarlio-Lahteenkorva, S.; Lahelma, E. The association of body mass index with social and economic disadvantage in women and men. Int. J. Epidemiol. 1999, 28, 445–449. [Google Scholar] [CrossRef]
- Sartorius, B.; Veerman, L.J.; Manyema, M.; Chola, L.; Hofman, K. Determinants of Obesity and Associated Population Attributability, South Africa: Empirical Evidence from a National Panel Survey, 2008-2012. PLoS ONE 2015, 10, e0130218. [Google Scholar] [CrossRef] [PubMed]
- Segheto, W.; Hallal, P.C.; Marins, J.C.B.; da Silva, D.C.G.; Coelho, F.A.; Ribeiro, A.Q.; Morais, S.H.O.; Longo, G.Z. Factors associated with body adiposity index (BAI) in adults: Population-based study. Cienc. Saude Coletiva 2018, 23, 773–783. [Google Scholar] [CrossRef]
- Seubsman, S.-A.; Lim, L.L.-Y.; Banwell, C.; Sripaiboonkit, N.; Kelly, M.; Bain, C.; Sleigh, A. Socioeconomic Status, Sex, and Obesity in a Large National Cohort of 15–87-Year-Old Open University Students in Thailand. J. Epidemiol. 2010, 20, 13–20. [Google Scholar] [CrossRef]
- Ahmed, S.H.; Meyer, H.E.; Kjøllesdal, M.K.; Madar, A.A. Prevalence and Predictors of Overweight and Obesity among Somalis in Norway and Somaliland: A Comparative Study. J. Obes. 2018, 2018, 1–8. [Google Scholar] [CrossRef]
- A Shayo, G.; Mugusi, F.M. Prevalence of obesity and associated risk factors among adults in Kinondoni municipal district, Dar es Salaam Tanzania. BMC Public Health 2011, 11, 365. [Google Scholar] [CrossRef] [PubMed]
- Sidik, S.M.; Rampal, L. The prevalence and factors associated with obesity among adult women in Selangor, Malaysia. Asia Pac. Fam. Med. 2009, 8, 2. [Google Scholar] [CrossRef] [PubMed]
- Sim, S.; Laohasiriwong, W. Fast Food Consumption, Overweight and Obesity among Working Age Persons in Cambodia. J. Clin. Diagn. Res. 2019, 13, LC1–LC6. [Google Scholar] [CrossRef]
- Smith, T.J.; Marriott, B.P.; Dotson, L.; Bathalon, G.P.; Funderburk, L.; White, A.; Hadden, L.; Young, A.J. Overweight and Obesity in Military Personnel: Sociodemographic Predictors. Obesity 2012, 20, 1534–1538. [Google Scholar] [CrossRef]
- Sobal, J.; Hanson, K.L.; Frongillo, E.A. Gender, Ethnicity, Marital Status, and Body Weight in the United States. Obesity 2009, 17, 2223–2231. [Google Scholar] [CrossRef]
- Song, N.; Liu, F.; Han, M.; Zhao, Q.; Zhai, H.; Li, X.-M.; Du, G.-L.; Li, X.-M.; Yang, Y.-N. Prevalence of overweight and obesity and associated risk factors among adult residents of northwest China: A cross-sectional study. BMJ Open 2019, 9, e028131. [Google Scholar] [CrossRef] [PubMed]
- Suzana, S.; Kee, C.C.; Jamaludin, A.R.; Noor Safiza, M.N.; Khor, G.L.; Jamaiyah, H.; Geeta, A.; Ahmad Ali, Z.; Rahmah, R.; Ruzita, A.T.; et al. The Third National Health and Morbidity Survey: Prevalence of obesity, and abdominal obesity among the Malaysian elderly population. Asia Pac. J. Public Health 2012, 24, 318–329. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, W.; Wuren; Kuriki, K. Associations between family factors and body weight gain from 20 years old. BMC Women’s Health 2019, 19, 1–10. [Google Scholar] [CrossRef]
- Taghdir, M.; Alimohamadi, Y.; Sepandi, M.; Rezaianzadeh, A.; Abbaszadeh, S.; Mahmud, F.M. Association between parity and obesity: A cross sectional study on 6,447 Iranian females. J. Prev. Med. Hyg. 2020, 61, E476–E481. [Google Scholar] [CrossRef]
