Metabolic Syndrome and Chronic Renal Disease


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Biochemical Measurements
2.3. Blood Pressure Measurements—Definitions
3. Data Analysis
4. Results
5. Discussion
6. Limitations
7. Conclusions
Author Contributions
Conflicts of Interest
Ethical Approval
Informed Consent
References
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [PubMed]
- Ford, E.S.; Giles, W.H.; Dietz, W.H. Prevalence of the metabolic syndrome among US adults: Findings from the third National Health and Nutrition Examination Survey. JAMA 2002, 287, 356–359. [Google Scholar] [CrossRef] [PubMed]
- Zammit, R.A.; Katz, J.M.; Derby, C.; Bitzer, M.; Lipton, B.R. Chronic Kidney Disease in Non-Diabetic Older Adults: Associated Roles of the Metabolic Syndrome, Inflammation, and Insulin Resistance. PLoS ONE 2015, 10, e0139369. [Google Scholar]
- Guembe, M.J.; Toledo, E.; Barba, J.; Martínez-Vila, E.; González-Diego, P.; Irimia, P.; Díez, J.; Viñes, J.J. Association between metabolic syndrome or its components and asymptomatic cardiovascular disease in the RIVANA-study. Atherosclerosis 2010, 211, 612–617. [Google Scholar] [CrossRef] [PubMed]
- Aguilar, M.; Bhuket, T.; Torres, S.; Liu, B.; Wong, R.J. Prevalence of the metabolic syndrome in the United States, 2003–2012. JAMA 2015, 313, 1973–1974. [Google Scholar] [PubMed]
- Tanamas, S.K.; Magliano, D.J.; Lynch, B.; Sethi, P.; Willenberg, L.; Polkinghorne, K.R. The Australian Diabetes, Obesity and Lifestyle Study (AusDiab); Baker IDI Heart and Diabetes Institute: Melbourne, Australia, 2013. [Google Scholar]
- Oguoma, V.M.; Nwose, E.U.; Richards, R.S. Prevalence of cardio-metabolic syndrome in Nigeria: A systematic review. Public Health 2015, 129, 413–423. [Google Scholar] [CrossRef] [PubMed]
