
Pharmacists’ Satisfaction with Work and Working Conditions in New Zealand—An Updated Survey and a Comparison to Canada


Abstract
:1. Introduction
- To determine the perception of current pharmacists’ working conditions in NZ and compare these with those recently found in Canada;
- To depict the work-related and psychological distress of NZ pharmacists and compare with a prior assessment;
- To explore relationships between work conditions and various predictor variables.
2. Method
2.1. Survey Administration/Mechanics
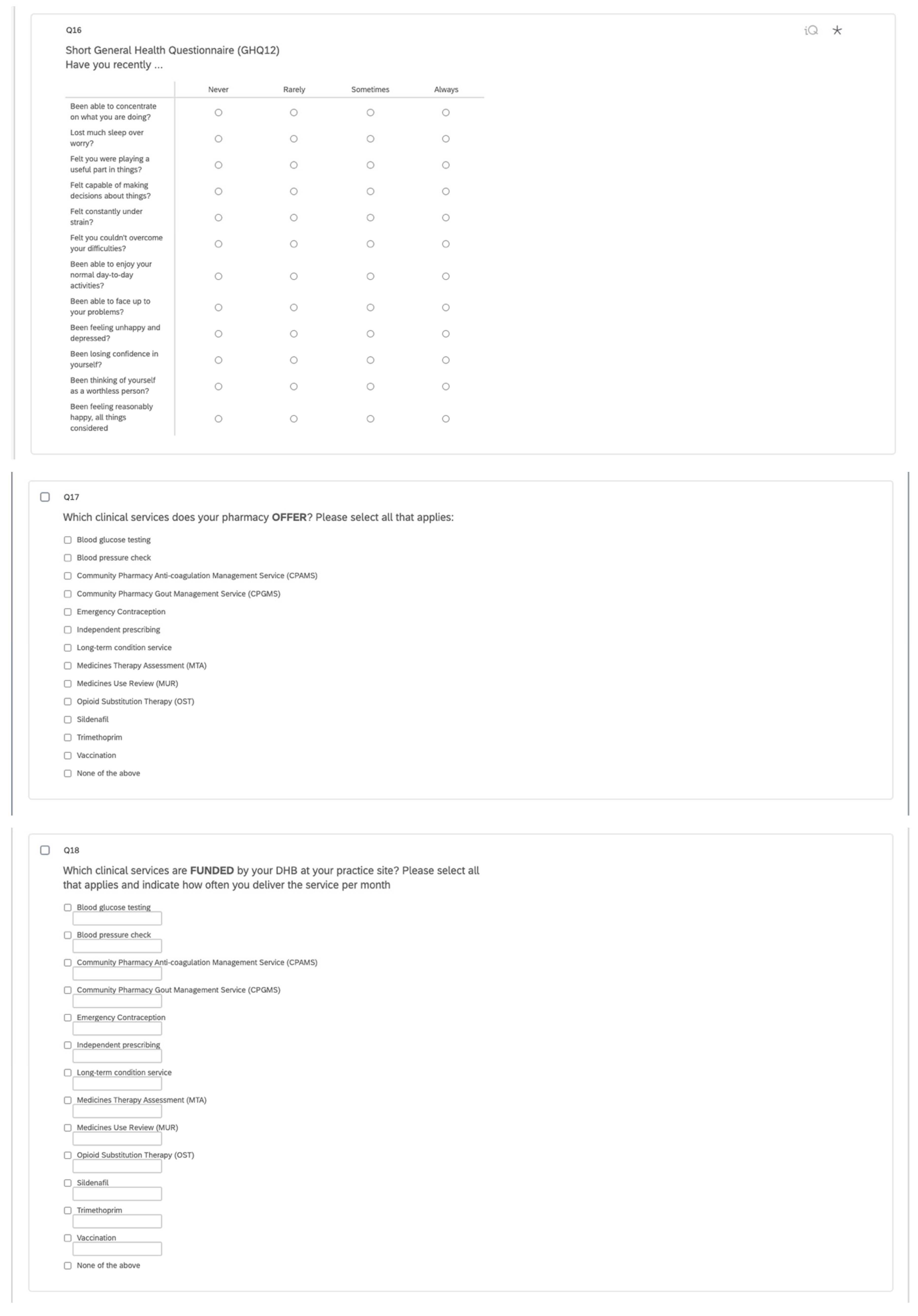
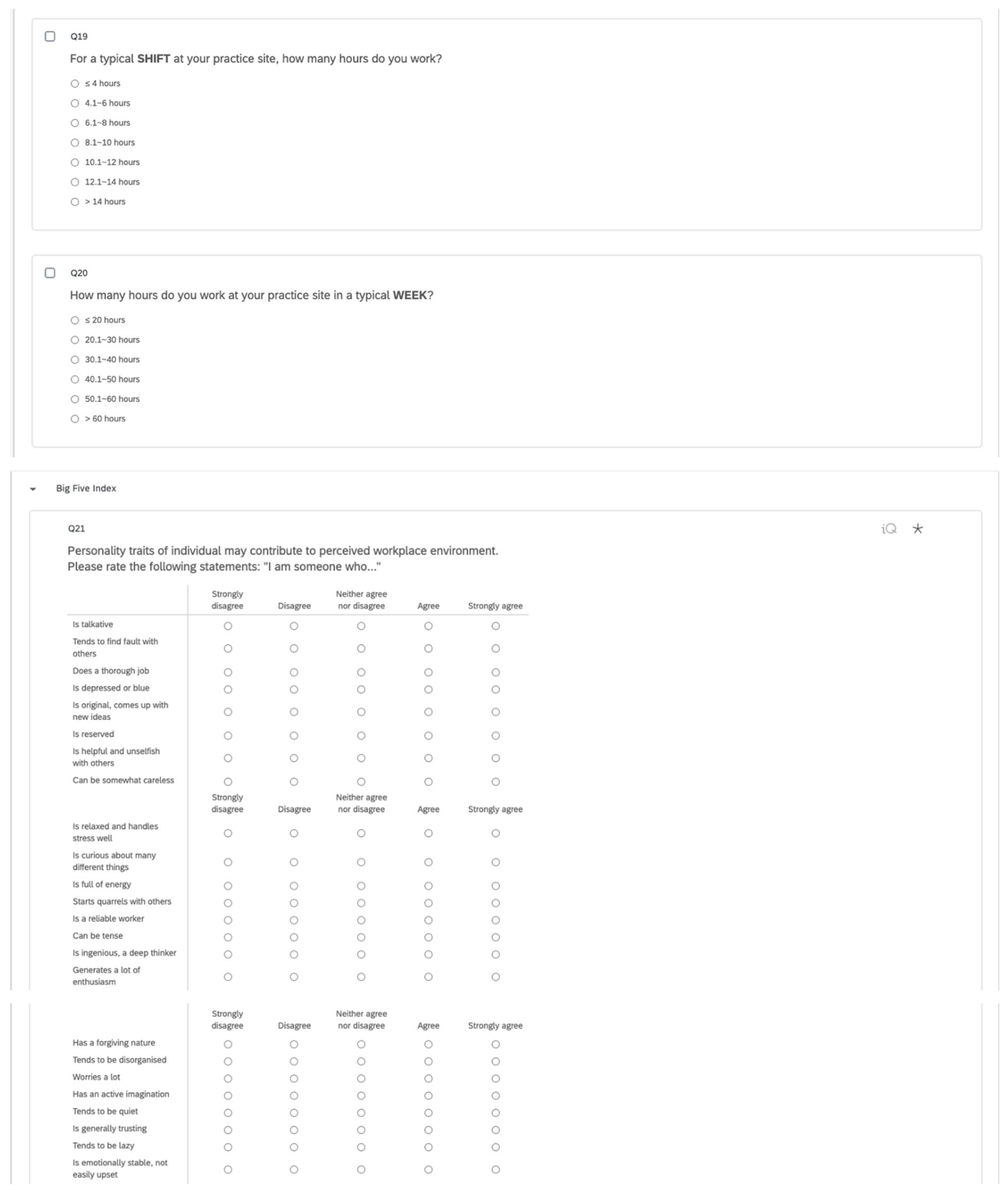
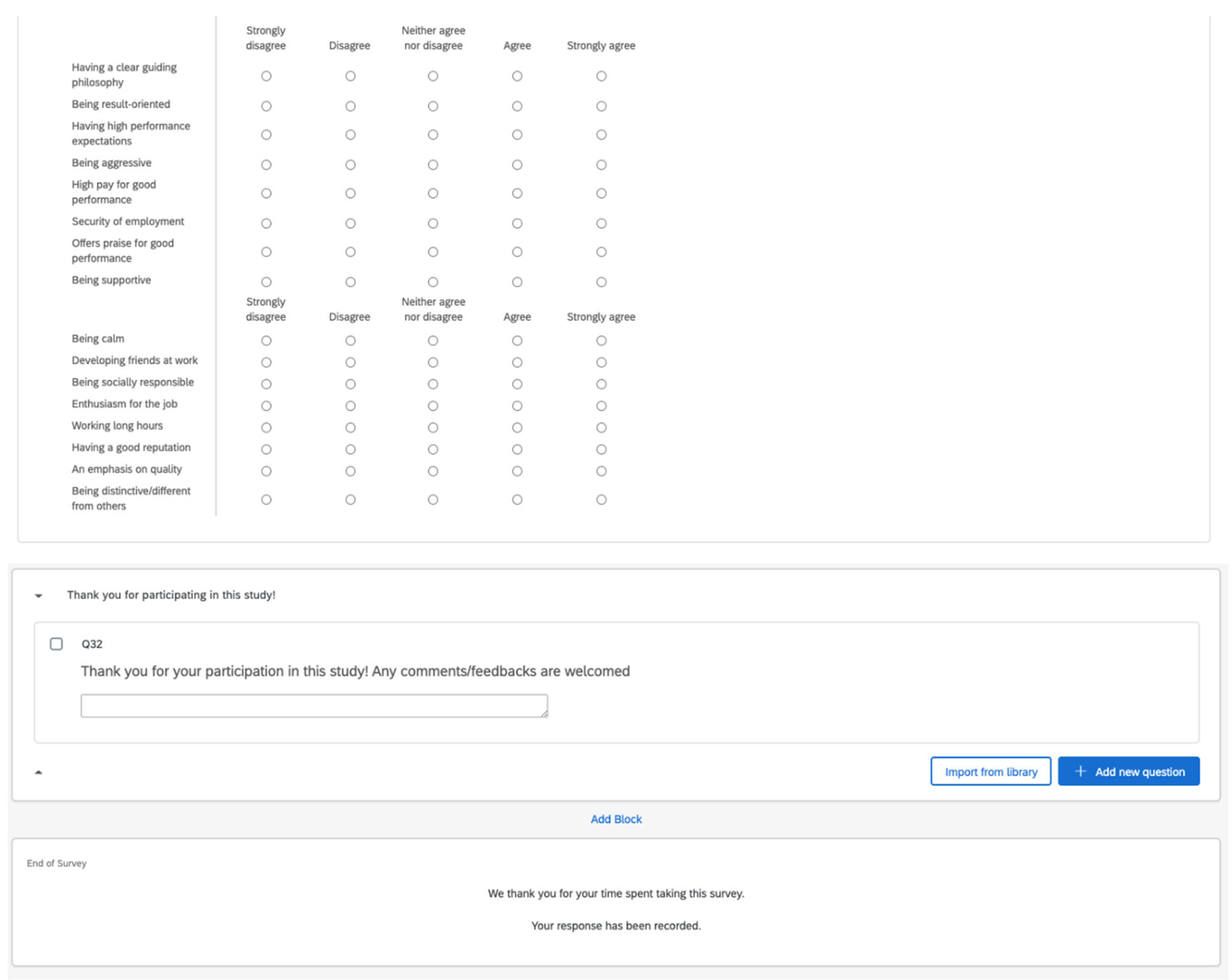
2.2. Survey Instrument
2.3. Data Collection
2.4. Data Analyses
3. Results
3.1. Respondents
3.2. Personal Pharmacy Experiences and Clinical Activities
3.3. Characteristics of the Pharmacy
3.4. Satisfaction with Working Conditions
4. Discussion
4.1. Strengths
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A








References
- Higuchi, Y.; Inagaki, M.; Koyama, T.; Kitamura, Y.; Sendo, T.; Fujimori, M.; Uchitomi, Y.; Yamada, N. A cross-sectional study of psychological distress, burnout, and the associated risk factors in hospital pharmacists in Japan. BMC Public Health 2016, 16, 534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooksey, J.A.; Knapp, K.K.; Walton, S.M.; Cultice, J.M. Challenges to the pharmacist profession from escalating pharmaceutical demand. Health Aff. 2002, 21, 182–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kreling, D.H.; Doucette, W.R.; Mott, D.A.; Gaither, C.A.; Pedersen, C.A.; Schommer, J.C. Community pharmacists’ work environments: Evidence from the 2004 National Pharmacist Workforce Study. J. Am. Pharm. Assoc. 2006, 46, 331–339. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.; Rosenthal, M.; Family, H.; Sutton, J.; Hall, K.; Tsuyuki, R.T. Personality traits of hospital pharmacists: Toward a better understanding of factors influencing pharmacy practice change. Can. J. Hosp. Pharm. 