A Case of Systemic Infection Caused by Streptococcus pyogenes Oral Infection in an Edentulous Patient

 ,
, {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
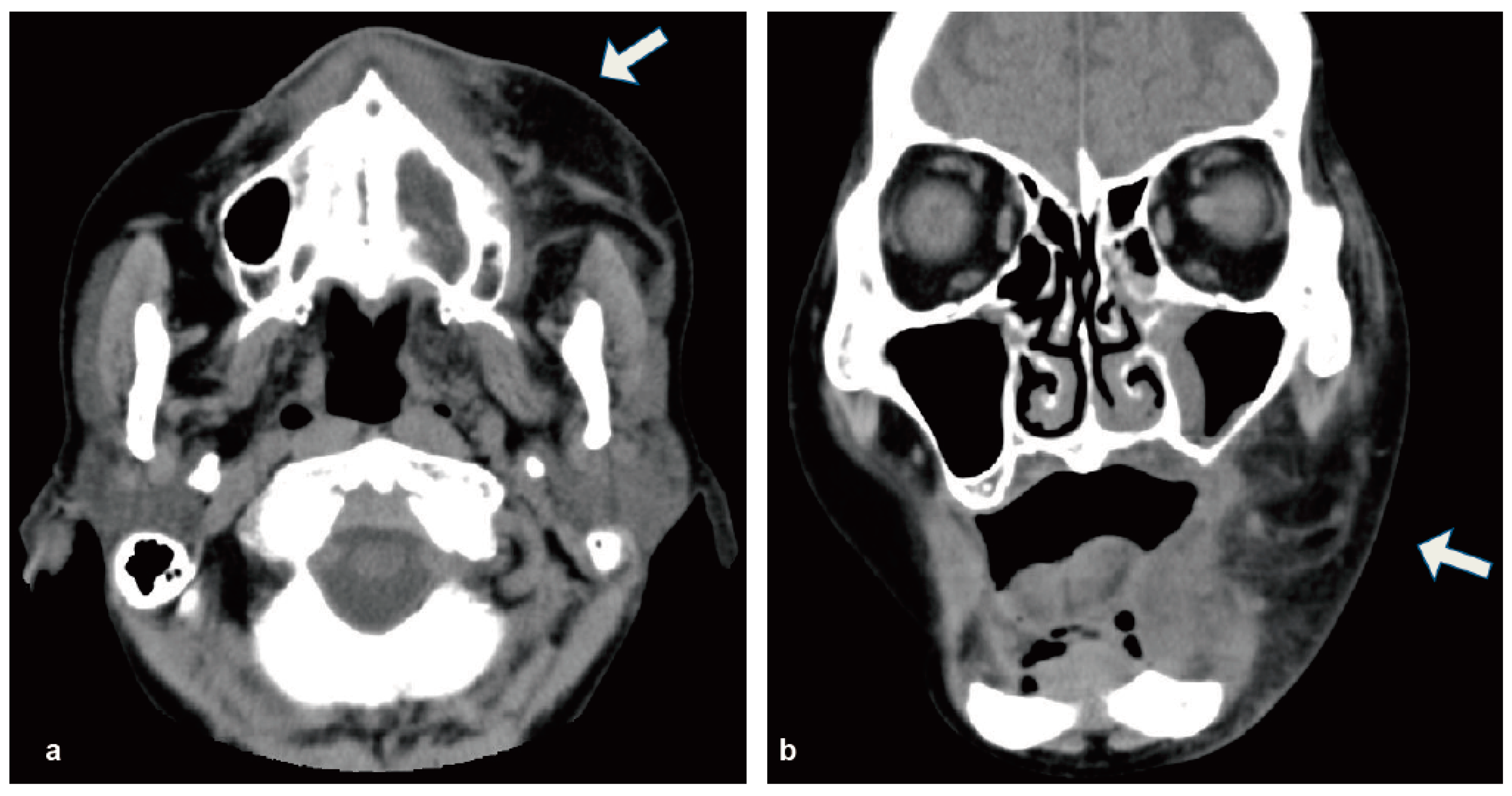
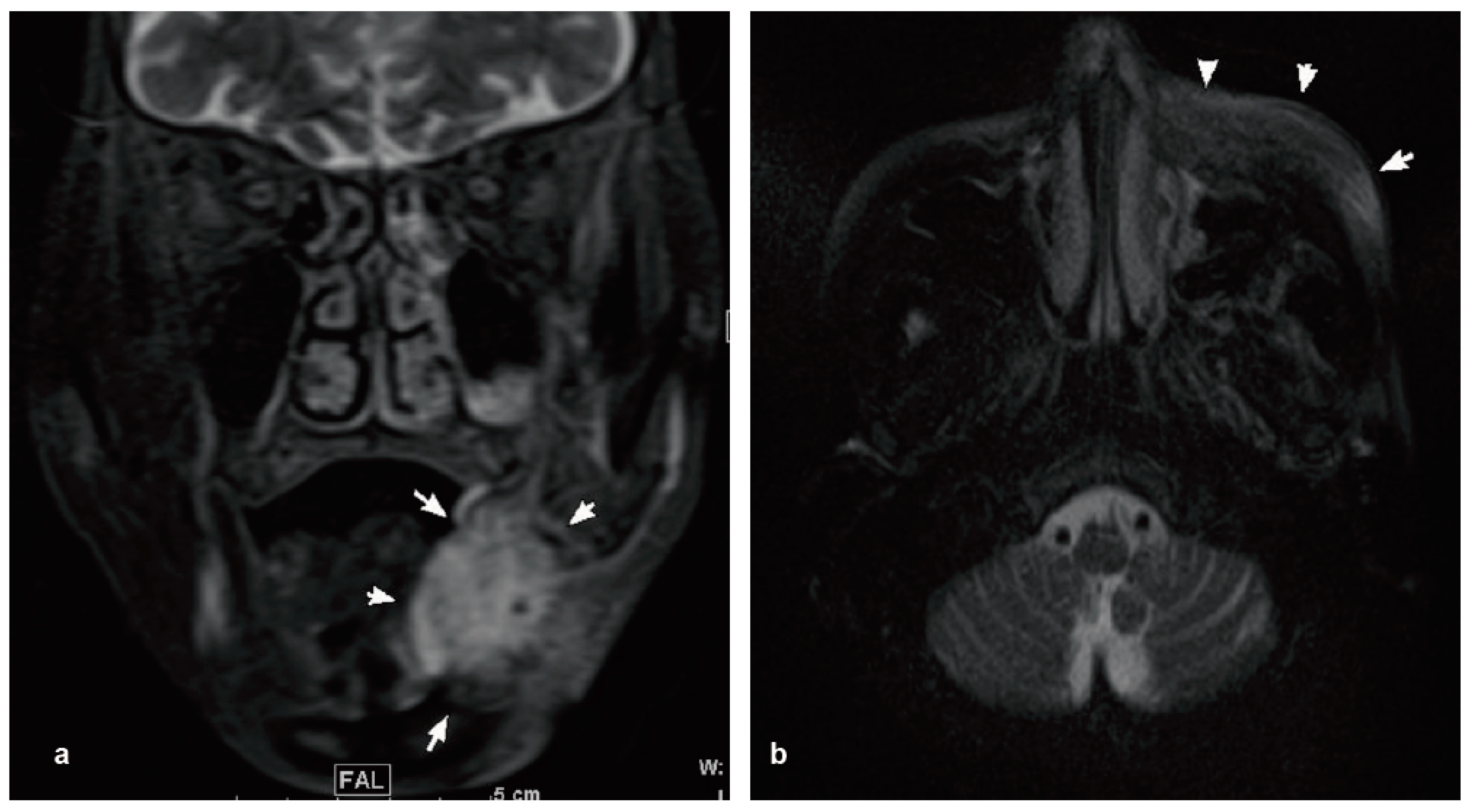
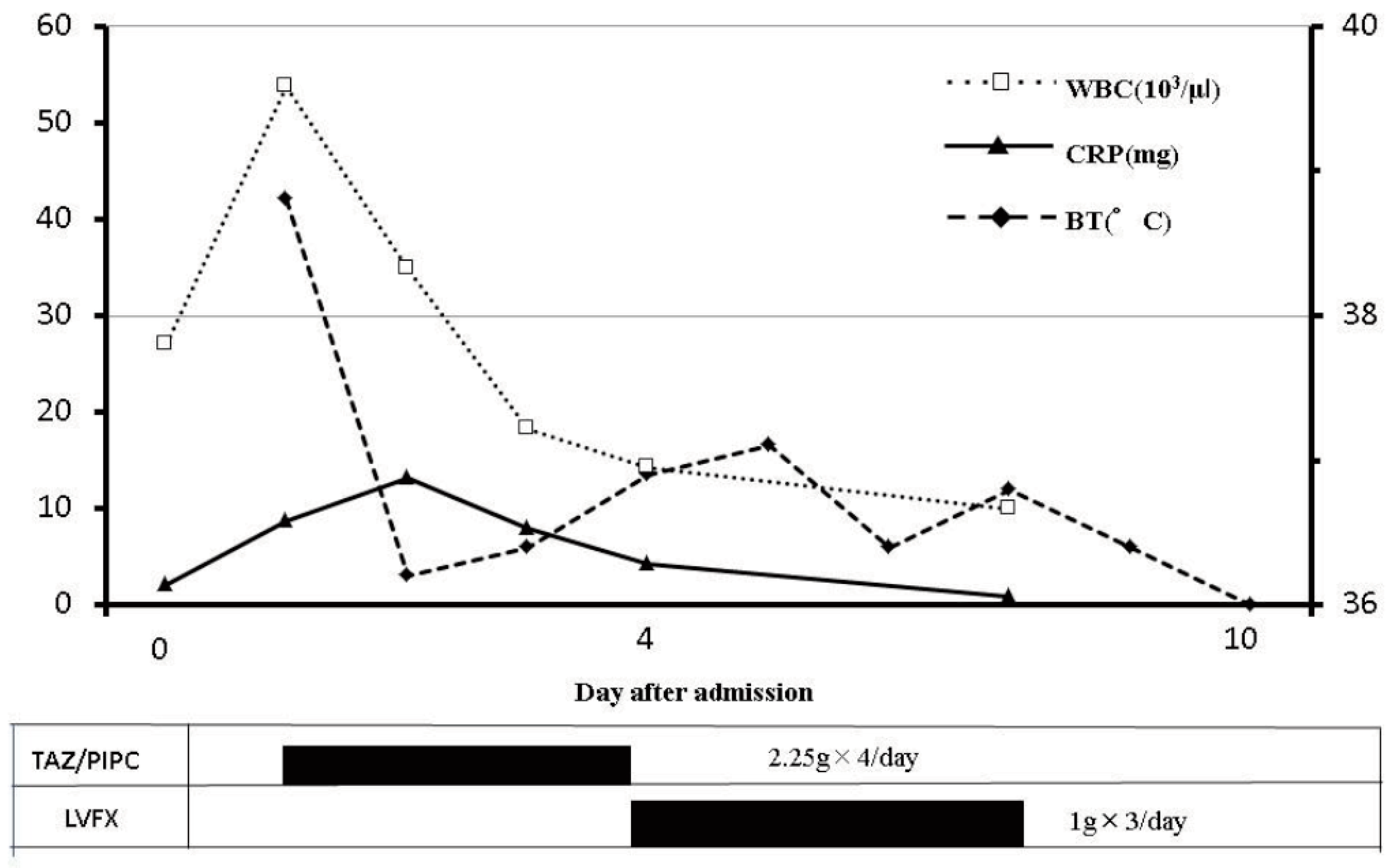
2. Case Report
3. Discussion
4. Ethics Approval and Informed Consent
Author Contributions
Conflicts of Interest
References
- Huang, T.T.; Tseng, F.Y.; Yeh, T.H.; Hsu, C.J.; Chen, Y.S. Factors affecting the bacteriology of deep neck infection: A retrospective study of 128 patients. Acta Otolaryngol. 2006, 126, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; An, J.; Zhang, Y.; Gong, X.; He, Y. Risk Factors for Life-Threatening Complications of Maxillofacial Space Infection. J. Craniofac. Surg. 2016, 27, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Opitz, D.; Camerer, C.; Camerer, D.M.; Raguse, J.D.; Menneking, H.; Hoffmeister, B.; Adolphs, N. Incidence and management of severe odontogenic infections—A retrospective analysis from 2004 to 2011. J. Craniomaxillofac. Surg. 2015, 43, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Bali, R.K.; Sharma, P.; Gaba, S.; Kaur, A.; Ghanghas, P. A review of complications of odontogenic infections. Natl. J. Maxillofac. Surg. 2015, 6, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Hu, L.; Wang, Z.; Nie, G.; Li, X.; Lin, D.; Luo, J.; Qin, H.; Wu, J.; Wen, W.; et al. Deep Neck Infection: A Review of 130 Cases in Southern China. Medicine 2015, 94, e994. