

Descriptive Report of a Pharmacist-Directed Preconception Care Outreach Program in a Rural Maternity Care Desert

Abstract
:1. Introduction
2. Project Description
2.1. Setting
2.2. Outreach Program Design
3. Findings
3.1. Reach
3.2. Effectiveness
3.3. Adoption
3.4. Implementation
3.5. Maintenance
4. Implications
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
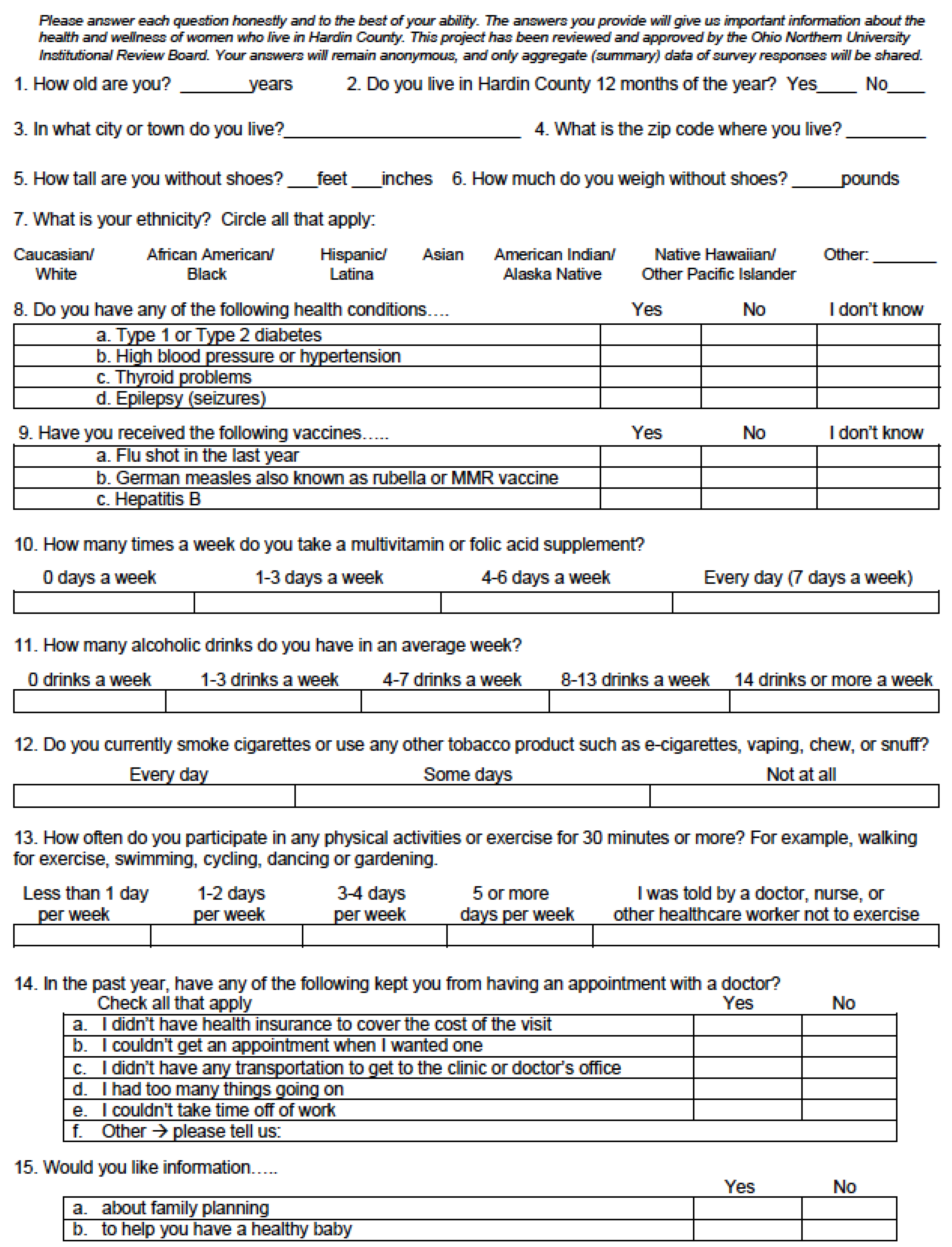
Appendix A
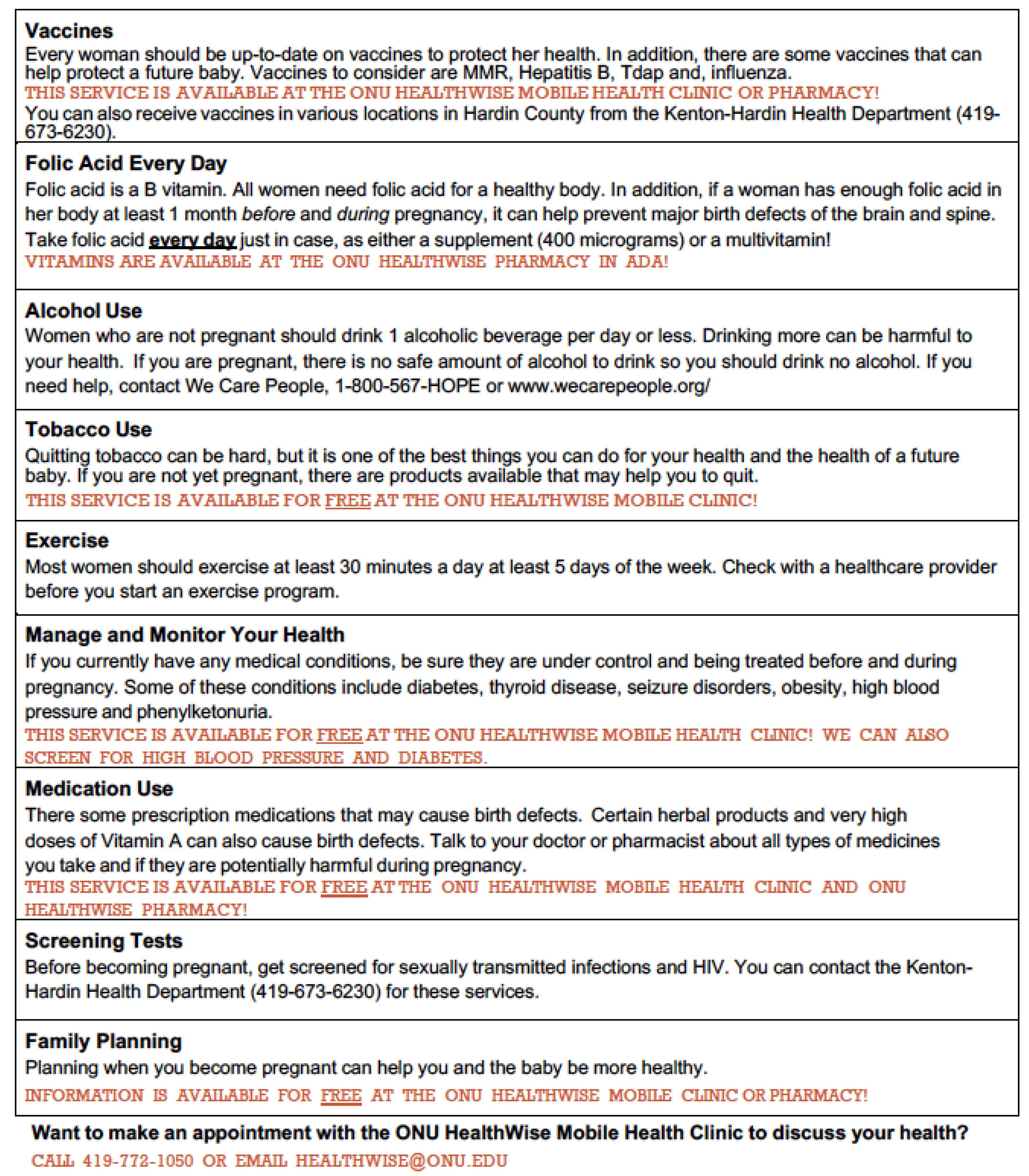
Appendix B

Appendix C
References
- U.S. Centers for Disease Control and Prevention. Recommendations to Improve Preconception Health and Health Care—United States: A Report of the CDC/ATSDR Preconception Care Work Group and the Select Panel on Preconception Care. MMWR 2006, 55, 1–22. [Google Scholar]
- American College of Obstetricians and Gynecologists. ACOG Committee Opinion No. 313: The Importance of Preconception Care in the Continuum of Women’s Health Care. Obstet. Gynecol. 2005, 106, 665–666. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Family Physicians. Preconception Care (Position Paper). Available online: https://www.aafp.org/about/policies/all/preconception-care.html (accessed on 30 August 2023).
