
The Use of Off-Label Medications in Newborn Infants Despite an Approved Alternative Being Available—Results of a National Survey


Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey of Clinical Practice in German Perinatal Centers
2.2. Analysis of EMA’s EPARs
2.3. Drug Price Comparison
2.4. Ethical Review Board (ERB) Approval
3. Results
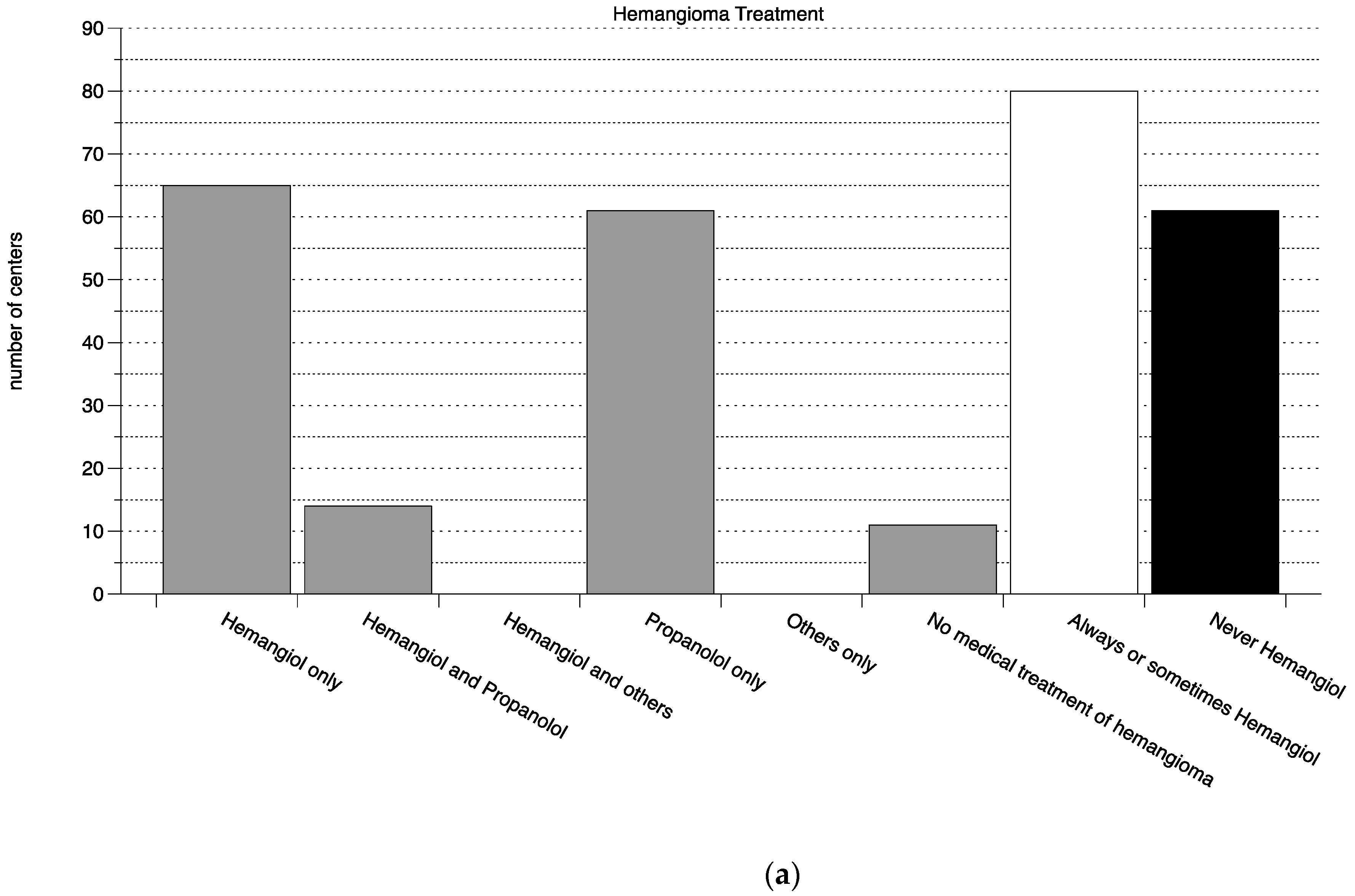
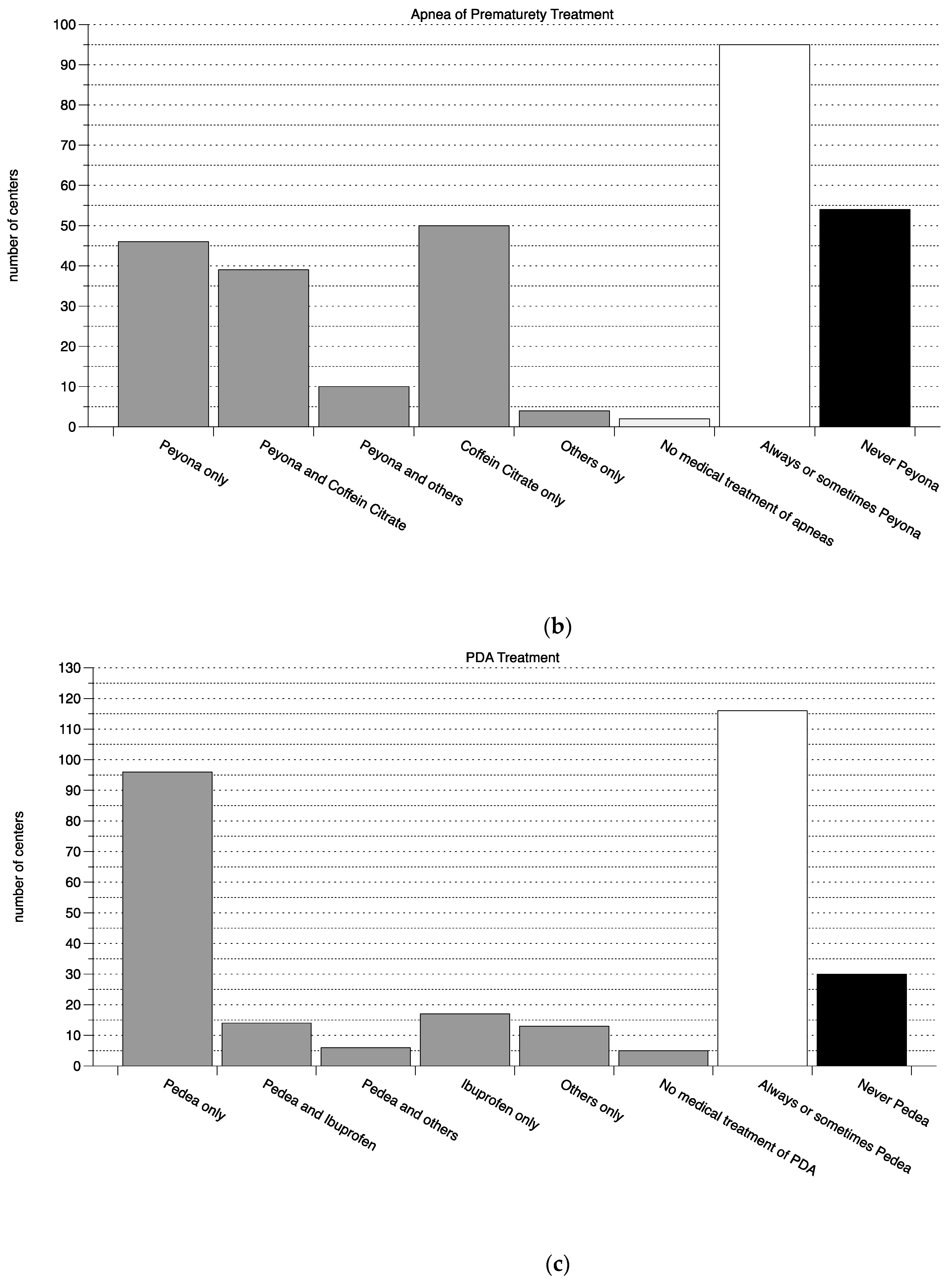
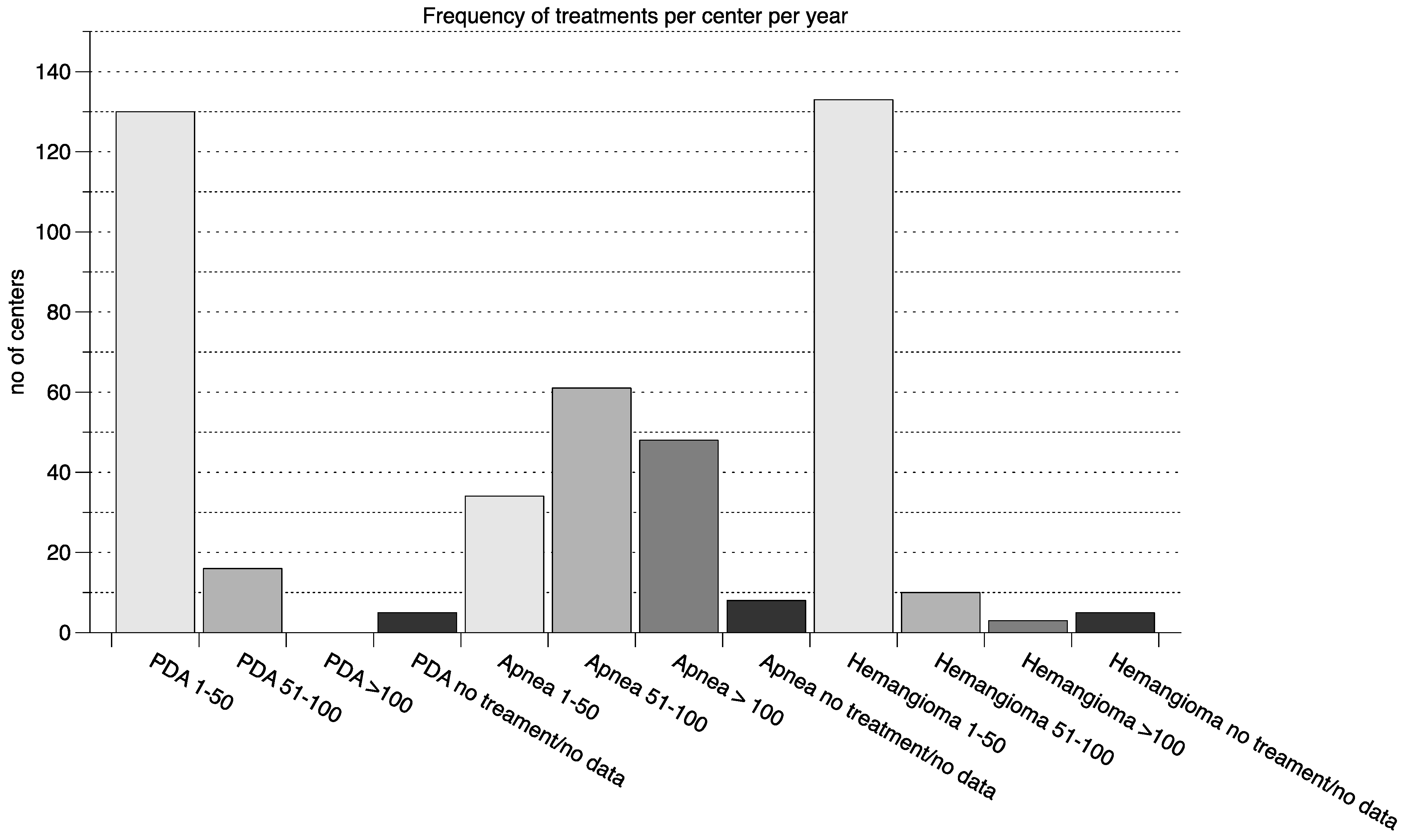
3.1. Survey of Clinical Practice in Perinatal Centers in Germany
3.2. Analysis of EMA’s EPARs
3.3. Drug Price Comparison
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- O’Donnell, C.P.F.; Stone, R.J.; Morley, C.J.; Davies, P.; Cheng, D.; Fox, A.; Lee, L. Unlicensed and Off-Label Drug Use in an Australian Neonatal Intensive Care Unit. Pediatrics 2002, 