
Collaborative Prescribing Practice in Managing Patients Post-Bariatric Surgery in a Tertiary Centre in Singapore


Abstract
1. Introduction
2. Materials and Methods
2.1. Development of Collaborative Prescribing Agreement (CPA)
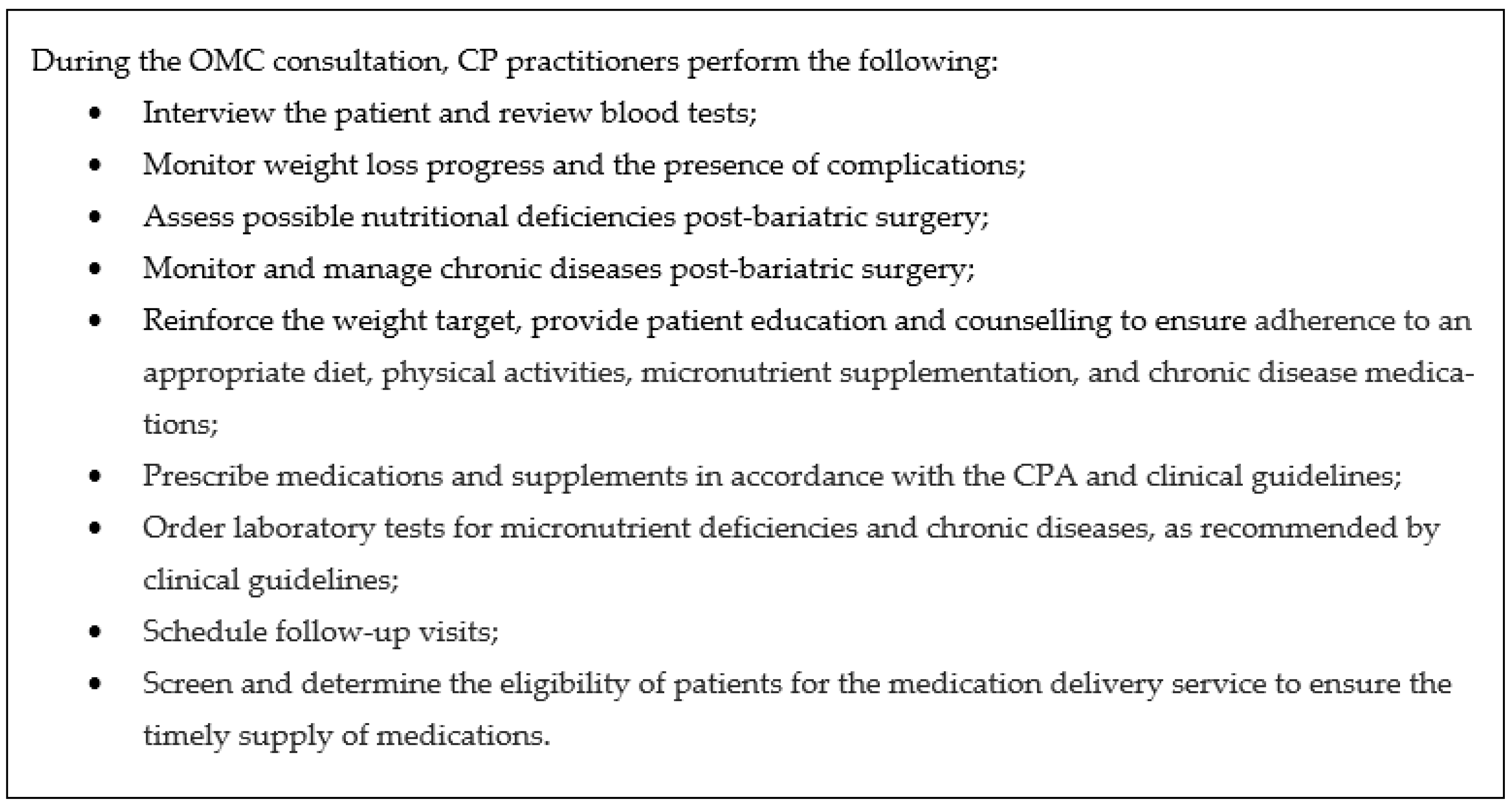
2.2. Scopes of Practice of OMC CP Practitioners
2.3. Post-Bariatric Surgery Patient’s Journey in a CP Model
2.4. Quality and Safety Monitoring
2.5. Competency Maintenance for CP Practitioner
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Allison, D.B.; Downey, M.; Atkinson, R.L.; Billington, C.J.; Bray, G.A.; Eckel, R.H.; Finkelstein, E.A.; Jensen, M.D.; Tremblay, A. Obesity as a disease: A white paper on evidence and arguments commissioned by the Council of the Obesity Society. Obesity 2008, 16, 1161–1177. [Google Scholar] [CrossRef]
- World Health Organisation. Obesity: Preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ. Tech. Rep. Ser. 2000, 894, 1–253. [Google Scholar]
- Bray, G.A.; Kim, K.K.; Wilding, J.P.H.; World Obesity Federation. Obesity: A chronic relapsing progressive disease process. A position statement of the World Obesity Federation. Obes. Rev. 2017, 18, 715–723. [Google Scholar] [CrossRef]
- National Task Force on the Prevention and Treatment of Obesity; Billington, C.J.; Epstein, L.H.; Goodwin, N.J.; Hill, J.O.; Pi-Sunyer, F.X.; Rolls, B.J.; Stern, J.; Wadden, T.A.; Weinsier, R.L.; et al. Overweight, obesity, and health risk. Arch. Intern. Med. 2000, 160, 898. [Google Scholar] [CrossRef]