- Guttmacher Institute. Unintended Pregnancy in the United States. Available online: https://www.guttmacher.org/fact-sheet/unintended-pregnancy-united-states (accessed on 30 August 2023).
- National Alliance of State Pharmacy Associations. Maternal Health Service Set for Pharmacists. Available online: https://naspa.us/resource/maternal-health-service-set-for-pharmacists/ (accessed on 30 August 2023).
- DiPietro Mager, N.; Bright, D.; Shipman, A.J. Beyond Contraception: Pharmacist Roles to Support Maternal Health. Pharmacy 2022, 10, 163. [Google Scholar] [CrossRef] [PubMed]
- DiPietro Mager, N.A. Fulfilling an Unmet Need: Roles for Clinical Pharmacists in Preconception Care. Pharmacotherapy 2016, 36, 141–151. [Google Scholar] [CrossRef]
- Whitfield, K.; Clavarino, A. Women’s Health from a Pharmacy Perspective. In Encyclopedia of Evidence in Pharmaceutical Public Health and Health Services Research in Pharmacy; Springer: Cham, Switzerland, 2022. [Google Scholar]
- El-Ibiary, S.Y.; Raney, E.C.; Moos, M.K. The Pharmacist’s Role in Promoting Preconception Health. J. Am. Pharm. Assoc. 2014, 54, e288–e303. [Google Scholar] [CrossRef]
- International Pharmaceutical Federation. The Effective Utilization of Pharmacists in Improving Maternal, Newborn, and Child Health. Available online: fip.org/file/1582 (accessed on 30 August 2023).
- Floyd, R.L.; Johnson, K.A.; Owens, J.R.; Verbiest, S.; Moore, C.A.; Boyle, C. A National Action Plan for Promoting Preconception Health and Health Care in the United States. J. Women’s Health 2013, 22, 797–802. [Google Scholar] [CrossRef]
- Hammarberg, K.; Stocker, R.; Romero, L.; Fisher, J. Pregnancy Planning Health Information and Service Needs of Women with Chronic Non-Communicable Conditions: A Systematic Review and Narrative Synthesis. BMC Pregnancy Childbirth 2022, 22, 236. [Google Scholar] [CrossRef]
- Marshall, C.J.; Huma, Z.; Deardorff, J.; Britton, L.E. Prepregnancy Counseling Among U.S. Women with Diabetes and Hypertension, 2016–2018. Am. J. Prev. Med. 2021, 61, 529–536. [Google Scholar] [CrossRef]
- Azeez, O.; Kulkarni, A.; Kuklina, E.V.; Kim, S.Y.; Cox, S. Hypertension and Diabetes in Non-pregnant Women of Reproductive Age in the United States. Prev. Chronic Dis. 2019, 16, E146. [Google Scholar] [CrossRef]
- U.S. Centers for Disease Control and Prevention. Smoking and Tobacco Use: Benefits of Quitting. Available online: https://www.cdc.gov/tobacco/quit_smoking/how_to_quit/benefits/index.htm (accessed on 30 August 2023).
