
Application of Precision Medicine Concepts in Ambulatory Antibiotic Management of Acute Pyelonephritis

 , ,
, ,  and
and 
Abstract
:1. Introduction
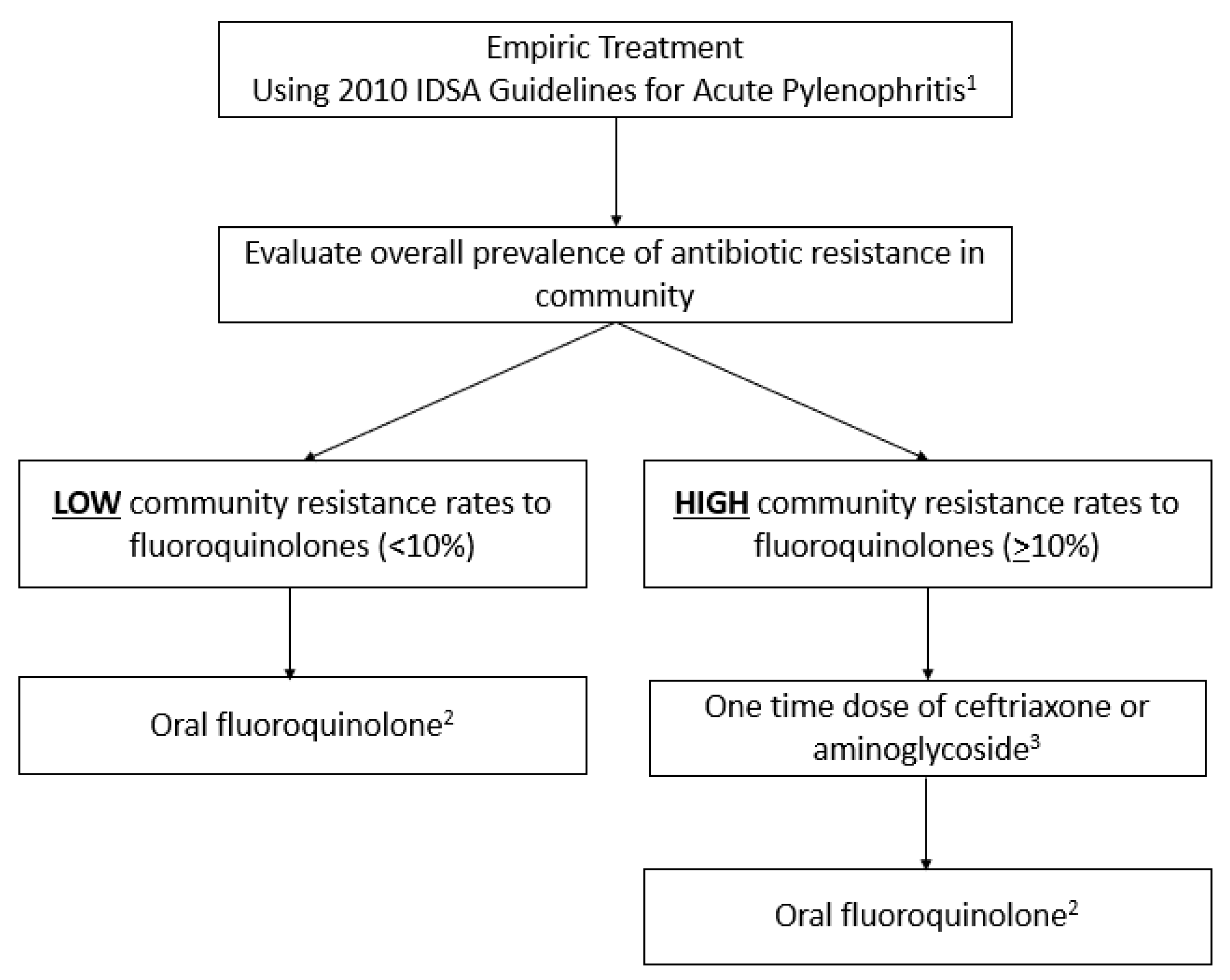
2. The 2010 Infectious Diseases Society of American (IDSA) and European Society of Clinical Microbiology and Infectious Diseases (ESCMID) Guidelines on APN
3. Prevalence of Antibiotic Resistance
4. Application of Precision Medicine Concept in APN
4.1. Summary of Concept
4.2. Resistance Rates in the United States
4.3. Institutional Antibiograms
4.4. Problems with Antibiograms
4.5. Institutional- vs. Unit-Based Antibiograms
4.6. All-Source versus Urine-Specific Antibiograms
4.7. Population Level vs. Patient-Specific Antibiograms
5. Prediction of Antibiotic Resistance in Enterobacterales
5.1. Prediction of Fluoroquinolone Resistance
5.2. Prediction of TMP-SMX Resistance
5.3. Prediction of Ceftriaxone Resistance (ESBL-Production)
5.4. Potential Benefits of Patient-Specific Therapy
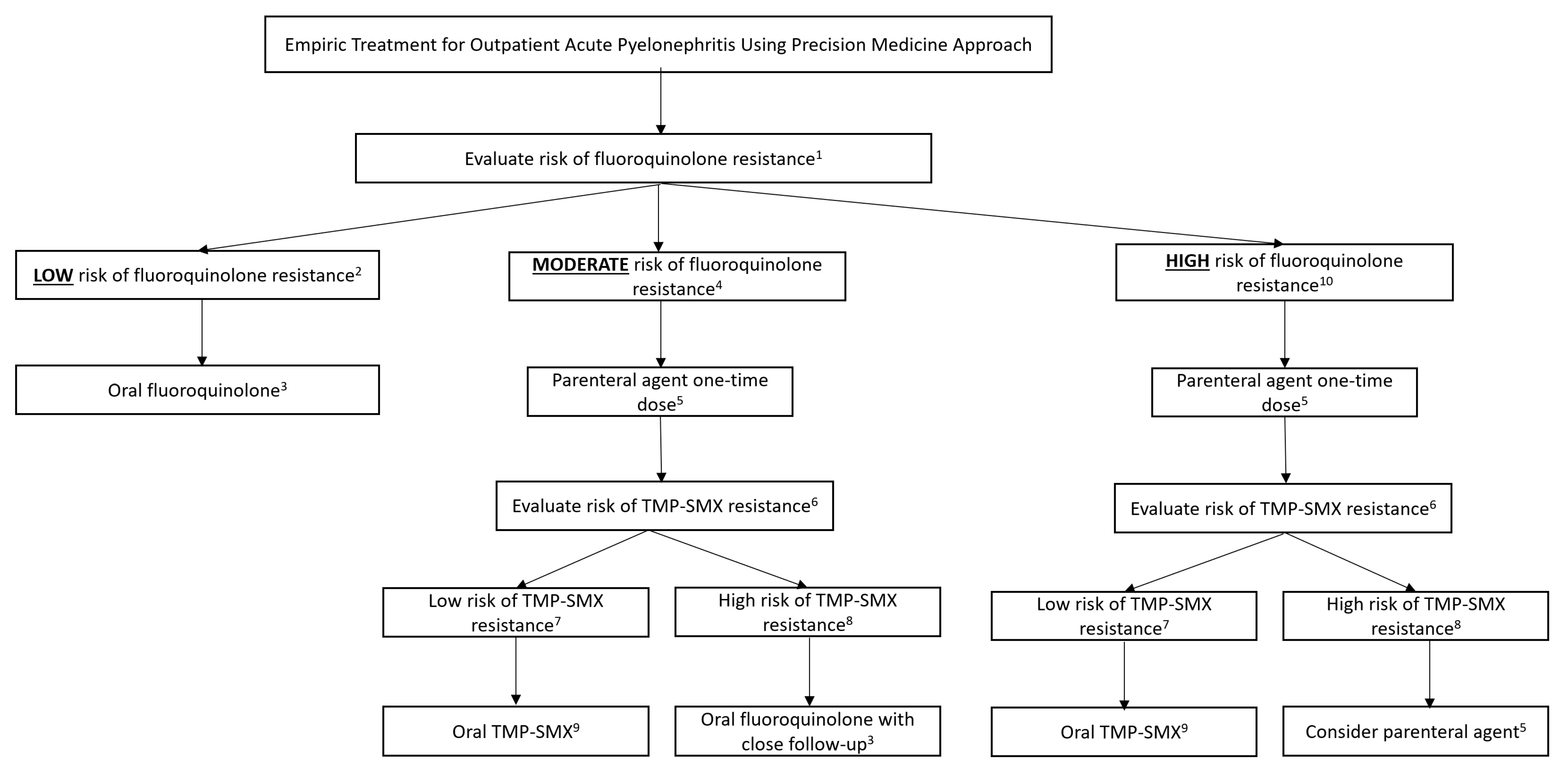
6. Clinical Application of Guideline-Based vs. Precision-Medicine-Based Empirical Therapy for APN (Figure 1 and Figure 2; Table 1, Table 2 and Table 3)



{kind=link}
{kind=link}
| Patient-Specific Characteristic | Points |
|---|---|
| Male sex | 1 |
| Diabetes mellitus | 1 |
| Residence in skilled nursing facility | 2 |
| Outpatient procedure in past 30 days | 3 |
| Fluoroquinolone use in past 3 months | 5 |
| Fluroquinolone use in past 3–12 months | 3 |
Fluroquinolone Resistance Score Interpretation
| |
| May utilize local validated risk scores if applicable with corresponding risk cutoffs | |
| Adapted from [18] | |
| Patient-Specific Characteristic | Points |
|---|---|
| TMP-SMX use in past 12 months | 1 |
| Prior urine cultures with TMP-SMX-resistant pathogen in past 12 months | 2 |
TMP-SMX Risk Score Interpretation
| |
| May utilize local validated risk scores if applicable with corresponding risk cutoffs | |
| Adapted from [20] | |
| Patient-Specific Characteristic | Points |
|---|---|
| Outpatient GI/GU procedure in past 30 days | 1 |
| One beta-lactam or fluoroquinolone courses within past 90 days | 1 |
| Two or more beta-lactam or fluoroquinolone courses within past 90 days | 3 |
| Documented colonization or infections with ESBLs within past 12 months | 4 |
ESBL Risk Score Interpretation
| |
| May utilize local validated risk scores if applicable with corresponding risk cutoffs | |
| Adapted from [24] | |
