The results are organized in two subsections, the first of which provides summary statistics describing the variables, while the second presents the results of the Pairwise Maximum Composite Likelihood estimation of the multivariate ordinal regression model (MVORM).
5.2. Econometric Results
For sensitivity and comparative model performance analysis, we have estimated both the multivariate ordered probit and multivariate ordered logit specifications of our Econometric model described in
Section 4.1.
Table A6 shows the performance indicators from the estimations of the two model specifications. Based on both, the Akaike (CLAIC) and Bayesian (CLBIC) composite likelihood information criteria, the multivariate logit model appears to have a relatively better performance. Indeed its CLAIC value of 16,345.22 is lower than that of the probit specification at 16,346.81; and similarly for its CLBIC =17,444.64, which is also lower than that of the probit specification at 17,445.57. Therefore, we choose the multivariate logit model as our preferred specification, the results of which are summarized in
Table A7, and presented in the next sub-section.
Recall however from the discussions in
Section 4.1 that we achieved identification in our current application by leaving the intercept terms
and
unrestricted, while fixing the first threshold parameter in each of the three outcomes (i.e.,
). As the results in the upper part of
Table A6 show, all estimated threshold parameters/cutoff points (for the first outcome variable
;
;
are statistically significant at an alpha of 0.1%.
Moreover, the estimated intercept terms in
Table A6 show that
and
are statistically significant, while
is not. The implications of these negative intercept values are that irrespective of any influencing factors, the expected process of acquiring the COVID-19 vaccine based immunization is associated with a dis-utility for the average individual. More specifically,
, suggests an expected 2.131 increased dis-utility along the vaccine continuum, for the average individual seeking the COVID-19 vaccine. Similarly,
suggests an average expected 176 AED increased dis-utility for every 100 AED increased spending to get the COVID-19 vaccine. Though the results also point out a dis-utility from the time spent getting the vaccine (