- Collaboration NCDRF. Trends in adult body-mass index in 200 countries from 1975 to 2014: A pooled analysis of 1698 population-based measurement studies with 19.2 million partici-pants. Lancet 2016, 387, 1377–1396. [Google Scholar] [CrossRef]
- Ministry of Health. National Population Health Survey 2020. 2020. Available online: https://www.moh.gov.sg/docs/librariesprovider5/default-document-library/nphs-2020-survey-report.pdf (accessed on 16 November 2023).
- Soon, G.; Koh, Y.H.; Wong, M.L.; Lam, P.W. Obesity Prevention and Control Efforts in Singapore. 2008. Available online: https://www.nbr.org/wp-content/uploads/pdfs/publications/obesity-prevention-and-control-efforts-in-singapore-2008-case-study.pdf (accessed on 16 November 2023).
- Goh, L.G.; Pang, J. Obesity in Singapore, Prevention and Control. Singap. Fam. Physician 2012, 38, 8–13. [Google Scholar]
- Wolfe, B.M.; Kvach, E.; Eckel, R.H. Treatment of Obesity: Weight Loss and Bariatric Surgery. Circ. Res. 2016, 118, 1844–1855. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Obesity: Identification, Assessment and Management. Clinical Guideline [CG189]. 2014. Available online: https://www.nice.org.uk/guidance/cg189 (accessed on 16 November 2023).