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.; Yoo, K.; Yoon, S.; Ha, J.; Jung, S.; Kook, M.; Park, H.; Ryu, S.; Oh, H. Odontogenic infection involving the secondary fascial space in diabetic and non-diabetic patients: A clinical comparative study. J. Korean Assoc. Oral Maxillofac. Surg. 2013, 39, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Renton, B.J.; Clague, J.E.; Cooke, R.P. Streptococcus oralis endocarditis presenting as infective discitis in an edentulous patient. Int. J. Cardiol. 2009, 137, e13–e14. [Google Scholar] [CrossRef] [PubMed]
- Van Winkelhoff, A.J.; Wolf, J.W. Actinobacillus actinomycetemcomitans-associated peri-implantitis in an edentulous patient. A case report. J. Clin. Periodontol. 2000, 27, 531–535. [Google Scholar] [CrossRef] [PubMed]
- Danser, M.M.; van Winkelhoff, A.J.; de Graaff, J.; Loos, B.G.; van der Velden, U. Short-term effect of full-mouth extraction on periodontal pathogens colonizing the oral mucous membranes. J. Clin. Periodontol. 1994, 21, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Bessen, D.E. Population biology of the human restricted pathogen, Streptococcus pyogenes. Infect. Genet. Evol. 2009, 9, 581–593. [Google Scholar] [CrossRef] [PubMed]