7. Case Example
- Metformin 1000 mg twice daily;
- Lisinopril 20 mg daily;
- Atorvastatin 40 mg daily.
7.1. Empiric Therapy Using 2010 IDSA Guidelines for APN
7.2. Empiric Therapy Using Precision Medicine Approach
8. Applications in Pharmacy Practice
9. Limitations
10. Summary
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Czaja, C.; Scholes, D.; Hooton, T.; Stamm, W. Population-Based Epidemiologic Analysis of Acute Pyelonephritis. Clin. Infect. Dis. 2007, 45, 273–280. [Google Scholar] [CrossRef]
- Talan, D.A.; Takhar, S.S.; Krishnadasan, A.; Abrahamian, F.M.; Mower, W.R.; Moran, G.J.; EMERG Ency ID Net Study Group. Fluoroquinolone-Resistant and Extended-Spectrum B-Lactamase-Producing Escherichia coli Infections in Patients with Pyelonephritis, United States. Emerg. Infect. Dis. 2016, 22, 1594–1603. [Google Scholar] [CrossRef] [PubMed]
- Gupta, K.; Hooton, T.M.; Naber, K.G.; Wullt, B.; Colgan, R.; Miller, L.G.; Moran, G.J.; Nicolle, L.E.; Raz, R.; Schaeffer, A.J.; et al. International Clinical Practice Guideline for the Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in Women: A 2010 Update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin. Infect. Dis. 2011, 52, 103–120. [Google Scholar] [CrossRef]
- Zhanel, G.G.; Hisanaga, T.L.; Laing, N.M.; DeCorby, M.R.; Nichol, K.A.; Weshnoweski, B.; Johnson, J.; Noreddin, A.; Low, D.E.; Karlowsky, J.A.; et al. Antibiotic resistance in Escherichia coli outpatient urinary isolates: Final results from the North American Urinary Tract Infection Collaborative Alliance (NAUTICA). Int. J. Antimicrob. Agents 2006, 6, 468–475. [Google Scholar] [CrossRef] [PubMed]
- Critchley, I.A.; Cotroneo, N.; Pucci, M.J.; Mendes, R. The burden of antimicrobial resistance among urinary tract isolates of Escherichia coli in the United States in 2017. PLoS ONE 2019, 14, e0220265. [Google Scholar] [CrossRef]
- Bouchillon, S.; Hoban, D.J.; Badal, R.; Hawser, S. Fluoroquinolone resistance among gram-negative urinary tract pathogens: Global smart program results, 2009–2010. Open Microbiol. J. 2012, 6, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Somorin, Y.M.; Weir, N.J.M.; Pattison, S.H.; Crockard, M.A.; Hughes, C.M.; Tunney, M.M.; Gilpin, D.F. Antimicrobial resistance in urinary pathogens and culture-independent detection of trimethoprim resistance in urine from patients with urinary tract infection. BMC Microbiol. 2022, 22, 144. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.; Russo, T. Acute Pyelonephritis in Adults. N. Engl. J. Med. 2018, 378, 48–59. [Google Scholar] [CrossRef]