- Sesso, R.C.; Lopes, A.A.; Thomé, F.S.; Lugon, J.R.; Martins, C.T. Brazilian Chronic Dialysis Survey 2016. J. Bras. Nefrol. 2017, 39, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Moţa, E.; Popa, S.G.; Moţa, M.; Mitrea, A.; Penescu, M.; Tuţă, L.; Serafinceanu, C.; Hâncu, N.; Gârneaţă, L.; Verzan, C. Prevalence of chronic kidney disease and its association with cardio-metabolic risk factors in the adult Romanian population: The PREDATORR study. Int. Urol. Nephrol. 2015, 47, 1831–1838. [Google Scholar] [CrossRef] [PubMed]
- Thomas, G.; Sehgal, R.A.; Kashyap, R.S.; Srinivas, R.T.; Kirwan, P.J.; Navaneethan, D.S. Metabolic Syndrome and Kidney Disease: A Systematic Review and Meta-analysis. Clin. J. Am. Soc. Nephrol. 2011, 6, 2364–2373. [Google Scholar] [CrossRef] [PubMed]
- Tozawa, M.; Iseki, C.; Tokashiki, K.; Chinen, S.; Kohagura, K.; Kinjo, K.; Takishita, S.; Iseki, K. Metabolic syndrome and risk of developing chronic kidney disease in Japanese adults. Hypertens. Res. 2007, 30, 937–943. [Google Scholar] [CrossRef] [PubMed]
- Ming, J.; Xu, S.; Yang, C.; Gao, B.; Wan, Y.; Xing, Y.; Zhang, L.; Yang, W.; Ji, Q.; China National Diabetes and Metabolic Disorders Study Group. Metabolic syndrome and chronic kidney disease in general Chinese adults: Results from the 2007–2008 China National Diabetes and Metabolic Disorders Study. Clin. Chim. Acta 2014, 430, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Kurella, M.; Chertow, G.M.; Fried, L.F.; Cummings, S.R.; Harris, T.; Simonsick, E.; Satterfield, S.; Ayonayon, H.; Yaffe, K. Chronic kidney disease and cognitive impairment in the elderly: The health, aging, and body composition study. J. Am. Soc. Nephrol. JASN 2005, 16, 2127–2133. [Google Scholar] [CrossRef] [PubMed]
- Alswat, K.A.; Althobaiti, A.; Alsaadi, K.; Alkhaldi, A.S.; Alharthi, M.M.; Abuharba, W.A.; Alzaidi, A.A. Prevalence of Metabolic Syndrome Among the End-Stage Renal Disease Patients on Hemodialysis. J. Clin. Med. Res. 2017, 9, 687–694. [Google Scholar] [CrossRef] [PubMed]