- Avenell, A.; Robertson, C.; Skea, Z.; Jacobsen, E.; Boyers, D.; Cooper, D.; Aceves-Martins, M.; Retat, L.; Fraser, C.; Aveyard, P.; et al. Bariatric surgery, lifestyle interventions and orlistat for severe obesity: The REBALANCE mixed-methods systematic review and economic evaluation. Health Technol. Assess. 2018, 22, 1–246. [Google Scholar] [CrossRef]
- Heymsfield, S.B.; Wadden, T.A. Mechanisms, pathophysiology, and management of obesity. N. Engl. J. Med. 2017, 376, 254–266. [Google Scholar] [CrossRef]
- Sjostrom, L.; Narbro, K.; Sjostrom, C.D.; Karason, K.; Larsson, B.; Wedel, H.; Lystig, T.; Sullivan, M.; Bouchard, C.; Carlsson, B.; et al. Effects of bariatric surgery on mortality in Swedish obese subjects. N. Engl. J. Med. 2007, 357, 741–752. [Google Scholar] [CrossRef]
- Courcoulas, A.P.; Belle, S.H.; Neiberg, R.H.; Pierson, S.K.; Eagleton, J.K.; Kalarchian, M.A.; Delany, J.P.; Lang, W.; Jakicic, J.M. Three-year outcomes of bariatric surgery vs lifestyle intervention for type 2 diabetes mellitus treatment: A randomized clinical trial. JAMA Surg. 2015, 150, 931–940. [Google Scholar] [CrossRef]
- Syn, N.L.; Cummings, D.E.; Wang, L.Z.; Lin, D.J.; Zhao, J.J.; Loh, M.; Koh, Z.J.; Chew, C.A.; Loo, Y.E.; Tai, B.C.; et al. Association of metabolic–bariatric surgery with long-term survival in adults with and without diabetes: A one-stage meta-analysis of matched cohort and prospective controlled studies with 174,772 participants. Lancet 2021, 397, 1830–1841. [Google Scholar] [CrossRef]
- Sjöström, L.; Peltonen, M.; Jacobson, P.; Sjöström, C.D.; Karason, K.; Wedel, H.; Ahlin, S.; Anveden, Å.; Bengtsson, C.; Bergmark, G.; et al. Bariatric surgery and long-term cardiovascular events. J. Am. Med. Assoc. 2012, 307, 56–65. [Google Scholar] [CrossRef]
- Kwok, C.S.; Pradhan, A.; Khan, M.A.; Anderson, S.G.; Keavney, B.D.; Myint, P.K.; Mamas, M.A.; Loke, Y.K. Bariatric surgery and its impact on cardiovascular disease and mortality: A systematic review and meta-analysis. Int. J. Cardiol. 2014, 173, 20–28. [Google Scholar] [CrossRef]
- ElSayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Hilliard, M.E.; Isaacs, D.; Johnson, E.L.; et al. Obesity and Weight Management for the Prevention and Treatment of Type 2 Diabetes: Standard of Care in Diabetes—2023. Diabetes Care 2023, 46 (Suppl. S1), S128–S139. [Google Scholar] [CrossRef]
- Mechanick, J.I.; Youdim, A.; Jones, D.B.; Garvey, W.T.; Hurley, D.L.; Mcmahon, M.M.; Heinberg, L.J.; Kushner, R.; Adams, T.D.; Shikora, S.; et al. Clinical practice guidelines for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient: 2013 update. Cosponsored by American Association of Clinical Endocrinologists, the Obesity Society, and American Society for Metabolic & Bariatric Surgery. Endocr. Pract. 2013, 19, 337–372. [Google Scholar]
- Aills, L.; Blankenship, J.; Buffington, C.; Furtado, M.; Parrott, J. ASMBS Allied health nutritional guidelines for the surgical weight loss patient. Surg. Obes. Relat. Dis. 2008, 4 (Suppl. S5), S73–S108. [Google Scholar] [CrossRef]
- Parrott, J.; Frank, L.; Rabena, R.; Craggs-Dino, L.; Isom, K.A.; Greiman, L. American Society for Metabolic and Bariatric Surgery integrated health nutritional guidelines for the surgical weight loss patient 2016 update: Micronutrients. Surg. Obes. Relat. Dis. 2017, 13, 727–741. [Google Scholar] [CrossRef]