), this opportunity cost driven dis-utility is not statistically significant. These results seem to suggest that all things being equal, the average individual would have rather preferred not to deal with the novel coronavirus disease, and the need to protect oneself from it, through vaccination. A finding quite natural, given that by its very nature a “dis”- ”ease” of any kind, including that brought by the SARS-CoV-2 virus is always utility depleting, while vaccine based immunization is, at least theoretically utility improving. Individuals’ perceptions of the interplay of these two utility forces, eventually shape their subjective preferences for the vaccines.
5.2.1. The Endogeneity Test for Time and Money Willing to Spend for COVID-19 Vaccine
Recall from the discussions of our random utility model of stated vaccine preferences analysis developed in
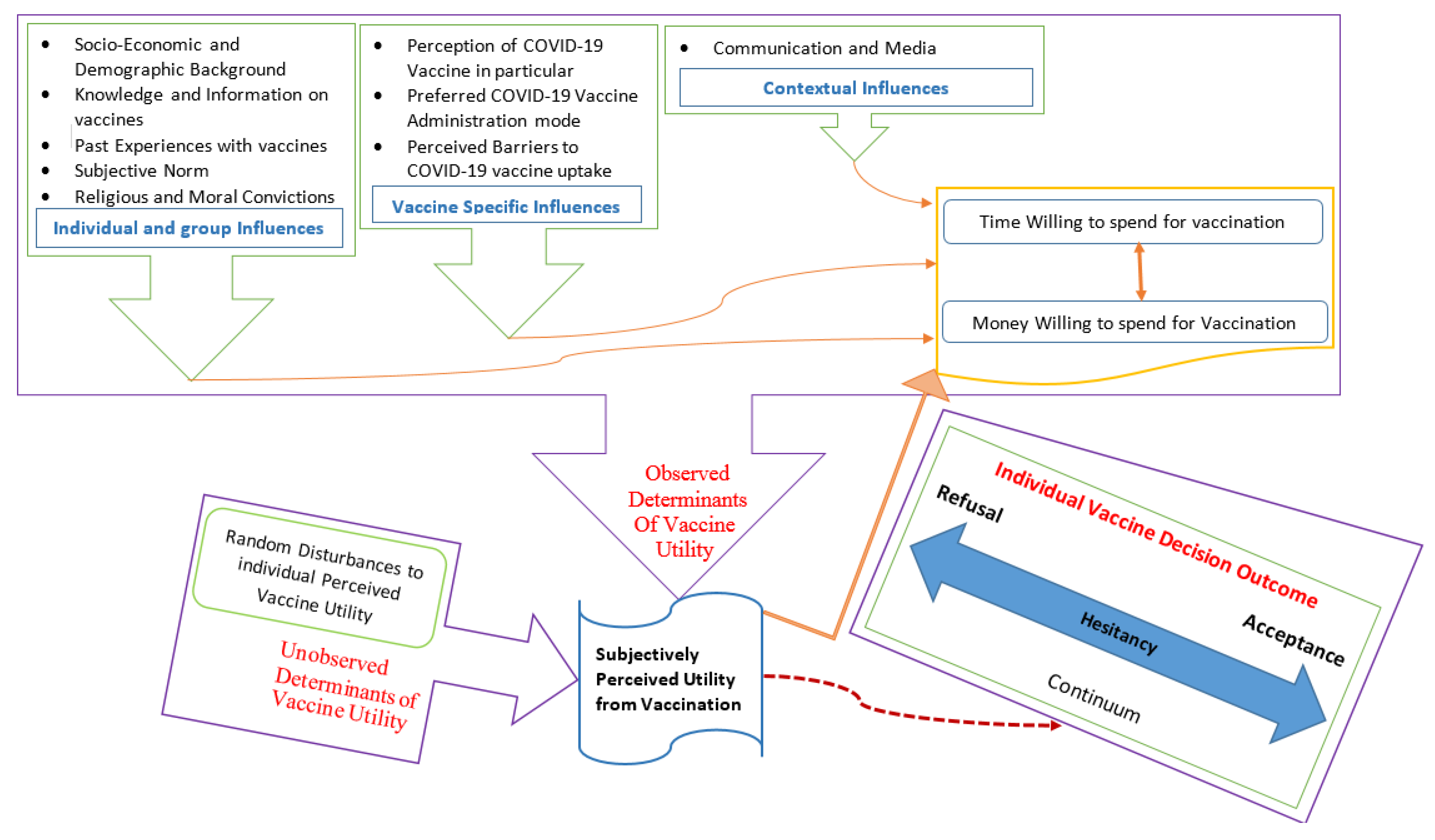
Section 4, that the observed component part of COVID-19 vaccine utility is assumed to be an indirect differentiable continuous and endogenous function of individuals’ willingness to spend time and money to get vaccinated [See observed determinants in orange,
Figure 1], but an exogenous function of the remaining identified vaccine demand determinants [See observed determinants in green,
Figure 1].
This endogeneity assumption has led to the joint modeling of the three processes in an endogeneity switching regression framework [
70], to allow for the potential correlations between their generated error terms
=
, in order to avoid potential biases from not accounting for such correlations. Testing for the validity of this assumption post-estimation, is achieved by evaluating the statistical significance of the estimated correlation coefficients [
71]. As shown in the bottom part of
Table A6, all three coefficients Corr
; Corr
; and Corr
are indeed statistically significant at an alpha of 0.1%, suggesting that the unobserved factors affecting individuals’ reported COVID-19 vaccine preferences, depend significantly on those influencing their willingness to spend time, and those influencing their willingness to spend money to get the COVID-19 vaccine. Thus, validating our hypothesized endogeneity of these latter two determinant factors of COVID-19 vaccine preference.
5.2.2. The Impact of Economic and Socio-Demographic Influences
Though age significantly affect individuals’ willingness to get the COVID-19 vaccine (−0.163); it does not appear to significantly influence the maximum time, nor money they are willing to spend for their chosen vaccine preferences. Indeed, aging appears to be a significant contributing factor of COVID-19 vaccine hesitancy, since expected utility appears to decrease by 16.3%, across each increasing age category. In addition, no significant gender based differences exist in individuals’ COVID-19 vaccine preferences in the UAE.