- Dunne, M.W.; Puttagunta, S.; Aronin, S.I.; Brossette, S.; Murray, J.; Gupta, V. Impact of Empirical Antibiotic Therapy on Outcomes of Outpatient Urinary Tract Infection Due to Nonsusceptible Enterobacterales. Microbiol. Spectr. 2022, 10, e0235821. [Google Scholar] [CrossRef]
- Haggard, E.; Hagedorn, M.; Bookstaver, P.B.; Justo, J.A.; Kohn, J.; Al-Hasan, M.N. Minimum Acceptable Susceptibility of Empirical Antibiotic Regimens for Gram-Negative Bloodstream Infections. A Survey of Clinical Pharmacists. Infect. Dis. Clin. Pract. 2018, 26, 283–287. [Google Scholar] [CrossRef]
- Moehring, R.W.; Hazen, K.C.; Hawkins, M.R.; Drew, R.H.; Sexton, D.J.; Anderson, D.J. Challenges in preparation of cumulative antibiogram reports for community hospitals. J. Clin. Microbiol. 2015, 53, 2977–2982. [Google Scholar] [CrossRef] [PubMed]
- Hostler, C.J.; Moehring, R.W.; Ashley, E.S.D.; Johnson, M.; Davis, A.; Lewis, S.S.; Sexton, D.J.; Anderson, D.J.; CDC Prevention Epicenters Program. Feasibility and Value of Developing a Regional Antibiogram for Community Hospitals. Infect. Control. Hosp. Epidemiol. 2018, 39, 718–722. [Google Scholar] [CrossRef] [PubMed]
- Kuster, S.P.; Ruef, C.; Zbinden, R.; Gottschalk, J.; Ledergerber, B.; Neuber, L.; Weber, R. Stratification of cumulative antibiograms in hospital unit, specimen type, isolate sequence and duration of hospital stay. J. Antimicrob. Chemother. 2008, 62, 1451–1461. [Google Scholar] [CrossRef]
- Binkley, S.; Fishman, N.O.; LaRosa, L.A.; Marr, A.M.; Nachamkin, I.; Wordell, D.; Bilker, W.B.; Lautenbach, E. Comparison of unit-specific and hospital-wide antibiograms: Potential implications for selection of empirical antimicrobial therapy. Infect. Control Hosp. Epidemiol. 2006, 27, 682–687. [Google Scholar] [CrossRef] [PubMed]
- Rabs, N.; Wieczorkiewicz, S.; Costello, M.; Zamfirova, I. Development of a urinary-specific antibiogram for gram-negative isolates: Impact of patient risk factors on susceptibility. Am. J. Infect. Control 2014, 42, 393–400. [Google Scholar] [CrossRef]
- Marsh, K.; Mundy, L.; Holter, J.; Johnson, J. Analysis of Urine-specific Antibiograms from Veterans to Guide Empiric Therapy for Suspected Urinary Tract Infection. Diagn. Microbiol. Infect. Dis. 2019, 95, 114874. [Google Scholar] [CrossRef] [PubMed]