- Griffith, D.P.; Liff, D.A.; Ziegler, T.R.; Esper, G.J.; Winton, E.F. Acquired copper deficiency: A potentially serious and preventable complication following gastric bypass surgery. Obesity 2009, 17, 827–831. [Google Scholar] [CrossRef]
- Genead, M.A.; Fishman, G.A.; Lindeman, M. Fundus white spots and acquired night blindness due to vitamin A deficiency. Doc. Ophthalmol. 2009, 119, 229–233. [Google Scholar] [CrossRef]
- Massoure, P.L.; Camus, O.; Fourcade, L.; Simon, F. Bilateral leg oedema after bariatric surgery: A selenium-deficient cardiomyopathy. Obes. Res. Clin. Pract. 2017, 11, 622–626. [Google Scholar] [CrossRef]
- Wilson, H.O.; Datta, D.B. Complications from micronutrient deficiency following bariatric surgery. Ann. Clin. Biochem. 2014, 51, 705–709. [Google Scholar] [CrossRef]
- Chacko, J.G.; Rodriguez, C.J.; Uwaydat, S.H. Nutritional optic neuropathy status post bariatric surgery. Neuroophthalmology 2012, 36, 165–167. [Google Scholar] [CrossRef]
- Lee, P.C.; Ganguly, S.; Dixon, J.B.; Tan, H.C.; Lim, C.H.; Tham, K.W. Nutritional Deficiencies in Severe Obesity: A Multiethnic Asian Cohort. Obes. Surg. 2019, 29, 166–171. [Google Scholar] [CrossRef]
- Lupoli, R.; Lembo, E.; Saldalamacchia, G.; Avola, C.K.; Angrisani, L.; Capaldo, B. Bariatric surgery and long-term nutritional issues. World J. Diabetes 2017, 8, 464–474. [Google Scholar] [CrossRef]
- Syn, N.L.; Lee, P.C.; Kovalik, J.; Tham, K.W.; Ong, H.S.; Chan, W.H.; Tan, C.S.; Lim, C.H. Associations of Bariatric Interventions With Micronutrient and Endocrine Disturbances. JAMA Netw. Open 2020, 3, e205123. [Google Scholar] [CrossRef]
- David, E.A.; Dana, A.T.; Robert, F.K.; Anita, P.C. Benefits and Risks of Bariatric Surgery in Adults: A Review. JAMA 2020, 324, 879–887. [Google Scholar] [CrossRef]
- Kim, H.J.; Madan, A.; Fenton-Lee, D. Does patient compliance with follow-up influence weight loss after gastric bypass surgery? A systematic review and meta-analysis. Obes. Surg. 2014, 24, 647–651. [Google Scholar] [CrossRef]
- Karefylakis, C.; Näslund, I.; Edholm, D.; Sundbom, M.; Karlsson, F.A.; Rask, E. Prevalence of anemia and related deficiencies 10 years after gastric bypass: A retrospective study. Obes. Surg. 2015, 25, 1019–1023. [Google Scholar] [CrossRef]
- Schijns, W.; Schuurman, L.T.; Melse-Boonstra, A.; van Laarhoven, C.J.H.M.; Berends, F.J.; Aarts, E.O. Do specialized bariatric multivitamins lower deficiencies after RYGB? Surg. Obes. Relat. Dis. 2018, 14, 1005–1012. [Google Scholar] [CrossRef] [PubMed]
- Mechanick, J.I.; Apovian, C.; Brethaver, S.; Garvey, W.T.; Joffe, A.M.; Kim, J.; Kushner, R.F.; Lindquist, R.; Pessah-Pollack, R.; Seger, J.; et al. Clinical Practice Guidelines for the Perioperative Nutrition, Metabolic, and Nonsurgical support of the Patients Undergoing Bariatric Procedures—2019 Update: Cosponsored by American Association of Clinical Endocrinologists/American College of Endocrinology, The Obesity Society, American Society for Metabolic & Bariatric Surgery, Obesity Medicine Association, and American Society of Anesthesiologists. Obesity 2020, 16, 175–247. [Google Scholar]
- National Institute for Health and Care Excellence. Obesity: Clinical Assessment and Management. Quality Standard [QS127]. 2016. Available online: https://www.nice.org.uk/guidance/qs127 (accessed on 16 November 2023).