- Bonnet, F.; Marre, M.; Halimi, J.M.; Stengel, B.; Lange, C.; Laville, M.; Tichet, J.; Balkau, B. Waist circumference and the metabolic syndrome predict the development of elevated albuminuria in non-diabetic subjects: The DESIR Study. J. Hypertens. 2006, 24, 1157–1163. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.-T.; Huang, J.-W.; Chiang, C.-K.; Yen, C.-J.; Hung, K.-Y.; Wu, K.-D. Metabolic syndrome and insulin resistance as risk factors for development of chronic kidney disease and rapid decline in renal function in elderly. JECM 2012, 97, 1268–1276. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- World Health Organization. BMI Classification. Global Database on Body Mass Index: An Interactive Surveillance Tool for Monitoring Nutrition Transition; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- WHO Expert Consultation. Waist Circumference and Waist-Hip Ratio; Report of a WHO Expert Consultation Geneva; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Kdigo CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar]
- Alberti, G.; Zimmet, P.; Shaw, J.; Grundy, S. IDF Worldwide Definition of the Metabolic Syndrome; International Diabetes Federation (IDF): Brussels, Belgium, 2006; Volume 1. [Google Scholar]
- Wen, M.J.; Hsieh, C.H.; Wu, C.Z.; Hsiao, F.C.; Hsia, T.L.; Hung, Y.J.; Pei, D. The adipokines and inflammatory marker in young type 2 diabetics with metabolic syndrome: A pilot study. Obes. Res. Clin. Pract. 2013, 7, e206–e210. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, S.; Saito, I.; Yamamoto, S.; Miyake, T.; Ueda, T.; Niiya, T.; Torisu, M.; Kumagi, T.; Sakai, T.; Minami, H. Nocturnal intermittent hypoxia as an associated risk factor for microalbuminuria in Japanese patients with type 2 diabetes mellitus. Eur. J. Endocrinol. 2013, 169, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, S.; Sakai, T.; Niiya, T.; Miyaoka, H.; Miyake, T.; Yamamoto, S.; Tanaka, K.; Ueda, T.; Senba, H.; Torisu, M. B-type natriuretic peptide and renal function in Japanese patients with type 2 diabetes mellitus: The Dogo Study. Endocr. J. 2017, 64, 1131–1136. [Google Scholar] [CrossRef] [PubMed]