2013, 66, 289–295. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, S.; Hassell, K.; Ashcroft, D.; Johnson, S.; O’Connor, E. Workplace stress in community pharmacies in England: Associations with individual, organizational and job characteristics. J. Health Serv. Res. Policy 2014, 19, 27–33. [Google Scholar] [CrossRef]
- James, K.L.; Barlow, D.; McArtney, R.; Hiom, S.; Roberts, D.; Whittlesea, C. Incidence, type and causes of dispensing errors: A review of the literature. Int. J. Pharm. Pract. 2009, 17, 9–30. [Google Scholar] [CrossRef]
- Lea, V.M.; Corlett, S.A.; Rodgers, R.M. Workload and its impact on community pharmacists’ job satisfaction and stress: A review of the literature. Int. J. Pharm. Pract. 2012, 20, 259–271. [Google Scholar] [CrossRef]
- Malone, D.C.; Abarca, J.; Skrepnek, G.H.; Murphy, J.E.; Armstrong, E.P.; Grizzle, A.J.; Rehfeld, R.A.; Woosley, R.L. Pharmacist workload and pharmacy characteristics associated with the dispensing of potentially clinically important drug-drug interactions. Med. Care 2007, 45, 456–462. [Google Scholar] [CrossRef]
- Schafheutle, E.I.; Seston, E.M.; Hassell, K. Factors influencing pharmacist performance: A review of the peer-reviewed literature. Health Policy 2011, 102, 178–192. [Google Scholar] [CrossRef]
- Szeinbach, S.; Seoane-Vazquez, E.; Parekh, A.; Herderick, M. Dispensing errors in community pharmacy: Perceived influence of sociotechnical factors. Int. J. Qual. Health Care 2007, 19, 203–209. [Google Scholar] [CrossRef] [Green Version]
- Gidman, W.K.; Hassell, K.; Day, J.; Payne, K. The impact of increasing workloads and role expansion on female community pharmacists in the United Kingdom. Res. Soc. Adm. Pharm. 2007, 3, 285–302. [Google Scholar] [CrossRef]
- Gothard, A.M.; Dade, J.P.; Murphy, K.; Mellor, E.J. Using error theory in the pharmacy dispensary can reduce accidents. Pharm. Pract. 2004, 14, 44–48. [Google Scholar]
