Relation between the Disability of the Arm, Shoulder and Hand Score and Muscle Strength in Post-Cardiac Surgery Patients

 ,
, 
Abstract
:1. Introduction
2. Methods
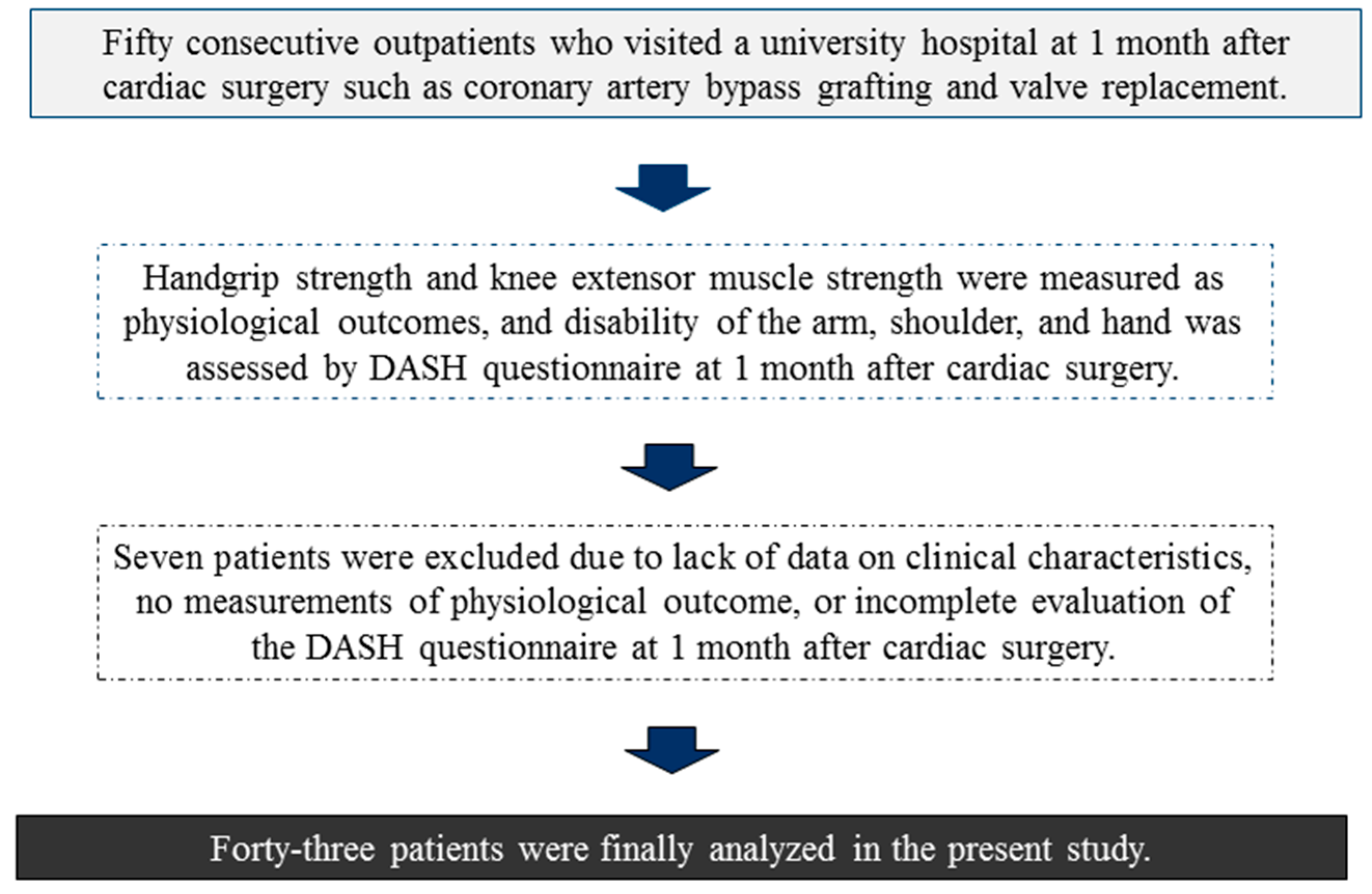
2.1. Participants
2.2. Physiological Outcomes
2.3. DASH Questionnaire
2.4. Statistical Analysis
3. Results
3.1. Clinical Characteristics of the Patients
3.2. Handgrip Strength, Knee Extensor Muscle Strength, and DASH Scores
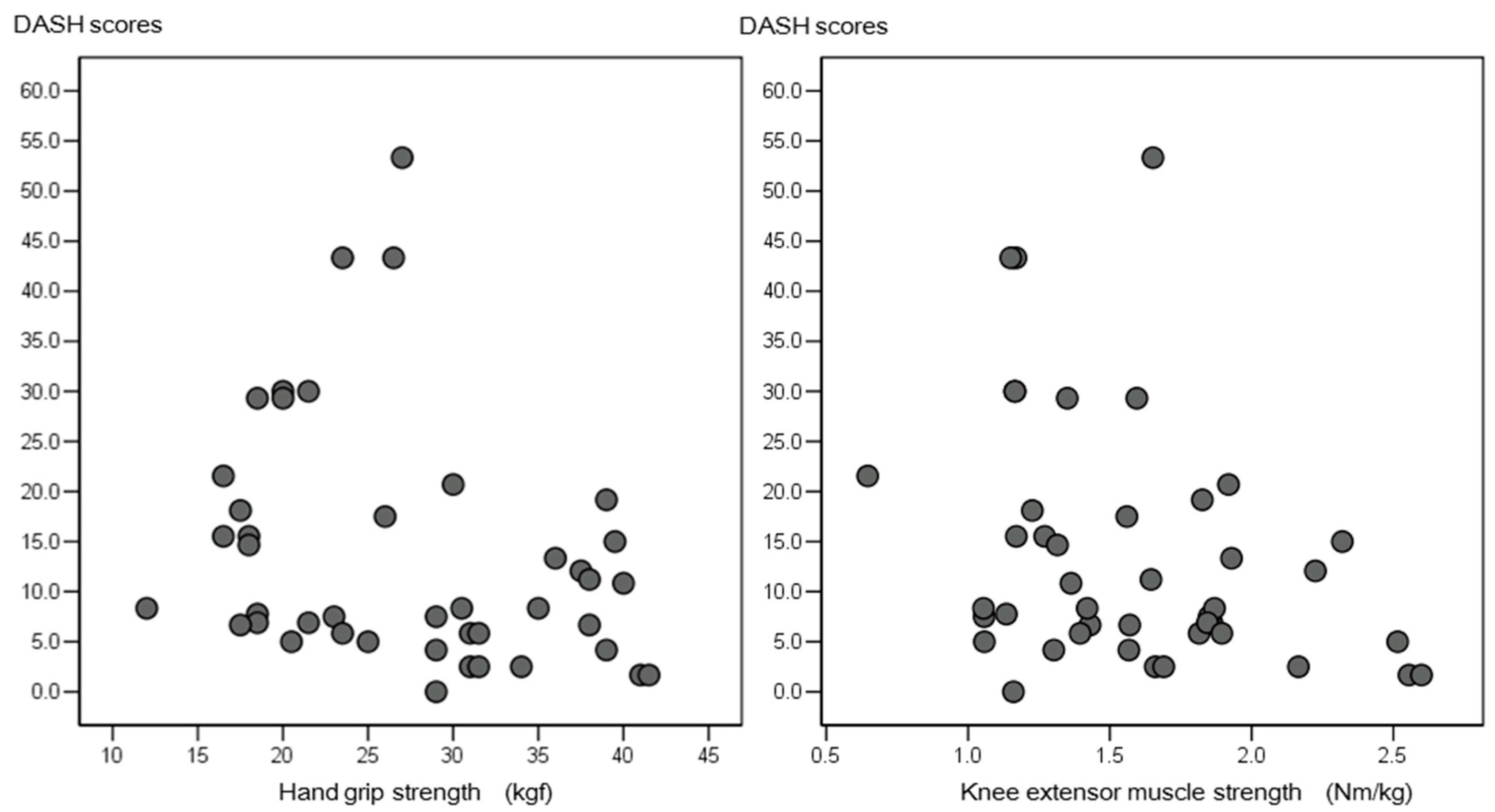
3.3. Relation between Physiological Outcomes of Handgrip and Knee Extensor Muscle Strength and DASH Score
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Menezes, A.R.; Lavie, C.J.; Milani, R.V.; Arena, R.A.; Church, T.S. Cardiac rehabilitation and exercise therapy in the elderly: Should we invest in the aged? J. Geriatr. Cardiol. 2012, 9, 68–75. [Google Scholar] [PubMed]
- Izawa, K.P.; Watanabe, S.; Oka, K.; Hiraki, K.; Morio, Y.; Kasahara, Y.; Iijima, S. Age-related differences in physiologic and psychosocial outcomes after cardiac rehabilitation. Am. J. Phys. Med. Rehabil. 2010, 89, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Hirano, Y.; Izawa, K.; Watanabe, S.; Yamada, S.; Oka, K.; Kasahara, Y.; Omiya, K. Physiological and health-related quality of life outcomes following cardiac rehabilitation after cardiac surgery. J. Jpn. Phys. Ther. Assoc. 