- Tanwi, T.S.; Chakrabarty, S.; Hasanuzzaman, S. Double burden of malnutrition among ever-married women in Bangladesh: A pooled analysis. BMC Women’s Health 2019, 19, 1–8. [Google Scholar] [CrossRef]
- Tchicaya, A.; Lorentz, N. Socioeconomic inequality and obesity prevalence trends in luxembourg, 1995–2007. BMC Res. Notes 2012, 5, 467. [Google Scholar] [CrossRef] [PubMed]
- Torp, J.A.; Berggren, V.; Erlandsson, L.-K.; Westergren, A. Weight Status among Somali Immigrants in Sweden in Relation to Sociodemographic Characteristics, Dietary Habits and Physical Activity. Open Public Health J. 2015, 8, 10–16. [Google Scholar] [CrossRef]
- Tzotzas, T.; Vlahavas, G.; Papadopoulou, S.K.; Kapantais, E.; Kaklamanou, D.; Hassapidou, M. Marital status and educational level associated to obesity in Greek adults: Data from the National Epidemiological Survey. BMC Public Health 2010, 10, 732. [Google Scholar] [CrossRef] [PubMed]
- Gigante, D.P.; Moura, E.C.D.; Sardinha, L.M.V. Prevalence of overweight and obesity and associated factors. Rev. Saude Publica 2009, 43, 83–89. [Google Scholar] [CrossRef]
- Veghari, G.; Sedaghat, M.; Joshaghani, H.; Hoseini, A.; Niknezhad, F.; Angizeh, A.; Tazik, E.; Moharloei, P. The Prevalence of Obesity and its Related Risk Factor in the North of Iran in 2006 ARTICLE INFORMATION ABSTRACT. J. Res. Health Sci. (JRHS) 2010, 10, 116–121. [Google Scholar]
- Wardle, J.; Waller, J.; Jarvis, M.J. Sex Differences in the Association of Socioeconomic Status with Obesity. Am. J. Public Health 2002, 92, 1299–1304. [Google Scholar] [CrossRef]
- Watson, K.; Roberts, B.; Chow, C.; Goryakin, Y.; Rotman, D.; Gasparishvili, A.; Haerpfer, C.; McKee, M. Micro- and meso-level influences on obesity in the former Soviet Union: A multi-level analysis. Eur. J. Public Health 2012, 23, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Weiderpass, E.; Botteri, E.; Longenecker, J.C.; Alkandari, A.; Al-Wotayan, R.; Al Duwairi, Q.; Tuomilehto, J. The Prevalence of Overweight and Obesity in an Adult Kuwaiti Population in 2014. Front. Endocrinol. 2019, 10, 449. [Google Scholar] [CrossRef]
- Woo, J.; Leung, S.; Ho, S.; Sham, A.; Lam, T.; Janus, E. Influence of educational level and marital status on dietary intake, obesity and other cardiovascular risk factors in a Hong Kong Chinese population. Eur. J. Clin. Nutr. 1999, 53, 461–467. [Google Scholar] [CrossRef]
- Liu, X.; Wu, W.; Mao, Z.; Huo, W.; Tu, R.; Qian, X.; Zhang, X.; Tian, Z.; Zhang, H.; Jiang, J.; et al. Prevalence and influencing factors of overweight and obesity in a Chinese rural population: The Henan Rural Cohort Study. Sci. Rep. 2018, 8, 1–11. [Google Scholar] [CrossRef]
- Wang, M.; Xu, S.; Liu, W.; Zhang, C.; Zhang, X.; Wang, L.; Liu, J.; Zhu, Z.; Hu, J.; Luo, X.; et al. Prevalence and changes of BMI categories in China and related chronic diseases: Cross-sectional National Health Service Surveys (NHSSs) from 2013 to 2018. EClinicalMedicine 2020, 26, 100521. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.; Xing, L.; Du, Z.; Tian, Y.; Jing, L.; Yan, H.; Lin, M.; Zhang, B.; Liu, S.; Pan, Y.; et al. Prevalence of Obesity and Associated Risk Factors and Cardiometabolic Comorbidities in Rural Northeast China. BioMed Res. Int. 2019, 2019, 1–9. [Google Scholar] [CrossRef]