- Tozawa, M.; Iseki, K.; Iseki, C.; Oshiro, S.; Ikemiya, Y.; Takishita, S. Triglyceride, but not total cholesterol or low-density lipoprotein cholesterol levels, predict development of proteinuria. Kidney Int. 2002, 62, 1743–1749. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Kong, X.; Jia, X.; Li, W.; Wang, Z.; Cui, M.; Xu, D. Association between metabolic syndrome and chronic kidney disease in a Chinese urban population. Clin. Chim. Acta 2017, 470, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Wisse, B.E. The inflammatory syndrome: The role of adipose tissue cytokines in metabolic disorders linked to obesity. J. Am. Soc. Nephrol. 2004, 15, 2792–2800. [Google Scholar] [CrossRef] [PubMed]
- Liao, M.-T.; Sung, C.-C.; Hung, K.-C.; Wu, C.-C.; Lo, L.; Lu, K.-C. Insulin resistance in patients with chronic kidney disease. J. Biomed. Biotechnol. 2012, 691369, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Lerman, L.O. The metabolic syndrome and chronic kidney disease. Transl. Res. 2017, 183, 14–25. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.C.; Chang, H.Y.; Huang, M.C.; Hwang, S.J.; Yang, Y.C.; Tai, T.Y.; Yang, H.J.; Chang, C.T.; Chang, C.J.; Li, Y.S. Association between insulin resistance and development of microalbuminuria in type 2 diabetes: A prospective cohort study. Diabetes Care 2011, 34, 982–987. [Google Scholar] [CrossRef] [PubMed]
- Gluba, A.; Mikhailidis, D.; Lip, G.Y.H.; Hannam, S.; Rysz, J.; Banach, M. Metabolic syndrome and renal disease. Int. J. Cardiol. 2013, 164, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Michishita, R.; Matsuda, T.; Kawakami, S.; Tanaka, S.; Kiyonaga, A.; Tanaka, H.; Morito, N.; Higaki, Y. Hypertension and hyperglycemia and the combination there of enhances the incidence of chronic kidney disease (CKD) in middle-aged and older males. Clin. Exp. Hypertens. 