- U.S. Department of Health and Human Services Office on Women’s Health. Vitamins and Minerals for Women. Available online: https://www.womenshealth.gov/healthy-eating/how-eat-health/vitamins-and-minerals-women (accessed on 30 August 2023).
- Scott, P.A.; Quotah, O.F.; Dalrymple, K.V.; White, S.L.; Poston, L.; Farebrother, J.; Lakhani, S.; Alter, M.; Blair, M.; Weinman, J.; et al. Community Pharmacist-Led Interventions to Improve Preconception and Pregnancy Health: A Systematic Review. Pharmacy 2021, 9, 171. [Google Scholar] [CrossRef]
- DiPietro Mager, N.A.; Bright, D.R. Promising Practices and Pockets of Excellence: Community Pharmacists Supporting Wellness for Reproductive-Age Women. Health Serv. Res. 2022, 57, 1384–1389. [Google Scholar] [CrossRef] [PubMed]
- Bright, D.R.; DiPietro Mager, N.A. Preconception Care and Contraception Services: Opportunities for Community Pharmacists. J. Am. Coll. Clin. Pharm. 2019, 2, 414–422. [Google Scholar] [CrossRef]
- Reidenbach, M.; Bade, L.; Bright, D.; DiPietro Mager, N.; Ellis, A. Preconception Care Needs Among Female Patients of Childbearing Age in an Urban Community Pharmacy Setting. J. Am. Pharm. Assoc. 2019, 49, S52–S56. [Google Scholar] [CrossRef] [PubMed]
- Luli, A.J.; Tran, N.; Ataya, A.; Rafie, S. Patient Screenings for Preconception Health Interventions at a Community Pharmacy. Pharmacy 2020, 8, 181. [Google Scholar] [CrossRef] [PubMed]
- U.S. Health Resources and Services Administration. Shortage Designation Scoring Criteria. Available online: https://bhw.hrsa.gov/shortage-designation/hpsas (accessed on 30 August 2023).
- March of Dimes. Nowhere to Go: Maternity Care Deserts across the U.S. Available online: https://www.marchofdimes.org/maternity-care-deserts-report (accessed on 30 August 2023).
- Center for Community Health and Development, University of Kansas. The Community Tool Box: Using Outreach to Increase Access. Available online: https://ctb.ku.edu/en/table-of-contents/implement/access-barriers-opportunities/outreach-to-increase-access/main (accessed on 30 August 2023).
- Surgo Ventures. Maternal Vulnerability in the U.S. Available online: https://mvi.surgoventures.org/ (accessed on 30 August 2023).
- American College of Obstetricians and Gynecologists. ACOG Committee Opinion No. 586: Health Disparities in Rural Women. Obstet. Gynecol. 2014, 123, 384–388. [Google Scholar] [CrossRef]
- Rural Health Information Hub. Rural Health Disparities. Available online: https://www.ruralhealthinfo.org/topics/rural-health-disparities (accessed on 30 August 2023).
- United States Census Bureau. Quick Stats—Hardin County, Ohio. Available online: https://www.census.gov/quickfacts/fact/table/hardincountyohio/PST045222 (accessed on 30 August 2023).
- ONU HealthWise. Available online: https://www.onu.edu/student-life/health-and-wellness-resources/onu-healthwise (accessed on 30 August 2023).
- Lee, V. ONU Healthwise Mobile Health Clinic Brings Needed Services to Underserved County. Available online: https://drugstorenews.com/pharmacy/onu-healthwise-mobile-health-clinic-brings-needed-services-medically-underserved-county (accessed on 30 August 2023).
- Rural Health Information Hub. Ohio Northern University’s HealthWise Mobile Outreach Program. Available online: https://www.ruralhealthinfo.org/project-examples/999 (accessed on 30 August 2023).