- Zapata, M.E.; Bibiloni, M.d.M.; Tur, J.A. Prevalence of overweihgt, obesity, abdominal-obesity and short stature of adult population of Rosario, Argentina. Nutr. Hosp. 2016, 33, 1149–1158. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Wang, Z.; Wang, X.; Chen, Z.; Shao, L.; Tian, Y.; Zheng, C.; Li, S.; Zhu, M.; Gao, R. Prevalence of overweight and obesity in China: Results from a cross-sectional study of 441 thousand adults, 2012–2015. Obes. Res. Clin. Pract. 2020, 14, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Cao, D.; Si, Y.; Zhu, X.; Du, L.; Zhang, Y.; Zhou, Z. Income-related inequities of adult obesity and central obesity in China: Evidence from the China Health and Nutrition Survey 1997-2011. BMJ Open 2020, 10, e034288. [Google Scholar] [CrossRef]
- Jeffery, R.W.; Rick, A.M. Cross-Sectional and Longitudinal Associations between Body Mass Index and Marriage-Related Factors. Obes. Res. 2002, 10, 809–815. [Google Scholar] [CrossRef]
- Marks, D.F. Homeostatic theory of obesity. Health Psychol. Open 2015, 2, 2055102915590692. [Google Scholar] [CrossRef]
- Meltzer, A.A.; Everhart, J.E. Self-Reported Substantial 1-Year Weight Change among Men and Women in the United States. Obes. Res. 1995, 3, 123s–134s. [Google Scholar] [CrossRef]
- Bove, C.F.; Sobal, J. Body weight relationships in early marriage. Weight relevance, weight comparisons, and weight talk. Appetite 2011, 57, 729–742. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Year of Publication | Country | Period of Observation | Number of Participants | Evaluated Factors of Obesity | Results for Marital Status and Obesity |
|---|---|---|---|---|---|
| Zhang, 2020 [116] | China | 2012–2015 | 441,306 | Sex, age, education level, smoking, alcohol consumption, marital status, family history of cardiovascular disease | A significantly higher prevalence of overweight and obesity was found among married and cohabiting individuals compared to those who are unmarried, OR 1.16 (95% CI 1.07–1.25). |
| Gouda, 2014 [45] | India | 2005–2006 | 124,385 women | Age, religion, caste, education level, marital status, parity, work status, region, mass media exposure | Married women were 1.86 and 2.14 times more likely to be overweight or to have obesity, respectively, than unmarried women, RR 2.14 (95% CI 1.680–2.729). |
| Janghorbani, 2008 [53] | Iran | 2004–2005 | 89,404 | Sex, age, marital status, education level, physical activity, smoking, area of residence | Ever-married status was associated with a significantly higher risk of overweight and obesity in both men and women. The multivariate OR of obesity was three times higher in married compared to unmarried. |
| Seubsman, 2010 [91] | Thailand | 2005–2005 | 87,134 |
Sex, age, marital status, educational attainment, monthly personal income, household assets classified by replacement value, housing type. | Obesity was substantially less prevalent among single men and women than in those with relationships. |
| Gong, 2021 [44] | USA, California | 2013–2014 | 47,970 asian-americans | Sex, age, ethnicity, household income, smoking, marital status, education level, physical activity, fast food consumption | Obesity was highly prevalent among married people. |