Though no significant difference exist also between married and unmarried individuals in their willingness to get the COVID-19 vaccine, nor the maximum amount of time they are willing to spend on this process, our findings show however that married individuals are relatively less willing to spend money to get the COVID-19 vaccine. Indeed, the expected utility from every 100 AED increased spending on COVID-19 vaccine is 61.7% lower for married individuals, compared to their unmarried counterparts. This finding seems to suggest that perhaps relatively speaking married individuals have greater subjectively perceived total out-of-pocket immunization expense requirements for the whole family, which leads them to prefer a lower family per-capita prospective cost of COVID-19 immunization. In other words, because unmarried individuals may perhaps just have to pay for themselves alone, their expected lower budgetary burden of COVID-19 immunization leads them to have a higher individual willingness to pay for the COVID-19 vaccine.
The estimated effects of nationality show a significant difference in COVID-19 vaccine preferences between locals and non-locals of the UAE. In fact, non-locals appear to exhibit more COVID-19 vaccine hesitancy (less willingness to get the vaccine), with an expected relative dis-utility of 68.2% from COVID-19 vaccine uptake, than to their local counterparts. However, non-locals show relatively 41.7% higher expected utility from every 30 min increase in the time spent acquiring the COVID-19 vaccine, but a 50.1% lower expected utility from every 100 AED increase spending on the COVID-19 vaccine. These findings suggest that compared to their local counterparts, non-locals are relatively more willing to spend their time, but less willing to spend their money to get the COVID-19 vaccine. Economically, these results seem to further suggest that UAE locals have a relatively higher perceived opportunity cost of their time than non-locals, while non-locals have a relatively higher perceived opportunity cost of their money than their local counterparts.
Education seems to have varying effects on individuals’ preferences for COVID-19 vaccine in the UAE. In fact, no significant difference in COVID-19 vaccine preferences (willingness to get the vaccine) exist between those with at most a high school degree, and those with a two year diploma. However, individuals with a graduate degree are seen to exhibit significantly more vaccine confidence, and more willingness to pay for the COVID-19 vaccine, than their counterparts with at most a high school degree. Indeed, the results show a relative 37.1% higher expected utility from COVID-19 vaccine uptake for individuals with a graduate degree, and a relative 39.8% higher expected utility from every 100 AED increase spending on the vaccine. Taking into account the estimated results for individuals with a post-graduate degree, our findings seem to suggest that increased levels of education lead to stronger preferences for COVID-19 vaccine immunization in the UAE. Indeed, we find that compared to individuals with at most a high school degree, those with a postgraduate degree have 45.5% higher expected utility from COVID-19 vaccine based immunity. They also have a relative 70.3% higher expected utility from every 30 min spent acquiring the COVID-19 vaccine, and a 53.4% higher expected utility from every 100 AED spent on the vaccine.
The impact of occupation is only significant for individuals’ willingness to get the vaccine (−0.365), for those working in governmental or semi-governmental institutions; however, it does not appear to significantly influence the maximum time, nor money individuals are willing to spend on their expressed vaccine preference. Indeed, compared to the individuals that are not working, those working in governmental or semi-governmental institutions appear show more COVID-19 vaccine hesitancy, with a relative 36.5% lower expected utility. Conversely however, self-employed or privately employed individuals appear to show no significant differences in willingness to get the COVID-19 vaccine, compared to those not working.