110, e52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuzzolin, L.; Atzei, A.; Fanos, V. Off-label and unlicensed prescribing for newborns and children in different settings: A review of the literature and a consideration about drug safety. Expert Opin. Drug Saf. 2006, 5, 703–718. [Google Scholar] [CrossRef] [PubMed]
- Dove, A. FDA in a quandary over Pediatric Rule. Nat. Med. 2002, 8, 541–542. [Google Scholar] [CrossRef] [PubMed]
- Hampton, T. Pediatric Drug Studies Required by Law. JAMA 2004, 291, 412–413. [Google Scholar] [CrossRef] [PubMed]
- Nir-Neuman, H.; Abu-Kishk, I.; Toledano, M.; Heyman, E.; Ziv-Baran, T.; Berkovitch, M. Unlicensed and Off-Label Medication Use in Pediatric and Neonatal Intensive Care Units: No Change Over a Decade. Adv. Ther. 2018, 35, 1122–1132. [Google Scholar] [CrossRef] [PubMed]
- Geißler, C.; Schulze, C.; Botzenhardt, S.; Rascher, W.; Neubert, A. Drug Utilisation and Off-Label Use on a German Neonatal Intensive Care Unit: A Retrospective Cohort Study and 10-Year Comparison. Pharmacy 2020, 8, 173. [Google Scholar] [CrossRef] [PubMed]
- Costa, H.T.M.D.L.; Costa, T.X.; Martins, R.R.; Oliveira, A.G. Use of off-label and unlicensed medicines in neonatal intensive care. PLoS ONE 2018, 13, e0204427. [Google Scholar] [CrossRef] [PubMed]
- EMA. European Public Assessment Report Pedea. 2005. Available online: https://www.ema.europa.eu/en/documents/scientific-discussion/pedea-epar-scientific-discussion_en.pdf (accessed on 1 December 2021).
- EMA. European Public Assessment Report Nymusa/Peyona. 2009. Available online: https://www.ema.europa.eu/en/documents/assessment-report/nymusa-epar-public-assessment-report_en.pdf (accessed on 1 December 2021).
- Erenberg, A.; Leff, R.D.; Haack, D.G.; Mosdell, K.W.; Hicks, G.M.; A Wynne, B. Caffeine citrate for the treatment of apnea of prematurity: A double-blind, placebo-controlled study. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2000, 20, 644–652. [Google Scholar] [CrossRef] [PubMed]
- EMA. European Public Assessment Report Hemangiol. 2014. Available online: https://www.ema.europa.eu/en/documents/assessment-report/hemangiol-epar-public-assessment-report_en.pdf (accessed on 1 December 2021).
- EMA. Orphan Drug Designation Pedea. 2009. Available online: https://www.ema.europa.eu/en/medicines/human/orphan-designations/eu301020 (accessed on 1 December 2021).
- EMA. Orphan Drug Designation Nymusa/Peyona. 2007. Available online: https://www.ema.europa.eu/en/medicines/human/orphan-designations/eu303132 (accessed on 1 December 2021).