| Baik, 2018 [25] | Republic of Korea | 1998–2011 | 42,584 | Sex, age, marital status, employment status, income, smoking, alcohol consumption, sleep duration, psychological factors, diet | Being married was associated with the prevalence of obesity. |
| Sartorius, 2015 [89] | South Africa | 2008–2012 | 28,247 | Sex, age, living in formal urban areas, white ethnicity, being married, not exercising and/or in higher socio-economic category and/or living in households with proportionate higher spending on food (and unhealthy food options) | Marriage was identified as an important determinant of obesity, with male obesity being more strongly associated with marital status. Leaving a marriage (divorce or widowhood) was associated with a considerable reduction of risk of obesity. |
| Hosseini, 2020 [48] | Canada | 2012–2015 | 28,238 | Age, marital status, smoking, education, social network size (sum of all social contacts), social participation (regular social activities) | Being single, widowed, or divorced/separated was associated with worse anthropometric outcomes in women. |
| Tzotzas, 2010 [105] | Greece | 2010–2010 | 17,341 | Gender, age, marital status, education level | A significant association between marital status and obesity was found in both sex groups. |
| № | Reference, Year of Publication | Country | Study Design | Obesity BMI Threshold | Age | Sample Size | The Results Given in the Article |
|---|---|---|---|---|---|---|---|
| 1 | Bakhshi et al., 2010 [26] | Iran | Cross-sectional study | ≥30 kg/m2 | 20–69 | 26,551 | Male OR 1.09 (0.9–1.32) Female OR 1.16 (1.03–1.31) |
| 2 | Erem et al., 2004 [39] | Turkey | Cross-sectional study | ≥30 kg/m2 | 20 or older | 5016 | Obesity prevalence: in women—29.4%, in men—16.5% |
| 3 | Klos et al., 2013 [61] | United States | Cross-sectional study | ≥30 kg/m2 | 20 or older | 8078 | Married OR 1.73 (1.20–2.52) |
| 4 | Fouad et al., 2006 [42] | Syrian Republic | Cross-sectional study | ≥30 kg/m2 | 18–65 | 2038 | Married OR 2.62 (1.13–6.10) |
| 5 | Khader et al., 2008 [60] | Jordan | Cross-sectional study | ≥30 kg/m2 | 25 or older | 1121 | Married OR 2.7 (1.4–5.2) |
| 6 | Sidik et al., 2009 [94] | Malasya | Cross-sectional study | ≥30 kg/m2 | 20–59 | 891 | Married OR 2.70 (1.50–5.01) |
| 7 | Janghorbani et al., 2008 [53] | Iran | Cross-sectional study | ≥30 kg/m2 | 15–65 | 87,597 | Married OR 2.53 (2.25–2.85) |
| 8 | Seubsman et al., 2010 [91] | Thailand | A survey in cohort study | ≥25 kg/m2 | 15–87 | 85,886 | Obesity prevalence: Partnered males 29.4%–36.7% Partnered females 12.2%–13.2% Single males 14.8%–15.9% Single females 8.0%–8.6% |
| 9 | Badr et al., 2013 [24] | Kuweit | Cross-sectional study | ≥30 kg/m2 | 50 or older | 2443 | Married OR 2.29 (1.69–3.08) |
| 10 | Veghari et al., 2010 [107] | Iran | Cross-sectional study | ≥30 kg/m2 | 15–65 | 2495 | Married OR 5.95 (3.54–10.0) |
| 11 | Amer et al., 2011 [18] | Brazil | Cross-sectional study | ≥30 kg/m2 | 18 or older | 369 | Married OR 1.6 (0.63–4.11) |
| 12 | Shayo et al., 2011 [93] | Tanzania | Cross-sectional study | ≥30 kg/m2 | 18–65 | 1249 | Married OR 1.6 (1.0–2.4) |