- McCann, L.; Adair, C.G.; Hughes, C.M. An exploration of work-related stress in Northern Ireland community pharmacy: A qualitative study. Int. J. Pharm. Pract. 2009, 17, 261–267. [Google Scholar] [CrossRef]
- Peterson, G.M.; Wu, M.S.; Bergin, J.K. Pharmacist’s attitudes towards dispensing errors: Their causes and prevention. J. Clin. Pharm. Ther. 1999, 24, 57–71. [Google Scholar] [CrossRef]
- Bond, C.A.; Raehl, C.L. Pharmacists’ assessment of dispensing errors: Risk factors, practice sites, professional functions, and satisfaction. Pharmacotherapy 2001, 21, 614–626. [Google Scholar] [CrossRef]
- Aldhwaihi, K.; Schifano, F.; Pezzolesi, C.; Umaru, N. A systematic review of the nature of dispensing errors in hospital pharmacies. Integr. Pharm. Res. Pract. 2016, 5, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Gidman, W. Exploring the impact of evolving health policy on independent pharmacy ownership in England. Pharm. World Sci. 2010, 32, 488–495. [Google Scholar] [CrossRef]
- Cox, E.R.; Fitzpatrick, V. Pharmacists’ job satisfaction and perceived utilization of skills. Am. J. Health Syst. Pharm. 1999, 56, 1733–1737. [Google Scholar] [CrossRef]
- Kerschen, A.M.; Armstrong, E.P.; Hillman, T.N. Job Satisfaction Among Staff, Clinical, and Integrated Hospital Pharmacists. J. Pharm. Pract. 2006, 19, 306–312. [Google Scholar] [CrossRef]
- Mak, V.S.; March, G.J.; Clark, A.; Gilbert, A.L. Why do Australian registered pharmacists leave the profession? A qualitative study. Int. J. Clin. Pharm. 2013, 35, 129–137. [Google Scholar] [CrossRef]
- Oregon Board of Pharmacy. Oregon Board of Pharmacy Workload Survey. November 2013. Available online: www.oregon.gov/pharmacy/Imports/OBOP-Pharmacy_Working_Conditions_Survey_Results11.13.pdf (accessed on 21 January 2021).