The impact of monthly income on individuals’ COVID-19 vaccine preferences in much more decisive. Indeed, for every 1000 EAD increase in monthly income, it can be noted that expected utility from COVID-19 vaccination increases by 26%, while the expected utility of each unit of time (every 30 min) and money (every 100 AED) spent on getting the COVID-19 vaccine increases by 19.1% and 29.8%, respectively. These results suggest a general perception of the COVID-19 vaccine as a “normal good”, since rising income increases individuals’ willingness to get the vaccine in the UAE. Putting these findings within the context of our above discussions with the intercept terms (where it was suggested that individuals’ perceptions of the interplay between the utility depleting COVID-19 disease, and its at least theoretically utility improving corresponding vaccine, would eventually shape their subjective preferences for the COVID-19 vaccines), the fact that the vaccine is perceived as a normal good, provides an empirical support for the theoretical utility improving proposition in our target population. Because increased income appear to reduce both the perceived opportunity cost of time and money spent on COVID-19 vaccine demand, all things being equal, if the prospective vaccine were to be affordable (whether free of charge or at a reduced fee), the prevailing outcome should be its general uptake in the UAE, contributing to creating the needed herd immunity, required to eradicate the disease from the UAE community.
The results from the place of residence suggest no significant difference in individuals expected utility from getting the vaccine, nor difference in expected utility from money spent doing so, across the different Emirates. However, a significant difference in expected utility from time spent getting the vaccine is observed between the different Emirates. In fact, Abu Dhabi and Dubai residents show 40.7% and 76.1%, respectively, higher expected utility from every prospective 30 min spent getting the COVID-19 vaccine, compared to residents of the remaining five Emirates. These spatial differentials in willingness to spend time in getting the vaccine may be due to the spatial differences in the impact of the COVID-19 pandemic, with the resulting differential measures that were implemented locally in each Emirate to curb to pandemic. Although restrictive measures were implemented nationwide, the sizes and strategic roles of the two Emirates of Abu Dhabi and Dubai as the federal capital and the tourism capital respectively, provided their residents with unique experiences during the COVID-19 pandemic, all of which contributed to shaping the spatial heterogeneity in perceived vaccine opportunity cost in the country.
5.2.3. The Impact of Personal and Peer Influences
The estimated individual and group specific influences on ones vaccine’s preferences are summarized in the mid-portion of
Table A6. It can be noted that the individuals reporting to be knowledgeable about vaccines highlight relatively more COVID-19 vaccine hesitancy (less willingness to get the vaccine), than their counterpart who do not. More specifically, they show a 29.2% higher expected dis-utility from COVID-19 vaccine based immunization than those reporting not knowing about vaccines. This finding seems to suggest that the information received by those reporting to knowing about vaccines, is perhaps of unfavorable nature. Indeed, the literature on general vaccine hesitancy has repeatedly shown the importance of the quality of vaccine information in the media, in shaping vaccine acceptance/refusal [
10,
12]. Both the rising prevalence of vaccine hesitancy, and anti-vaccine movement observed in different parts of the world, have been credited in the literature to misinformation on vaccines and their safety [
49]. This situation has led [
57] to propose good practices in developing sensitive communications that take into account the complexity of the cognitive processing and valuation of information for optimal community level vaccine uptake.
Indeed, of the 1109 study participants in the present analysis, 650 (58.61%) reported not getting enough information on vaccines and their safety, with only 209 (18.85%) identifying as “anti-vaxxer”, against 900 (81.15%) who identified themselves otherwise [
59], suggesting perhaps a low prevalence of anti-vaccine sentiments in the UAE. Our econometric findings however show no significant difference in vaccine hesitancy between those reporting to getting enough information on vaccine safety, and their counterparts reporting not. Conversely however, compared to those not getting enough information on vaccines and their safety, those reporting to getting such information show relatively 28.9% and 25.5% lower expected utility from each unit of time (every 30 min) and money (every 100 AED) spent on acquiring the COVID-19 vaccine. Thus, confirming further, the critical nature of the quality of vaccine communications in insuring better vaccine perception and uptake. Hence, building on the recommendations by [
57] to ensure general vaccine confidence, the fact that our findings show relatively more COVID-19 vaccine hesitancy and lower expected utility among individuals reporting to being knowledgeable about vaccines, suggest that future communications by UAE health authorities in relation to the prospective COVID-19 vaccine could benefit from (i) establishing trust, (ii) providing both the risks and benefits of the COVID-19 vaccine, (iii) giving the facts before addressing the myths, (iv) using visual aids, and finally (v) testing alternative communication materials prior to launching the COVID-19 vaccination program in the UAE.