- Overly, S.; Hayes, S.; Mehta, J.; Hamilton, K.; Peterson, D. Evaluating Patient-Specific Antibiograms. Open Forum Infect. Dis. 2017, 4 (Suppl. S1), S258. [Google Scholar] [CrossRef]
- Shah, A.; Justo, J.A.; Bookstaver, P.B.; Kohn, J.; Albrecht, H.; Al-Hasan, M.N. Application of Fluoroquinolone Resistance Score in Management of Complicated Urinary Tract Infections. Antimicrob. Agents Chemother. 2017, 61, e02313–e02316. [Google Scholar] [CrossRef] [PubMed]
- Rattanaumpawan, P.; Tolomeo, P.; Bilker, W.B.; Lautenbach, E. A Clinical Prediction Rule for Fluoroquinolone Resistance in Health-Acquired Gram-Negative Urinary Tract Infection. Infect. Control Hosp. Epidemiol. 2011, 32, 1124–1126. [Google Scholar] [CrossRef] [PubMed]
- DeMarsh, M.; Bookstaver, P.B.; Gordon, C.; Lim, J.; Griffith, N.; Bookstaver, N.K.; Justo, J.A.; Kohn, J.; Al-Hasan, M.N. Prediction of trimethoprim/sulfamethoxazole resistance in community-onset urinary tract infections. J. Glob. Antimicrob. Resist. 2020, 21, 218–222. [Google Scholar] [CrossRef]
- Metlay, J.P.; Strom, B.L.; Asch, D.A. Prior antimicrobial drug exposure: A risk factor for trimethoprim-sulfamethoxazole-resistant urinary tract infections. J. Antimicrob. Chemother. 2003, 51, 963–970. [Google Scholar] [CrossRef] [PubMed]
- Brown, P.D.; Freeman, A.; Foxman, B. Prevalence and Predictors of Trimthoprim-Sulfamethoxazole Resistance among Uropathogenic Escherichia coli Isolates in Michigan. Clin. Infect. Dis. 2002, 34, 1061–1066. [Google Scholar] [CrossRef] [PubMed]
- Goyal, D.; Dean, N.; Neill, S.; Jones, P.; Dascomb, K. Risk Factors for Community-Acquired Extended-Spectrum Beta-Lactamase-Producing Enterobacteriaceae Infections—A Retrospective Study of Symptomatic Urinary Tract Infections. Open Forum Infect. Dis. 2019, 4, ofy357. [Google Scholar] [CrossRef]
- Augustine, M.R.; Testerman, T.L.; Justo, J.A.; Bookstaver, P.B.; Kohn, J.; Albrecht, H.; Al-Hasan, M.N. Clinical Risk Score for Prediction of Extended-Spectrum B-Lactamase-Producing Enterobacteriaceae in Bloodstream Isolates. Infect. Control Hosp. Epidemiol. 2017, 38, 266–272. [Google Scholar] [CrossRef]
- Goodman, K.E.; Lessler, J.; Harris, A.D.; Milstone, A.M.; Tamma, P.D. A methodological comparison of risk scores versus decision trees for predicting drug-resistant infections: A case study using extended-spectrum beta-lactamase (ESBL) bacteremia. Infect. Control Hosp. Epidemiol. 2019, 40, 400–407. [Google Scholar] [CrossRef]