- Tsao, N.W.; Lynd, L.D.; Gastonguay, L.; Li, K.; Nakagawa, B.; Marra, C.A. Factors associated with pharmacists’ perceptions of their working conditions and safety and effectiveness of patient care. Can. Pharm. J. 2016, 149, 18–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsao, N.W.; Salmasi, S.; Li, K.; Nakagawa, B.; Lynd, L.D.; Marra, C.A. Pharmacists’ perceptions of their working conditions and the factors influencing this: Results from 5 Canadian provinces. Can. Pharm. J. 2020, 153, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, M.; Tsao, N.W.; Tsuyuki, R.T.; Marra, C.A. Identifying relationships between the professional culture of pharmacy, pharmacists’ personality traits, and the provision of advanced pharmacy services. Res. Soc. Adm. Pharm. 2016, 12, 56–67. [Google Scholar] [CrossRef] [PubMed]
- Dowell, A.C.; Westcott, T.; McLeod, D.K.; Hamilton, S. A survey of job satisfaction, sources of stress and psychological symptoms among New Zealand health professionals. N. Z. Med. J. 2001, 114, 540. [Google Scholar]
- Goldberg, D.P.; Blackwell, B. Psychiatric illness in general practice. A detailed study using a new method of case identification. Br. Med. J. 1970, 1, 439–443. [Google Scholar] [CrossRef] [Green Version]
- Goldberg, D.P.; Gater, R.; Sartorius, N.; Ustun, T.B.; Piccinelli, M.; Gureje, O.; Rutter, C. The validity of two versions of the GHQ in the WHO study of mental illness in general health care. Psychol. Med. 1997, 27, 191–197. [Google Scholar] [CrossRef]
- O’ Reilly, C.A.; Chatman, J.; Caldwell, D.F. People and Organizational Culture: A Profile Comparison Approach to Assessing Person-Organization Fit. Acad. Manag. J. 1991, 34, 487. [Google Scholar] [CrossRef] [Green Version]
- Pharmacy Council. New Zealand Pharmacy Council 2020 Workforce Demographic Report. Available online: https://pharmacycouncil.org.nz/wp-content/uploads/2021/03/Workforce-Demographic-Report-2020.pdf (accessed on 12 May 2020).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number (n = 579) | Percentage (%) |