With regards to respondents’ past experience with vaccines, our econometric results show no significant difference in vaccine hesitancy, nor willingness to spend time getting the COVID-19 vaccine between individuals with prior vaccine refusals, and those without. However, it can be noted that individuals with prior vaccine refusal show a significant 27.7% lower expected utility from each 100 AED increase spending on getting the COVID-19 vaccine. These findings suggest that individuals with prior vaccine refusals are not necessarily more hesitant towards, nor unwilling to get vaccinated against the coronavirus disease, but perhaps are relatively more cost sensitive/financially constrained; a situation that may contribute to impeding their COVID-19 vaccine uptake. Given that this group represent 24.80% of our studied sample, and that herd immunity are reported at around 75% effective vaccine coverage in the population, ensuring COVID-19 vaccine affordability (whether free of charge, or at a significantly reduced fee) in the UAE, would be key to ensuring the effectiveness of the prospective COVID-19 vaccine program, in eradicating the pandemic from the general population.
Similarly, our econometric results show no significant difference in vaccine hesitancy, nor willingness to spend time getting the COVID-19 vaccine between individuals with prior knowledge of a bad vaccine reaction, and those without. However, it can be noted that those reporting to have such prior knowledge of someone with a bad vaccine reaction still paradoxically exhibit 45.2% more expected utility from each 100 AED increase spending on acquiring the COVID-19 vaccine. This paradoxical finding seems to suggest that knowing someone that has had an adverse reaction to a vaccine, does not necessarily discourage individual financial investment to acquiring vaccine based immunity, but rather seem to contribute to the individual being willing to invest more money, perhaps to get a quality vaccine with better perceived safety.
With regards to the perceived subjective norm of the COVID-19 vaccine, our econometric findings show that the stronger one believes that everyone should get the vaccine once available, the more accepting one is of the COVID-19 vaccine for oneself, and the greater one’s willingness to spend time, and also money in acquiring the COVID-19 vaccine. More specifically, each level increase in such belief appears to raise individuals’ expected utility from COVID-19 vaccination by 66.6%; while raising their expected utility from time (every 30 min) and money (every 100 AED) spent by 39.1% and 65.5%, respectively. These latter findings seem to suggest that the UAE’s prospective COVID-19 vaccination program could benefit further in effectiveness, by leveraging socio-collective values in the UAE community, through COVID-19 vaccine communications that highlight individuals’ inter-dependence in resolving the COVID-19 pandemic in the nation.
On the impact of religious and moral convictions on individuals’ COVID-19 vaccine preferences, it can be noted from
Table A6 that religious or moral convictions do not significantly determine differences in vaccine hesitancy, nor willingness to spend time, nor money in getting the COVID-19 vaccine in the UAE. However, individuals perceiving such convictions based vaccine refusal as health risks exhibit relatively 22% higher expected utility from every 30 min spent getting the COVID-19 vaccine. This latter finding seems to suggest that risk perception is indeed a significant motivator of COVID-19 vaccine seeking behavior in the UAE, in terms of the time the average person is willing to spend to get vaccinated.
5.2.4. The Impact of Contextual and Vaccine Specific Influences
The results of the impact that COVID-19 information source has on vaccine demand suggest no significant differences in vaccine hesitancy, nor willingness to spend time, nor money in getting the COVID-19 vaccine, across the various sources of COVID-19 information in the UAE. These findings seem to suggest that irrespective of whether COVID-19 messages are communicated through government websites, the general internet, or other channels of communications, the medium through which the information is transmitted is not as important as the quality of the message in insuring successful vaccine uptake.