2017, 7, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Kurata, M.; Tsuboi, A.; Takeuchi, M.; Fukuo, K.; Kazumi, T. Association of Metabolic Syndrome with Chronic Kidney Disease in Elderly Japanese Women: Comparison by Estimation of Glomerular Filtration Rate from Creatinine, Cystatin C, and Both. Metab. Syndr. Relat. Disord. 2016, 14, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.; Zimmet, P.; Shaw, J.; IDF Epidemiology Task Force Consensus Group. The metabolic syndrome—A new worldwide definition. Lancet 2005, 366, 1059–1062. [Google Scholar] [CrossRef]
- Fan, A.Z.; Russell, M.; Dorn, J.; Freudenheim, J.L.; Nochajski, T.; Hovey, K.; Trevisan, M. Lifetime alcohol drinking pattern is related to the prevalence of metabolic syndrome. The Western New York Health Study (WNYHS). Eur. J. Epidemiol. 2006, 21, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Djousse, L.; Arnett, D.K.; Eckfeldt, J.H.; Province, M.A.; Singer, M.R.; Ellison, R.C. Alcohol consumption and metabolic syndrome: Does the type of beverage matter? Obes. Res. 2004, 12, 1375–1385. [Google Scholar] [CrossRef] [PubMed]
- Koppes, L.L.; Dekker, J.M.; Hendriks, H.F.; Bouter, L.M.; Heine, R.J. Moderate alcohol consumption lowers the risk of type 2 diabetes: A meta-analysis of prospective observational studies. Diabetes Care 2005, 28, 719–725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xin, X.; He, J.; Frontini, M.G.; Ogden, L.G.; Motsamai, O.I.; Whelton, P.K. Effects of alcohol reduction on blood pressure: A meta-analysis of randomized controlled trials. Hypertension 2001, 38, 1112–1117. [Google Scholar] [CrossRef] [PubMed]
- Kato, I.; Kiyohara, Y.; Kubo, M.; Tanizaki, Y.; Arima, H.; Iwamoto, H.; Shinohara, N.; Nakayama, K.; Fujishima, M. Insulin-mediated effects of alcohol intake on serum lipid levels in a general population: The Hisayama Study. J. Clin. Epidemiol. 2003, 56, 196–204. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Frequency in Number of Patients |
|---|---|
| Gender (males/females) | 77/72 |
| BMI (<25/>25) | 12/137 |
| Waist circumference (<80 or 94/>80 or 94) | 11/138 |
| Hypertension (yes/no) | 132/17 |