2005, 8, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Hirschhorn, A.D.; Richards, D.A.; Mungovan, S.F.; Morris, N.R.; Adams, L. Does the mode of exercise influence recovery of functional capacity in the early postoperative period after coronary artery bypass graft surgery? A randomized controlled trial. Interact. Cardiovasc. Thorac. Surg. 2012, 15, 995–1003. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.; Thompson, D.R.; Oldridge, N.; Zwisler, A.D.; Rees, K.; Martin, N.; Taylor, R.S. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst. Rev. 2016. [Google Scholar] [CrossRef] [Green Version]
- Izawa, K.; Hirano, Y.; Yamada, S.; Oka, K.; Omiya, K.; Iijima, S. Improvement in physiological outcomes and health-related quality of life following cardiac rehabilitation in patients with acute myocardial infarction. Circ. J. 2004, 68, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Izawa, K.P.; Watanabe, S.; Oka, K.; Hiraki, K.; Morio, Y.; Kasahara, Y.; Makuuchi, H. Cardiac rehabilitation outcome following percutaneous coronary intervention compared to cardiac surgery. Recent Pat. Cardiovasc. Drug Discov. 2011, 6, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Iida, Y.; Yamazaki, T.; Arima, H.; Kawabe, T.; Yamada, S. Predictors of surgery-induced muscle proteolysis in patients undergoing cardiac surgery. J. Cardiol. 2016, 68, 536–541. [Google Scholar] [CrossRef] [PubMed]