- Jorgensen, S.; Zurayk, M.; Yeung, S.; Terry, J.; Dunn, M.; Nieberg, P.; Wong-Beringer, A. Risk factors for early return visits to the emergency department in patients with urinary tract infection. Am. J. Emerg. Med. 2018, 36, 12–17. [Google Scholar] [CrossRef]
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing, 33rd ed.; CLSI supplement M100; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2023. [Google Scholar]
- Wang, H.; Wang, H.; Yu, X.; Zhou, H.; Li, B.; Chen, G.; Ye, Z.; Wang, Y.; Cui, X.; Zheng, Y.; et al. Impact of antimicrobial stewardship managed by clinical pharmacists on antibiotic use and drug resistance in a Chinese hospital, 2010–2016: A retrospective observational study. BMJ Open 2019, 9, e026072. [Google Scholar] [CrossRef]
- Eudy, J.L.; Pallotta, A.M.; Neuner, E.A.; Brummel, G.L.; Postelnick, M.J.; Schulz, L.T.; Spivak, E.S.; Wrenn, R.H. Antimicrobial Stewardship Practice in the Ambulatory Setting From a National Cohort. Open Forum Infect. Dis. 2020, 7, ofaa513. [Google Scholar] [CrossRef] [PubMed]
- Bookstaver, P.B.; Bland, C.M.; Griffin, B.; Stover, K.R.; Eiland, L.S.; McLaughlin, M. A Review of Antibiotic Use in Pregnancy. Pharmacotherapy 2015, 35, 1052–1062. [Google Scholar] [CrossRef]
- Urinary Tract Infections in Pregnant Individuals. Obstet. Gynecol. 2023, 142, 435–445. [CrossRef]
| Characteristic | Result | Reference Range |
|---|---|---|
| Color | Yellow | Clear Yellow |
| Clarity | Cloudy | Clear |
| LE | Moderate | Negative |
| Nitrite | Moderate | Negative |
| Protein | Negative | Negative |
| WBC | 126 HPF | 0–5 HPF |
| RBC | 0 HPF | 0–2 HPF |
| Bacteria | Moderate | Negative |
| LE = leukocyte esterase HPF = cells per high power field | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pizzuti, M.; Tsai, Y.V.; Winders, H.R.; Bookstaver, P.B.; Al-Hasan, M.N. Application of Precision Medicine Concepts in Ambulatory Antibiotic Management of Acute Pyelonephritis. Pharmacy 2023, 11, 169. https://doi.org/10.3390/pharmacy11060169
Pizzuti M, Tsai YV, Winders HR, Bookstaver PB, Al-Hasan MN. Application of Precision Medicine Concepts in Ambulatory Antibiotic Management of Acute Pyelonephritis. Pharmacy. 2023; 11(6):169. https://doi.org/10.3390/pharmacy11060169
Chicago/Turabian StylePizzuti, Morgan, Yuwei Vivian Tsai, Hana R. Winders, Paul Brandon Bookstaver, and Majdi N. Al-Hasan. 2023. "Application of Precision Medicine Concepts in Ambulatory Antibiotic Management of Acute Pyelonephritis" Pharmacy 11, no. 6: 169. https://doi.org/10.3390/pharmacy11060169