| Smoking (yes/no) | 29/120 |
| Alcohol intake (yes/no) | 42/107 |
| Physical activity (yes/no) | 49/100 |
| Family history of cardiovascular events (yes/no) | 116/33 |
| Prevalence of MetS (yes/no) | 120/29 |
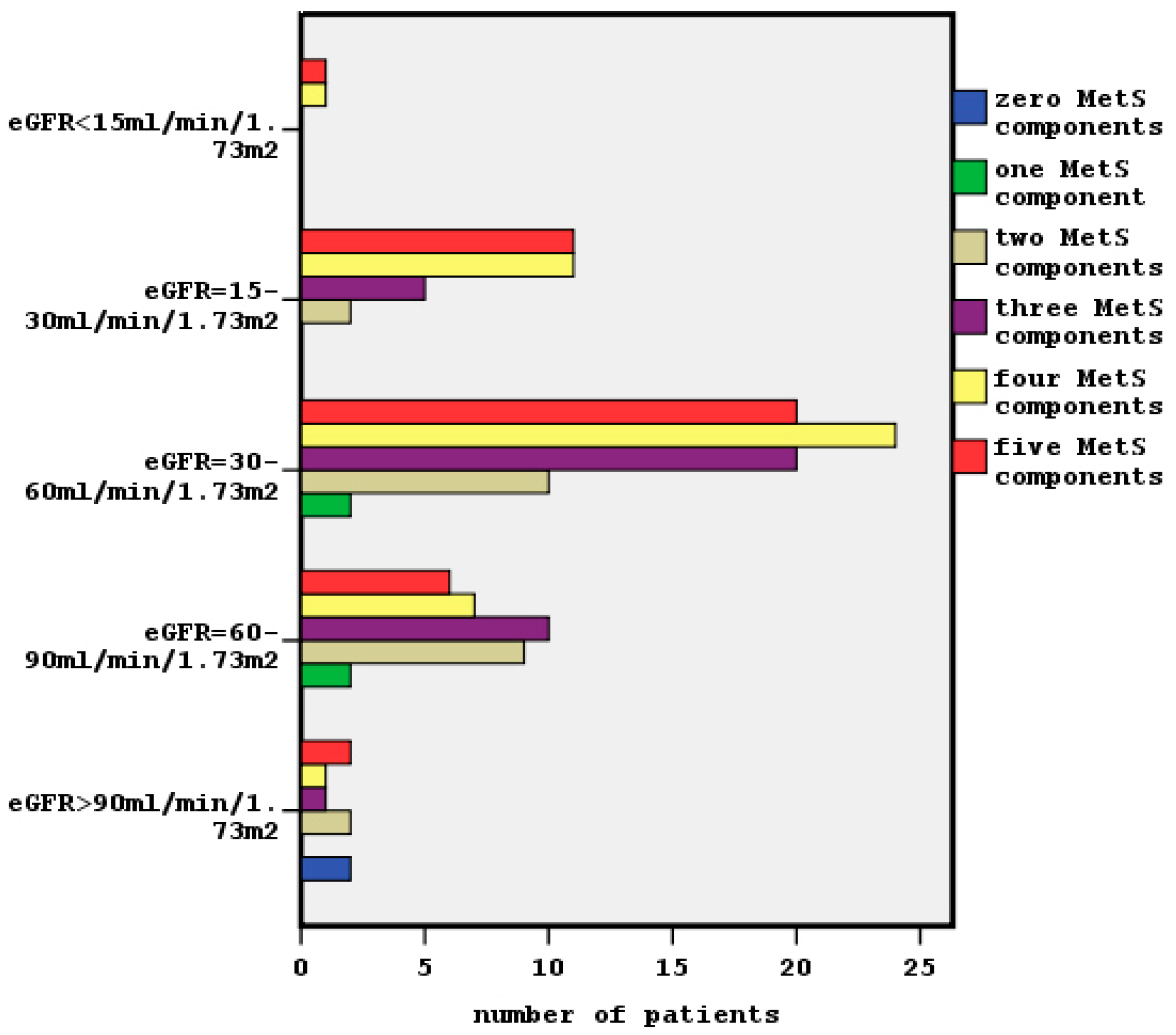
| Clustering of MetS (0 to 5 components) | 2/4/23/36/44/40 |
| Underlying disease: | |
| diabetes mellitus | n = 36 |
| Hypertension | n = 75 |
| Chronic glomerulonephritis | n = 8 |
| Interstitial nephritis | n = 8 |
| Polycystic disease | n = 4 |
| Other/unknown | n = 18 |
| Characteristic | Frequency in Number of Patients |
|---|---|
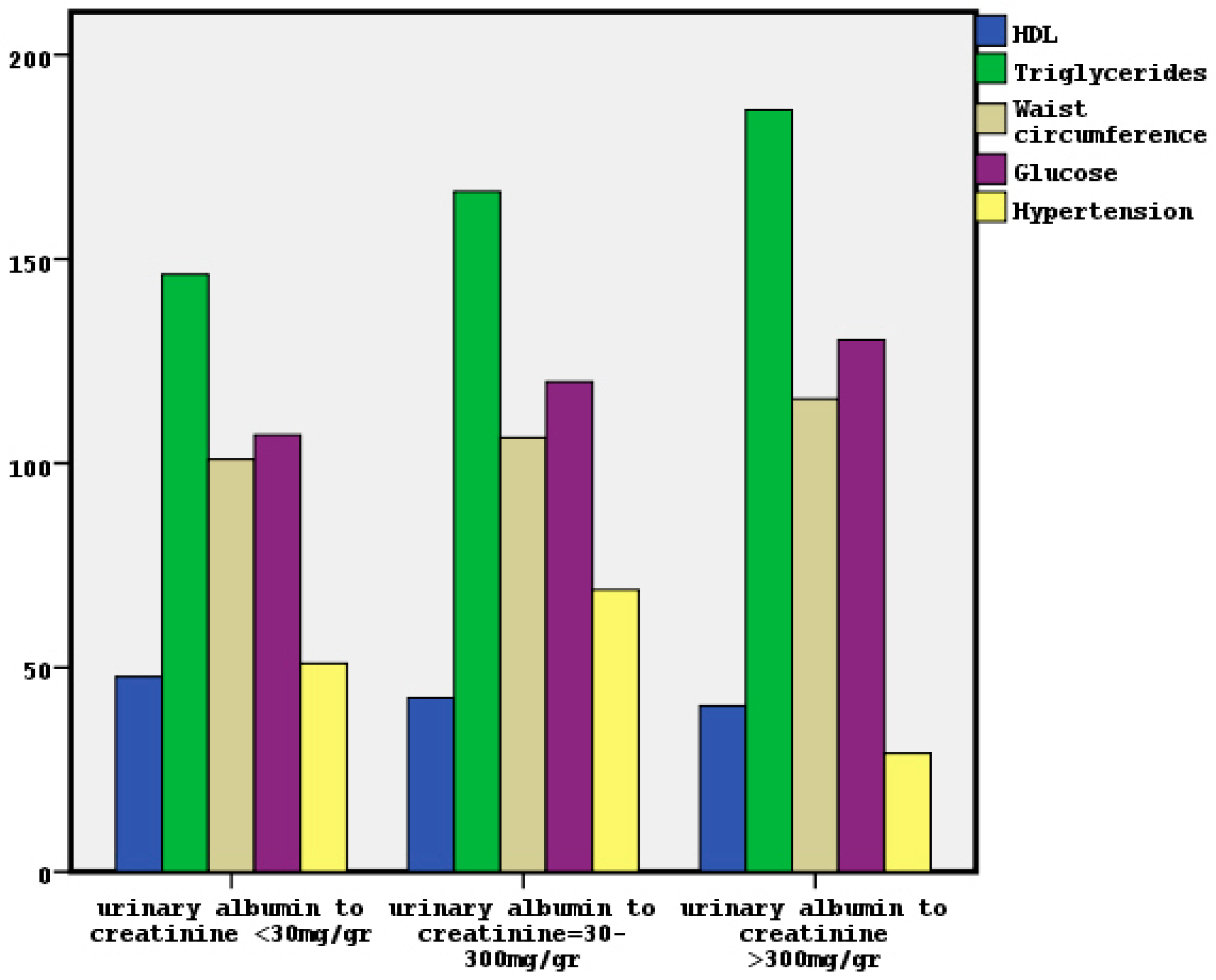
| HDL-C (>40 or 50/<40 or 50) | 72/77 |
| Triglycerides (<150/>150) | 60/89 |
| Glucose (<100/>100) | 50/99 |
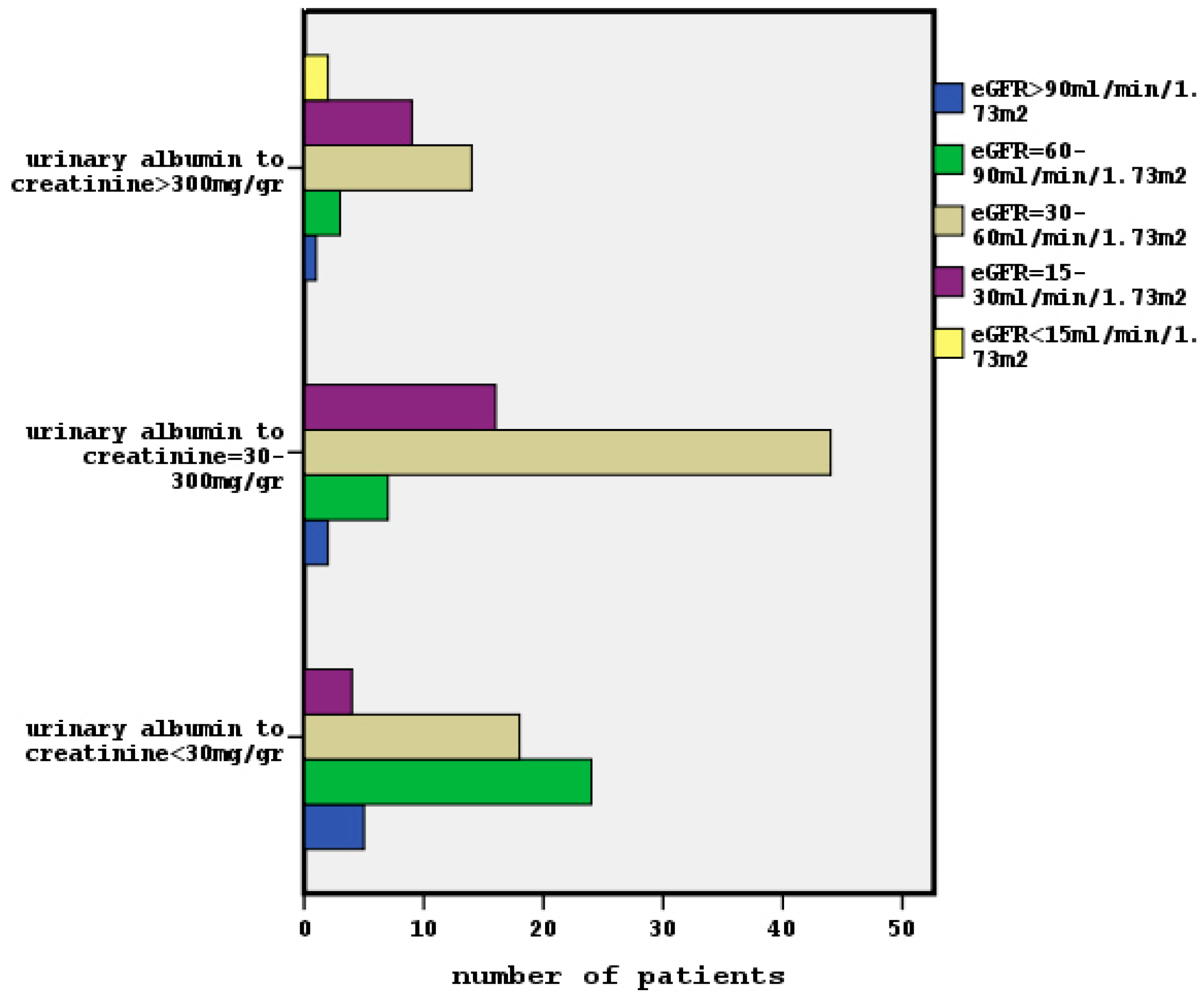
| ACR (<30/>30 mg/gr) | 51/98 |
| Classified albuminuria: | |
| A1: ACR < 30 mg/gr | n = 51 |
| A2: ACR = 30–300 mg/gr | n = 69 |
| A3: ACR > 300 mg/gr | n = 29 |
| eGFR < 60 mL/min/1.73 m2 (yes/no) | 107/42 |
| Classified eGFR: | |
| G1: eGFR > 90 mL/min/1.73 m2 | n = 8 |
| G2: eGFR = 60–90 mL/min/1.73 m2 | n = 34 |
| G3: eGFR = 30–60 mL/min/1.73 m2 | n = 76 |
| G4: eGFR = 15–30 mL/min/1.73 m2 | n = 29 |
| G5: eGFR <15 mL/min/1.73 m2 | n = 2 |
| Characteristic | Patients with MetS (n = 120) Mean ± SD/Mean Rank | Patients without MetS (n = 29) Mean ± SD/Mean Rank | p Value |
|---|---|---|---|
| Sex (%males/%females) | 55 (45.8%)–65 (54.2%) * | 22(75.9%)–7 (24.1%) | 0.003 |
| Age (years) | 70.8 ± 13.5 | 64.0 ± 18.05 | 0.06 |
| BMI (Kg/m2) | /81.1 * | /49.5 | 0.001 |
| eGFR (mL/min/1.73 m2) | 45.1 ± 19.2 * | 58.4 ± 23.7 | 0.002 |
| Classified eGFR: * | |||
| G1: eGFR > 90 mL/min/1.73 m2 | 4 (50%) | 4 (50%) | |
| G2: eGFR = 60–90 mL/min/1.73 m2 | 23 (67.6%) | 11 (32.4%) | |
| G3: eGFR = 30–60 mL/min/1.73 m2 | 64 (84.2%) | 12 (15.8%) | 0.01 |
| G4 :eGFR = 15–30 mL/min/1.73 m2 | 27 (93.1%) | 2 (6.9%) | |
| G5 :eGFR < 15 mL/min/1.73 m2 | 2 (100%) | 0 (0%) | |
| ACR (mg/gr) | /79.6 * | /55.8 | 0.008 |