- O’Kane, M.; Pinkney, J.; Aasheim, E.; Barth, J.H.; Batterham, R.L.; Welbourn, R. BOMSS Guidelines on Peri-Operative and Postoperative Biochemical Monitoring and Micronutrient Replacement for Patients Undergoing Bariatric Surgery. 2014. Available online: https://bomss.org/wp-content/uploads/2021/06/BOMSS-guidelines-Final-version1Oct14.pdf (accessed on 16 November 2023).
- Busetto, L.; Dicker, D.; Azran, C.; Batterham, R.L.; Farpour-Lambert, N.; Fried, M.; Hjelmesæth, J.; Kinzl, J.; Leitner, D.R.; Makaronidis, J.M.; et al. Practical recommendations of the Obesity Management Task Force of the European Association for the Study of Obesity for the post-bariatric surgery medical management. Obes. Facts 2017, 10, 597–632. [Google Scholar] [CrossRef] [PubMed]
- National University of Singapore. Media Factsheet on National Collaborative Prescribing Programme. 2018. Available online: https://medicine.nus.edu.sg/nursing/2018/07/media-factsheet-on-national-collaborative-prescribing-programme/ (accessed on 16 November 2023).
- Ministry of Health. Guidelines for the Implementation of Collaborative Prescribing Services. 2018. Available online: https://www.moh.gov.sg/docs/librariesprovider4/guidelines/guidelines-for-implementation-of-collaborative-prescribing-services.pdf (accessed on 16 November 2023).
- Committee of Supply: Beyond Quality to Value. Ensuring an Affordable and Sustainable Healthcare System. 2018. Available online: https://www.moh.gov.sg/docs/librariesprovider5/pressroom/current-issues/cos-2018-media-factsheet-beyond-quality-to-value.pdf (accessed on 16 November 2023).
- Han, A.; Nguyen, N.Y.; Kamalay, S. Efficacy of a Bariatric Surgery Clinic-Based Pharmacist. Obes. Surg. 2022, 32, 2618–2624. [Google Scholar] [CrossRef] [PubMed]
- Prooyen, A.M.V.; Hicks, J.L.; Lin, E.L.; Davis, S.S.; Singh, A.; Harris, D.A.; Elissa, A.; Falconer, E.A.; Hechenbleikner, E.M. Evaluation of an Inpatient Pharmacy Consult on Discharge Medications in Bariatric Surgery Patients. J. Pharm. Pract. 2021, 36, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Sahebzamani, F.M. Management of inadequate weight loss or weight regain in post-bariatric surgical patients. J. Am. Assoc. Nurse Pract. 2020, 32, 490–492. [Google Scholar] [CrossRef]
- Grindel, M.E.; Grindel, C.G. Nursing care of the person having bariatric surgery. Medsurg Nurs. Off. J. Acad. Med.-Surg. Nurses 2006, 15, 129–145. [Google Scholar]
- Courtenay, M. An overview of developments in nurse prescribing in the UK. Nurs. Stand. 2018, 33, 40–44. [Google Scholar] [CrossRef]
- Jebara, T.; Cunningham, S.; MacLure, K.; Awaisu, A.; Pallivalapila, A.; Stewart, D. Stakeholders’ views and experiences of pharmacist prescribing: A systematic review. Br. J. Clin. Pharmacol. 2018, 84, 1883–1905. [Google Scholar] [CrossRef]
- Creedon, R.; O’Connell, E.; McCarthy, G.; Lehane, B. An evaluation of nurse prescribing. Part 1: A literature review. Br. J. Nurs. 2009, 18, 1322–1327. [Google Scholar] [CrossRef]
- Buchwald, H.; Avidor, Y.; Braunwald, E.; Jensen, M.D.; Pories, W.; Fahrbach, K.; Schoelles, K. Bariatric surgery: A systematic review and meta-analysis. JAMA 2004, 292, 1724–1737. [Google Scholar] [CrossRef]