| 13 | Watson et al., 2013 [109] | CIS countries | Cross-sectional study | ≥30 kg/m2 | 18 or older | 16,944 | Single OR 0.62 (0.50–0.75) |
| 14 | Kamal et al., 2015 [56] | Bangladesh | Cross-sectional study | ≥30 kg/m2 | 15–49 | 16,273 | Married OR 1.01 (0.82–1.25) |
| 15 | Wang et al., 2016 [84] | China | Cross-sectional study | ≥28 kg/m2 | 18–79 | 20,839 | Married OR 1.44 (1.19–1.74) |
| 16 | Memish et al., 2013 [68] | Saudi Arabia | Cross-sectional study | ≥30 kg/m2 | 15 or older | 10,702 | Single OR 0.53 (0.46–0.63) |
| 17 | Eum et al., 2021 [40] | Republic of Korea | Cross-sectional study | ≥25 kg/m2 | 19–60 | 2592 | Married RR 1.78 (1.25–2.54) |
| 18 | Mangemba et al., 2020 [67] | Republic of Zimbabwe | Cross-sectional study | ≥30 kg/m2 | 15–49 | 8904 | Married OR 1.54 (1.27–1.87) |
| 19 | Ahmed et al., 2020 [63] | Tanzania | Cross-sectional study | ≥30 kg/m2 | 15–49 | 11,741 | Married RR 1.78(1.25–2.54 |
| 20 | Najafi et al., 2018 [75] | Iran | A survey in cohort study | ≥30 kg/m2 | 35–65 | 10,086 | Overall prevalence of obesity 26.72% |
| 21 | Aladeniyi et al., 2017 [14] | Nigeria | Cross-sectional study | ≥30 kg/m2 | 24 or older | 4828 | Married OR 2.1 (1.7–2.8) |
| 22 | Liu et al., 2018 [112] | China | A survey in cohort study | ≥30 kg/m2 | 18–79 | 39,034 | Single OR 0.86 (0.77–0.96) |
| 23 | Omar et al., 2020 [79] | Eastern Sudan | Cross-sectional study | ≥30 kg/m2 | 20 or older | 594 | Married OR 4.37(2.60–7.35) |
| 24 | Song et al., 2019 [98] | China | Cross-sectional study | ≥28 kg/m2 | 35–80 | 14,618 | Married OR 1.8 (1.4–2.5) |
| Studies | Sample Size (N) | Odds Ratio | 95% Confidence Interval for OR |
|---|---|---|---|
| All studies (n = 24) | 369,499 | 1.70 | 1.38–2.10 * |
| Obesity threshold of BMI ≥ 30 kg/m2 (n = 19) | 218,655 | 1.88 | 1.54–2.29 * |
| Obesity threshold of BMI ≥ 28 kg/m2 (n = 3) | 63,682 | 1.34 | 0.91–1.97 |
| Obesity threshold of BMI ≥ 25 kg/m2 (n = 2) | 87,162 | 0.98 | 0.59–1.63 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nikolic Turnic, T.; Jakovljevic, V.; Strizhkova, Z.; Polukhin, N.; Ryaboy, D.; Kartashova, M.; Korenkova, M.; Kolchina, V.; Reshetnikov, V. The Association between Marital Status and Obesity: A Systematic Review and Meta-Analysis. Diseases 2024, 12, 146. https://doi.org/10.3390/diseases12070146
Nikolic Turnic T, Jakovljevic V, Strizhkova Z, Polukhin N, Ryaboy D, Kartashova M, Korenkova M, Kolchina V, Reshetnikov V. The Association between Marital Status and Obesity: A Systematic Review and Meta-Analysis. Diseases. 2024; 12(7):146. https://doi.org/10.3390/diseases12070146
Chicago/Turabian StyleNikolic Turnic, Tamara, Vladimir Jakovljevic, Zulfiya Strizhkova, Nikita Polukhin, Dmitry Ryaboy, Mariia Kartashova, Margarita Korenkova, Valeriia Kolchina, and Vladimir Reshetnikov. 2024. "The Association between Marital Status and Obesity: A Systematic Review and Meta-Analysis" Diseases 12, no. 7: 146. https://doi.org/10.3390/diseases12070146
APA StyleNikolic Turnic, T., Jakovljevic, V., Strizhkova, Z., Polukhin, N., Ryaboy, D., Kartashova, M., Korenkova, M., Kolchina, V., & Reshetnikov, V. (2024). The Association between Marital Status and Obesity: A Systematic Review and Meta-Analysis. Diseases, 12(7), 146. https://doi.org/10.3390/diseases12070146