| Classified albuminuria: * | |||
| A1: ACR < 30 mg/gr | 34 (66.7%) | 17 (33.3%) | |
| A2: ACR = 30–300 mg/gr | 59 (85.5%) | 10 (14.5%) | 0.006 |
| A3: ACR > 300 mg/gr | 27 (93.1%) | 2 (6.9%) | |
| Underlying disease: * | |||
| - diabetes mellitus | 36 (100%) | 0 (0%) | |
| - Hypertension | 60 (80%) | 15 (20%) | |
| - Chronic glomerulonephritis | 6 (75%) | 2 (25%) | |
| - Interstitial nephritis | 5 (62.5%) | 3 (37.5%) | 0.003 |
| - Polycystic disease | 3 (75%) | 1 (25%) | |
| - Other/unknown | 10 (55.6%) | 8 (44.4%) | |
| Family cardiovascular history (yes/no) | 88 (73.3%)/32 (26.7%) * | 28 (96.6%)/1 (3.4%) | 0.003 |
| Characteristic | p-Value | Odds Ratio | Confidence Interval |
|---|---|---|---|
| Age * | 0.001 | 1.07 | 1.04–1.11 |
| Gender * | 0.02 | 0.3 | 0.1–0.9 |
| smoking | 0.2 | 0.4 | 0.1–1.3 |
| Alcohol intake | 0.9 | 0.9 | 0.3–2.7 |
| Physical activity | 0.5 | 0.7 | 0.3–1.9 |
| presence of MetS * | 0.006 | 5.3 | 1.6–17.8 |
| Diabetes mellitus | 0.9 | 0.93 | 0.3–2.8 |
| Characteristic | p-Value | Odds Ratio | Confidence Interval |
|---|---|---|---|
| age | 0.07 | 1.02 | 0.9–1.05 |
| gender | 0.1 | 0.5 | 0.2–1.1 |
| smoking | 0.9 | 0.95 | 0.3–2.6 |
| Alcohol intake | 0.4 | 1.5 | 0.6–3.9 |
| Physical activity | 0.3 | 0.6 | 0.2–1.5 |
| presence of MetS * | 0.02 | 3.2 | 1.2–8.8 |
| Diabetes mellitus * | 0.03 | 3.5 | 1.1–11.3 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raikou, V.D.; Gavriil, S. Metabolic Syndrome and Chronic Renal Disease. Diseases 2018, 6, 12. https://doi.org/10.3390/diseases6010012
Raikou VD, Gavriil S. Metabolic Syndrome and Chronic Renal Disease. Diseases. 2018; 6(1):12. https://doi.org/10.3390/diseases6010012
Chicago/Turabian StyleRaikou, Vaia D., and Sotiris Gavriil. 2018. "Metabolic Syndrome and Chronic Renal Disease" Diseases 6, no. 1: 12. https://doi.org/10.3390/diseases6010012
APA StyleRaikou, V. D., & Gavriil, S. (2018). Metabolic Syndrome and Chronic Renal Disease. Diseases, 6(1), 12. https://doi.org/10.3390/diseases6010012