- Healthy Lifestyles Coalition of Hardin County. Available online: https://www.facebook.com/HardinHLC (accessed on 30 August 2023).
- Shannon, G.D.; Alberg, C.; Nacul, L.; Pashayan, N. Preconception Healthcare Delivery at a Population Level: Construction of Public Health Models of Preconception Care. Matern. Child Health J. 2014, 18, 1512–1531. [Google Scholar] [CrossRef]
- Ohio State Health Improvement Plan (SHIP) 2020–2022. Available online: https://odh.ohio.gov/static/SHIP/2020-2022/2020-2022-SHIP.pdf (accessed on 30 August 2023).
- Hardin County Community Health Status Assessment. Available online: https://www.ohiohealth.com/siteassets/find-a-location/hospitals/hardin-memorial-hospital/about-us/community-health-needs-assessment/ohiohealth-chna-2022-hardin-memorial-hospital.pdf (accessed on 30 August 2023).
- Squiers, L.; Mitchell, E.W.; Levis, D.M.; Lynch, M.; Dolina, S.; Margolis, M.; Scales, M.; Kish-Doto, J. Consumers’ Perceptions of Preconception Health. Am. J. Health Promot. 2013, 27, S10–S19. [Google Scholar] [CrossRef]
- U.S. Centers for Disease Control and Prevention. Behavioral Risk Factor Surveillance System. Available online: https://www.cdc.gov/brfss/ (accessed on 30 August 2023).
- U.S. Centers for Disease Control and Prevention. Pregnancy Risk Assessment Monitoring System. Available online: https://www.cdc.gov/prams/index.htm (accessed on 30 August 2023).
- Ohio Department of Health. Ohio Pregnancy Assessment Survey. Available online: https://odh.ohio.gov/know-our-programs/ohio-pregnancy-assessment-survey-opas (accessed on 30 August 2023).
- DiPietro Mager, N.A.; Zollinger, T.W.; Turman, J.E., Jr.; Zhang, J.; Dixon, B.E. Preconception Health Status and Associated Disparities Among Rural, Midwestern Women in the United States. Birth 2023, 50, 127–137. [Google Scholar] [CrossRef]
- Robbins, C.L.; D’angelo, D.; Zapata, L.; Boulet, S.L.; Sharma, A.J.; Adamski, A.; Farfalla, J.; Stampfel, C.; Verbiest, S.; Kroelinger, C. Preconception Health Indicators for Public Health Surveillance. J. Women’s Health 2018, 27, 430–443. [Google Scholar] [CrossRef]
- RE-AIM: Improving Public Health Relevance and Population Health Impact. Available online: https://re-aim.org/ (accessed on 30 August 2023).
- Kwan, B.M.; McGinnes, H.L.; Ory, M.G.; Estabrooks, P.A.; Waxmonsky, J.A.; Glasgow, R.E. RE-AIM in the Real World: Use of the RE-AIM Framework for Program Planning and Evaluation in Clinical and Community Settings. Front. Public Health. 2019, 7, 345. [Google Scholar] [CrossRef]
- RE-AIM: Assessments Using RE-AIM and PRISM. Available online: https://re-aim.org/assessments/ (accessed on 30 August 2023).