Our findings show however that perceived COVID-19 vaccine importance significantly raises COVID-19 vaccine acceptance, as well as individuals willingness to spend time, and money in acquiring the vaccine. Indeed, every level increase in perceived vaccine importance raises by 38.8% individuals expected utility from COVID-19 vaccine uptake, In addition to raising by 41.2% and 32.4%, respectively the expected utility from each unit of time (every 30 min) and money (every 100 AED) spent getting vaccinated. With respect to individuals’ concerns about the COVID-19 vaccine, it can be noted that while increased levels of concerns about the vaccine significantly raises COVID-19 vaccine acceptance, it reduces however individuals willingness to spent time, while leaving unaffected their willingness to spend money to acquire the COVID-19 vaccine. Indeed, each increased level of concern for the vaccine is seen to raises by 13.6% individuals expected utility from COVID-19 vaccine uptake, while reducing by 17% the expected utility from every 30 min spent getting vaccinated.
Our results further show that the administration mode of the prospective COVID-19 vaccine is a significant determinant of individuals’ vaccine demand. In fact, compared to those that prefer not to get vaccinated, those that prefer oral administration, injection and nasal spray of the vaccine all show greater expected utility from COVID-19 vaccine uptake, and are also relatively more willing to spent time and money to get the vaccine. Indeed, the results show that compared to those preferring not to get vaccinated, those that prefer oral administration, injection and nasal spray of the COVID-19 vaccine exhibit 59.2%, 69.5% and 61.7% higher expected utility from COVID-19 vaccine uptake, respectively. Similarly, compared to those preferring not to get vaccinated, those preferring oral administration, injection and nasal spray of the COVID-19 vaccine exhibit 64.6%, 54.6% and over 100% higher expected utility from every 100 AED spent on getting the vaccine, respectively. Moreover, while those with oral administration shown no significant difference with their counterparts that prefer not to get vaccinated, compared to member of the latter group, individuals preferring injection and nasal spray of the prospective COVID-19 vaccine show 54.7% and 97.9%, respectively, higher expected utility from every 30 min spent getting vaccinated.
On the influences of perceived barriers to COVID-19 vaccine uptake, it can be noted that financial, temporal and spatial constraints significantly shape COVID-19 vaccine preferences in the UAE. Indeed, starting with the financial constraint, it can be noted that compared to individuals reporting the financial cost of the prospective COVID-19 vaccine to not be a potential barrier to their vaccine uptake, those reporting such barrier show over 100% lower expected utility from COVID-19 vaccine uptake, with a significant 95.1% lower expected utility from every 100 AED spent on getting the vaccine. Moving to the temporal constraint, it can be noted that compared to the individuals that are unwilling, those reporting to being willing to travel over an hour to get the COVID-19 vaccine do exhibit 75% higher expected utility from COVID-19 vaccine uptake, with respectively 59.7% and 47.7% higher expected utility from every 30 min, and every 100 AED spent on getting vaccinated. A similar pattern is observed with the spatial constraint, where compared to the individuals that are unwilling to travel to a different emirate to get the vaccine if not available in their immediate emirate of residence, those reporting to being willing to travel do exhibit 63.3% higher expected utility from COVID-19 vaccine uptake, with respectively 47.7% and 74.2% higher expected utility from every 30 min, and every 100 AED spent traveling to another emirate to get the COVID-19 vaccine.
Given that for all three perceived barriers, the constraints are binding for at least 33% of the study participants, the required 75% effective immunization coverage for herd immunity may be compromised if mitigating measures are not put in place to overcome the perceived financial, temporal and spatial constraints to vaccine uptake. A situation most likely to also compromise the efforts of any prospective COVID-19 vaccine program in the country. Potential mitigating measures of these perceived barriers could include: (i) ensuring the availability of the vaccine locally in each Emirate to reduce/eliminate the need for cross-Emirate travels to get vaccinated (to circumvent the spatial constraint); (ii) within each emirate, ensuring also the geographical distribution of vaccines across health centers to reduce the travel time to get the vaccine (to circumvent the temporal constraint); and finally (iii) ensuring that the available vaccine is also financially affordable to the average person, whether free of charge or at a reduced fee (to circumvent the financial constraint). Our results suggest that taking such measures would contribute to the overall effectiveness of the prospective COVID-19 vaccination program in the UAE, and therefore help eradicate the COVID-19 pandemic from the country.




{kind=link}