- Imaeda, T.; Uchiyama, S.; Wada, T.; Okinaga, S.; Sawaizumi, T.; Omokawa, S.; Nishida, J. Reliability, validity, and responsiveness of the Japanese version of the Patient-Rated Wrist Evaluation. J. Orthop. Sci. 2010, 15, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Imaeda, T.; Toh, S.; Nakao, Y.; Nishida, J.; Hirata, H.; Ijichi, M.; Kohri, C.; Nagano, A. Validation of the Japanese Society for Surgery of the Hand version of the Disability of the Arm, Shoulder, and Hand questionnaire. J. Orthop. Sci. 2005, 10, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Beumer, A.; Lindau, T.R. Grip strength ratio: A grip strength measurement that correlates well with DASH score in different hand/wrist conditions. BMC Musculoskelet. Disord. 2014, 15, 336. [Google Scholar] [CrossRef] [PubMed]
- Gummesson, C.; Atroshi, I.; Ekdahl, C. The disabilities of the arm, shoulder and hand (DASH) outcome questionnaire: Longitudinal construct validity and measuring self-rated health change after surgery. BMC Musculoskelet. Disord. 2003, 4, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iida, Y.; Yamazaki, T.; Kawabe, T.; Usui, A.; Yamada, S. Postoperative muscle proteolysis affects systemic muscle weakness in patients undergoing cardiac surgery. Int. J. Cardiol. 2014, 172, 595–597. [Google Scholar] [CrossRef] [PubMed]
- Sears, B. Sternal Precautions after Open Heart Surgery. Available online: https://www.verywell.com/sternal-precautions-2696084 (accessed on 19 July 2012).