- Eastwood, K.A.; Allen-Walker, V.A.; Maxwell, M.; McKinley, M.C. Raising Awareness of Pre-conception Care in Community Pharmacies: A Feasibility Study. Pilot Feasibil. Stud. 2022, 8, 44. [Google Scholar] [CrossRef] [PubMed]
- Silverio, S.A.; Karki, P.; Lakhani, S.; Alter, M.; Weinman, J.; Flynn, A. “People Still Want a Face and That’s Where We Can Fill In”: A Qualitative Study of Community Pharmacists’ Experiences of Providing Healthcare Advice About Preconception and Pregnancy. Int. J. Pharm. Pract. 2023, 31, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Ng, C.; Najjar, R.; DiPietro Mager, N.; Rafie, S. Pharmacist and Student Pharmacist Perspectives on Providing Preconception Care in the United States. J. Am. Pharm. Assoc. 2018, 58, 426–431. [Google Scholar] [CrossRef] [PubMed]
- Ceulemans, M.; Liekens, S.; Van Calsteren, K.; Allegaert, K.; Foulon, V. Community Pharmacists’ Attitudes, Barriers, Knowledge and Counseling Practice with Regard to Preconception, Pregnancy and Lactation. Res. Soc. Adm. Pharm. 2020, 16, 1192–1200. [Google Scholar] [CrossRef]
- U.S. Centers for Medicare and Medicaid Services. The Accountable Health Communities Health-Related Social Needs Screening Tool. Available online: https://innovation.cms.gov/files/worksheets/ahcm-screeningtool.pdf (accessed on 30 August 2023).
- Clark, A.D.; DiPietro Mager, N.A. “Nobody Talks About It”: Preconception Health and Care Among Women in the Rural, Midwestern United States. Womens Health 2022, 18, 1–10. [Google Scholar] [CrossRef]
- Frey, K.A.; Navarro, S.M.; Kotelchuck, M.; Lu, M.C. The Clinical Content of Preconception Care: Preconception Care for Men. Am. J. Obstet. Gynecol. 2008, 199, S389–S395. [Google Scholar] [CrossRef]
- U.S. Centers for Disease Control and Prevention. Preconception Health and Health Care Is Important for All. Available online: https://www.cdc.gov/preconception/overview.html (accessed on 30 August 2023).
- Zagaria, M.A.E. Male Preconception Health: Impact of Age, Medications, and Other Exposures. US Pharm. 2016, 41, 15–17. [Google Scholar]
- Sainafata, A.; Ikhlasiahc, M.; Matd, S.B.; Hassand, H.C. Preconception Care in Adolescents. Enferm. Clín. 2020, 30, 73–76. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Age, Years n (%) | Race/Ethnicity n (%) |
|---|---|
| 18–24: 24 (17.0%) | White, non-Hispanic: 135 (95.8%) |
| 25–34: 63 (44.7%) | Two or more races: 4 (2.8%) |
| 35–45: 54 (38.3%) | White, Hispanic: 2 (1.4%) |
| Characteristic | n (%) |
|---|---|
| Medical Conditions | |
| Type 1 or 2 diabetes | 3 (2.1%) |
| Hypertension | 13 (9.2%) |
| Overweight/obesity | 112 (79.4%) |
| Health Behaviors | |
| Tobacco use | 29 (20.6%) |
| Not taking folic acid or multivitamin daily | 94 (66.7%) |
| Eight or more alcoholic drinks/week | 1 (0.7%) |
| Not exercising at least 30 min for 5 days/week | 106 (75.2%) |
| Barrier | n (%) |
|---|---|
| No health insurance | 17 (12.1%) |
| Unable to get appointment | 18 (12.8%) |
| No transportation | 15 (10.6%) |
| Too many things going on | 47 (33.3%) |
| Could not take time off of work | 28 (19.9%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
DiPietro Mager, N. Descriptive Report of a Pharmacist-Directed Preconception Care Outreach Program in a Rural Maternity Care Desert. Pharmacy 2023, 11, 176. https://doi.org/10.3390/pharmacy11060176
DiPietro Mager N. Descriptive Report of a Pharmacist-Directed Preconception Care Outreach Program in a Rural Maternity Care Desert. Pharmacy. 2023; 11(6):176. https://doi.org/10.3390/pharmacy11060176
Chicago/Turabian StyleDiPietro Mager, Natalie. 2023. "Descriptive Report of a Pharmacist-Directed Preconception Care Outreach Program in a Rural Maternity Care Desert" Pharmacy 11, no. 6: 176. https://doi.org/10.3390/pharmacy11060176