- Lee, P.C.; Tham, K.W.; Ganguly, S.; Tan, H.C.; Eng, A.K.H.; Dixon, J.B. Ethnicity Does Not Influence Glycemic Outcomes or Diabetes Remission After Sleeve Gastrectomy or Gastric Bypass in a Multiethnic Asian Cohort. Obes. Surg. 2018, 28, 1511–1518. [Google Scholar] [CrossRef] [PubMed]
- Von, D.A.; Andris, D.A. Anemia after bariatric surgery: More than just iron deficiency. Nutr. Clin. Pract. 2009, 24, 217–226. [Google Scholar] [CrossRef]
- Chen, G.L.; Kubat, E.; Eisenberg, D. Prevalence of Anemia 10 Years After Roux-en-Y Gastric Bypass in a Single Veterans Affairs Medical Center. JAMA Surg. 2018, 153, 86–87. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.Y.T.; Syn, N.L.; Lin, D.J.; Lim, C.H.; Ganguly, S.; Ong, H.S.; Tan, J.T.H.; Lee, P.C. Centile Charts for Monitoring of Weight Loss Trajectories After Bariatric Surgery in Asian Patients. Obes. Surg. 2021, 31, 4781–4789. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Indicators | Target |
|---|---|---|
| Process | Number of patient visits per year | ≥30 |
| Safety | Number of errors or near-misses in prescribing or laboratory test ordering Number of CP agreement deviations | No event No event |
| Outcome | Appropriate weight loss post-surgery
| ≥50% ≥30% |
| Quality | Proportion of patients with nutritional deficiency and disease control:
| <10% <10% <10% <10% >80% |
| Criteria for Escalation to Referring Endocrinologist | Number of Consultation |
|---|---|
| Abnormalities in blood tests or vital signs | 66 |
| Acute or new medical problems since the last visit that require further investigation or hospitalisation | 35 |
| Complications | 12 |
| Pregnancy | 6 |
| 10% weight regain above the previous visit | 4 |
| Total | 123 |
| Types of Therapy Adjustment | Number |
|---|---|
| Micronutrient supplement initiation/adjustment | 195 |
| Others (starting or stopping medications or meal replacement, ordering additional investigations for acute medical conditions, etc.) | 73 |
| Chronic disease medication initiation/adjustment | 51 |
| Weight loss medication initiation/adjustment | 23 |
| Intravenous iron infusion initiation | 21 |
| Bringing forward appointments for early review | 19 |
| Referral to specialists of other disciplines or the emergency department | 11 |
| Total | 393 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khee, G.Y.; Lim, P.S.; Chan, Y.L.; Lee, P.C. Collaborative Prescribing Practice in Managing Patients Post-Bariatric Surgery in a Tertiary Centre in Singapore. Pharmacy 2024, 12, 31. https://doi.org/10.3390/pharmacy12010031
Khee GY, Lim PS, Chan YL, Lee PC. Collaborative Prescribing Practice in Managing Patients Post-Bariatric Surgery in a Tertiary Centre in Singapore. Pharmacy. 2024; 12(1):31. https://doi.org/10.3390/pharmacy12010031
Chicago/Turabian StyleKhee, Giat Yeng, Paik Shia Lim, Yoke Ling Chan, and Phong Ching Lee. 2024. "Collaborative Prescribing Practice in Managing Patients Post-Bariatric Surgery in a Tertiary Centre in Singapore" Pharmacy 12, no. 1: 31. https://doi.org/10.3390/pharmacy12010031
APA StyleKhee, G. Y., Lim, P. S., Chan, Y. L., & Lee, P. C. (2024). Collaborative Prescribing Practice in Managing Patients Post-Bariatric Surgery in a Tertiary Centre in Singapore. Pharmacy, 12(1), 31. https://doi.org/10.3390/pharmacy12010031