- Stevens, D.L.; Bryant, A.E. Severe Group A Streptococcal Infections. In Streptococcus pyogenes: Basic Biology to Clinical Manifestations; Ferretti, J.J., Stevens, D.L., Fischetti, V.A., Eds.; EDN: Oklahoma City, OK, USA, 2016. [Google Scholar]
- Abe, M.; Mori, Y.; Saijo, H.; Hoshi, K.; Ohkubo, K.; Ono, T.; Takato, T. The efficacy of dental therapy for an adult case of Henoch-Schönlein Purpura. Oral Sci. Int. 2012, 9, 59–62. [Google Scholar] [CrossRef]
- Inaki, R.; Igarashi, M.; Abe, M.; Saijo, H.; Hoshi, K.; Takato, T. A case of infective endocarditis by Streptococcus mutans bacteremia induced by asymptomatic chronic dental caries in a wisdom tooth. Oral Sci. Jpn. 2014, 9, 95–96. [Google Scholar]
- Abe, M.; Mori, Y.; Inaki, R.; Ohata, Y.; Abe, T.; Saijo, H.; Ohkubo, K.; Hoshi, K.; Takato, T. A Case of Odontogenic Infection by Streptococcus constellatus Leading to Systemic Infection in a Cogan’s Syndrome Patient. Case Rep. Dent. 2014, 2014, 793174. [Google Scholar] [PubMed]
- Abe, M.; Abe, T.; Mogi, R.; Kamimoto, H.; Hatano, N.; Taniguchi, A.; Saijo, H.; Hoshi, K.; Takato, T. Cervical necrotizing fasciitis of odontogenic origin in a healthy young patient without pre-systemic disorders. J. Oral Maxillofac. Surg. Med. Pathol. 2017, 29, 341–344. [Google Scholar] [CrossRef]
- Offenbacher, S.; Barros, S.P.; Altarawneh, S.; Beck, J.D.; Loewy, Z.G. Impact of tooth loss on oral and systemic health. Gen. Dent. 2012, 60, 494–500. [Google Scholar] [PubMed]