|---|---|---|
| Gender Female Male | 382 197 | 65.9 34.1 |
| Qualifications Bachelor of Pharmacy (BPharm) Diploma of Pharmacy Postgraduate qualifications (e.g., PGCertPharm, PGCertPharPres, etc.) Others (e.g., PhD, BSc, PGDip Management, etc.) | 294 93 138 54 | 50.8 16 23.8 9.4 |
| Primary Practice Site Community pharmacy (chain or independent) In-patient hospital pharmacy Others (e.g., academia, primary care, industry, etc.) | 423 84 72 | 73.1 14.4 12.5 |
| Primary Practice Site Location Main urban area (≥30,000 people) Secondary urban area (10,000~29,999 people) Minor urban/rural area (<9999 people) | 362 122 95 | 62.5 21.0 16.5 |
| Practice Role Clinical/specialist pharmacist Pharmacy manager Pharmacy director/owner Staff pharmacist Others (e.g., industry, academia, etc.) | 103 88 126 179 83 | 17.8 15.2 21.8 30.9 14.3 |
| Years as Registered Pharmacist ≤5 6–15 16–24 ≥25 | 106 153 92 219 | 18.3 26.4 15.8 37.9 |
| Canadian Pharmacists n = 1016 | NZ Pharmacists n = 579 | |||
|---|---|---|---|---|
| Disagree (%) | Agree (%) | Disagree (%) | Agree (%) | |
| “I have adequate time for break/lunches at my practice site” | 48 | 40 | 46 | 40 |
| “I am satisfied with the amount of time I have to do my job” | 45 | 34 | 51 | 31 |
| “My employer provides a work environment that is conducive to providing safe and effective primary care” ^ | 28 | 47 | 20 | 57 |
| “My site has adequate pharmacist staff to provide safe and effective primary care” | 36 | 41 | 32 | 46 |
| “My site has adequate technician staff to provide safe and effective primary care” * | 35 | 32 | 33 | 45 |
| “My site has adequate retail assistant staff to provide safe and effective primary care” | 31 | 45 | 25 | 42 |
| 2001 NZ Pharmacists n = 303 | 2021 NZ Pharmacists n = 423 | 2021 NZ Pharmacists (Proportion Agree/Strongly Agree) | |
|---|---|---|---|