- Bloch, S.A.; Lee, J.Y.; Wort, S.J.; Polkey, M.I.; Kemp, P.R.; Griffiths, M.J. Sustained elevation of circulating growth and differentiation factor-15 and a dynamic imbalance in mediators of muscle homeostasis are associated with the development of acute muscle wasting following cardiac surgery. Crit. Care Med. 2013, 41, 982–989. [Google Scholar] [CrossRef] [PubMed]
- Petersson, B.; Wernerman, J.; Waller, S.O.; Von der Decken, A.; Vinnars, E. Elective abdominal surgery depresses muscle protein synthesis and increases subjective fatigue: Effects lasting more than 30 days. Br. J. Surg. 1990, 77, 796–800. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.; Prakash, M.; Froelicher, V.; Do, D.; Partington, S.; Atwood, J.E. Exercise capacity and mortality among men referred for exercise testing. N. Engl. J. Med. 2002, 346, 793–801. [Google Scholar] [CrossRef] [PubMed]
- Izawa, K.P.; Watanabe, S.; Oka, K.; Hiraki, K.; Morio, Y.; Kasahara, Y.; Omiya, K. Upper and lower extremity muscle strength levels associated with an exercise capacity of 5 metabolic equivalents in male patients with heart failure. J. Cardiopulm. Rehabil. Prev. 2012, 32, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Izawa, K.P.; Oka, K.; Watanabe, S.; Yokoyama, H.; Hiraki, K.; Morio, Y.; Omiya, K. Gender-related differences in clinical characteristics and physiological and psychosocial outcomes of Japanese patients at entry into phase II cardiac rehabilitation. J. Rehabil. Med. 2008, 40, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Yamasaki, H.; Yokoyama, H.; Aoki, U. Relationship between muscle strength in knee extensors and gait speed, independent gait in the elderly patients. Sogo Rehabil. 1998, 26, 689–692. (In Japanese) [Google Scholar]
- Fernandes, M.R. Patient-reported measures of quality of life and functional capacity in adhesive capsulitis. Rev. Assoc. Med. Bras. 2017, 63, 347–354. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| No. of Patients | 43 |
| Age (years, range) | 62.1 ± 9.1, 42–78 |
| Sex (male) | 32 |
| BMI (kg/m2) | 22.1 ± 0.7 |
| LVEF (%) | 53.5 ± 0.7 |
| Etiology (%) | |
| CABG | 58.1 |
| VR | 41.9 |
| Co-morbidity (%) | |
| Diabetes | 37.8 |
| Medications (%) | |
| Beta-blockers | 47.7 |
| ACEI/ARB | 43.2 |
| Diuretic | 70.5 |
| Values | Average | Minimum | Maximum |
|---|---|---|---|
| Handgrip strength (kgf) | 27.4 ± 8.3 | 12.0 | 42.0 |
| Knee extensor muscle strength (Nm/kg) | 1.6 ± 0.4 | 0.6 | 2.6 |
| DASH score | 13.3 ± 12.3 | 0.0 | 53.3 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Izawa, K.P.; Kasahara, Y.; Hiraki, K.; Hirano, Y.; Watanabe, S. Relation between the Disability of the Arm, Shoulder and Hand Score and Muscle Strength in Post-Cardiac Surgery Patients. Diseases 2017, 5, 31. https://doi.org/10.3390/diseases5040031
Izawa KP, Kasahara Y, Hiraki K, Hirano Y, Watanabe S. Relation between the Disability of the Arm, Shoulder and Hand Score and Muscle Strength in Post-Cardiac Surgery Patients. Diseases. 2017; 5(4):31. https://doi.org/10.3390/diseases5040031
Chicago/Turabian StyleIzawa, Kazuhiro P., Yusuke Kasahara, Koji Hiraki, Yasuyuki Hirano, and Satoshi Watanabe. 2017. "Relation between the Disability of the Arm, Shoulder and Hand Score and Muscle Strength in Post-Cardiac Surgery Patients" Diseases 5, no. 4: 31. https://doi.org/10.3390/diseases5040031
APA StyleIzawa, K. P., Kasahara, Y., Hiraki, K., Hirano, Y., & Watanabe, S. (2017). Relation between the Disability of the Arm, Shoulder and Hand Score and Muscle Strength in Post-Cardiac Surgery Patients. Diseases, 5(4), 31. https://doi.org/10.3390/diseases5040031