- Migliorati, C.A.; Siegel, M.A.; Elting, L.S. Bisphosphonate-associated osteonecrosis: A long-term complication of bisphosphonate treatment. Lancet Oncol. 2006, 7, 508–514. [Google Scholar] [CrossRef]
- Danser, M.M.; van Winkelhoff, A.J.; de Graaff, J.; van der Velden, U. Putative periodontal pathogens colonizing oral mucous membranes in denture-wearing subjects with a past history of periodontitis. J. Clin. Periodontol. 1995, 22, 854–859. [Google Scholar] [CrossRef] [PubMed]
- Danser, M.M.; van Winkelhoff, A.J.; van der Velden, U. Periodontal bacteria colonizing oral mucous membranes in edentulous patients wearing dental implants. J. Periodontol. 1997, 68, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, D.E.; Shatzkes, D.R. Masticator space: Imaging anatomy for diagnosis. Otolaryngol. Clin. N. Am. 2012, 45, 1233–1251. [Google Scholar] [CrossRef] [PubMed]
- Bahl, R.; Sandhu, S.; Singh, K.; Sahai, N.; Gupta, M. Odontogenic infections: Microbiology and management. Contemp. Clin. Dent. 2014, 5, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Rega, A.J.; Aziz, S.R.; Ziccardi, V.B. Microbiology and antibiotic sensitivities of head and neck space infections of odontogenic origin. J. Oral Maxillofac. Surg. 2006, 64, 1377–1380. [Google Scholar] [CrossRef] [PubMed]
- Storoe, W.; Haug, R.H.; Lillich, T.T. The changing face of odontogenic infections. J. Oral Maxillofac. Surg. 2001, 59, 739–748. [Google Scholar] [CrossRef] [PubMed]