- Park, J.; Yoon, S.J.; Han, J.; Song, I.G.; Lim, J.; E Shin, J.; Eun, H.S.; I Park, K.; Park, M.S.; Lee, S.M. Patent ductus arteriosus treatment trends and associated morbidities in neonates. Sci. Rep. 2021, 11, 10689. [Google Scholar] [CrossRef] [PubMed]
- Stark, A.; Smith, P.B.; Hornik, C.P.; Zimmerman, K.O.; Hornik, C.D.; Pradeep, S.; Clark, R.H.; Benjamin, D.K.; Laughon, M.; Greenberg, R.G. Medication Use in the Neonatal Intensive Care Unit and Changes from 2010 to 2018. J. Pediatr. 2021, 240, 66–71.e4. [Google Scholar] [CrossRef] [PubMed]
- Anderson, K.R.; Schoch, J.; Lohse, C.M.; Hand, J.L.; Davis, D.M.; Tollefson, M.M. Increasing incidence of infantile hemangiomas (IH) over the past 35 years: Correlation with decreasing gestational age at birth and birth weight. J. Am. Acad. Dermatol. 2015, 74, 120–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sinha, M.S.; Najafzadeh, M.; Rajasingh, E.K.; Love, J.; Kesselheim, A.S. Labeling Changes and Costs for Clinical Trials Performed Under the US Food and Drug Administration Pediatric Exclusivity Extension, 2007 to 2012. JAMA Intern. Med. 2018, 178, 1458–1466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schrier, L.; Hadjipanayis, A.; Stiris, T.; I Ross-Russell, R.; Valiulis, A.; Turner, M.A.; Zhao, W.; De Cock, P.; De Wildt, S.N.; Allegaert, K.; et al. Off-label use of medicines in neonates, infants, children, and adolescents: A joint policy statement by the European Academy of Paediatrics and the European society for Developmental Perinatal and Pediatric Pharmacology. Eur. J. Pediatr. 2020, 179, 839–847. [Google Scholar] [CrossRef] [PubMed]
- Nicholl, D.J.; Hilton-Jones, D.; Palace, J.; Richmond, S.; Finlayson, S.; Winer, J.; Weir, A.; Maddison, P.; Fletcher, N.; Sussman, J.; et al. Open letter to prime minister David Cameron and health secretary Andrew Lansley. BMJ 2010, 341, c6466. [Google Scholar] [CrossRef] [PubMed]
- Quartel, A.; Lennertz, J. BioMarin Europe replies. BMJ 2010, 341, c7006. [Google Scholar] [CrossRef] [PubMed]
- Simoens, S.; Picavet, E.; Dooms, M.; Cassiman, D.; Morel, T. Cost-effectiveness assessment of orphan drugs: A scientific and political conundrum. Appl. Health Econ. Health Policy 2013, 11, 1–3. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Indication and Product | MAH Sponsored Studies | ||
|---|---|---|---|
| Non-Clinical | Clinical | ||
| Healthy Volunteers | Target Population | ||
| PDA product: Pedea® |
| ||
| apnea of prematurity product: Peyona® | 0 | 0 | |
| hemangioma product: Hemangiol® |
|
|
|
| Indication and Product | |
|---|---|
| PDA product: Pedea® | No studies conducted, label changes to PSUR analysis (gastric perforation added as risk) |
| apnea of prematurity product: Peyona® | European non-interventional post-authorization study to assess drug utilization and safety of caffeine citrate in the treatment of premature infants affected by apnea |
| hemangioma product: Hemangiol® | Updated efficacy and safety report of the pivotal study as well as the results of a small study conducted in France |
| Indication | Product Approved in the Indication/Price in € | Alternative Product, Not Approved in the Indication/Price in € | Price Increase Not Approved to Approved in the Indication |
|---|---|---|---|
| PDA | Pedea® 16.22 €/mg | Caldolor® 0.04 €/mg | ×405 |
| apnea of prematurity | Peyona® 0.86 €/mg | caffeine citrate 0.0005 €/mg | ×1720 |
| hemangioma | Hemangiol® 0.56 €/mg | propanolol 0.015 €/mg | ×37 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Veldman, A.; Richter, E.; Hacker, C.; Fischer, D. The Use of Off-Label Medications in Newborn Infants Despite an Approved Alternative Being Available—Results of a National Survey. Pharmacy 2022, 10, 19. https://doi.org/10.3390/pharmacy10010019
Veldman A, Richter E, Hacker C, Fischer D. The Use of Off-Label Medications in Newborn Infants Despite an Approved Alternative Being Available—Results of a National Survey. Pharmacy. 2022; 10(1):19. https://doi.org/10.3390/pharmacy10010019
Chicago/Turabian StyleVeldman, Alex, Eva Richter, Christian Hacker, and Doris Fischer. 2022. "The Use of Off-Label Medications in Newborn Infants Despite an Approved Alternative Being Available—Results of a National Survey" Pharmacy 10, no. 1: 19. https://doi.org/10.3390/pharmacy10010019