| Contemplated leaving your job due to work stress | 4 (2–6) | 5 (3–7) | 45% |
| Felt that work stress has affected health | 4 (3–5) | 5 (3–7) | 45% |
| Felt unable to remain competent at work | 3 (2–4) | 3 (1–5) | 15% |
| Felt overwhelmed by paper work | 6 (5–7) | 5 (3–7) | 40% |
| Felt frustrated over bureaucratic interference | 7 (6–7) | 6 (4–7) | 58% |
| Feel work has interfered significantly with family/social life | 5 (4–6) | 5 (3–7) | 38% |
| Likelihood of not repeating career choice again | 5 (3–6) | 6 (4–7) | 55% |
| Government funding for patient care has increased | 2 (2–4) | 1 (1–3) | 3% |
| Pharmacists should have a greater role in primary care | 5 (4–7) | 6 (5–7) | 71% |
| 2001 NZ Pharmacists | 2021 NZ Pharmacists | |
|---|---|---|
| Count | n = 300 | n = 389 |
| Total GHQ-12 mean (SD) | 3.21 (3.20) | 3.50 (1.83) |
| Proportion GHQ score 4–12 | 41% | 47% |
| Proportion GHQ score 8–12 * | 11% | 2% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lam, S.J.; Lynd, L.D.; Marra, C.A. Pharmacists’ Satisfaction with Work and Working Conditions in New Zealand—An Updated Survey and a Comparison to Canada. Pharmacy 2023, 11, 21. https://doi.org/10.3390/pharmacy11010021
Lam SJ, Lynd LD, Marra CA. Pharmacists’ Satisfaction with Work and Working Conditions in New Zealand—An Updated Survey and a Comparison to Canada. Pharmacy. 2023; 11(1):21. https://doi.org/10.3390/pharmacy11010021
Chicago/Turabian StyleLam, Sharon Jessie, Larry D. Lynd, and Carlo A. Marra. 2023. "Pharmacists’ Satisfaction with Work and Working Conditions in New Zealand—An Updated Survey and a Comparison to Canada" Pharmacy 11, no. 1: 21. https://doi.org/10.3390/pharmacy11010021
APA StyleLam, S. J., Lynd, L. D., & Marra, C. A. (2023). Pharmacists’ Satisfaction with Work and Working Conditions in New Zealand—An Updated Survey and a Comparison to Canada. Pharmacy, 11(1), 21. https://doi.org/10.3390/pharmacy11010021