- Fenaux, P.; Haase, D.; Sanz, G.F.; Santini, V.; Buske, C.; Group, E.G.W. Myelodysplastic syndromes: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2014, 25 (Suppl. 3), 57–69. [Google Scholar] [CrossRef] [PubMed]
- Ades, L.; Itzykson, R.; Fenaux, P. Myelodysplastic syndromes. Lancet 2014, 383, 2239–2252. [Google Scholar] [CrossRef]



© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inagaki, Y.; Abe, M.; Inaki, R.; Zong, L.; Suenaga, H.; Abe, T.; Hoshi, K. A Case of Systemic Infection Caused by Streptococcus pyogenes Oral Infection in an Edentulous Patient. Diseases 2017, 5, 17. https://doi.org/10.3390/diseases5030017
Inagaki Y, Abe M, Inaki R, Zong L, Suenaga H, Abe T, Hoshi K. A Case of Systemic Infection Caused by Streptococcus pyogenes Oral Infection in an Edentulous Patient. Diseases. 2017; 5(3):17. https://doi.org/10.3390/diseases5030017
Chicago/Turabian StyleInagaki, Yumi, Masanobu Abe, Ryoko Inaki, Liang Zong, Hideyuki Suenaga, Takahiro Abe, and Kazuto Hoshi. 2017. "A Case of Systemic Infection Caused by Streptococcus pyogenes Oral Infection in an Edentulous Patient" Diseases 5, no. 3: 17. https://doi.org/10.3390/diseases5030017
APA StyleInagaki, Y., Abe, M., Inaki, R., Zong, L., Suenaga, H., Abe, T., & Hoshi, K. (2017). A Case of Systemic Infection Caused by Streptococcus pyogenes Oral Infection in an Edentulous Patient. Diseases, 5(3), 17. https://doi.org/10.3390/diseases5030017